
The 2019 Philippine UHC Act, Pandemic Management and Implementation Implications in a Post-COVID-19 World: A Content Analysis

 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Overview of the Philippine Health System
1.2. Pandemic Performance
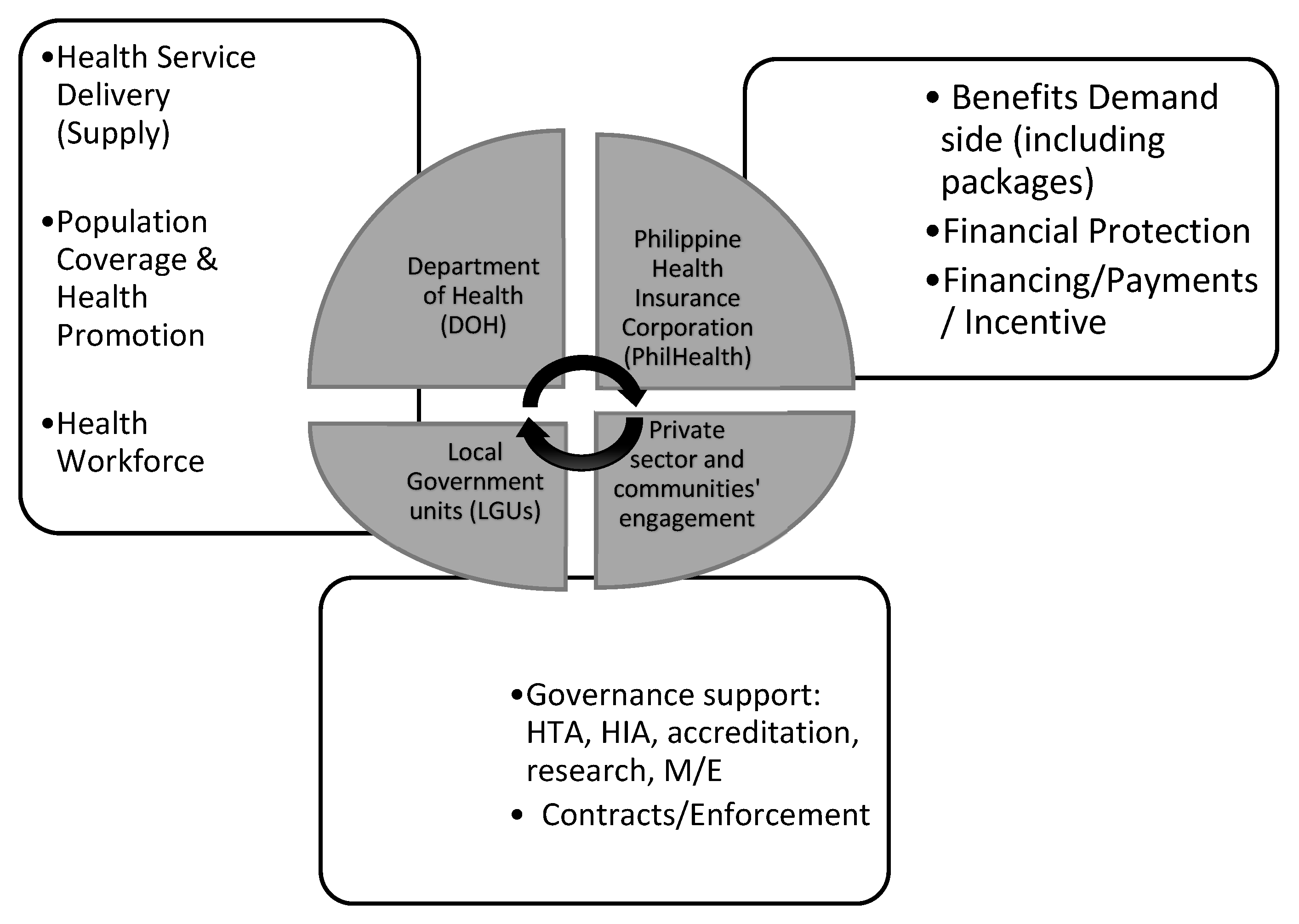
1.3. Framework
2. Materials and Methods
3. Results
4. Discussion
4.1. National-Local Interactions
4.2. Other Stakeholders and Contracting
4.3. Other Cross-Cutting Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- An Act Instituting Universal Health Care for All Filipinos, Prescribing Reforms in the Health Care System, and Appropriating Funds Therefore. 2019. Available online: https://www.doh.gov.ph/sites/default/files/health_magazine/RANo11223_UHC.pdf (accessed on 9 August 2021).
- Kutzin, J. Health financing for universal coverage and health system performance: Concepts and implications for policy. Bull World Health Organ. 2013, 91, 602–611. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3738310/ (accessed on 2 February 2022). [CrossRef]
- Slapin, J.; Proskch, S.-O. Words as Data: Content Analysis in Legislative Studies; Martin, S., Saalfeld, T., Strøm, K.W., Eds.; The Oxford Handbook of Legislative Studies, USA-OSO; ProQuest: Ann Arbor, MI, USA, 2014. [Google Scholar]
- Kayes, N.; Shun-King, M. The role of document analysis in health policy analysis studies in low and middle-income countries: Lessons for HPA researchers from a qualitative systematic review. In Health Policy Open; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Derakhshani, N.; Doshmangir, L.; Ahmadi, A.; Fakhri, A.; Sadeghi-Bazargani, H.; Gordeev, V.S. Monitoring Barriers and Enablers Towards Universal Health Coverage within sutainable development goals: A systematic review and content analysis. Clin. Econ. Outcomes Res. 2020, 12, 459–472. [Google Scholar] [CrossRef] [PubMed]
- British Academy. The COVID Decade: Understanding the Long-Term Societal Impacts of COVID-19; The British Academy: London, UK, 2021. [Google Scholar] [CrossRef]
- World Bank. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=PH (accessed on 2 February 2022).
- Philippine Statistics Authority. Health Spending Registered 12.6 Percent Growth, Share of Health to Economy Went Up to 5.6 Percent in 2020. Reference no. 2021-427. 14 October 2021. Available online: https://psa.gov.ph/pnha-press-release/node/165216 (accessed on 2 February 2022).
- Capuno, J.J.; Kraft, A.D.; O’Donnell, O. Filling potholes on the road to universal health coverage in the philippines. Health Syst. Reform. 2022, 7, e1911473. Available online: https://www.sciencegate.app/document/10.1080/23288604.2021.1911473 (accessed on 2 February 2022). [CrossRef]
- UHC Service Coverage Index—Philippines. Available online: https://data.worldbank.org/indicator/SH.UHC.SRVS.CV.XD?locations=PH (accessed on 2 February 2022).
- Philippine Statistics Authority. National Demographic and Health Survey 2017. Philippines National Demographic and Health Survey 2017 [FR347]. Available online: https://psa.gov.ph/sites/default/files/PHILIPPINE%20NATIONAL%20DEMOGRAPHIC%20AND%20HEALTH%20SURVEY%202017_new.pdf (accessed on 2 February 2022).
- Dayrit, M.; Lagrada, L.; Picazo, O.; Pons, M.; Villaverde, M. The Philippines Health System Review; Regional Office for South East Asia, Health in Transition Series; World Health Organization: New Delhi, India, 2018; Volume 8. [Google Scholar]
- Philippine Statistics Authority. Philippine Statistical Yearbook. 2018. Available online: https://psa.gov.ph/sites/default/files/2018%20PSY_final%28revised%20asof26Mar19%29_0.pdf (accessed on 2 February 2022).
- Nikki. A Look into the UHC Advanced Implementation Sites (AIS) Rollout. 2020. Available online: https://www.curally.ph/blog/67 (accessed on 22 November 2021).
- Philippine Congress. Republic Act 7305: Magna Carta of Public Health Workers; Philippine Congress: Manila, Philippines, 1992. [Google Scholar]
- Tangcalagan, K.; Bool, D.P. Universal Health Care in the Philippines through the Lens of Workforce 2030: An Omnibus Review of Human Resources for Health Policies; USAID Human Resources for Health 2030: Manila, Philippines, 2019. [Google Scholar]
- World Bank. Philippines: Mandanas Ruling Provides Opportunities for Improving Service Delivery through Enhanced Decentralization; Press Release: London, UK, 2021; Available online: https://www.worldbank.org/en/news/press-release/2021/06/10/philippines-mandanas-ruling-provides-opportunities-for-improving-service-delivery-through-enhanced-decentralization (accessed on 22 November 2021).
- Department of Health. COVID-19 National Cases Data as of 15 February 2022. COVID-19 hotline (viber messaging).
- Calonzo, A. Why the Philippines Is Once Again the Worst Place to Be in COVID. Available online: https://www.bloomberg.com/news/articles/2022-01-27/why-the-philippines-is-once-again-the-worst-place-to-be-in-covid (accessed on 27 January 2022).
- Leischow, S.J.; Best, A.; Trochim, W.M.; Clark, P.I.; Gallagher, R.S.; Marcus, S.E.; Matthews, E. Systems thinking to improve the public’s health. Am. J. Prev. Med. 2008, 35 (Suppl. 2), S196–S203. [Google Scholar] [CrossRef] [Green Version]
- Adam, T. Advancing the application of systems thinking in health. Health Res. Policy Syst. 2014, 12, 50. [Google Scholar] [CrossRef] [Green Version]
- Yap, M. Panel Member Response to Keynote Paper, Presented to the Third Health Leadership Summit; AC Health and Ateneo Professional Schools: Makati, Philippines, 2022. [Google Scholar]
- Asian Development Bank. Public-Private Partnership Monitor: Philippines; Asian Development Bank: Mandaluyong, Philippines, 2020. [Google Scholar]
- World Health Organization. Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies; World Health Organization: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/258734 (accessed on 9 August 2021).
- The Independent Panel. COVID-19: Make It the Last Pandemic; Summary of the Main Report: Geneva, Switzerland, 2021; Available online: https://theindependentpanel.org/wp-content/uploads/2021/05/Summary_COVID-19-Make-it-the-Last-Pandemic_final.pdf (accessed on 9 August 2021).
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Medicine. 2016, 15, 155–163. Available online: https://www.sciencedirect.com/science/article/pii/S1556370716000158 (accessed on 16 July 2021). [CrossRef] [PubMed] [Green Version]
- StataCorp. Icc—Intraclass correlation coefficients. In Stata: Release 15. Statistical Software; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Implementing Rules and Regulations of the Universal Health Care Act (Republic Act No. 11223). 2019. Available online: https://doh.gov.ph/sites/default/files/health_magazine/UHC-IRR-signed.pdf (accessed on 15 November 2021).
- Republic of the Philippines. Republic Act 7160: The Local Government Code of 1991; Government of the Philippines: Manila, Philippines, 1991.
- Salaverria, L.; Gascon, M.; Burgos, N. PhilHealth Fails to Stop Exit of 7 Iloilo Hospitals; Philippine Daily Inquirer: Manila, Philippines, 29 December 2021; Available online: https://newsinfo.inquirer.net/1533254/philhealth-fails-to-stopexit-of-7-iloilo-hospitals (accessed on 2 February 2022).
- Schuhmann, R.; Bautista, M.C.G. Contracting for Health Care under the New Philippine UHC Act. In VRÜ Verfassung und Recht in Übersee/WCL; Nomos: Berlin, Germany, 2021; Volume 54, pp. 98–115. [Google Scholar]
- Francisco-Alcantara, K. Introspective: Our Brand Is Crisis: Controversies, Challenges and Opportunities in Pandemic Procurement, Business World. Available online: https://www.bworldonline.com/opinion/2021/09/26/399009/our-brand-is-crisis-controversies-challenges-and-opportunities-in-pandemic-procurement/ (accessed on 26 September 2021).
- Salaverria, L. Malacanang Urges PhilHealth to Settle Hospital Claims. Available online: https://newsinfo.inquirer.net/1477758/malacanang-to-philhealth-settle-hospital-claims (accessed on 24 August 2021).
- Cheng, S.H.; Jin, H.H.; Yang, B.M.; Blank, R.H. Health Expenditure Growth under Single-Payer Systems: Comparing South Korea and Taiwan. Value Health Reg. Issues 2018, 15, 149–154. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Features | Figures (as Indicated) | ||
|---|---|---|---|
| Current Health Expenditures-CHE (NHA 2020 in [8]) | 5.6% of GDP | Growth Rate of (CHE) | |
| 2019–2020 | 12.6% | ||
| 2018–2019 | 10.2% | ||
| Health financing (NHA: 2020 in [8])-households (out of pocket) | 44.7% | Government and Compulsory Schemes | 45.7% |
| Distribution of Household Out of pocket Expenses (NHA: 2020 in [8]) | 43.8% hospitals | 28.2% drugs, pharmacies | 9.0% preventive care |
| UHC Coverage Index (WHO and World Bank data in [10]) | 55% | ||
| HC Utilization by households (DHS: 2017 in [11]) | 8% of household population sought care past 30 days | 59% sought from public medical facilities | 40% sought care from private medical facilities |
| Health service delivery (Dayrit et al., 2018 in [12]) | 1224 Hospital facilities, 64% private and 35% public in 2016; 66% located in main island | 2587 city/rural health centers, 20,216 village health stations In 2016 | Two-thirds are level 1 hospitals, with 41 beds on average; 10% are level 3, with 318 beds on average |
| Health Human Resources (Philippine Statistical Yearbook/PSY, 2018 in [13]) | 83% of health and medical graduates in 2015–2016 were from private schools (HIT, 2018) | 3131 doctors in govt service; 1875 Dentists; 5975 Nurses | 17,112 Midwives |
| Public sector employs 61% of nurses and 90% of midwives (HIT, 2018) | 91% of Medical doctors and 74% of nurses work in hospitals (HiT,2018) | ||
| Health Governance | DOH as the overall policy setting of population-based care, and provision of regional hospital and specialist services; PhilHealth, the social insurance arm, as purchaser of personal-based care | LGUs as facility owners, managers and implementers of health programs and services | Local Health Boards as advisers to chief executives and local legislatures, with DoH representative |
| Implementing Agency | Investment (Php) | J-Yen | USD | Status | |
|---|---|---|---|---|---|
| Philippine General Hospital-Diliman | University of the Philippines | 21.3 billion | 47.9 trillion | 414.92 million | before ICC for approval |
| Baguio General Hospital and Medical Center, Renal Center | LGU and DOH | 470 million | 1 billion | 8.0 million | |
| Cagayan Valley Medical Center Hemodialysis Center | LGU and DOH | 330 million | 742 million | 6.4 million | |
| Philippine General Hospital—PGH Manila Cancer Center | PGH | 4.6 billion | 10.3 billion | 89.6 million | before ICC for approval |
| Mariveles Mental Health and Wellness Center | LGU and DOH | ||||
| Makati Life Medical Center | LGU-Prv | 5 billion | 11 billion | 97.2 million |
| Component | Mean ± Std. Deviation | Minimum–Maximum Frequency |
|---|---|---|
| DOH/national government | 55.9 ± 8.5 | 42–68 |
| PhilHealth | 50.9 ± 9.3 | 39–67 |
| Contracts/Enforcement | 46.5 ± 23.2 | 11–70 |
| Governance Support (HTA, HIA, accreditation, research, ME) * | 42.7 ± 11.6 | 21–60 |
| Financing/Payments/Incentives | 39 ± 6.5 | 26–45 |
| Community/Engagement | 34.7 ± 12.5 | 16–53 |
| Supply: Service Delivery | 29.9 ± 8.8 | 22–48 |
| Private Providers/Other Partners, (e.g., HMOs, Fund Managers) * | 25.0 ± 6.9 | 19–37 |
| Population Coverage and Health Promotion | 23.9 ± 4.5 | 17–29 |
| Financial Protection | 23.6 ± 10.8 | 9–38 |
| Values/Principles/Ethics | 18.4 ± 6.4 | 11–29 |
| Benefits Demand Side (Including packages) | 16.6 ± 9.9 | 3–28 |
| LGU/DILG | 13.4 ± 4.0 | 8–19 |
| Human Resource (HR)/Workforce Support Systems | 4.4 ± 2.9 | 1–8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bautista, M.C.G.; Acacio-Claro, P.J.; Mendoza, N.B.; Pulmano, C.; Estuar, M.R.J.; Dayrit, M.M.; Festin, V.E.; Valera, M.; Sugon, Q., Jr.; Villamor, D.A. The 2019 Philippine UHC Act, Pandemic Management and Implementation Implications in a Post-COVID-19 World: A Content Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9567. https://doi.org/10.3390/ijerph19159567
Bautista MCG, Acacio-Claro PJ, Mendoza NB, Pulmano C, Estuar MRJ, Dayrit MM, Festin VE, Valera M, Sugon Q Jr., Villamor DA. The 2019 Philippine UHC Act, Pandemic Management and Implementation Implications in a Post-COVID-19 World: A Content Analysis. International Journal of Environmental Research and Public Health. 2022; 19(15):9567. https://doi.org/10.3390/ijerph19159567
Chicago/Turabian StyleBautista, Maria Cristina G., Paulyn Jean Acacio-Claro, Nori Benjamin Mendoza, Christian Pulmano, Maria Regina Justina Estuar, Manuel M. Dayrit, Vincent Edward Festin, Madeleine Valera, Quirino Sugon, Jr., and Dennis Andrew Villamor. 2022. "The 2019 Philippine UHC Act, Pandemic Management and Implementation Implications in a Post-COVID-19 World: A Content Analysis" International Journal of Environmental Research and Public Health 19, no. 15: 9567. https://doi.org/10.3390/ijerph19159567
APA StyleBautista, M. C. G., Acacio-Claro, P. J., Mendoza, N. B., Pulmano, C., Estuar, M. R. J., Dayrit, M. M., Festin, V. E., Valera, M., Sugon, Q., Jr., & Villamor, D. A. (2022). The 2019 Philippine UHC Act, Pandemic Management and Implementation Implications in a Post-COVID-19 World: A Content Analysis. International Journal of Environmental Research and Public Health, 19(15), 9567. https://doi.org/10.3390/ijerph19159567