
Validation of the Muscle Dysmorphic Disorder Inventory (MDDI) among Italian Women Practicing Bodybuilding and Powerlifting and in Women Practicing Physical Exercise

 ,
, 
 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Main Sample
2.3. Retest Sample
2.4. Measures
2.5. Analytic Strategy
3. Results
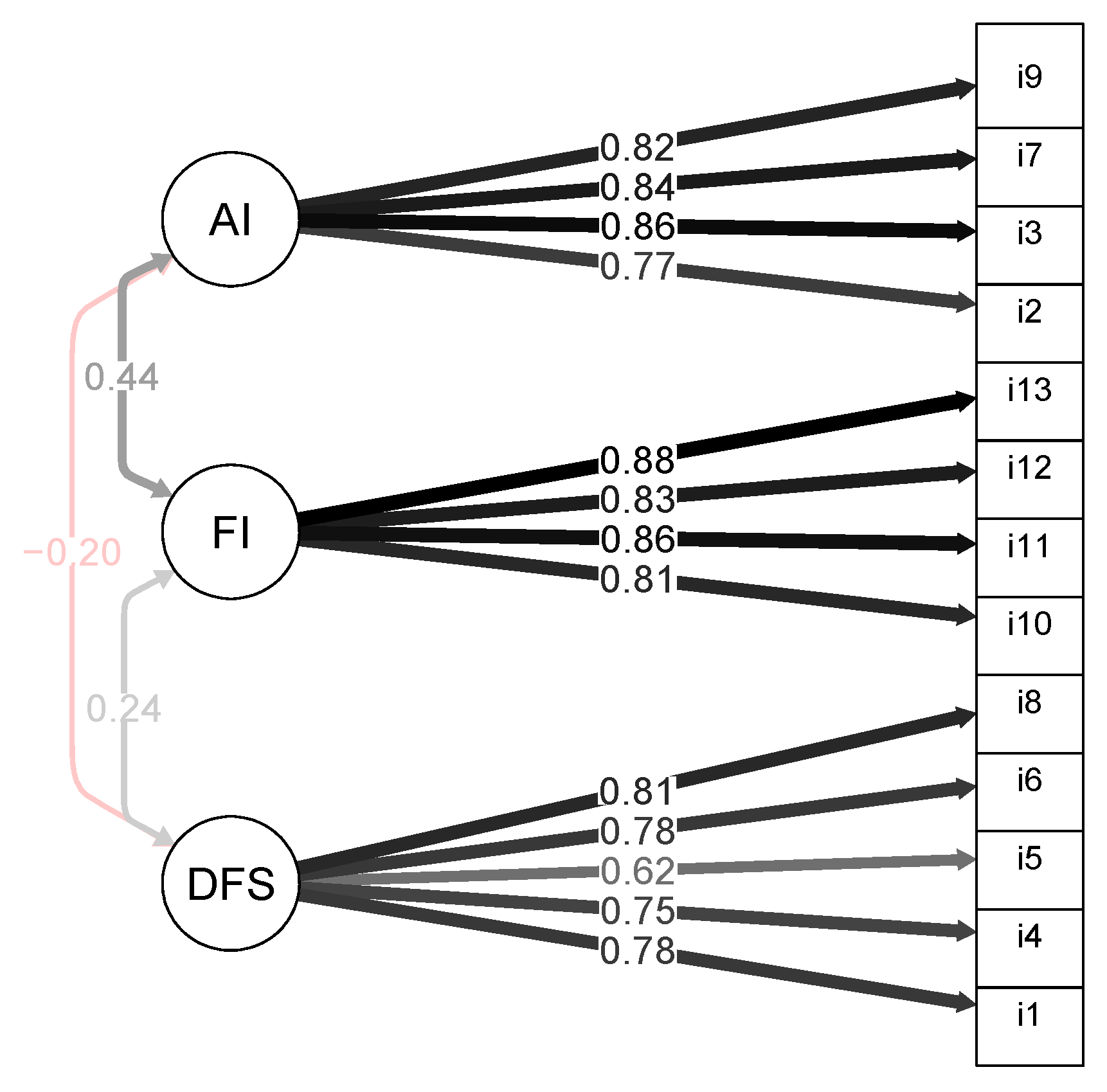
3.1. Confirmatory Factor Analysis
3.2. Group Invariance
3.3. Internal Consistency
3.4. Correlations among the MDDI Scales
3.5. Convergent and Divergent Validity
3.6. Associations between MDDI Scores and Socio-Demographic (Age, Education), BMI, and Training Features (Starting Date of Training and Weekly Training)
3.7. Between-Group Comparisons
3.8. Retest Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pope, H.G., Jr.; Gruber, A.J.; Choi, P.; Olivardia, R.; Phillips, K.A. Muscle dysmorphia: An underrecognized form of body dysmorphic disorder. Psychosomatics 1997, 38, 548–557. [Google Scholar] [CrossRef]
- Olivardia, R.; Pope, H.G., Jr.; Hudson, J.I. Muscle dysmorphia in male weightlifters: A case-control study. Am. J. Psychiat. 2000, 157, 1291–1296. [Google Scholar] [CrossRef] [PubMed]
- González-Martí, I.; Fernández-Bustos, J.G.; Contreras Jordán, O.R.; Sokolova, M. Muscle dysmorphia: Detection of the use-abuse of anabolic androgenic steroids in a Spanish sample. Adicciones 2018, 30, 243–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildebrandt, T.; Schlundt, D.; Langenbucher, J.; Chung, T. Presence of muscle dysmorphia symptomology among male weightlifters. Compr. Psychiatry 2006, 47, 127–135. [Google Scholar] [CrossRef]
- Murray, S.B.; Griffiths, S.; Mond, J.M.; Kean, J.; Blashill, A.J. Anabolic steroid use and body image psychopathology in men: Delineating between appearance-versus performance-driven motivations. Drug Alcohol. Depend. 2016, 165, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Zoccali, R.; Ponzo, V.; Soldati, L.; De Carli, L.; Benso, A.; Fea, E.; Rainoldi, A.; Durazzo, M.; Fassino, S.; et al. University courses, eating problems and muscle dysmorphia: Are there any associations? J. Transl. Med. 2014, 12, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerea, S.; Bottesi, G.; Pacelli, Q.F.; Paoli, A.; Ghisi, M. Muscle dysmorphia and its associated psychological features in three groups of recreational athletes. Sci. Rep. 2018, 8, 8877. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, L.; Murray, S.B.; Cobley, S.; Hackett, D.; Gifford, J.; Capling, L.; O’ Connor, H. Muscle dysmorphia symptomatology and associated psychological features in bodybuilders and non-bodybuilder resistance trainers: A systematic review and meta-analysis. Sports Med. 2017, 47, 233–259. [Google Scholar] [CrossRef]
- dos Santos Filho, C.A.; Tirico, P.P.; Stefano, S.C.; Touyz, S.W.; Medeiros Claudino, A. Systematic review of the diagnostic category muscle dysmorphia. Aust. N. Z. J. Psychiatry 2016, 50, 322–333. [Google Scholar] [CrossRef]
- Homan, K. Athletic-ideal and thin-ideal internalization as prospective predictors of body dissatisfaction, dieting, and compulsive exercise. Body Image 2010, 7, 240–245. [Google Scholar] [CrossRef]
- Steinfeldt, J.A.; Carter, H.; Benton, E.; Steinfeldt, M.C. Muscularity beliefs of female college student-athletes. Sex Roles 2011, 64, 543–554. [Google Scholar] [CrossRef] [Green Version]
- Readdy, T.; Watkins, P.L.; Cardinal, B.J. Muscle dysmorphia, gender role stress, and sociocultural influences: An exploratory study. Res. Q. Exerc. Sports 2011, 82, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Gruber, A.J.; Pope, H.G., Jr. Psychiatric and medical effects of anabolic-androgenic steroid use in women. Psychoter. Psychosom. 2000, 69, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Leone, J.E. Muscle dysmorphia symptomatology and extreme drive for muscularity in a 23-year-old woman: A case study. J. Strength Cond. Res. 2009, 23, 988–999. [Google Scholar] [CrossRef]
- Compte, E.J.; Cattle, C.J.; Lavender, J.M.; Murray, S.B.; Brown, T.A.; Capriotti, M.R.; Flentje, A.; Lubensky, M.E.; Obedin-Maliver, J.; Lunn, M.R.; et al. Psychometric evaluation of the Muscle Dysmorphic Disorder Inventory (MDDI) among cisgender gay men and cisgender lesbian women. Body Image 2021, 38, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, T.; Langenbucher, J.; Schlundt, D.G. Muscularity concerns among men: Development of attitudinal and perceptual measures. Body Image 2004, 1, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Compte, E.J.; Nagata, J.M.; Sepúlveda, A.R.; Rivas, A.; Sbdar, L.S.; Menga, S.; Rica, R.; Torrente, F.; Murray, S.B. Assessment and validation of a spanish version of the muscle dysmorphia disorder inventory in argentinian men who exercise: Inventario de dismorfia muscular. Body Image 2019, 31, 24–34. [Google Scholar] [CrossRef]
- Nagata, J.M.; Junqueira, A.C.P.; Cattle, C.J.; de Carvalho, P.H.B.; Bagolin, V.; Murray, S.B.; Compte, E.J.; Costa, T.M.B.; de Sousa Almeida, S.; Laus, M.F. Validation of the muscle dysmorphic disrder inventory (MDDI) in Brazilian women. Body Image 2022, 41, 58–66. [Google Scholar] [CrossRef]
- Santarnecchi, E.; Dèttore, D. Muscle dysmorphia in different degrees of bodybuilding activities: Validation of the italian version of muscle dysmorphia disorder inventory and bodybuilder image grid. Body Image 2012, 9, 396–403. [Google Scholar] [CrossRef]
- Sepúlveda, A.R.; Rica, R.; Moreno, A.; Román, F.J.; Compte, E.J. Asessing the male body image: Spanish validation of two instruments. Psychiatry Res. 2019, 272, 483–490. [Google Scholar] [CrossRef]
- Galiana, L.; Badenes-Ribera, L.; Fuentes, M. Validación de la versión española del inventario del trastorno por dismorfia muscular en una muestra de estudiantes universitarios. In Atención a las Necesidades Comunitarias Para la Salud; Núñez, J.C., Molero, M.M., Gázquez, J.J., Pérez-Fuentes, M.C., Simón, M.M., Martos, A., Barragan, Y.A.B., Eds.; Scinfoper: Almería, Spain, 2017; pp. 41–46. [Google Scholar]
- Zeeck, A.; Welter, V.; Alatas, H.; Hildebrandt, T.; Lahmann, C.; Hartmann, A. Muscle dysmorphic disorder inventory (MDDI): Validation of a german version with a focus on gender. PLoS ONE 2018, 13, e0207535. [Google Scholar] [CrossRef] [PubMed]
- Hale, B.D.; Diehl, D.; Weaver, K.; Briggs, M. Exercise dependence and muscle dysmorphia in novice and experienced female bodybuilders. J. Behav. Addict. 2013, 2, 244–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hale, B.D.; Smith, D. Bodybuilding. In Encyclopedia of Body Image and Human Appearance; Cash, T.F., Ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2012; pp. 66–73. [Google Scholar] [CrossRef]
- Tod, D.; Lavallee, D. Towards a conceptual understanding of muscle dysmorphia development and sustainment. Int. Rev. Sport Exerc. Psychol. 2010, 3, 111–131. [Google Scholar] [CrossRef]
- Gruber, A.J.; Pope, H.G., Jr. Compulsive weight lifting and anabolic drug abuse among women rape victims. Compr. Psychiatry 1999, 40, 273–277. [Google Scholar] [CrossRef]
- Campos, P.F.; Almeida, M.; Neves, C.M.; Rodgers, R.F.; Ferreira, M.E.C.; de Carvalho, P.H.B. Assessing the Rising Emphasis on Muscolarity for Women: Psychometric Properties of the Brazialian Version of the Female Muscolarity Scale. Sex Roles 2021, 85, 313–325. [Google Scholar] [CrossRef]
- Foster, A.; Shorter, G.; Griffiths, M. Muscle Dysmorphia: Could it be classified as an addiction to body image? J. Behav. Addict. 2015, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Cafri, G.; Yamamiya, Y.; Brannick, M.; Thompson, J.K. The influence of sociocultural factors on body image: A meta-analysis. Clin. Psychol. Sci. Pract. 2005, 12, 421–433. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965; Available online: https://www.jstor.org/stable/j.ctt183pjjh (accessed on 30 September 2021).
- Prezza, M.; Trombaccia, F.R.; Armento, L. La Scala Dell’autostima di Rosenberg: Traduzione e Validazione Italiana; Giunti Organizzazioni Speciali: Florence, Italy, 1997; Volume 223, pp. 35–44. [Google Scholar]
- Mattick, R.P.; Clarke, J.C. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav. Res. 1998, 36, 455–470. [Google Scholar] [CrossRef]
- Sica, C.; Musoni, I.; Chiri, L.R.; Bisi, B.; Lolli, V.; Sighinolfi, C. Social phobia scale (SPS) and social interaction anxiety scale (SIAS): Italian translation and adaptation. Boll. Psicol. Applicata. 2007, 252, 59–71. Available online: https://flore.unifi.it/handle/2158/256030 (accessed on 30 September 2021).
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian Version of the Depression Anxiety Stress Scales-21: FactorStructure and Psychometric Properties on Community and Clinical Samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014; Available online: http://www.r-project.org/index.html (accessed on 4 February 2022).
- Rosseel, Y. lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Hox, J. Multilevel Analysis: Techniques and Applications, 2nd ed.; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Byrne, B. Structural Equation Modeling with LISREL, PRELIS, and SIMPLIS: Basic Concepts, Applications, and Programming; Lawrence Erlbaum: Mahwah, NJ, USA, 1998. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Dunn, T.J.; Baguley, T.; Brunsden, V. From alpha to omega: A practical solution to the pervasive problem of internal consistency estimation. Br. J. Psychol. 2014, 105, 399–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunnally, J.C. An overview of psychological measurement. In Clinical Diagnosis of Mental Disorders; Wolman, B.B., Ed.; Springer: Boston, MA, USA, 1978; pp. 97–146. [Google Scholar] [CrossRef]
- Cohen, J. Quantitative methods in psychology: A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Peters, G. Userfriend Lyscience: Quantitative Analysis Made Accessible. R Package Version 0.7.2. Available online: https://userfriendlyscience.com (accessed on 4 February 2022).
- Wu, A.D.; Li, Z.; Zumbo, B.D. Decoding the meaning of factorial invariance and updating the practice of multi-group confirmatory factor analysis: A demonstration with TIMSS data. Pract. Assess. Res. Eval. 2007, 12, 3. [Google Scholar] [CrossRef]
- Giuntoli, L.; Ceccarini, F.; Sica, C.; Caudek, C. Validation of the italian versions of the flourishing scale and of the scale of positive and negative experience. SAGE Open 2017, 7, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hargreaves, D.A.; Tiggemann, M. Idealized media images and adolescent body image: “Comparing” boys and girls. Body Image 2004, 1, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Leit, R.A.; Pope , H.G., Jr.; Gray, J.J. Cultural expectations of muscularity in men: The evolution of Playgirl centerfolds. Int. J. Eat. Disord. 2001, 29, 90–93. [Google Scholar] [CrossRef]
- Rodgers, R.F.; Franko, D.L.; Lovering, M.E.; Luk, S.; Pernal, W.; Matsumoto, A. Development and validation of the female muscularity scale. Sex Roles 2018, 78, 18–26. [Google Scholar] [CrossRef]
- Skemp, K.M.; Mikat, R.P.; Schenck, K.P.; Kramer, N.A. Muscle dysmorphia: Risk may be influenced by goals of the weightlifter. J. Strength Cond. Res. 2013, 27, 2427–2432. [Google Scholar] [CrossRef] [PubMed]
- Frederick, D.A.; Forbes, G.B.; Grigorian, K.E.; Jarcho, J.M. The UCLA body project I: Gender and ethnic differences in self-objectification and body satisfaction among 2206 undergraduates. Sex Roles 2017, 57, 317–327. [Google Scholar] [CrossRef]
- Swami, V.; Frederick, D.A.; Aavik, T.; Alcalay, L.; Allik, J.; Anderson, D.; Andrianto, S.; Arora, A.; Brännström, A.; Cunningham, J.; et al. The attractive female body weight and female body dissatisfaction in 26 countries across 10 world regions: Results of the international body project I. Person. Soc. Psychol. Bull. 2010, 36, 309–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiggemann, M.; Zaccardo, M. ‘Strong is the new skinny’: A content analysis of #fitspiration images on instagram. J. Health Psychol. 2018, 23, 1003–1011. [Google Scholar] [CrossRef]
- Boepple, L.; Ata, R.N.; Rum, R.; Thompson, J.K. Strong is the new skinny: A content analysis of fitspiration websites. Body Image 2016, 17, 132–135. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Overall Sample (n = 518) M (DS)/% | Non-Competing Bodybuilding/Powerlifting (n = 165) M (DS)/% | Physical Exercise (n = 353) M (DS)/% | t(517)/χ2(4/6) | p | ηp2 | |
|---|---|---|---|---|---|---|
| Age | 30.01 (8.05) | 29 (7.78) | 30.49 (8.16) | −1.96 | 0.05 | - |
| Education | 15.28 (2.87) | 15.65 (3.08) | 15.09 (2.74) | 2.06 | 0.03 | - |
| Body mass index | 22.91 (3.95) | 22.03 (3.05) | 23.33 (4.26) | −3.87 | p < 0.001 | 0.02 |
| Marital Status | ||||||
| Single | 23.1 | 30.7 | 19.5 | |||
| In a relationship | 32.4 | 36.7 | 30.3 | |||
| Married/cohabiting | 42.2 | 31.9 | 47 | 17.32 | 0.002 | - |
| Separated/divorced | 2.1 | 0.6 | 2.8 | |||
| Widowed | 0.2 | 0 | 0.3 | |||
| Occupation | ||||||
| Student | 28.8 | 28.3 | 29.2 | |||
| Full-time employed | 29.9 | 26.5 | 31.4 | |||
| Part-time employed | 11 | 14.5 | 9.3 | 6.67 | 0.35 | - |
| Housewife | 5.6 | 3.6 | 6.5 | |||
| Unemployed | 8.9 | 8.4 | 9.1 | |||
| Other | 15.8 | 18.6 | 14.4 | |||
| Starting date of exercise (in months) | 34.22 (50.02) | 29.69 (24.06) | 35.93 (57.02) | −1.45 | 0.15 | - |
| Weekly training (days) | 4.18 (1.69) | 3.89 (1.12) | 4.30 (1.89) | −2.94 | 0.003 | 0.01 |
| Retest Sample (n = 100) M (DS)/% | Non-Competing Bodybuilding/Powerlifting (n = 50) M (DS)/% | Physical Exercise (n = 50) M (DS)/% | |
|---|---|---|---|
| Age | 24.74 (4.53) | 25.52 (5.69) | 23.96 (2.80) |
| Education | 15.18 (2.40) | 14.52 (2.52) | 15.84 (2.08) |
| Body mass index | 21.15 (2.70) | 21.81 (3.07) | 20.48 (2.09) |
| Marital Status | |||
| Single | 31 | 36 | 26 |
| In a relationship | 54 | 38 | 70 |
| Married/cohabiting | 13 | 22 | 4 |
| Separated/divorced | 2 | 4 | 0 |
| Widowed | 0 | 0 | 0 |
| Occupation | |||
| Student | 53 | 42 | 64 |
| Full-time employed | 21 | 30 | 12 |
| Part-time employed | 11 | 12 | 10 |
| Housewife | 1 | 2 | 0 |
| Unemployed | 4 | 6 | 2 |
| Other | 10 | 8 | 12 |
| Starting date of exercise (in months) | 48.71 (52.81) | 38.18 (25.49) | 59.24 (68.99) |
| Weekly training (days) | 3.33 (1.11) | 3.90 (0.76) | 2.76 (1.12) |
| Model | χ2 | df | CFI | TLI | RMSEA | SRMR |
|---|---|---|---|---|---|---|
| Configural | 353.206 | 124 | 0.956 | 0.945 | 0.085 | 0.093 |
| Thresholds | 376.606 | 137 | 0.954 | 0.948 | 0.083 | 0.093 |
| Metric | 388.126 | 145 | 0.954 | 0.951 | 0.080 | 0.093 |
| Scalar | 399.013 | 157 | 0.953 | 0.954 | 0.078 | 0.094 |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) MDDI_tot | 0.81 ** | 0.59 ** | 0.57 ** | −0.43 ** | 0.45 ** | 0.45 ** | −0.17 * | −0.01 | 0.02 | 0.12 | 0.21 ** | |
| (2) MDDI_FI | 0.80 ** | 0.31 ** | 0.28 ** | −0.20 ** | 0.28 ** | 0.35 ** | −0.07 | 0.04 | −0.02 | 0.29 ** | 0.40 ** | |
| (3) MDDI_AI | 0.73 ** | 0.38 ** | −0.15 | −0.60 ** | 0.52 ** | 0.42 ** | −0.14 | −0.04 | 0.46 ** | 0.03 | 0.01 | |
| (4) MDDI_DFS | 0.43 ** | 0.19 ** | −0.09 | −0.05 | 0.09 | 0.11 | −0.12 | −0.03 | −0.39 ** | −0.08 | 0.01 | |
| (5) RSES | −0.49 ** | −0.29 ** | −0.54 ** | −0.09 | −0.63 ** | −0.56 ** | 0.19 * | 0.17 * | −0.14 | −0.04 | 0.12 | |
| (6) SPS | 0.45 ** | 0.26 ** | 0.46 ** | 0.13 ** | −0.53 ** | 0.54 ** | −0.24 ** | −0.20 ** | 0.08 | 0.12 | −0.01 | |
| (7) DASS-21 | 0.50 ** | 0.34 ** | 0.45 ** | 0.17 ** | −0.68 ** | 0.52 ** | −0.25 ** | −0.03 | 0.12 | −0.03 | 0.02 | |
| (8) Age | −0.21 ** | −0.16 ** | −0.07 | −0.22 ** | 0.26 ** | −0.27 ** | −0.18 * | 0.09 | 0.10 | 0.11 | −0.02 | |
| (9) Education | −0.09 | −0.03 | −0.06 | −0.09 | 0.07 | −0.18 ** | −0.08 | 0.09 | 0.09 | 0.12 | 0.06 | |
| (10) BMI | 0.05 | −0.04 | 0.41 ** | −0.39 ** | −0.13 * | 0.07 | 0.04 | 0.22 ** | 0.02 | −0.02 | −0.06 | |
| (11) Months of Training | −0.07 | 0.04 | −0.17 ** | 0.01 | 0.06 | −0.14 * | −0.09 | 0.13 * | 0.13* | −0.12 | 0.21 ** | |
| (12) Weekly Training (days) | 0.06 | 0.19 ** | −0.07 | 0.01 | 0.14 * | −0.12 * | −0.13 * | 0.11 * | −0.12 * | −0.12 * | 0.01 |
| Non-Competing Bodybuilding/Powerlifting (n = 165) M (DS) | Physical Exercise (n = 353) M (DS) | t(517) | p | ηp2 | |
|---|---|---|---|---|---|
| MDDI Total Score | 31.52 (8.44) | 27.44 (7.34) | 5.34 | p < 0.001 | 0.06 |
| MDDI FI | 11.32 (4.38) | 8.59 (3.73) | 6.92 | p < 0.001 | 0.09 |
| MDDI AI | 11.09 (4.24) | 11.89 (4.23) | −2.01 | 0.04 | - |
| MDDI DFS | 9.11 (4.21) | 6.95 (2.88) | 5.96 | p < 0.001 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerea, S.; Giraldo, M.; Caudek, C.; Bottesi, G.; Paoli, A.; Ghisi, M. Validation of the Muscle Dysmorphic Disorder Inventory (MDDI) among Italian Women Practicing Bodybuilding and Powerlifting and in Women Practicing Physical Exercise. Int. J. Environ. Res. Public Health 2022, 19, 9487. https://doi.org/10.3390/ijerph19159487
Cerea S, Giraldo M, Caudek C, Bottesi G, Paoli A, Ghisi M. Validation of the Muscle Dysmorphic Disorder Inventory (MDDI) among Italian Women Practicing Bodybuilding and Powerlifting and in Women Practicing Physical Exercise. International Journal of Environmental Research and Public Health. 2022; 19(15):9487. https://doi.org/10.3390/ijerph19159487
Chicago/Turabian StyleCerea, Silvia, Matteo Giraldo, Corrado Caudek, Gioia Bottesi, Antonio Paoli, and Marta Ghisi. 2022. "Validation of the Muscle Dysmorphic Disorder Inventory (MDDI) among Italian Women Practicing Bodybuilding and Powerlifting and in Women Practicing Physical Exercise" International Journal of Environmental Research and Public Health 19, no. 15: 9487. https://doi.org/10.3390/ijerph19159487
APA StyleCerea, S., Giraldo, M., Caudek, C., Bottesi, G., Paoli, A., & Ghisi, M. (2022). Validation of the Muscle Dysmorphic Disorder Inventory (MDDI) among Italian Women Practicing Bodybuilding and Powerlifting and in Women Practicing Physical Exercise. International Journal of Environmental Research and Public Health, 19(15), 9487. https://doi.org/10.3390/ijerph19159487