1. Introduction
Owing to its multiple mutations, immune evasion, and fast transmissibility, in the COVID-19 pandemic, the SARS-coronavirus-2 (SARC-CoV-2) omicron variant emerged as a very alarming wave of infection. According to recent statistics, SARC-CoV-2 has infected over 421 million people globally, with over 5.8 million deaths. In November 2021, a new SARS-CoV-2 variant of concern (VOC) named “omicron” was first detected in South Africa [
1]. Although the omicron variant is less severe than earlier variants of SARC-CoV-2, the rapid transmissibility of this variant has imposed severe effects on other health conditions and led to overwhelmed health systems across the globe. Furthermore, the risks of hospitalization, intensive care unit admission, and mortality from omicron are still considerable in non-vaccinated people [
2].
As frontline respondents to this deadly pandemic, frontline healthcare workers (F-HCWs), including doctors, nurses, and paramedics, are most prone to contracting this fatal infection. F-HCWs are working as key players to mitigate the effect of the COVID-19 pandemic and its consequences, as well as implementing preventive measures to stop the transmission of the virus. Going through the published literature, it has been well investigated that, regarding COVID-19, these F-HCWs have significant psychological stress, worry, and anxiety and have been struggling with uncertainty since the beginning of the COVID-19 pandemic [
2]. Similarly, in the context of the omicron upsurge, difficult tolerance of preventive obstacles and high uncertainty outcomes have been observed and found to correlate with stress and anxiety in the daily life of frontline healthcare professionals’ mental health. Thus, it is crucial to explore this correlation between F-HCW’s mental health and ongoing pandemic uncertainty and obstacles in daily life. In the present study, considering the clinical and psychological importance of association, by employing coping theory, we investigated and predicted the linkages between daily obstacles and frontline healthcare professionals’ mental health during omicron under the five essential components: cognitive efforts, behavioral efforts, internal demands, external pressures, and resources (
Figure 1).
The coping theory was used in this study to investigate the predicted linkages. According to the definition of coping, it is “the cognitive and behavioral efforts made to deal with specific external and/or internal demands that are regarded as demanding or exceeding the person’s resources” [
3]. Coping is concerned with a person’s adaptive actions in response to stressful events in his or her life. Coping theory is the most extensively used and accepted in psychology under the contextual model [
4]. The five essential components of this idea are cognitive efforts, behavioral efforts, internal demands, external pressures, and resources [
5].
The things that individuals deal with, as well as their significance and relevance, are evaluated (primary appraisal). Similarly, during the omicron wave, medical experts ask themselves, “What am I risking in this position?” The major issue is assessing the likely implications of this occurrence (specific internal/external demands), as well as the disruption’s relevance. In monitoring, disruptive events are divided into two categories: challenges and threats. Individuals will obtain information regarding COVID-19 or omicron in this study. Challenges are events that are believed to have good results. In contrast, threats are events that have negative effects (they will receive stress regarding COVID-19 and are prone to threat, psychological distress, and adverse work outcomes). In addition to appraising the severity of an experience, people frequently examine the coping skills (as an internal resource) available to them (secondary appraisal). People decide how much control they have over the problem and what they should do about it using the coping abilities at their disposal [
4]. As previously stated, the coping theory is suited for analyzing the hypothesized model since it encompasses the complete mechanism of how health workers would react to COVID-19 while performing their duties, specifically in the omicron wave.
3. Method
3.1. Sampling and Data Collection Procedures
Sample and procedure full-time health professionals were recruited physically (where researchers are providing services as a psychologist), as well as through electronic postings on several representative social media sites (e.g., Facebook, LinkedIn, WhatsApp). The recruitment advertisements explained the process of the study, inclusion criteria, and compensation for participation (a $5 gift card for each participant). The study was completed in two stages. In Stage 1, participants were emailed their consent details, and, in stage 2, participants completed daily surveys over two weeks (ten consecutive working days).
Sample and procedure full-time health professionals were recruited both physically (where 2st and 3nd authors provide services as a psychologist) and electronically (via posts on various popular social networking sites) (e.g., Facebook, LinkedIn, WhatsApp). The recruiting ads outlined the study’s procedure, inclusion criteria, and pay ($5 gift card for each participant).
The research was split into two parts. Participants were emailed their consent details in stage 1, and they completed daily surveys over two weeks in stage 2 (ten consecutive working days). To be eligible, participants had to be full-time (more than 30 h per week) health workers aged 18 to 65 who were proficient in English. During the research period, participants must work during typical working hours (e.g., 9 a.m. to 5 p.m., Monday through Friday) and have access to email and the internet at home and work.
One-hundred-ninety-three people expressed interest in the study by contacting the researchers and sharing their email addresses. Eligible participants were emailed a link to a detailed research overview, an informed consent form, and a one-time first survey. After individuals who completed the consent form at the first stage and whose initial consent was returned, Stage 2 of the research began. For 10 consecutive workdays, participants were emailed a diary survey after work between 5:30 and 9:00 p.m. (i.e., over two weeks). As is common in daily diary research (see
Table 1), 103 participants missed some of the daily surveys (
n = 29), who did not submit their survey questionnaire,
n = 46 who did not show any response after 4 days,
n = 26 who did not submit their responses after one week study, and 11 who did not show responses to some items). More than 40 percent of the 10 diary questionnaires were completed by all participants (1 survey in a day for 10 days as seen in
Table 1). As a result, our final acceptable sample consists of
n = 79 (79 × 10 = 790) people having day-level data see
Table 2. The participants’ ages vary from 21 to 65, with an average age of 35.41 (SD = 7.62) and an average of 8.45 (SD = 94) daily hours worked. The sample’s details and additional descriptions are listed in
Table 2.
3.2. Measurement Scale
The measurement scales used in this study were similar to those used in previous studies. The participants’ responses were collected using four valid and reliable questionnaires: COVID-19 phobia scale, work stress questionnaire, positive mental health questionnaire, burnout questionnaire, and handwashing behavior.
3.2.1. COVID-19 Phobia Scale
The COVID-19 phobia scale (C19P-S) is a 20-item scale that was developed to assess COVID-19 phobia in the general public. Answers are provided on a five-point Likert scale, with 1 representing “strongly disagree,” 2 representing “disagree,” 3 representing “neither agree nor disagree,” 4 representing “agree,” and 5 representing “strongly agree.” The final score is obtained by combining the scores for all 20 items; hence, the total score range is 20–100. Higher scores indicate a higher level of COVID-19 phobia. For this analysis, Cronbach’s alpha value was 0.91 [
22].
3.2.2. Work Stress Questionnaire
This study employed a 21-item work stress scale developed by Frantz & Holmgren [
74]. This 21-item measure is used to assess people’s work-related stress. Cronbach’s alpha is 0.93, and the scale is evaluated on a four-point Likert scale ranging from 1 “yes, always” to 5 “no, never”.
3.2.3. Mental Health
The positive mental health measure was firstly developed by Lukat [
75]. This scale has 9 items, and small adjustments were made to the scale statements to reflect the specific context of mental health. Cronbach’s alpha is 0.91, and all statements are evaluated on a four-point Likert scale ranging from 0 “do not agree” to 3 “agree”.
3.2.4. Burnout
We also used 21-item burnout questionnaires adopted by Malach-Pines (2005) [
76]. This questionnaire measures an individual’s burnout level. Seven-point Likert scale: 1 equals “never,” 2 equals “almost never,” 3 equals “rarely,” 4 equals “sometimes,” 5 equals “often,” 6 equals “very often,” and 7 equals “always”. This scale has high validity and reliability.
3.2.5. Handwashing Frequency
This study utilized the one-item measure to quantify handwashing frequency during the COVID-19 pandemic [
68]. One question was, “On average, how many times did you wash or sanitize your hands every day this week?” The handwashing frequency construct has valid reliability (α = 0.91).
5. Discussion
In light of the growing prevalence of the omicron wave of COVID-19 and digital interaction, this study investigated the role of health care professionals’ modern interaction styles during the omicron wave. This study aims to fill the gap by examining whether current healthcare professionals suffer from mental health issues, COVID-19 phobia, work-related stress, and burnout due to the COVID-19 pandemic. The current research aimed to learn more about the mediating role of burnout and work-related stress between COVID-19 phobia and mental health and consider the moderating impact of handwashing behavior.
Our model demonstrated that COVID-19 phobia significantly negatively impacts mental health, whereas previous research has shown that phobia of illness harms mental function [
82]. Videbeck and Haktanir suggested that phobia regarding objects significantly disturbs mental health. The results supported our hypotheses that COVID-19 phobia impacts burnout of healthcare professionals [
83]. This study confirms the findings of studies [
31,
84] in which it has been theorized that phobia is closely associated with burnout. Our study confirms that phobia of contracting COVID-19 is closely linked with burnout.
This study also found that burnout has an adverse impact on the mental health of healthcare professionals. Burnout is a common occurrence in stressful situations, and it can lead to mental illness during stressful situations such as the COVID-19 pandemic [
85,
86]. Scholars have also proved that burnout can be caused by increasing mental health problems, such as anxiety, work stress, depression, and occupational impairment [
86,
87]. According to the published literature, phobia causes work distress, which is the direct source of burnout. Therefore, previous studies are in line with the current findings [
88,
89].
The results also show that burnout significantly mediates the relationship between COVID-19 phobia and the mental health of healthcare professionals. This finding is consistent with the view of Vignoli, who argued that burnout significantly influences the relationship between phobia and mental illness [
90]. Scholars have documented that burnout is a significant cause of both phobia and mental health problems because burnout is significantly associated with high phobia and high mental problems [
91]. Therefore, burnout acts as a bridge that links COVID-19 phobia to mental health problems. If burnout is ignored between COVID-19 and mental health problems, they may not be able to affect each other directly.
In addition, the results indicated that work-related stress significantly mediates the relationship between COVID-19 phobia and poor mental health. Usually, the researcher claims that work stress is a common symptom of all mental illnesses and situational phobias [
92]. Furthermore, according to the theory of mind, work impairment has a significant effect on arising social phobia and mental health problems [
93]. However, this study indicated that work-related stress significantly mediates the relationship between COVID-19 phobia and mental health. On the other hand, several earlier studies found that work-related stress significantly influenced mental health [
94,
95,
96]. For example, argue that work-related stress mediates the association between COVID-19 -related phobia and mental illness among university students [
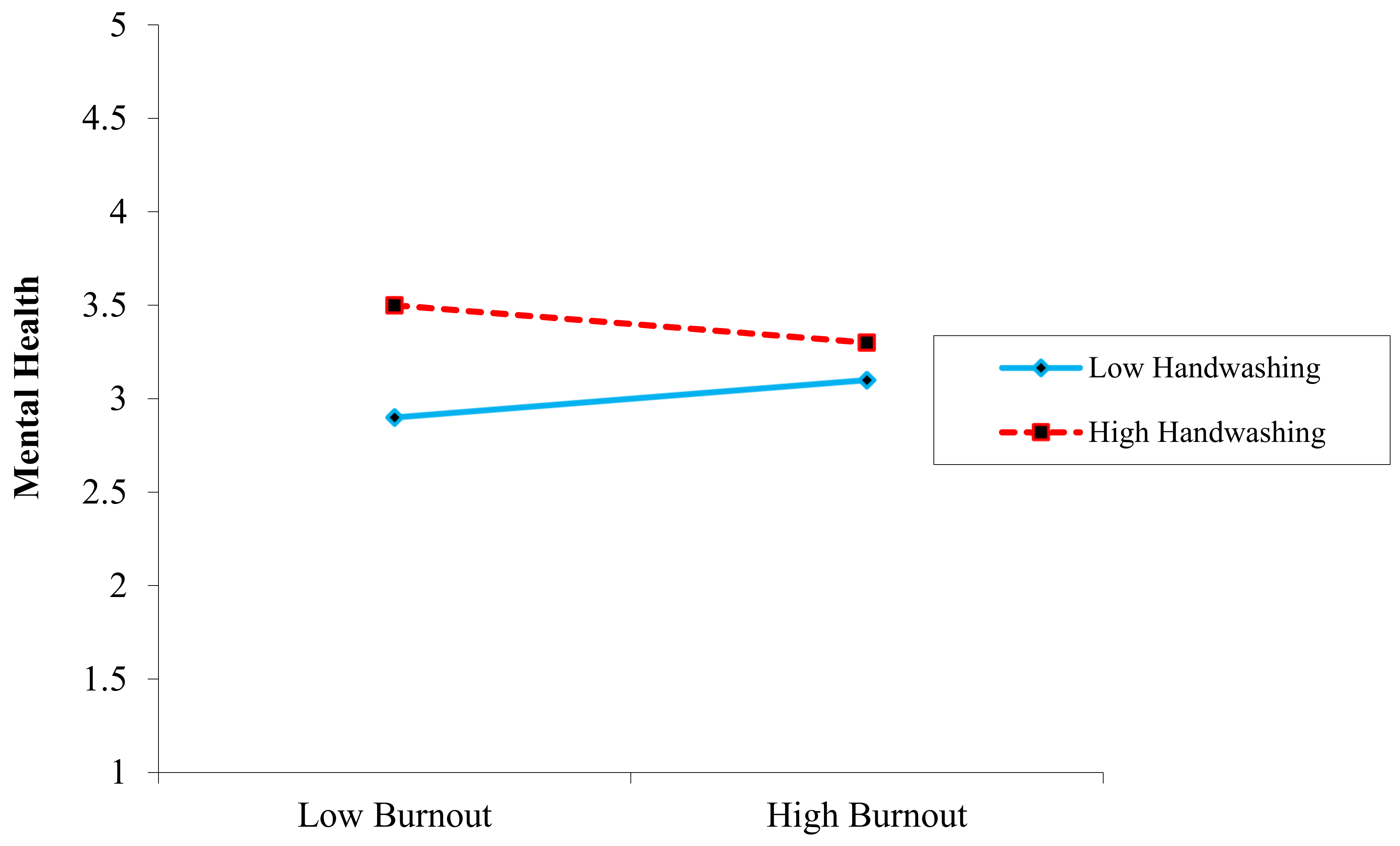
97]. Therefore, our study accepted this hypothesis. This study also found support for the process model showing that the relationship between COVID-19 and mental health as well as burnout and work-related stress are each significant regarding COVID-19 phobia on mental health, as hypothesized. These findings demonstrate that handwashing behavior or attitudinal reactions differ, supporting the coping mechanism of coping theory [
3]. As a result, our research discovered that handwashing behavior did not significantly moderate the relationship between work-related stress and mental health (surprisingly, rejected H7). Still, it did buffer a substantial role in the relationship between burnout and mental health (accepted H8).
5.1. Theoretical Contribution
From a practical aspect, our research speaks volumes about frontline health care experiences during the COVID-19 crisis, particularly in the omicron wave. We were able to capture the experiences of frontline health professionals from the cases of the first omicron wave and thus provide a fundamental understanding of how the situation has impacted healthcare workers’ lives, as well as how they might experience and deal with COVID-19 related phobia situations more broadly. To begin with, it is known that COVID-19 -related phobia has an impact on mental health, burnout, and work-related stress. It is obvious that COVID-19 phobia has consequences for work effectiveness, family engagement, and health status. Our findings also show that, in the face of COVID-19 phobia, problem-focused coping in the form of a simple behavior such as handwashing can help reduce the impact of COVID-19 -related phobia. However, we do not claim that handwashing is a universal coping mechanism that can be used in various phobia situations. Instead, we emphasize the importance of engaging in appropriate coping behaviors that are appropriate for the situation that individuals are dealing with. Handwashing has been widely recommended to combat phobia during the COVID-19 crisis. In other cases, such as when someone has a phobia or fears being laid off, taking active steps to ensure work is completed effectively may help to reduce the impact of the threat or phobia of COVID-19 and work-related stress.
In various aspects, this study added to the coping theory and mental health literature, as well as deleterious mental health variables (phobia, burnout, and work-related stress) in the context of the omicron wave. First, previous research has looked at these variables in distinct COVID-19 contexts [
98,
99]. In past studies, less emphasis was placed on coping behaviors such as handwashing. Such study has been requested because, in both health and organizational contexts, such research is needed to address a gap in the literature and respond to a research demand. Second, this study adds to the existing research on stress and burnout by proposing the idea of COVID-19 phobia and its link to mental health outcomes [
100,
101]. This study supported previous findings regarding coping theory during the omicron wave by providing empirical evidence for handwashing as a boundary condition against the negative effects of COVID-19-related phobia, burnout, and work-related stress [
3].
The outcomes of this study demonstrated a substantial correlation between COVID-19 phobia and mental health during omicron, which is similar to an earlier study that established specific phobia negatively affects an individual’s mental health in a normal context [
102,
103].
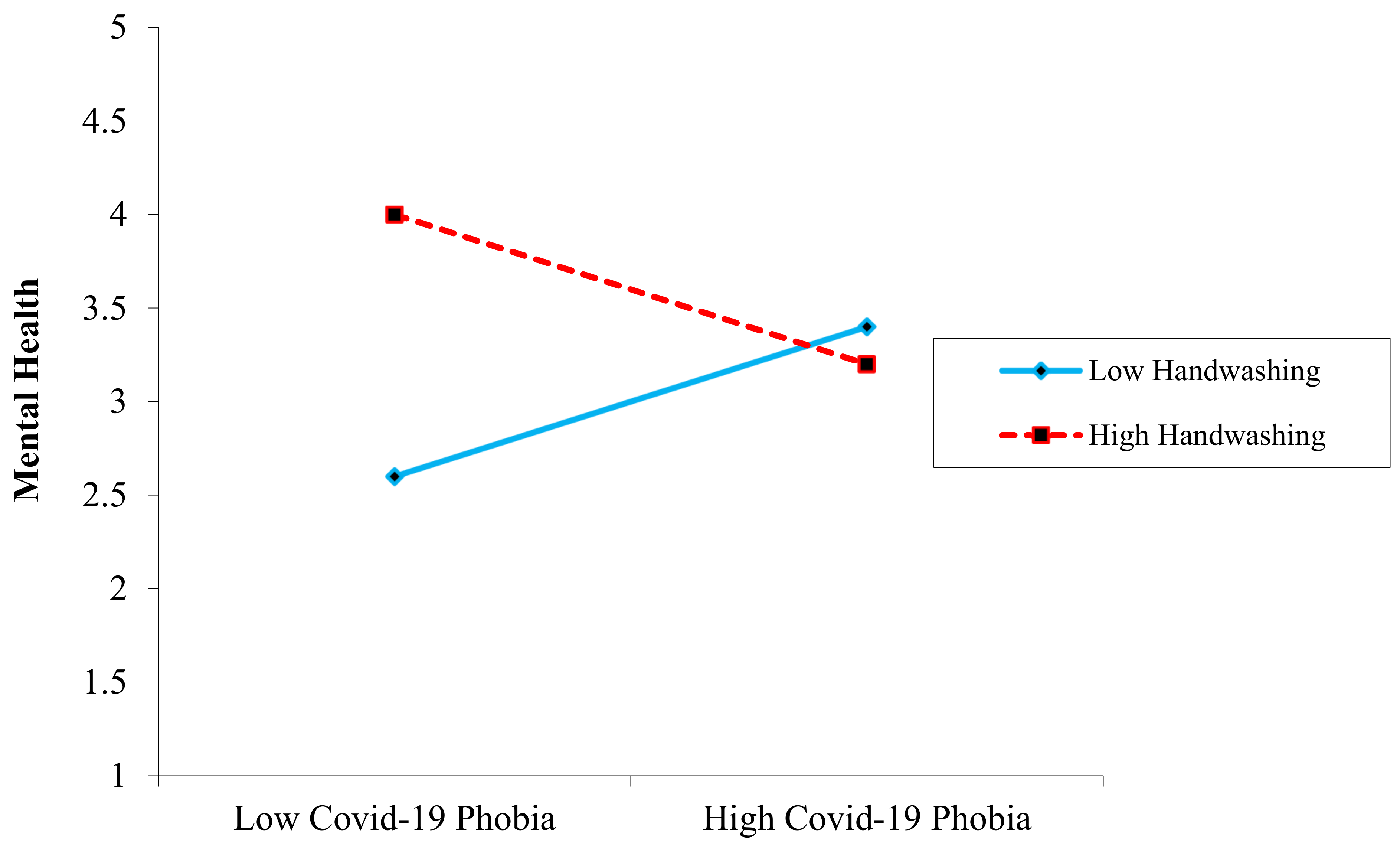
In the H4 and H5 indirect link between COVID-19 phobia and mental health, a mediating effect of burnout usage, as well as work-related stress, were expected, and the results indicated partial mediation. This result or concept is unique in the current literature because COVID-19 phobia is a new concept in psychology. A moderating impact of handwashing was hypothesized in H6, H7, and H8, which indicated that handwashing significantly weakened the link between COVID-19 phobia and mental health, as well as COVID-19 phobia and burnout. The results confirmed these hypotheses. While H8 was rejected because COVID-19 phobia is a novel notion in psychology, this conclusion or concept is unique in the existing literature. COVID-19 phobia has yet to be researched.
5.2. Practical Implications
This research has several practical implications for healthcare professionals that work with COVID-19 patients daily. This research adds to the existing body of knowledge in the following ways. To begin with, there is a rareness of well-designed studies on the links between COVID-19 phobia, burnout, work-related stress, and mental health problems in healthcare workers. We found that COVID-19 phobia and burnout in healthcare practitioners might lead to a rise in mental health issues, which can have significant psychological effects. We investigated the significant role of burnout and work-related stress in mediating the association between COVID-19 phobia and mental health problems.
A crucial requirement for causality is to investigate the directivity and mechanism between the variables. Second, we address a gap in the literature by looking at psychological variables linked to healthcare professionals’ mental health during the omicron wave of COVID-19. We expanded the previous study by involving healthcare professionals, focusing on the effects of COVID-19 on mental health. In terms of practical consequences, the research findings provide critical evidence for the development of COVID-19 phobia treatments aimed at safeguarding healthcare workers’ mental health, improving their quality of life, and making policy recommendations. It is critical to protect healthcare workers’ mental health from infection risks if they are to combat COVID-19 effectively.
Treatments for COVID-19 phobia and mental illnesses can be provided online via social networking sites, allowing for the least amount of direct contact with healthcare providers. Such interventions could aim to (a) support healthcare professionals in maintaining their mental health so that they can continue to provide primary care and health services without experiencing psychological problems during the pandemic, and (b) identify healthcare professionals who may be vulnerable to stressors due to an inability to cope with adversity during a pandemic. In addition to online therapy, psychiatric clinics can be a beneficial way to provide mental health services to healthcare workers actively fighting COVID-19 and exhibiting signs of mental health problems, including anxiety and stress-related illnesses.
The study’s findings are thought to offer insight into the nature of the secondary effects that healthcare professionals will have depending on the epidemic, as well as preventative measures to be employed for the preservation of healthcare workers’ psychological health. Given the fast development of the pandemic around the world, it is hoped that it will aid in the study of the behavioral implications of the emotional condition caused by COVID-19. Today, studies focused on the secondary effects of the outbreak are gaining traction, and comparable research concepts are likely to be developed.
Overall, based on our present research, we conclude that mental health professionals now have a crucial role in improving public wellbeing.
5.3. Limitations and Future Research
First, the data used to complete the proposed study were obtained from Pakistani health professionals; hence, generalization should be made only when a sample population from many nationalities and cultures has been included. This study focuses on health professionals’ relationships with COVID-19 phobia, burnout, work-related stress, and mental health, without going into depth into other elements of health professionals’ lives, such as the bio-socio model. A mediating role of burnout, as well as work-related stress, may be considered for further studies. Furthermore, the moderating role of handwashing behavior may be considered for further investigations.
In addition, the researchers propose that qualitative research utilizing narrative analysis or an interpretive phenomenological method may be used to gather real-world data to support the positivist approach used in this study. The research was only conducted in a relational and cross-sectional environment due to the pandemic’s unfavorable effects. Data were obtained physically, as well as online using the same logic and a more basic sampling technique. These should be taken into account while interpreting study results. The research only included on-the-job healthcare professionals who have not yet been affected. In this context, research involving healthcare workers who have been infected with the virus and have recovered is believed to be necessary. Furthermore, adopting multimethod or mixed methods research in terms of data diversity is thought to produce substantial results in terms of external validity. Furthermore, research focused on cross-national comparisons is believed to yield crucial findings in terms of comprehending the nature of the problem.


 ,
, 


{kind=link}
{kind=link}
{kind=link}