
Three-Dimensional Analysis of the Pulp Chamber and Coronal Tooth of Primary Molars: An In Vitro Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Storage and Group Formation
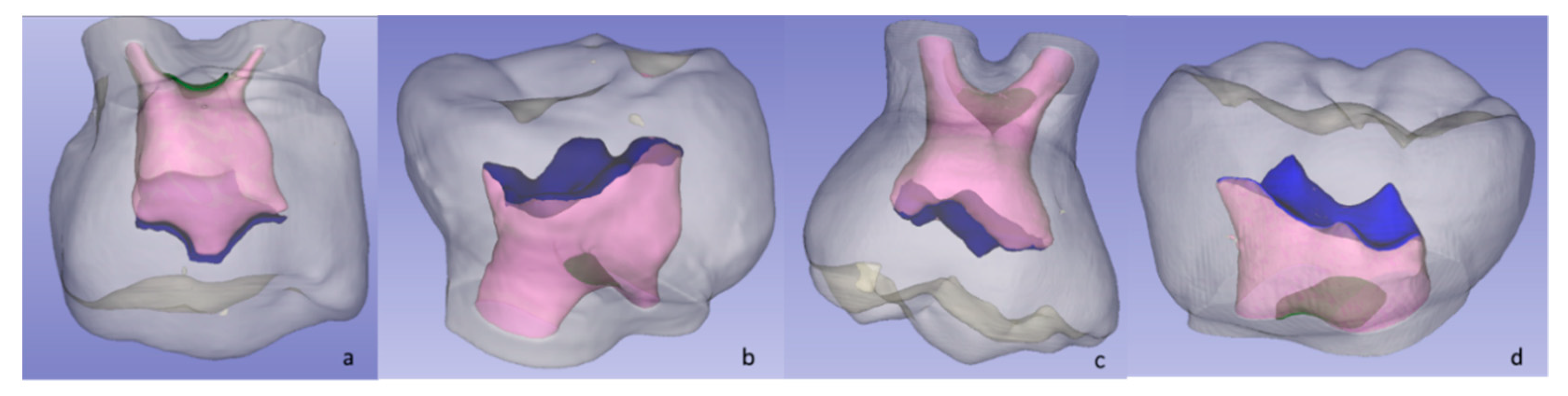
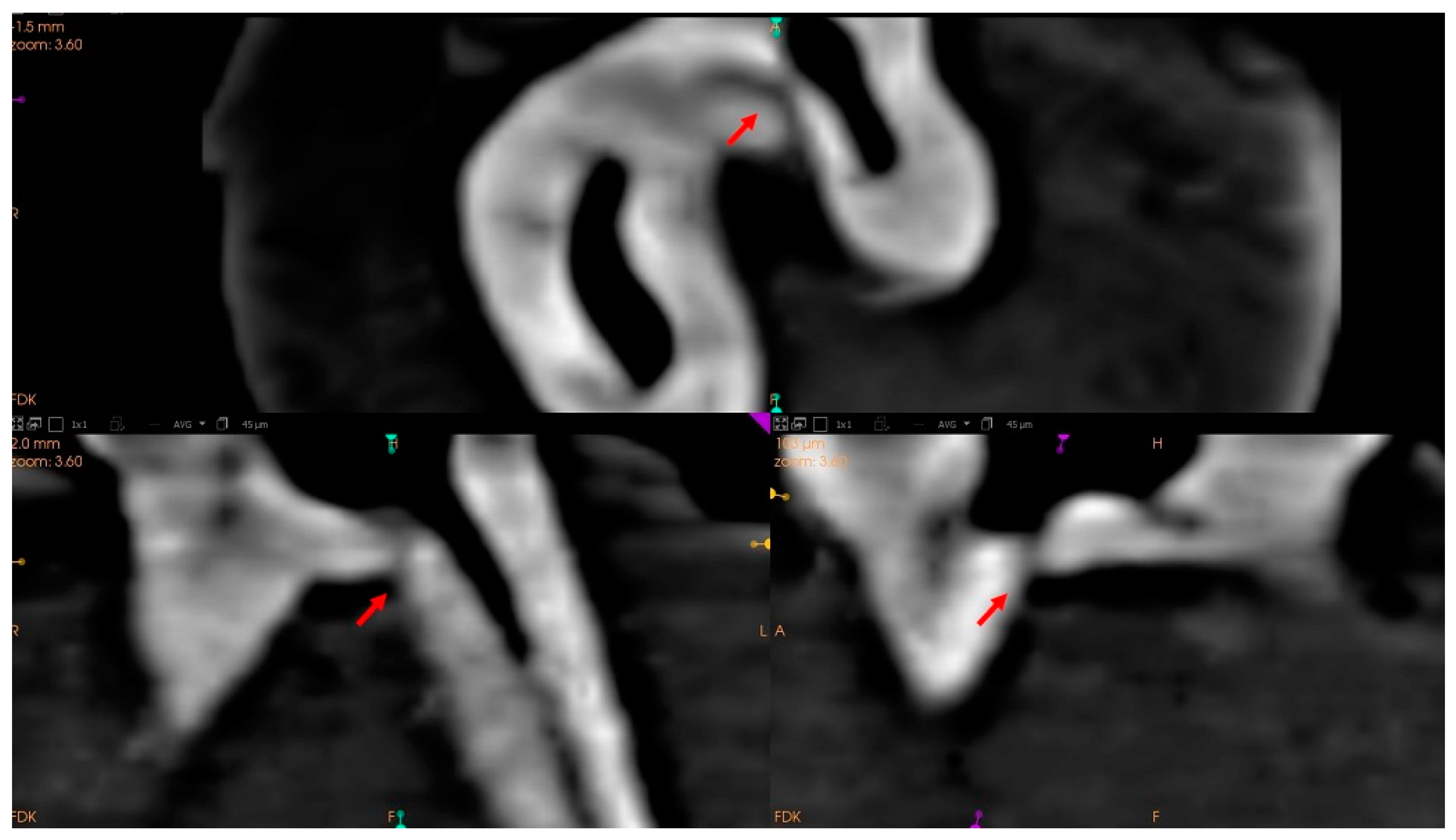
2.3. Image Acquisition and 3D Analysis
2.4. Measurements
2.4.1. Pulp Chamber Roof (PCR) and Pulp Chamber Floor (PCF)
2.4.2. Distance between Pulp Chamber Floor and Furcation (FD)
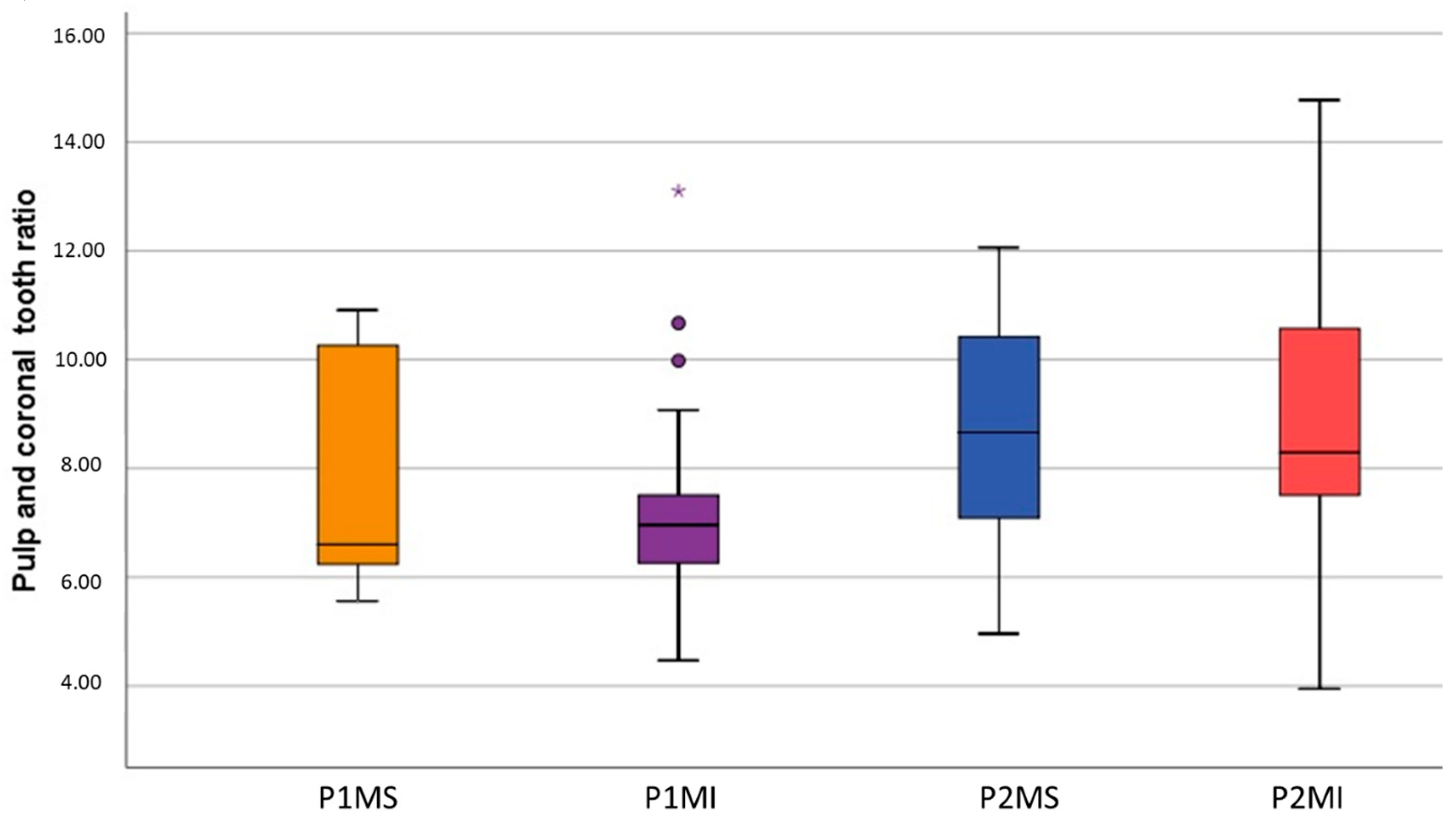
2.4.3. Pulp Chamber Volume (PV), Dental Crown Volume (CV), and Volume Ratio (VR)
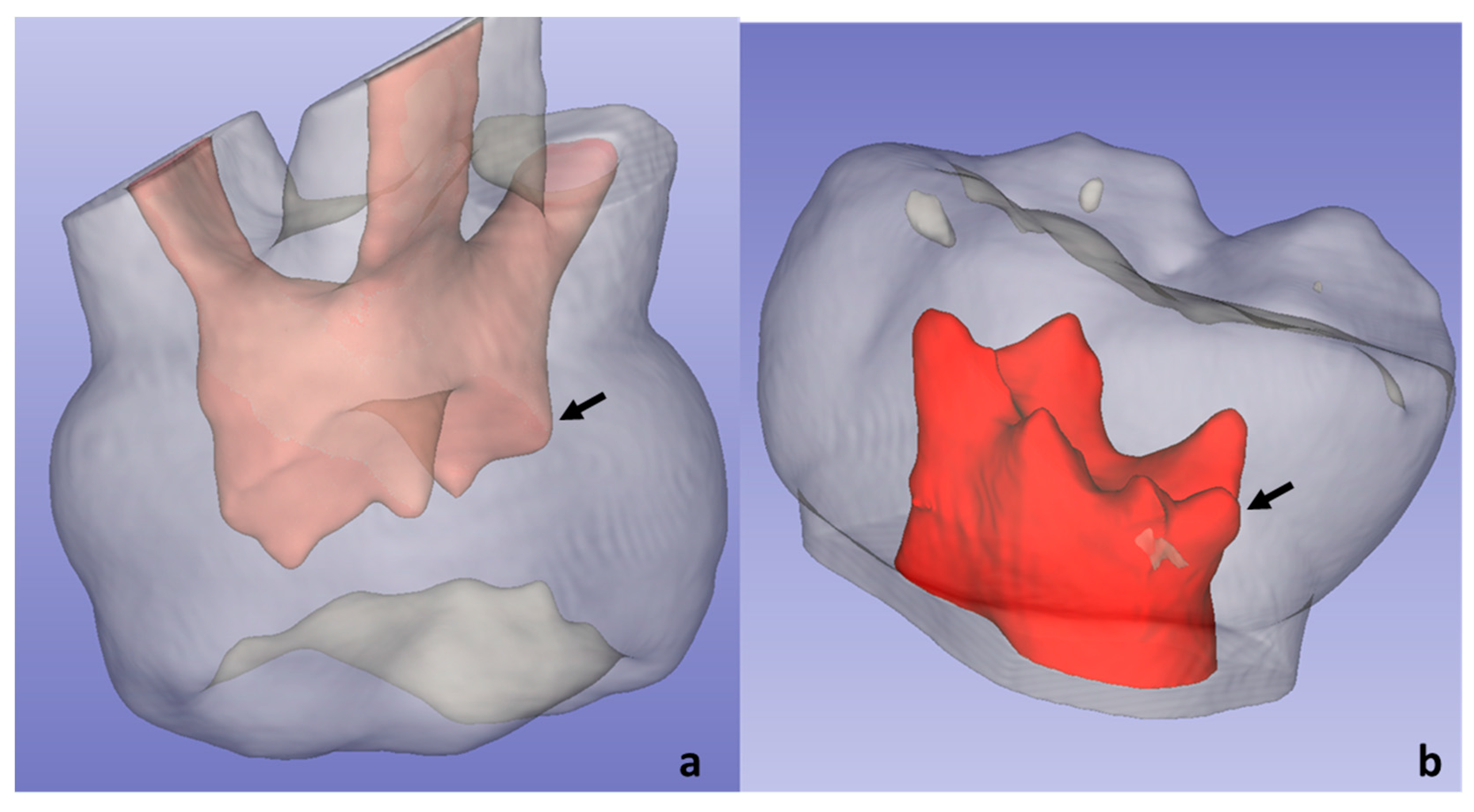
2.4.4. Other Peculiarities
2.5. Calibration, Pilot Test, Internal Validity
2.6. Statistical Analysis
3. Results
Sample Distribution
4. Discussion
4.1. Study Characteristics and Morphometric Analysis
4.2. Pulp Chamber Dimensions
4.3. Furcation Dimensions
4.4. Dental Crown and Pulp Chamber Volume
4.5. Anatomical Peculiarities
4.6. Limitations and Strenghts
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amano, M.; Agematsu, H.; Abe, S.; Usami, A.; Matsunaga, S.; Suto, K.; Ide, Y. Three-dimensional analysis of pulp chambers in maxillary second deciduous molars. J. Dent. 2006, 34, 503–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikari, Y.; Kinoshita, H.; Agematsu, H.; Saka, H.; Matsunaga, S.; Ide, Y.; Abe, S. Three-Dimensional Analysis of Pulp Chambers in Mandibular Second Deciduous Molars. J. Hard Tissue Biol. 2014, 23, 211–216. [Google Scholar] [CrossRef] [Green Version]
- Orhan, A.I.; Orhan, K.; Ozgul, B.M.; Öz, F.T. Analysis of pulp chamber of primary maxillary second molars using 3D micro-CT system: An in vitro study. Eur. J. Paediatr. Dent. 2015, 16, 305–310. [Google Scholar]
- Cheong, J.; Chiam, S.; King, N.M.; Anthonappa, R.P. Pulp Chamber Analysis of Primary Molars Using Micro-Computed Tomography: Preliminary Findings. J. Clin. Pediatr. Dent. 2019, 43, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Agematsu, H.; Ohnishi, M.; Matsunaga, S.; Saka, H.; Nakahara, K.; Ide, Y. Three-dimensional analysis of pulp chambers in mandibular first deciduous molars. Pediatr. Dent. J. 2010, 20, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Baccouche, C.; Ghoul-Mazgar, S.; Baaziz, A.; Said, F.; Salem, K. Ben Topography of the Pulp Chamber in the Maxillary Primary Molars of a Tunisian Children. Indian J. Dent. Res. 2013, 24, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Dabawala, S.; Chacko, V.; Suprabha, B.S.; Rao, A.; Natarajan, S.; Ongole, R. Evaluation of Pulp Chamber Dimensions of Primary Molars from Bitewing Radiographs. Pediatr. Dent. 2015, 37, 361–365. [Google Scholar]
- Khojastepour, L.; Rahimizadeh, N.; Khayat, A. Morphologic Measurements of Anatomic Landmarks in Pulp Chambers of Human First Molars: A Study of Bitewing Radiographs. Iran. Endod. J. 2008, 2, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Selvakumar, H.; Kavitha, S.; Vijayakumar, R.; Eapen, T.; Bharathan, R. Study of Pulp Chamber Morphology of Primary Mandibular Molars using Spiral Computed Tomography. J. Contemp. Dent. Pract. 2014, 15, 726–729. [Google Scholar] [CrossRef]
- Guglielmi, C.A.B.; Ramalho, K.M.; Scaramucci, T.; Da Silva, S.R.E.P.; Imparato, J.C.P.; Pinheiro, S.L. Evaluation of the furcation area permeability of deciduous molars treated by neodymium:yttrium–aluminum–garnet laser or adhesive. Lasers Med. Sci. 2010, 25, 873–880. [Google Scholar] [CrossRef]
- Kramer, P.F.; Júnior, I.M.F.; Meira, R. A SEM investigation of accessory foramina in the furcation areas of primary molars. J. Clin. Pediatr. Dent. 2004, 27, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Lugliè, P.F.; Grabesu, V.; Spano, G.; Lumbau, A.M.I. Accessory foramina in the furcation area of primary molars. A SEM investigation. Eur. J. Paediatr. Dent. 2012, 13, 329–332. [Google Scholar]
- Sharma, U.; Gulati, A.; Gill, N. An investigation of accessory canals in primary molars—An analytical study. Int. J. Paediatr. Dent. 2016, 26, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Palatyńska-Ulatowska, A.; Fernandes, M.C.; Pietrzycka, K.; Koprowicz, A.; Klimek, L.; Souza, R.A.; Pradebon, M.; de Figueiredo, J.A.P. The Pulp Stones: Morphological Analysis in Scanning Electron Microscopy and Spectroscopic Chemical Quantification. Medicina 2022, 58, 5. [Google Scholar] [CrossRef]
- Havale, R.; Rao, D.G.; Latha, A.M.; Nagaraj, M.; Karobari, N.M.; Tharay, N. Coronal pulp: An age biomarker—A cross-sectional radiographic study in children. J. Oral Maxillofac. Pathol. 2020, 24, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Gaurav, V.; Srivastava, N.; Rana, V.; Adlakha, V. A study of root canal morphology of human primary incisors and molars using cone beam computerized tomography: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2013, 31, 254–259. [Google Scholar] [CrossRef]
- Kalaskar, R.; Baliga, S.; Balasubramanian, S. Evaluation of the Average Pulp Cavity Volume of Primary Second Molar and Canine for Obturation of a Single Primary Tooth: A Preliminary Cone-beam Computed Tomographic Study Ritesh. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 79–84. [Google Scholar] [PubMed]
- Mashyakhy, M.; Abu-Melha, A.S. Analysis of Bilateral Symmetry of Root Canal Anatomy in Permanent Dentition: An In Vivo CBCT Study in a Saudi Arabian Population. J. Contemp. Dent. Pract. 2021, 22, 867–875. [Google Scholar]
- Moyaho-Bernal, M.; Carrasco-Gutiérrez, R.; Jiménez-Flores, R.; Juárez-Luna, G.; Pino, G.L.-D.; Mendoza-García, L.; Teutle-Coyotecatl, B. Prevalence of three-rooted primary mandibular first and second molars: Clinical and radiographic findings in a Mexican population. Acta Odontol. Latinoam. 2021, 34, 149–155. [Google Scholar] [CrossRef]
- Nazeer, M.R.; Khan, F.R. Evaluation of the root and canal morphology of mandibular first permanent molars in a sample of Pakistani population by cone-beam computed tomography. J. Pak. Med. Assoc. 2019, 69, 1084–1089. [Google Scholar]
- Ozcan, G.; Sekerci, A.E.; Cantekin, K.; Aydinbelge, M.; Dogan, S. Evaluation of root canal morphology of human primary molars by using CBCT and comprehensive review of the literature. Acta Odontol. Scand. 2016, 74, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, G.; Kocoglu, F.; Sekerci, A.E. C-shaped mandibular primary first molar diagnosed with cone beam computed tomography: A novel case report and literature review of primary molars? root canal systems. J. Indian Soc. Pedod. Prev. Dent. 2016, 34, 397. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Yang, C.; Liu, Y.; Hu, Y.; Zou, J. Evaluate root and canal morphology of primary mandibular second molars in Chinese individuals by using cone-beam computed tomography. J. Formos. Med. Assoc. 2013, 112, 390–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanolli, C.; Bayle, P.; Macchiarelli, R. Proportions Des Tissus et Distribution de l’épaisseur de l’émail Des Molaires Déciduales Humaines Du Début Du Pléistocène Moyen de Tighenif, Algérie. Comptes Rendus Palevol 2010, 9, 341–348. [Google Scholar] [CrossRef]
- Ziya, M.; Yüksel, B.N.; Şari, S. Root Canal Morphology of Mandibular Primary Molars: A Micro-Ct Study. Cumhur. Dent. J. 2019, 22, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Acar, B.; Kamburoğlu, K.K.; Tatar, İ.I.İ.; Arıkan, V.; Çelik, H.H.; Yüksel, S.; Özen, T.; Arikan, V.; Çelik, H.H.; Yüksel, S. Comparison of Micro-Computerized Tomography and Cone-Beam Computerized Tomography in the Detection of Accessory Canals in Primary Molars. Imaging Sci. Dent. 2015, 45, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Neboda, C.; Anthonappa, R.P.; King, N.M. Preliminary investigation of the variations in root canal morphology of hypomineralised second primary molars. Int. J. Paediatr. Dent. 2018, 28, 310–318. [Google Scholar] [CrossRef]
- Wetselaar, P.; Wetselaar-Glas, M.J.M.; Katzer, L.D.; Ahlers, M.O.; Wetselaar-Glas, M.M.J. Diagnosing tooth wear, a new taxonomy based on the revised version of the Tooth Wear Evaluation System (TWES 2.0). J. Oral Rehabil. 2020, 47, 703–712. [Google Scholar] [CrossRef]
- Katge, F.; Wakpanjar, M. Root canal morphology of primary molars by clearing technique: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 151–157. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Bueno, M.R.; Azevedo, B.-C.; Estrela, C.R.A.; Sousa-Neto, M.D.; Estrela, C. Method to identify accessory root canals using a new CBTC Sotwaqre. Braz. Dent. J. 2021, 32, 28–35. [Google Scholar] [CrossRef]
- Barbería, E.; Suárez, M.C.; Villalón, G.; Maroto, M.; García-Godoy, F. Standards for mesiodistal and buccolingual crown size and height of primary molars in a sample of Spanish children. Eur. J. Paediatr. Dent. 2009, 10, 169–175. [Google Scholar]
- Koora, K.; Sriram, C.H.; Muthu, M.S.; Rao, C.; Sivakumar, N. Morphological Characteristics of Primary Dentition in Children of Chennai and Hyderabad. J Indian Soc Pedod Prev Dent 2010, 28, 60–67. [Google Scholar]
- Savara, B.S.; Steen, J.C. Timing and sequence of eruption of permanent teeth in a longitudinal sample of children from Oregon. J. Am. Dent. Assoc. 1978, 97, 209–214. [Google Scholar] [CrossRef]
- Dammaschke, T.; Witt, M.; Ott, K.; Schäfer, E. Scanning electron microscopic investigation of incidence, location, and size of accessory foramina in primary and permanent molars. Quintessence Int. 2004, 35, 699–705. [Google Scholar]
- Wrbas, K.T.; Kielbassa, A.; Hellwig, E. Microscopic studies of accessory canals in primary molar furcations. ASDC J. Dent. Child. 1997, 64, 118–122. [Google Scholar]
- Goto, G.; Zhang, Y. Study of cervical pulp horns in human primary molars. J. Clin. Pediatr. Dent. 1995, 20, 41–44. [Google Scholar]
- Kumar, V.D. A scanning electron microscope study of prevalence of accessory canals on the pulpal floor of deciduous molars. J. Indian Soc. Pedod. Prev. Dent. 2009, 27, 85–89. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tooth | PCR (mm2) | PCF (mm2) | FD (mm) | PV (mm3) | CV (mm3) | VR (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| P1MS | 26.07 | 4.12 | 10.49 | 1.61 | 1.02 | 0.26 | 23.22 | 6.23 | 173.68 | 21.77 | 7.93 | 1.97 |
| P1MI | 28.46 | 5.25 | 8.48 | 1.99 | 0.81 | 0.17 | 26.95 | 6.89 | 183.76 | 20.79 | 7.18 | 1.78 |
| P2MS | 39.31 | 4.06 | 17.34 | 3.61 | 1.22 | 0.27 | 44.43 | 12.64 | 359.90 | 36.59 | 8.68 | 2.25 |
| P2MI | 41.88 | 6.70 | 11.27 | 3.93 | 1.26 | 0.26 | 42.19 | 16.42 | 338.37 | 37.15 | 8.77 | 2.32 |
| p-value * | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.014 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diéguez-Pérez, M.; Ticona-Flores, J.M. Three-Dimensional Analysis of the Pulp Chamber and Coronal Tooth of Primary Molars: An In Vitro Study. Int. J. Environ. Res. Public Health 2022, 19, 9279. https://doi.org/10.3390/ijerph19159279
Diéguez-Pérez M, Ticona-Flores JM. Three-Dimensional Analysis of the Pulp Chamber and Coronal Tooth of Primary Molars: An In Vitro Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9279. https://doi.org/10.3390/ijerph19159279
Chicago/Turabian StyleDiéguez-Pérez, Montserrat, and Jesús Miguel Ticona-Flores. 2022. "Three-Dimensional Analysis of the Pulp Chamber and Coronal Tooth of Primary Molars: An In Vitro Study" International Journal of Environmental Research and Public Health 19, no. 15: 9279. https://doi.org/10.3390/ijerph19159279