Abstract
Human immunodeficiency virus (HIV) is a global health problem, with sexual risk behaviors (SRB) being the main routes of spreading the virus. Evidence indicates that different psychological factors influence SRB (e.g., attitude towards condoms, sexual self-concept, sexual sensation seeking, knowledge of sexual risk behaviors, risk perception). This study proposes an explanatory model of sexual risk behaviors in young people and adults. The sample consisted of 992 young people and adults aged between 18 and 35 years. The model presented good levels of fit (X2 = 3311.433, df = 1471, CFI = 0.964, TLI = 0.959, RMSEA = 0.036), explaining 56% of the variance of sexual activity with multiple partners, 77% of the inadequate use of protective barriers, and 58.8% of sexual activity under the influence of alcohol or drugs from a set of psychological factors in self-report measures. The details of the results offer novel contextual evidence for the prioritization of prevention-oriented psychosocial interventions.
1. Introduction
Human immunodeficiency virus (hereafter, HIV) is a major public health problem, and even though life expectancy has increased following advances in treatments (i.e., antiretroviral therapy) [1], it remains particularly acute in low-income countries [2]. Although the spread of HIV infections has slowed in recent decades, the number of new infections remains alarming, reaching 1.5 million new infections in 2020, concentrated mostly in young people and adults [3,4].
This age focus is attributed to economic, social, and individual factors [5] but mainly to developmental stages where it is more common to have a higher number of sexual partners and to engage in other risky sexual behaviors [6].
Sexual risk behaviors (hereafter, SRB) refer to behaviors that increase the probabilities of the unwanted consequences of sexual activity (e.g., unintended pregnancy, sexually transmitted diseases) [7]. They are the main route of HIV transmission (e.g., [8,9,10]); therefore, to avoid new cases of HIV, it is necessary to prevent high-risk sexual behaviors.
The identified risk behaviors that have evidenced a significant relationship in the literature are the inadequate use of protective barriers, sexual encounters under the influence of alcohol and drugs, and multiple sexual partners [10,11].
The literature has shown different explanatory models of SRBs, such as the planned action theory [12], the health belief model [13], and the protective motivation theory [14]. In particular, these models highlight the relevance of self-efficacy, sexual assertiveness, knowledge, attitudes, and perception of risk and severity, among other variables [15], as associated factors with SRBs [16]. Evidence shows that different safe (e.g., increased condom use) or risky behaviors (e.g., multiple sexual partners; inappropriate condom use) are associated with different psychological factors, including behavioral dispositions or personality traits [17]; ability to identify risky and safe behaviors [18]; perceived vulnerability or risk [19]; sexual self-image [20]; and attitude toward condoms [21]. Specifically, for this study, the following psychological factors were selected.
Attitude toward condoms: an individual’s favorable or unfavorable evaluation of condom use [22]. Attitude toward condom use has frequently been related to SRB [16]; specifically, negative attitudes towards condom use would be an obstacle to the adequate use of protective barriers [18,23], while positive attitudes would increase the likelihood of condom use [24].
Sexual self-concept is people’s thoughts and beliefs that about themselves in the sexual domain [25]. These self-evaluations are associated with sexual risk behaviors [20], showing that when the self-concept is low, there is greater sexual risk-taking, a higher number of sexual partners, and a lower use of condoms [26]. In this direction, it has been suggested that those with a high (higher) self-concept have a greater cognition (awareness) of sexual risk, which translates into a higher number of safe actions [27].
Sexual sensation seeking is a personality trait characterized by a preference for seeking novelty and sexual thrill-seeking experiences to achieve optimal sexual arousal [28]. Evidence suggests that people with higher levels of sexual sensation seeking tend to have a higher number of sexual partners and more permissive attitudes toward sexual encounters [29].
Knowledge of Risky/No-Risky Sexual Behaviors is the degree of information one has about risky behaviors and situations [30]. Evidence suggests that people with a lower ability to identify SRBs are more likely to have sex under the influence of alcohol and without protective barriers [31].
HIV risk perception is the self-perceived likelihood of contracting HIV [32]. Evidence suggests that those who perceive themselves to have a lower HIV risk tend to engage in condomless sex and are likely to have less HIV testing [33].
Given the prevalence that HIV has in the population and the severe consequences it can generate on people’s health [34], multiple research efforts have been conducted to establish effective strategies to prevent SRBs (e.g., [35,36]). Although the variables incorporated in the present study (i.e., attitude towards condoms, sexual self-concept, sexual sensation seeking, knowledge of risky sexual behaviors, risk perception) possess plenty of evidence of their relationship with SRBs, in diverse populations, available studies have been limited to estimate relationships restricted to a smaller number of variables, which prevents an adequate assessment of the joint effects (e.g., [17,37]), especially considering that the independent variables involved can have significant covariation effects (e.g., [38]). This restriction can lead to an overestimation of the effects of the variables studied and, therefore, does not allow adequate prioritization for prevention and intervention programs, with the risk that some of the observed relationships are overestimated or are spurious effects.
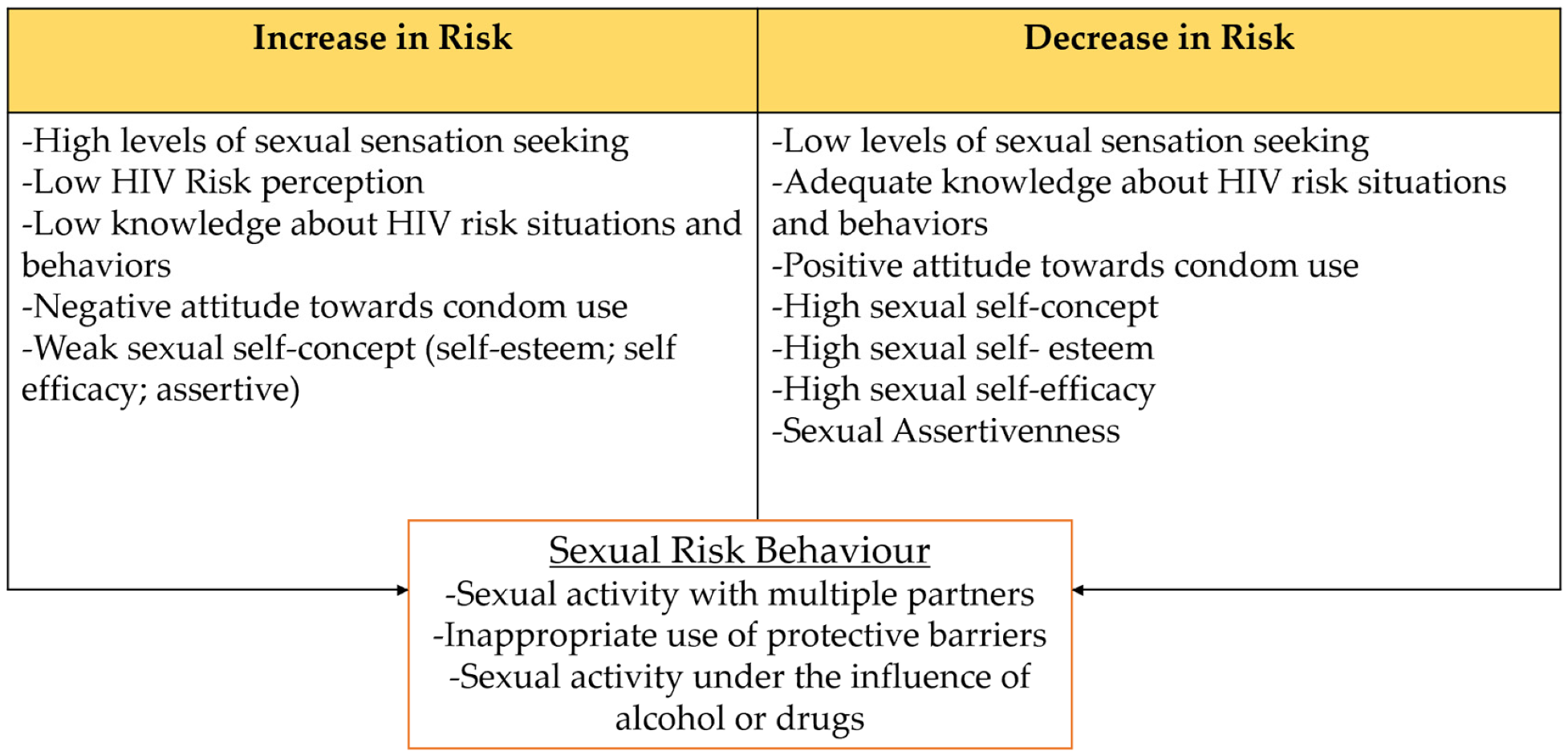
Therefore, the current study proposes an explanatory model (see Figure 1) of sexual risk behaviors in young people and adults by analyzing the combined effects of psychological factors (i.e., attitude towards condoms, sexual self-concept, sexual sensation seeking, knowledge of sexual risk behaviors, risk perception), integrating variables from different explanatory models of social and health psychology, on sexual risk behaviors (i.e., inadequate use of protective barriers, sexual activity under the influence of alcohol and drugs, and multiple sexual partners).
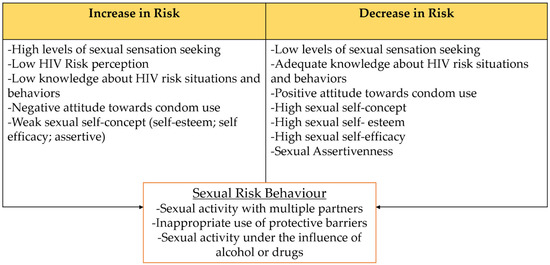
Figure 1.
Theoretical relationships between dimensions of sexual risk behaviors and psychological factors.
2. Materials and Methods
2.1. Design and Participants
Non-experimental cross-sectional study with a correlational scope [39]. Participants were recruited through a non-probabilistic sampling strategy, by quotas [40], considering the main demographic characteristics (city, age, sex, and educational level) according to the reference proportions granted by the results of the CENSO 2017 [41]. The inclusion criteria were to reside in the study cities and to be of legal age (18 years and older for Chile). All individuals who responded to less than 80% of the questionnaire or presented aberrant response patterns (i.e., surveys without variability, where participants selected the same response option in all items) were excluded from the study.
The valid sample was composed of 992 young people and adults between 18 and 35 years of age, 52.4% (n = 514) were women and 47.3% (n = 464) were men, from the five main cities of Norte Grande de Chile: Arica (22.0%; n = 218), Iquique (14.3%; n = 142), Alto Hospicio (9.5%; n = 94), Antofagasta (37.1%; n = 368), and Calama (17.1%; n = 170). Of the total sample, 82.4% (n = 818) identified themselves as heterosexual, 45.0% (n = 447) reported having been tested for HIV/AIDS, and 37.9% (n = 377) reported not having used protective barriers during the last two years. Demographic details are shown in Table 1.

Table 1.
Sociodemographic characteristics of the sample.
2.2. Instruments
Sexual risk behavior scale Haga clic o pulse aquí para escribir texto.: 12-item scale, designed to measure four dimensions of sexual risk behaviors: sexual activity with multiple partners (4 items), inappropriate use of protective barriers (4 items), sexual activity under the influence of alcohol or drugs (4 items), and knowledge of the partner’s sexual record (items = 4). Response options corresponded to behavior/attitude statements in a Likert format of four ordered categories (i.e., 0 = “never” to 3 = “always”), which were conditioned to only report behaviors in the past two years. Higher scores suggest a higher frequency of risky sexual behaviors. The scale showed evidence of validity based on the internal test-retest structure and adequate levels of reliability [42].
Scale of knowledge about HIV risk situations and behaviors Haga clic o pulse aquí para escribir texto.: This 16-item scale measured two dimensions: knowledge about risky behaviors (6 items) and knowledge about non-risky behaviors (10 items). The knowledge scale was composed of behavioral/attitudinal statements. Some referred to sexual behaviors that constitute real transmission risks, and others referred to interactions with people with HIV/AIDS that do not constitute a risk of transmission. The scale scoring constituted a test of optimal performance, assigning a hit (1) when the rating was adequate and a miss (0) when the rating was inadequate. The scale presented evidence of validity based on the test’s internal structure and adequate levels of reliability [43].
Condom Use Attitudes Scale Haga clic o pulse aquí para escribir texto.: 10-item scale which measured the subjective valence of prevention behaviors and the use of protective barriers through three attitudinal dimensions: affective (3 items), behavioral (3 items), and cognitive (4 items). The response options were in a four-category ordered Likert format (i.e., 1 = “Strongly disagree” to 4 = “Strongly agree”). The statements referred to negative attitudes/behaviors toward condom use; therefore, high scores suggest an unfavorable attitude toward condom use. The scale presented evidence of validity based on an internal test–retest structure and adequate levels of reliability [44].
HIV risk perception scale Haga clic o pulse aquí para escribir texto.: 9-item scale designed to measure young adults’ perceived HIV risk through two dimensions: perceived HIV susceptibility (4 items) and perceived HIV severity (5 items). Response options corresponded to behavioral/attitudinal statements in a four-ordered Likert format with differential references for perceived HIV susceptibility (i.e., 0 = “false” to 3 = “true”) and perceived HIV severity (i.e., 0 = “not at all” to 3 = “severely”). Higher scores suggest higher levels of perceived HIV risk. The scale presented evidence of validity based on the internal test structure and adequate levels of reliability [45].
Multidimensional scale of sexual self-concept: 16-item scale designed to measure four dimensions of sexual self-concept: sexual self-esteem (4 items), sexual self-efficacy (4 items), assertive sexual behavior (4 items), and assertive sexual communication (4 items). Response options corresponded to behavioral/attitudinal statements in a Likert format of four ordered categories (1 = “Never” to 4 = “Always”; 1 = “Strongly disagree” to 4 = “Strongly agree”). Higher scores suggest higher levels of sexual self-concept. The scale presented evidence of validity based on the internal structure of the test and satisfactory levels of reliability in all its dimensions [46].
Two-Dimensional Sexual Sensation Seeking Scale: 9-item scale designed to measure sensation seeking in the sexual domain through two dimensions: sexual thrill-seeking (4 items) and tendency to sexual boredom (5 items). Response options corresponded to behavioral/attitudinal statements in a Likert format of four ordered categories (i.e., 0 = “never” to 3 = “always”). Higher scores suggest higher levels of sexual sensation seeking. The scale reported evidence of validity based on the test’s internal structure and adequate levels of reliability [47].
2.3. Procedure
Initially, a total of 20 surveyors were trained in the cities of Arica, Alto Hospicio, Iquique, Antofagasta, and Calama, who invited young people and young adults who passed through the busiest areas of each city to participate voluntarily, explaining the objectives of the study, and inviting them to respond on the spot. The sample collection process was carried out between March and July 2019. Those young people who chose to participate were provided with an informed consent form along with the questionnaire, which established the research objectives, confidentiality, anonymity, and the rights of the participants. Anonymity was safeguarded by returning the questionnaire in a sealed envelope without personal identification. The questionnaires were self-administered in pencil and paper format, the response procedure lasted 15–20 min, and the participants did not receive any reward in return.
The Scientific Ethics Committee of the Universidad de Tarapacá approved this research within the framework of the FONDECYT Initiation Project No. 11170395.
2.4. Data Analysis
Prior to the estimation of the structural equation model (SET-ESEM), the measurement models were tested and debugged through confirmatory factor analysis (CFA) and exploratory structural equation modeling (ESEM) with the WLSMV estimation method, which is robust with non-normal discrete variables [48,49]. Due to the ordinal data structure, the CFA and ESEM were also estimated from the polychoric correlation matrix [50]. Fit was assessed following the cut-point recommendations proposed by Schreiber [51] for the comparative fit index (CFI), Tucker–Lewis index (TLI), and root mean squared error of approximation (RMSEA) (e.g., CFI and TLI > 0.90 is acceptable and >0.95 is satisfactory; RMSEA < 0.08 is acceptable and <0.06 is satisfactory).
Finally, with the debugged measurement models, a SET-ESEM model of direct effects of HIV risk perception, knowledge of HIV risk behaviors, negative attitudes toward condom use, sexual self-efficacy, and sexual sensation seeking (hereafter psychological factors) on sexual risk behaviors were estimated, with covariation among the independent variables restricted only to the dimensions of each measurement model.
The SET-ESEM model was estimated from the polychoric correlation matrix using the WLSMV estimation method. The cut-off points proposed by Schreiber [51] were used for interpretation. Finally, latent variable analyses were performed with Mplus software version 8.2 [52], while descriptive analyses were performed with Jamovi software version 0.9.5.11 [53].
3. Results
Measurement Models
According to the most common fit criteria in the literature (CFI > 0.95, TLI > 0.95 and RMSEA < 0.08) [51], the measurement models evidenced adequate levels of fit, and the details are presented in Table 2.
Table 2.
Global fit of measurements models.
Subsequently, to identify the relationships of the explicative model, a SET-ESEM model was tested. The model presented adequate fit indexes (X2 = 3311.433, df = 1471, CFI = 0.964, TLI = 0.959, RMSEA = 0.036, RMSEA CI 90% = 0.035–0.038), showing it to be an adequate representation of the observed relationships.
According to the standardized effects of the psychological factors on SRB, 19 of the 33 direct effects were statistically significant, with seven mild, five moderate, and seven large effects, according to Cohen’s criteria [54]. The model explained 56% of the variance of sexual activity with multiple partners, 77% of the inadequate use of protective barriers, and 58.8% of sexual activity under the influence of alcohol or drugs. Details of the standardized model effects are presented in Table 3.
Table 3.
Standardized effects of the SET-ESEM model.
In the case of multiplicity of sexual partners, it was observed that the variables risk perception (γ = 0.197, p < 0.000), the affective dimension of attitudes (γ = 0.205, p = 0.001), sexual self-efficacy (γ = 0.444, p =.000), assertive sexual communication (γ = 0.116, p < 0.047) and sexual sensation seeking (γ = 0.578, p < 0.000), showed direct effects, whereas sexual self-esteem (γ = −0.308, p = 0.000) and assertive sexual behavior (γ = −0.162, p = 0.002), showed inverse effects.
Regarding the inadequate use of protective barriers, it was observed that risk perception (γ = 0.160, p < 0.000), the behavioral dimension of negative attitudes towards condom use (γ = 0.780, p < 0.000), assertive sexual communication (γ = 0.214, p < 0.000), and sexual sensation seeking (γ = 0.375, p < 0.000) presented direct effects, while knowledge about risky (γ = −0.102, p < 0.000) and risk-free (γ = −0.356, p < 0.000) behaviors, together with the cognitive dimension of negative attitudes toward condom use (γ = −0.356, p = 0.000) showed inverse effects.
Finally, in the case of sexual activity under the influence of alcohol and/or drugs, it was shown that the affective dimension of negative attitudes towards condom use (γ = 0.169, p = 0.006), sexual self-efficacy (γ = 0.295, p = 0.000), and sexual sensation seeking (γ = 0.666, p < 0.000) had direct effects, whereas the sexual self-esteem variable showed an inverse effect (γ = −0.238, p = 0.000).
4. Discussion
This study aimed to propose an explanatory model of sexual risk behaviors (i.e., inappropriate use of protective barriers, sexual activity under the influence of alcohol and drugs, and multiple sexual partners) in young people and adults due to the joint effects of psychological factors (i.e., attitude towards the use of condoms, sexual self-concept, sexual sensation seeking, knowledge of sexual risky/non-risky behaviors, and risk perception). From a statistical point of view, the proposed model seems to be a sufficient representation of the population based on the covariations observed in the sample. Therefore, it can be considered a plausible explanation for self-reported risky sexual behaviors.
In addition, the relationships showed similarities with the model based on the literature (see Figure 1), although with some exceptions. In this sense, it was observed that although knowledge is commonly indicated as a protective factor [55], the effects observed in this research were minor. In the same way, even though the perception of risk is conceptualized as one of the highly related components associated with preventive action [56], only slight effects or even the absence of evidence of population effects were shown in this research. These results are particularly interesting since the prevention programs carried out in the study country are focused on prevention information and risk perception [57], which could be insufficient in light of these results.
These results can be explained, to some extent, by interaction effects not included in this study; for example, the authors of [58] stated that the relationship between knowledge and risky sexual behaviors hinges on the perception of risk and that knowledge per se would not affect these practices.
Therefore, although both variables can be considered a necessary condition for decision making, the results in this study reflect the need to diversify the preventive actions beyond information campaigns or focused on increasing risk perceptions. These actions could include, for example, variables such as self-perception of the individuals about their sexuality, the perception of their abilities, their communication skills, and assertive sexual behavior, as well as personality changes associated with the search for sexual emotions.
However, in the results, a particular case was observed and was apparently contradictory since the cognitive dimension of attitudes presented an inverse relationship with the inadequate use of protective barriers, which is far from what is commonly found in the literature, where attitude is usually pointed out as one of the variables with the highest incidence when explaining the intention or use of condoms [23,59]. Nonetheless, after a detailed analysis of the items (i.e., “I think condoms should only be used by promiscuous people; The use of condoms is only for one-night stands”; “I think condoms are unnecessary in healthy people”; “I think that suggesting the use of condoms generates mistrust”), we believe that this discrepancy is attributable to methodological limitations of the scale used since the items could be reflecting conservative positions, rather than a general cognitive assessment towards condom use.
Finally, it is imperative to mention that this study has some limitations that must be considered. The first of these limitations is the impossibility of inferring causality, given that it was a cross-sectional study with a correlational scope; therefore, the results should be considered as an initial approximation. A second restriction is the non-probabilistic nature of the sample, which reduces the possibility of generalizing based on these findings. A third element to consider is that all the variables were measured with Likert-type, self-report, pencil, and paper scales; for this reason, the total explained variance is expected to be slightly overestimated, given the possible common fluctuation of the method. In addition, it is necessary to recognize a series of individual, economic, social, and cultural elements or factors that have not been included in the model and may have some effect on sexual risk behaviors [24].
Despite these observations, the results of this study, while providing support for most of the relationships reported in the literature between psychological factors (e.g., attitude toward condoms, sexual self-concept, sexual sensation seeking) and sexual risk behaviors, draw attention to the emphasis commonly given to some of them. Therefore, these findings emphasize the need to incorporate other psychological and behavioral variables in the study of factors that reduce sexual risk behaviors and invite the incorporation of uncommon variables (e.g., personality traits and self-assessment of their capabilities) in the different actions of health promotion and the prevention of risk behaviors in intervention strategies.
5. Conclusions
The results support the explanatory role of the joint effects of some psychological factors widely used in health intervention models model of risky sexual behaviors (i.e., inadequate use of protective barriers, sexual encounters under the influence of alcohol and drugs, and multiple sexual partners), in youth and young adults in northern Chile. In addition, it was shown that sexual self-concept and sexual sensation seeking are variables that notably increased the prediction power of the model, given their influence on the manifestation of sexual risk behaviors.
Author Contributions
Conceptualization, R.F.-U. and G.S.-P.; methodology, P.M.-C.; software, P.M.-C.; validation, R.F.-U. and G.S.-P.; formal analysis, P.M.-C.; investigation, R.F.-U.; resources, R.F.-U.; data curation, G.S.-P. and P.M.-C.; writing—original draft preparation, G.S.-P.; writing—review and editing, R.F.-U.; visualization, M.H.; supervision, M.H.; project administration, R.F.-U.; funding acquisition, R.F.-U. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by ANID (National Agency for Research and Development), grant number 11170395 FONDECYT de iniciación.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Universidad de Tarapacá (protocol code n°29-2017, 22 November 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Riddell, J., IV; Amico, K.R.; Mayer, K.H. HIV Preexposure Prophylaxis: A Review. JAMA 2018, 319, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- World Health Organizatión WHO. Global Health Sector Strategy on HIV 2016–2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/246178/WHO?sequence=1 (accessed on 8 May 2022).
- World Health Organization (WHO). Key Facts HIV [Internet]. 2020. Available online: https://cdn.who.int/media/docs/default-source/hq-hiv-hepatitis-and-stis-library/key-facts-hiv-2020.pdf?sfvrsn=582c3f6e_13 (accessed on 8 May 2022).
- Centers for Disease Control and Prevention. Estimated HIV Incidence and Prevalence in the United States, 2015–2019. 2021. Available online: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. (accessed on 10 June 2022).
- World Health Organization (WHO). Sexual Health and Its Linkages to Reproductive Health: An Operational Approach. 2017. Available online: https://apps.who.int/iris/handle/10665/258738 (accessed on 10 June 2022).
- Darteh, E.K.M.; Dickson, K.S.; Amu, H. Understanding the Socio-demographic Factors Surrounding Young Peoples’ Risky Sexual Behaviour in Ghana and Kenya. J. Community Health 2020, 45, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Pawlowsky-Glahn, V.; Egozcue, J.J.; Planes-Pedra, M.; Pawlowsky-Glahn, V.; Egozcue, J.J.; Planes-Pedra, M. Survey Data on Perceptions of Contraceptive Methods as Compositional Tables. Rev. Latinoam. Psicol. 2018, 50, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; Zhang, L.; Luo, H.; Rong, W.; Meng, X.; Yu, H.; Tan, X. Factors associated with risk sexual behaviours of HIV/STDs infection among university students in Henan, China: A cross-sectional study. Reprod. Health 2021, 18, 172. [Google Scholar] [CrossRef]
- Gómez-Melasio, D.A.; Onofre-Rodríguez, D.J.; Benavides-Torres, R.A.; Trujillo-Hernández, P.E. A Systematic Review of Individual, Psychological and Sociocultural Factors Associated with Safe and Risky Sexual Behavior in Older Adults. Am. J. Sex. Educ. 2021, 16, 415–434. [Google Scholar] [CrossRef]
- Fetene, N.; Mekonnen, W. The prevalence of risky sexual behaviors among youth center reproductive health clinics users and non-users in Addis Ababa, Ethiopia: A comparative cross-sectional study. PLoS ONE 2018, 13, e0198657. [Google Scholar] [CrossRef]
- Srahbzu, M.; Tirfeneh, E. Risky Sexual Behavior and Associated Factors among Adolescents Aged 15–19 Years at Governmental High Schools in Aksum Town, Tigray, Ethiopia, 2019: An Institution-Based, Cross-Sectional Study. BioMed Res. Int. 2020, 2020, 3719845. [Google Scholar] [CrossRef]
- Ajzen, I. From Intentions to Actions: A Theory of Planned Behavior. In Action-Control: From Cognition to Behavior; Kuhl, J., Beckmann, J., Eds.; Springer: New York, NY, USA, 1985; pp. 11–39. [Google Scholar]
- Becker, M.H.; Maiman, L.A. Sociobehavioral determinants of compliance with health and medical care recommendations. Med. Care 1975, 13, 10–24. [Google Scholar] [CrossRef]
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change1. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef]
- Morell-Mengual, V.; Gil-Llario, M.; Ruiz-Palomino, E.; Castro-Calvo, J.; Ballester-Arnal, R. Factors Associated with Condom Use in Vaginal Intercourse Among Spanish Heterosexual and Bisexual Men. Sex Res. Soc. Policy 2022, 1–11. [Google Scholar] [CrossRef]
- Lawal, A.M.; Olley, B.O. Psychosocial factors predicting risky sexual behaviour among long distance truck drivers in Lagos, Nigeria. SAHARA-J. 2017, 14, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Morell-Mengual, V.; Gil-Llario, M.D.; Fernádez-García, O.; Ballester-Arnal, R. Factors Associated with Condom Use in Anal Intercourse Among Spanish Men Who Have Sex with Men: Proposal for an Explanatory Model. AIDS Behav. 2021, 25, 3836–3845. [Google Scholar] [CrossRef]
- Keto, T.; Tilahun, A.; Mamo, A. Knowledge, attitude and practice towards risky sexual behaviors among secondary and preparatory students of Metu town, south western Ethiopia. BMC Public Health 2020, 20, 1394. [Google Scholar] [CrossRef]
- Haile, Z.; Kingori, C.; Darlington, K.A.; Basta, T.; Chavan, B. HIV Risk Perception Among College Students at a University in the Midwest. Sex. Cult. 2017, 21, 62–73. [Google Scholar] [CrossRef]
- Arsandaux, J.; Montagni, I.; Macalli, M.; Bouteloup, V.; Tzourio, C.; Galéra, C. Health Risk Behaviors and Self-Esteem Among College Students: Systematic Review of Quantitative Studies. Int. J. Behav. Med. 2020, 27, 142–159. [Google Scholar] [CrossRef]
- Ha, T.; Schensul, S.L.; Schensul, J.J.; Nguyen, T.; Nguyen, N. Sexual Risk Behaviors, HIV Prevalence and Access to Reproductive Health Services Among Young Women Migrant Workers in the Industrial Zones in Vietnam. Front. Reprod. Health. 2021, 3, 88. Available online: https://www.frontiersin.org/article/10.3389/frph.2021.775375 (accessed on 3 May 2022). [CrossRef]
- Sheeran, P.; Abraham, C.; Orbell, S. Psychosocial correlates of heterosexual condom use: A meta-analysis. Psychol Bull. 1999, 125, 90132. [Google Scholar] [CrossRef]
- Choi, S.K.; LeGrand, S.; Dong, W.; Muessig, K.E.; Hightow-Weidman, L. Condom use intentions mediate the relationships between psychosocial constructs and HIV sexual risk behavior in young Black men who have sex with men. AIDS Care 2019, 31, 5360. [Google Scholar] [CrossRef]
- Parajuli, B.; Adhikari, C.; Tripathi, N. Determinants of condom use during last sexual intercourse among male college youth of Kaski, Nepal: A cross-sectional survey. PLoS ONE 2022, 16, e0261501. [Google Scholar] [CrossRef]
- McBride Murry, V.; Brody, G.H.; McNair, L.D.; Luo, Z.; Gibbons, F.X.; Gerrard, M.; Wills, T.A. Parental Involvement Promotes Rural African American Youths’ Self-Pride and Sexual Self-Concepts. J. Marriage Fam. 2005, 67, 627–642. [Google Scholar] [CrossRef]
- Potard, C.; Lancelot, C.; Courtois, R. Examining relationships between sexual risk–safety behaviors and physical self-concept by gender: A cluster analytical approach. Emerg. Adulthood 2019, 7, 3144. [Google Scholar] [CrossRef]
- Lou, J.H.; Chen, S.H.; Li, R.H.; Yu, H.Y. Relationships among sexual self-concept, sexual risk cognition and sexual communication in adolescents: A structural equation model. J. Clin. Nurs. 2011, 20, 1696704. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Johnson, J.R.; Adair, V.; Rompa, D.; Multhauf, K.; Kelly, J.A. Sexual Sensation Seeking: Scale Development and Predicting AIDS-Risk Behavior Among Homosexually Active Men. J. Pers. Assess. 1994, 62, 385–397. [Google Scholar] [CrossRef]
- Curry, I.; Luk, J.W.; Trim, R.S.; Hopfer, C.J.; Hewitt, J.K.; Stallings, M.C.; Brown, S.A.; Wall, T.L. Impulsivity Dimensions and Risky Sex Behaviors in an At-Risk Young Adult Sample. Arch. Sex. Behav. 2018, 47, 52936. [Google Scholar] [CrossRef]
- Hollar, D.S.; Snizek, W.E. The influences of knowledge of HIV/AIDS and self-esteem on the sexual practices of college students. Soc. Behav. Personal. Int. J. 1996, 24, 7586. [Google Scholar] [CrossRef]
- Kadengye, D.T.; Dalal, S. Social intolerance, risky sexual behaviors and their association with HIV knowledge among Ugandan adults: Results from a national survey. AIDS Care 2019, 31, 2504. [Google Scholar] [CrossRef]
- Macintyre, K.; Rutenberg, N.; Brown, L.; Karim, A. Understanding Perceptions of HIV Risk Among Adolescents in KwaZulu-Natal. AIDS Behav. 2004, 8, 237–250. [Google Scholar] [CrossRef]
- Goldenberg, T.; Finneran, C.; Sullivan, S.P.; Andes, K.L.; Stephenson, R. “I consider being gay a very high risk factor”: How Perceptions of a Partner’s Sexual Identity Influence Perceptions of HIV Risk Among Gay and Bisexual Men. Sex Res. Soc. Policy 2017, 14, 3241. [Google Scholar] [CrossRef]
- Remien, R.H.; Stirratt, M.J.; Nguyen, N.; Robbins, R.N.; Pala, A.N.; Mellins, C.A. Mental health and HIV/AIDS: The need for an integrated response. AIDS 2019, 33, 141120. Available online: https://pubmed.ncbi.nlm.nih.gov/30950883 (accessed on 3 May 2022). [CrossRef]
- Dave, S.; Peter, T.; Fogarty, C.; Karatzas, N.; Belinsky, N.; Pant Pai, N. Which community-based HIV initiatives are effective in achieving UNAIDS 90-90-90 targets? A systematic review and metaanalysis of evidence (2007–2018). PLoS ONE 2019, 7, e0219826. [Google Scholar] [CrossRef] [Green Version]
- Restar, A.; Nguyen, M.; Nguyen, K.; Adia, A.; Nazareno, J.; Yoshioka, E.; Hernandez, L.; Operario, D. Trends and emerging directions in HIV risk and prevention research in the Philippines: A systematic review of the literature. PLoS ONE 2018, 5, e0207663. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Yan, H.; Duan, Z.; Yang, H.; Li, X.; Ding, C.; Deng, S.; Li, S. Relationship between sexual sensation seeking and condom use among young men who have sex with men in China: Testing a moderated mediation model. AIDS Care 2021, 33, 9149. [Google Scholar] [CrossRef] [PubMed]
- Khezri, M.; Farokhzadian, J.; Nematollahi, M.; Foroughameri, G.; Sharifi, H. HIV/AIDS prevention education: An effective tool for enhancing street children’s knowledge and attitude. A randomized controlled trial. Child. Youth Serv. Rev. 2019, 104, 104351. [Google Scholar] [CrossRef]
- Ato, M.; López-García, J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. Anal. Psicol. 2013, 27, 14259. [Google Scholar] [CrossRef] [Green Version]
- Otzen, T.; Manterola, C. Técnicas de Muestreo sobre una Población a Estudio. Int. J. Morphol. 2017, 35, 22732. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadísticas. Síntesis de Resultados Censo 2017. 2018. Available online: http://www.censo2017.cl/descargas/home/sintesis-de-resultados-censo2017.pdf (accessed on 13 June 2022).
- Ferrer-Urbina, R.; Leal-Soto, F.; Bravo, N.; Huaranca, C.; Perez, J.; Salinas, T. Scale of Risk Behaviors, Associated with STI/HIV-AIDS, For Young Chileans. Eur. Proc. Soc. Behav. Sci. 2019, 60, 800–809. [Google Scholar] [CrossRef]
- Sepúlveda-Páez, G.; Mena-Chamorro, P.; Ferrer-Urbina, R. Desarrollo de una Escala para Valorar Conocimiento sobre Situaciones y Conductas de Riesgo de Contagio de VIH, en Jóvenes y Adultos Jóvenes en un Contexto Latinoamericano. RIDEP 2021, 60, 157167. [Google Scholar] [CrossRef]
- Ferrer-Urbina, R.; Mena-Chamorro, P.; Sepúlveda-Páez, G.; Carmona-Halty, M. Development and Evidence of the Validity of the Condom Use Attitudes Scale for Youth and Adults in a Chilean Context. Front. Psychol. 2021, 12, 727499. Available online: https://www.frontiersin.org/article/10.3389/fpsyg.2021.727499 (accessed on 15 March 2022). [CrossRef]
- Mena-Chamorro, P.; Ferrer-Urbina, R.; Sepúlveda-Páez, G.; Cortés-Mercado, F.; Gutierrez-Mamani, C.; Lagos-Maldonado, K.; Peña-Daldo, M. Development and evidence of validity of the HIV risk perception scale for young adults in a Hispanic-American context. PLoS ONE 2020, 15, 0231558. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-Urbina, R.; Sepúlveda-Páez, G.; Henríquez, D.T.; Acevedo-Castillo, D.I.; Llewellyn-Alvarado, D.A. Development and validity evidence of the multidimensional scale of sexual self-concept in a Spanish-speaking context. Psicol. Refl. Crít. 2019, 32, 22. [Google Scholar] [CrossRef]
- Ferrer-Urbina, R.; Mena-Chamorro, P.; Zambrana, P.; Ramírez, C. Development and validity evidence of the Two-Dimensional Sexual Sensation Seeking Scale. Rev. Latin. Psic. 2020, 52, 17683. [Google Scholar] [CrossRef]
- Li, C.H. Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav Res. 2016, 48, 936949. [Google Scholar] [CrossRef] [Green Version]
- DiStefano, C.; Morgan, G.B. A Comparison of Diagonal Weighted Least Squares Robust Estimation Techniques for Ordinal Data. Struct. Equ. Modeling Multidis. J. 2014, 21, 425–438. [Google Scholar] [CrossRef]
- Barendse, M.T.; Oort, F.J.; Timmerman, M.E. Using Exploratory Factor Analysis to Determine the Dimensionality of Discrete Responses. Struct. Equ. Modeling Multidis. J. 2015, 22, 87101. [Google Scholar] [CrossRef]
- Schreiber, J.B. Update to core reporting practices in structural equation modeling. Res. Soc. Administ. Pharm. 2017, 13, 63443. [Google Scholar] [CrossRef]
- Muthén, L.; Muthén, B. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- The Jamovi Project. Jamovi. (Version 2.2) [Computer Software]. Available online: https://www.jamovi.org (accessed on 12 July 2022).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Oxfordshire, UK, 1988. [Google Scholar]
- Boti, N.; Hussen, S.; Shegaze, M.; Shibru, S.; Shibiru, T.; Zerihun, E.; Godana, W.; Abebe, S.; Gebretsadik, W.; Desalegn, N.; et al. Effects of comprehensive sexuality education on the comprehensive knowledge and attitude to condom use among first-year students in Arba Minch University: A quasi-experimental study. BMC Res. Notes 2019, 12, 700. [Google Scholar] [CrossRef] [Green Version]
- Kiviniemi, M.T.; Orom, H.; Waters, E.A.; McKillip, M.; Hay, J.L. Education-based disparities in knowledge of novel health risks: The case of knowledge gaps in HIV risk perceptions. Br. J. Health Psychol. 2018, 23, 42035. [Google Scholar] [CrossRef]
- Ministerio de Educación. Educación Sexual, Estrategia en sexualidad afectividad y género. Available online: http://mileschile.cl/cms/wp-content/uploads/2019/01/Estrateg%C3%ADa-en-educaci%C3%B3n-sexual-MINEDUC-2018.pdf (accessed on 12 July 2022).
- Noroozinejad, G.; Yarmohamadi, M.; Bazrafkan, F.; Sehat, M.; Rezazadeh, M.; Ahmadi, K. Perceived Risk Modifies the Effect of HIV Knowledge on Sexual Risk Behaviors. Front. Public Health 2013, 1, 15. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Correa, P.; Ramírez-Santana, M. Predicting Condom Use among Undergraduate Students Based on the Theory of Planned Behaviour, Coquimbo, Chile, 2016. Int. J. Environ. Res. Public Health 2018, 15, 1689. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).