
The Risk for Neonatal Hypoglycemia and Bradycardia after Beta-Blocker Use during Pregnancy or Lactation: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
1.1. Mechanisms of Action and Potential Risks
1.2. Aim of the Study
2. Materials and Methods
2.1. Protocol and Registration
2.2. Patient and Public Involvement
2.3. Eligibility Criteria
- Randomized controlled trials, case series, case reports and observational studies reporting the adverse effects of beta-blockers exposure during pregnancy and lactation on the neonate;
- The described effect on the neonate should focus on hypoglycemia and/or bradycardia (the chosen cut-off value for hypoglycemia and bradycardia could vary between studies);
- Studies in English;
- Studies in human subjects.
- 5.
- Articles studying only the effect of the disease of the mother on the neonate;
- 6.
- Studies on the effect of beta-blockers on only the fetus and not the neonate;
- 7.
- Reviews and editorials;
- 8.
- Letters to the Editor.
2.4. Information Sources
2.5. Search Strategy
2.6. Study Selection
2.7. Data Collection Process
2.8. Data Items
2.9. Risk of Bias Assessment
2.10. Certainty of Evidence Assessment
2.11. Data Synthesis
3. Results
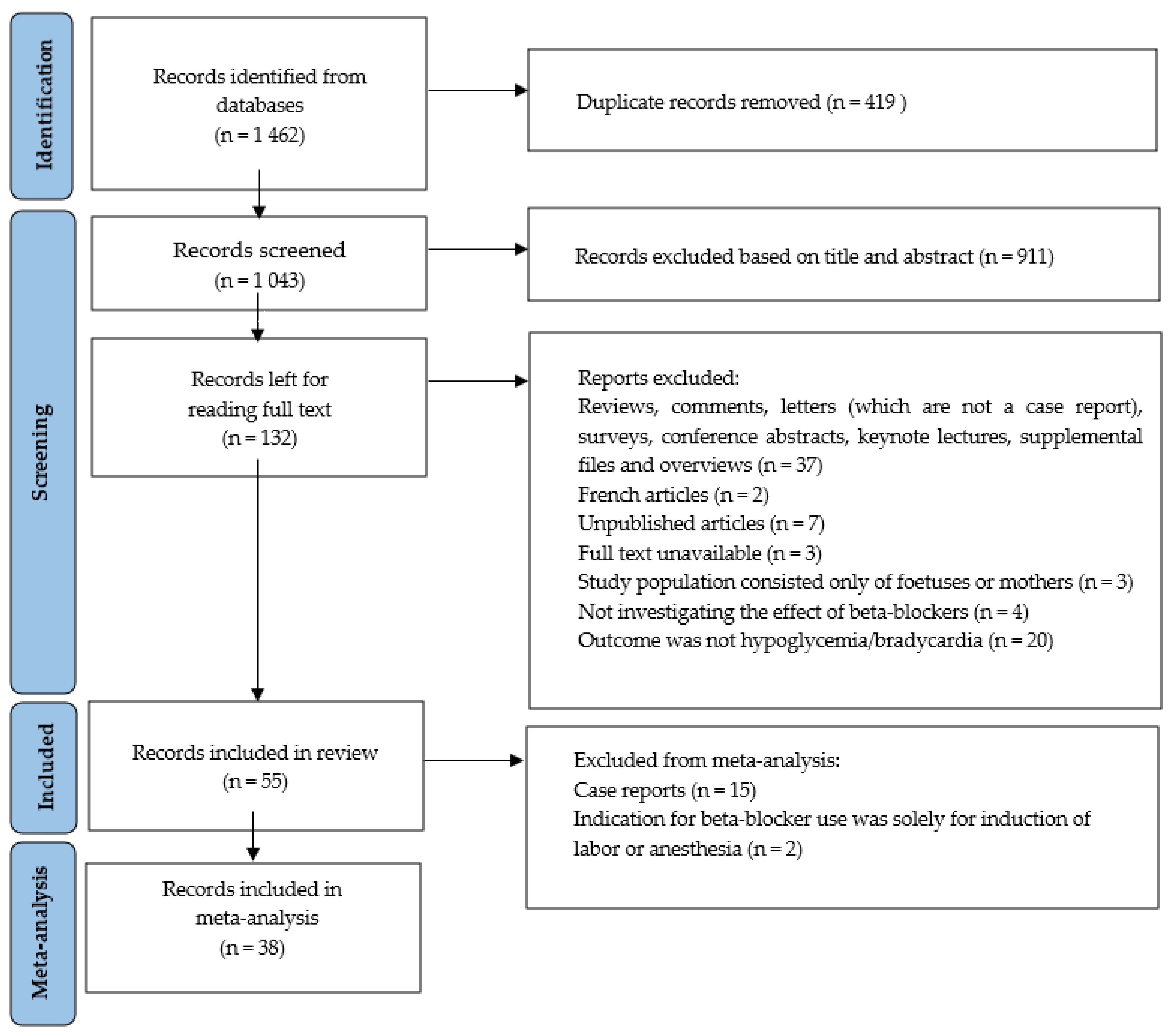
3.1. Study Selection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Study Group | Number of Patients | Country | Study Design | Objective | Treatment Indication | Outcome |
|---|---|---|---|---|---|---|---|
| Bigelow CA, 2021 [29] | Nulliparous patients undergoing term induction of labor with a single, non-anomalous gestation received propranolol or placebo | n = 121 cases vs. n = 119 controls | United States | RCT | To determine whether the addition of a single dose of propranolol to induce labor in nulliparous women would decrease total time to vaginal delivery | Induction of labor | Hypoglycemia |
| Kayser A, 2020 [30] | Neonates of hypertensive women treated with metoprolol and/or bisoprolol after the first trimester, but not with methyldopa at any time during pregnancy | n = 294 cases vs. n = 225 controls (methyldopa) vs. n = 588 controls (nonhypertensive mothers) | Germany | Cohort study | To evaluate the effects of beta blockers during the second and third trimester on fetal growth, length of gestation and postnatal symptoms in exposed infants | Chronic or pregnancy-induced hypertension | Hypoglycemia and bradycardia |
| Kumar N, 2020 [31] | All the infants born ≥34 weeks with mothers using beta blockers prenatally compared to mothers with diabetes, both beta-blockers and diabetes or without pregnancy conditions | n = 228 cases (BB) and n = 60 both vs. n = 379 controls (diabetes), and n = 4.103 controls (no pregnancy condition) | United States | Cohort study | To evaluate whether pregnancy glycated hemoglobin (HbA1c) levels of ≤6% and maternal race impacts neonatal hypoglycemia and birthweight, and whether diabetes and beta blocker use during pregnancy additively impacts neonatal outcomes | Not described in article | Hypoglycemia |
| Mazkereth R, 2019 [32] | Infants born to mothers who were treated with beta-blockers during pregnancy and until delivery | n = 153 cases vs. n = 153 controls | Israel | Case–control | To evaluate infants exposed to intrauterine beta blockers in order to estimate the need of postnatal monitoring | Cardiac disease (arrhythmia, rheumatic heart disease and cardiomyopathy), chronic hypertension, migraine, PIH (pregnancy induced hypertension) and pre-eclampsia | Hypoglycemia and bradycardia |
| Easterling T, 2019 [33] | Pregnant woman older than 18 years and gestational age of at least 28 weeks received labetalol, nifedipine or methyldopa | n = 295 cases vs. n = 298 controls (nifedipine) vs. n = 301 controls (methyldopa) | India | RCT | To compare the efficacy and safety of oral labetalol, nifedipine retard and methyldopa for the management of severe hypertension in pregnancy | Hypertension in pregnancy | Hypoglycemia and bradycardia |
| Thewissen L, 2017 [34] | Preterm neonates prenatally exposed to labetalol because of maternal HDP | n = 22 cases vs. n = 22 controls with maternal HDP without labetalol and n = 22 controls without maternal HDP | Belgium | Case–control | To investigate labetalol-induced effects on neonatal hemodynamics and cerebral oxygenation in the first 24 h after birth | Hypertensive disorders in pregnancy (HDP) | Bradycardia |
| Bateman BT, 2016 [35] | Completed pregnancies linked to liveborn infants | n = 2,292,116 | United States | Cohort study | To define the risks of neonatal hypoglycemia and bradycardia associated with maternal exposure to beta blockers at the time of delivery | Pre-existing or gestational hypertension, pre-eclampsia, migraine, cardiac arrhythmia, ischemic heart disease, anxiety and congestive heart failure | Hypoglycemia and bradycardia |
| Singh R, 2016 [36] | Women with severe hypertension in pregnancy who received labetalol or hydralazine | n = 50 cases vs. n = 50 controls | India | RCT | To evaluate the efficacy and safety of intravenous labetalol and intravenous hydralazine in managing hypertensive emergency in pregnancy | Hypertension in pregnancy | Hypoglycemia |
| Heida KY,2012 [37] | Infants from mothers suffering from severe preeclampsia and/or HELLP treated with labetalol | n = 55 cases and n = 54 controls | The Netherlands | Case–control | Analysis of possible association between intrauterine labetalol exposure and side effects | Preeclampsia and/or HELLP-syndrome | Hypoglycemia and bradycardia |
| Verma R, 2012 [38] | Pregnant patients newly diagnosed with systolic blood pressure of ≥140 mmHg and a diastolic blood pressure of ≥90 mmHg and gestational age between 20–40 weeks of pregnancy received labetalol or methyldopa | n = 45 cases vs. n = 45 controls | India | RCT | (1) To evaluate the effect of labetalol versus methyldopa on maternal outcomes in the treatment of new onset hypertension during pregnancy (2) To evaluate the effect of labetalol versus methyldopa on fetal and neonatal outcomes in the treatment of new onset hypertension during pregnancy | Pregnancy induced hypertension | Hypoglycemia and bradycardia |
| Davis RL, 2011 [39] | Women older than 15 years delivering an infant, who had been continuously enrolled with prescription drug coverage for ≥1 year prior to delivery | n = 584 cases (full-term infants exposed to beta blockers), n = 804 controls (full-term infants exposed to calcium-channel blockers) and >75,000 unexposed infants | United States | Cohort study | To study risks for perinatal complications and congenital defects among infants exposed to beta blockers in utero | Not described in article | Hypoglycemia |
| Vigil-De Gracia P, 2006 [40] | Women with severe hypertension in pregnancy treated with labetalol or hydralazine | n = 100 cases vs. n = 100 controls (and n = 103 case children vs. n = 102 control children) | Panama | RCT | To compare the safety and efficacy of intravenous labetalol and intravenous hydralazine for acutely lowering blood pressure in pregnancy | Severe preeclampsia, gestational hypertension, superimposed preeclampsia, chronic hypertension, eclampsia and severe preeclampsia with HELLP | Hypoglycemia and bradycardia |
| Darcie S, 2004 [41] | Newborns of mothers treated with atenolol, isradipine or a low sodium diet during pregnancy | n = 40 cases vs. n = 39 controls (isradipine) vs. n = 14 controls (low sodium diet) | Brazil | RCT | To evaluate the effect of isradipine on the evolution of glycemia levels in newborns of pregnant women who have arterial hypertension, comparing it to the use of atenolol and situations where the blood pressure control was done without using antihypertensive medications | Specific hypertensive disease of pregnancy (SHDP) or chronic arterial hypertension and superimposed SHDP | Hypoglycemia |
| Paran E, 1995 [42] | Woman with moderate pregnancy-induced hypertension | n = 17 cases propranolol/hydralazine vs. n = 19 cases pindolol/hydralazine vs. n = 13 controls with hydralazine | Turkey | RCT | To compare the effect of propranolol/hydralazine to pindolol/hydralazine combination therapy with hydralazine monotherapy and to evaluate the clinical effects on the mother and on the fetus | Moderate pregnancy-induced hypertension | Hypoglycemia |
| Munshi UK, 1992 [43] | Neonates born to mothers suffering from pregnancy-induced hypertension (PIH) and receiving labetalol compared to children of mothers treated with drugs other than labetalol for their PIH | n = 48 cases vs. n = 81 controls | India | Case–control | To assess the incidence of birth asphyxia, intrauterine growth retardation and hypoglycemia in the neonates of mothers suffering from pregnancy induced hypertension treated with labetalol | Pregnancy induced hypertension | Hypoglycemia and bradycardia |
| Bott-Kanner G, 1992 [44] | Women presenting with a diastolic blood pressure of 85–90 mmHg before the 35th week of pregnancy treated with pindolol or placebo | n = 30 cases vs. n = 30 controls | Israel | RCT | To investigate the benefits of early treatment of hypertension of pregnancy with pindolol and to compare the effects of initiating treatment at a DBP of 85–99 mmHg as opposed to starting treatment when DBP is ≥100 mmHg. The study examined the effects of treatment in incidence of maternal and fetal complications. | A diastolic blood pressure of 85–90 mmHg before the 35th week of pregnancy | Hypoglycemia and bradycardia |
| Pickles CJ, 1989 [45] | Patients with mild to moderate, non-proteinuric pregnancy-induced hypertension treated with labetalol or placebo | n = 70 cases vs. n = 74 controls | England | RCT | The fetal outcome of labetalol versus placebo in pregnancy-induced hypertension | Pregnancy induced hypertension: a blood pressure of 140–160 mmHg systolic and 90–105 mmHg diastolic after 15 min rest on two occasions separated by 24 h | Hypoglycemia and bradycardia |
| Ramanathan J, 1988 [28] | Woman with pre-eclampsia who were scheduled to undergo caesarean section under general anesthesia receiving labetalol pretreatmemt or no antihypertensive therapy before induction of anesthesia | n = 15 cases vs. n = 10 controls | United States | RCT | To study the effectiveness of labetalol in attenuating the hypertensive and tachycardiac responses associated with laryngoscopy and endotracheal intubation in pre-eclamptic women undergoing general anesthesia for caesarean section | Pre-eclampsia (diastolic blood pressure 96 to 120 mmHg and proteinuria) in combination with caesarean section | Hypoglycemia and bradycardia |
| Ashe RG, 1987 [46] | Primigravida’s with severe hypertension in pregnancy at 32 weeks’ gestation or more receiving labetalol or dihydrallazine | n = 10 cases vs. n = 10 controls | South Africa | RCT | To compare the efficacy of dihydralazine with labetalol when administered as intravenous infusions to primigravida’s with severe hypertension in pregnancy at 32 weeks’ gestation or more | Severe hypertension in pregnancy (a diastolic blood pressure of 110 mmHg or more (Korotkoff phase IV sound), which had not settled after 2 h bed rest and sedation with phenobarbitone (sodium gardenal 200 mg intramuscularly)) | Hypoglycemia |
| Mabie WC, 1987 [47] | Pregnant women with hypertension during pregnancy or in the puerperium receiving labetalol or hydralazine | n = 40 cases vs. n = 20 controls | United States | RCT | To compare the safety and efficacy of intravenous labetalol and intravenous hydralazine hydrochloride for acutely lowering blood pressure in the pregnant or recently postpartum patient | Pre-eclampsia and chronic hypertension with or without superimposed pre-eclampsia | Hypoglycemia and bradycardia |
| Boutroy MJ, 1986 [48] | Hypertensive mothers | n = 7 | France | Case series | To evaluate the possible risk of exposure to beta blockers of newborn infants breast-fed by mothers being treated with acebutolol | Hypertension in pregnancy | Bradycardia |
| Macpherson M, 1986 [49] | Infants born to women with hypertensive disease of pregnancy who had received labetalol for at least 7 days before delivery although some had begun treatment at 16 weeks gestation | n = 11 cases vs. n = 11 controls | England | Case–control | To examine a number of aspects of sympathetic function in infants born to labetalol-treated mothers compared with untreated controls to see if there were any clinically important effects of combined alfa and beta blockade | Hypertensive disease of pregnancy | Hypoglycemia and bradycardia |
| Högstedt S, 1985 [50] | Women with mild and moderate hypertension in pregnancy treated with metoprolol and hydralazine vs. control | n = 82 cases vs. n = 79 controls | Sweden | RCT | To assess whether treatment with metoprolol, a beta-1 selective adrenoceptor blocking agent, in combination with hydralazine is of benefit for the mother and/or the fetus as compared with non-pharmacological treatment, in mild to moderate hypertension of pregnancy | A diastolic blood pressure of at least 90 mmHg on two or more occasions during pregnancy | Hypoglycemia and bradycardia |
| Reynolds B, 1984 [51] | Women who developed hypertension in the last trimester of pregnancy received Atenolol or placebo | n = 60 cases vs. n = 60 controls | Scotland | RCT | To describe the findings of pediatric follow up to 1 year of age after the use of atenolol in pregnancy-associated hypertension | Pregnancy-associated hypertension | Bradycardia |
| Williams ER, 1983 [52] | Women with mild to moderate hypertension | n = 9 Acebutolol and n = 11 Methyldopa | England | Case–control | To compare acebutolol with methyldopa in hypertensive pregnancy | A blood pressure of 130/90 mmHg or above, a systolic pressure of 135 mmHg or above or a diastolic pressure of 85 mmHg or above | Hypoglycemia and bradycardia |
| Rubin PC, 1983 [53] | Women with mild to moderate pregnancy-associated hypertension who were also initially managed conventionally by bed rest received atenolol or placebo | n = 46 cases vs. n = 39 controls | Scotland | RCT | To examine the efficacy and safety of atenolol in the treatment of pregnancy-associated hypertension | Pregnancy-associated hypertension: a blood-pressure between 140 and 170 mmHg systolic or between 90 and 110 mmHg diastolic (after 10 mins’ rest supine or after 5 mins’ standing) on two occasions separated by 24 h | Hypoglycemia and bradycardia |
| Liedholm H, 1983 [54] | Hypertensive pregnancies | n = 88 cases vs. n = 22 controls | Sweden | Cohort study | To determine the effects of atenolol and metoprolol on maternal blood pressure and on the fetus and new-born | Chronic or pregnancy-related hypertension | Hypoglycemia |
| Liedholm H, 1983 [27] | Pregnant women under treatment with atenolol for hypertension (during pregnancy or in the peripartum) | n = 7 | Sweden | Case series | To investigate atenolol’s ability to cross the human placental barrier and to study the excretion of atenolol in breast milk. | Hypertension in pregnancy | Bradycardia |
| Livingstone I, 1983 [55] | Pregnancy-associated hypertension treated with propranolol or methyldopa | n = 14 cases and n = 14 controls | Australia | RCT | To compare propranolol with methyldopa in hypertensive pregnancy | A blood pressure of 140/90 or above, on two consecutive readings at least twenty-four hours apart. | Hypoglycemia and bradycardia |
| Dubois D, 1983 [26] | High-risk pregnancies with hypertension using beta blockers | n = 125 | France | Case series | To investigate the outcome of beta blocker use in high-risk pregnancies | Hypertension in pregnancy | Hypoglycemia |
| Boutroy MJ, 1982 [56] | Children born from hypertensive pregnant women treated with acebutolol | n = 31 | France | Case series | To determine the pharmacokinetics of acebutolol in the mother, as well as its placental transfer, and the pharmacokinetics in the fetus | Chronic or pregnancy-associated hypertension, after failure of strict bed rest and methyldopa with or without hydralazine | Bradycardia |
| Rubin PC, 1982 [57] | Infants of women using atenolol for management of essential hypertension in pregnancy | n = 9 | Scotland | Case series | To report the experience of using atenolol for several weeks during pregnancy in the management of essential hypertension | Systolic blood pressure exceeding 140 mmHg or diastolic pressure exceeding 90 mmHg on two separate occasions at least one day apart | Hypoglycemia and bradycardia |
| Sandström B, 1982 [58] | Pregnant women with hypertension treated with metoprolol combined with thiazide or hydralazine compared with women treated with hydralazine and a thiazide | n = 184 cases (n = 101 with thiazide and n = 83 with hydralazine and n = 97 controls | Sweden | Case–control | To report further experiences of using metoprolol in hypertension of pregnancy. (In addition to a previous study) | Pregnancy-induced hypertension, pre-existing hypertension, eclampsia and hypertension with moderate/marked proteinuria | Hypoglycemia and bradycardia |
| Garden A, 1982 [59] | Women with severe hypertension in pregnancy treated with labetalol or dihydralazine | n = 3 cases vs. n = 3 controls | South Africa | RCT | To compare the effect of labetalol and dihydralazine in increasing doses in woman with severe hypertension in pregnancy | Severe hypertension and imminent eclampsia or eclampsia | Bradycardia |
| Dumez Y, 1981 [60] | Infants born to mothers who received acebutolol or methyldopa during pregnancy | n = 10 cases vs. n = 10 controls | France | Case–control | To evaluate any deleterious effect of the beta-adrenergic-blocking agent in newborn infants. | If the diastolic blood pressure exceeded 90 mm Hg on two occasions at least 24 h apart during pregnancy | Hypoglycemia and bradycardia |
| Bott-Kanner G, 1980 [61] | Infants of mothers treated with propranolol and hydralazine because of longstanding hypertension during pregnancy | n = 14 | Israel | Case series | To assess the efficiency of a combination of hydralazine and propranolol in the management of pregnant patients with essential hypertension | Essential hypertension | Hypoglycemia |
| O’Hare MF, 1980 [62] | Hypertensive pregnant women receiving sotalol | n = 12 | Northern Ireland | Case series | To study the effects and distribution of sotalol by administering it as sole therapy to a group of chronically hypertensive pregnant women. | Chronic or pregnancy-induced hypertension | Hypoglycemia and bradycardia |
| Gallery ED, 1979 [63] | Pregnant women with moderately severe hypertension treated with oxprenolol or methyldopa | n = 26 cases vs. n = 27 controls | Australia | RCT | To examine the effects of antihypertensive treatment more closely and to evaluate alternative forms of treatment | Moderately severe hypertension in pregnancy | Hypoglycemia |
| Pruyn SC, 1979 [64] | Infants from mothers who used propranolol chronically during pregnancy | n = 12 | United States | Case series | To examine maternal, fetal and neonatal complications of propranolol therapy in pregnancy | Thyrotoxicosis, hypertension, Barlow syndrome with arrhythmia, Lown-Ganong-Levine syndrome and supraventricular/paroxysmal atrial tachycardia | Hypoglycemia and bradycardia |
| Eliahou HE, 1978 [65] | Infants from mothers treated with propranolol during pregnancy | n = 22 | Israel | Case series | To report the experience of 25 women who received propranolol orally for the treatment of hypertension during 26 pregnancies with 22 liveborn infants | Essential hypertension, recurrent hypertension of pregnancy, pre-eclampsia and unilateral chronic pyelonephritis | Hypoglycemia |
3.2. Risk of Bias Assessment
3.2.1. RCTs
3.2.2. Non-RCTs
3.3. Bradycardia
3.3.1. Beta-Blocker vs. Control Group without a Beta-Blocker
3.3.2. Beta-Blocker vs. Placebo
3.3.3. Beta-Blocker vs. Methyldopa
| Article | Study Groups | Bradycardia | Heart Rate (Beats per Minute) | Definition of Bradycardia | Time of Control of Bradycardia |
|---|---|---|---|---|---|
| Kayser A, 2020 [30] | ß-blocker vs. methyldopa ß-blocker vs. non-hypertensive mother | 5/252 (2.0%) vs. 5/199 (2.5%) (NS) 5/252 (2.0%) vs. 5/588 (0.8%) (NS) | Diagnosis of bradycardia was retrieved from medical reports | N | |
| Mazkereth R, 2019 [32] | ß-blocker vs. control | 6/153 (3.9%) vs. 0/153 (0%) p = 0.030 | Heart rate < 100 bpm | In the first 48 h after birth | |
| Easterling T, 2019 [33] | Labetalol vs. nifedipine Labetalol vs. methyldopa | 0/280 (0%) vs. 0/297 (0%) 0/280 (0%) vs. 0/298 (0%) | Heart rate < 110 bpm | N | |
| Thewissen L, 2017 [34] | Labetalol vs. control | 0/22 vs. 0/22 vs. 0/22 | N | In the first 24 h after birth | |
| Bateman BT, 2016 [35] | ß-blocker vs. control Labetalol vs. control Metoprolol vs. control Atenolol vs. control Propensity-score 1 corrected available | 165/10,585 (1.6%) vs. 11,659/2,281,531 (0.5%) 124/6748 (1.8%) vs. 11,659/2,281,531 (0.5%) 12/1485 (0.8%) vs. 11,659/2,281,531 (0.5%) 12/1121 (1.1%) vs. 11,659/2,281,531 (0.5%) | Heart rate ≤ 100 bpm | N | |
| Heida KY, 2012 [37] | Labetalol vs. control Labetalol i.v. vs. labetalol oral | 4/55 (7.3%) vs. 1/54 (1.9%) p = 0.18 5.4 vs 11.1% p = 0.39 | Heart rate < 100 bpm | In the first minutes after birth and during the first 48 h | |
| Verma R, 2012 [38] | Labetalol vs. methyldopa | 1/45 (2.22%) vs. 0/45 (0%) (NS) | N | N | |
| Vigil-De Gracia P, 2006 [40] | Labetalol vs. hydralazine | 11/103 (10.6%) vs. 2/102 (1.9%) (p = 0.008) | Heart rate < 110 bpm | N | |
| Munshi UK, 1992 [43] | Labetalol vs. control | 6/48 (12.5%) vs 4/81 (5%) (NS) | Heart rate < 100 bpm | At 5-min as part of Apgar scoring | |
| Bott-Kanner G, 1992 [44] | Pindolol vs. placebo | 2 | Heart rate < 100 bpm | During the first 24 h after birth | |
| Pickles CJ, 1989 [45] | Labetalol vs. placebo | 4/70 (5.7%) vs. 4/74 (5.4%) | Heart rate < 120 bpm | At five minutes | |
| Ramanathan J, 1988 [28] | Labetalol vs. control | 0/15 (0%) vs. 0/10 (0%) | 138.2 ± 2.5 vs. 144 ± 3.2 (NS) | N | During 10–20 min after birth and thereafter for 12 to 24 h |
| Mabie WC, 1987 [47] | Labetalol vs. hydralazine | 0/13 (0%) vs. 0/6 (0%) | Heart rate < 110 bpm | N | |
| Macpherson M, 1986 [49] | Labetalol vs. control | No difference between the two groups | N | At 2, 4, 8,16, 24, 48 and 72 h after birth | |
| Boutroy MJ, 1986 [48] | 3 | ||||
| Högstedt S, 1985 [50] | Metoprolol and hydralazine vs. control (intended-to-treat) 4 Metoprolol and hydralazine vs. control (cause–effect) | 1/82 (1.2%) vs. 4/79 (5.1%) 1/69 (1.4%) vs. 3/66 (4.5%) | N | N | |
| Reynolds B, 1984 [51] | 5 | ||||
| Williams ER, 1983 [52] | Acebutolol vs. methyldopa | 0/9 vs. 0/11 | N | N | |
| Rubin PC, 1983 [53] | Atenolol vs. placebo | 18/46 (39.1%) vs. 4/39 (10.3%) (p < 0.01) | Heart rate < 120 bpm | Continuously recorded in the first 24 h after birth | |
| Liedholm H, 1983 [27] | Atenolol (no control group) | 6 | N | N | |
| Livingstone I, 1983 [55] | Propranolol vs. methyldopa | 0/14 (0%) vs. 0/14 (0%) | N | During 48 h after birth | |
| Boutroy MJ, 1982 [56] | Acebutolol (no control group) | 12/31 (38.7%) | Basal heart rate < 120 beats per minute and lasting longer than 1 h | During 72 h after birth | |
| Sandström B, 1982 [58] | Bendroflumethiazide + metoprolol vs. metoprolol + hydralazine vs. Bendroflumethiazide + hydralazine | 7/101 vs. 1/83 vs. 16/97 (8/184 vs. 16/97) | Heart rate < 100 bpm | At birth | |
| Garden A, 1982 [59] | Labetalol vs. hydralazine | 3/3 (100%) vs. 0/3 (0%) | Heart rate < 100 bpm | Immediately after birth | |
| Rubin PC, 1982 [57] | Atenolol (no control group) | 0/9 (0%) | Heart rate < 120 bpm | During 24 h after birth | |
| Dumez Y, 1981 [60] | Acebutolol vs. methyldopa | Day 1: 118 ± 19 vs. 132 ± 9 (p < 0.05) Day 2: 123 ± 18 vs. 139 ± 10 (p < 0.05) Day 3: 126 ± 21 vs. 148 ± 12 (p < 0.02) | N | Daily during the 3 first days after birth, when the babies were sleeping | |
| O’Hare MF, 1980 [62] | Sotalol (no control group) | 6/12 (50%) | Heart rate < 120 bpm | Four-hourly for at least 24 h | |
| Pruyn SC, 1979 [64] | Propranolol (no control group) | 1/12 (8.3%) | N | N |
3.3.4. Beta-Blocker vs. Hydralazine
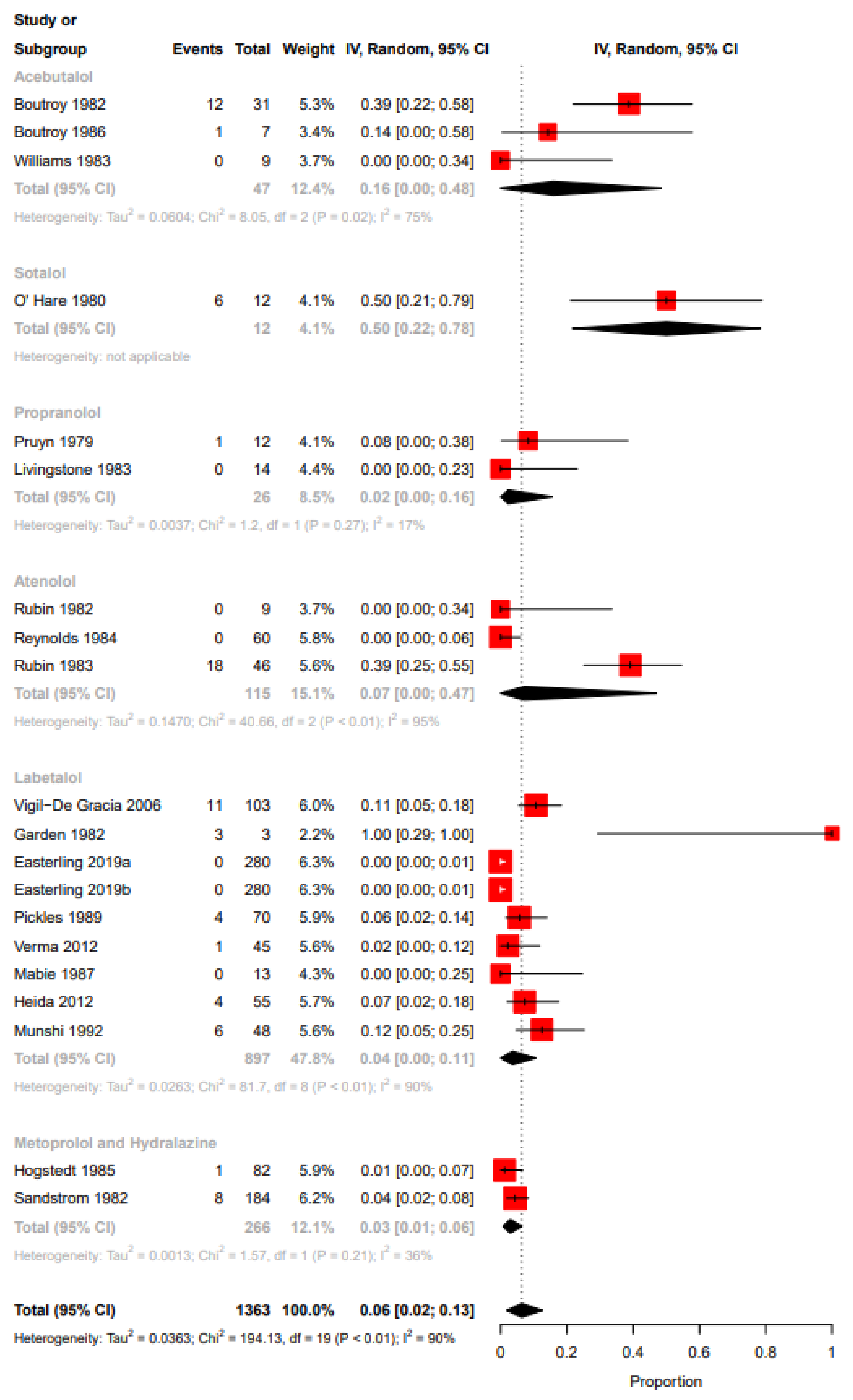
3.3.5. No Control Group
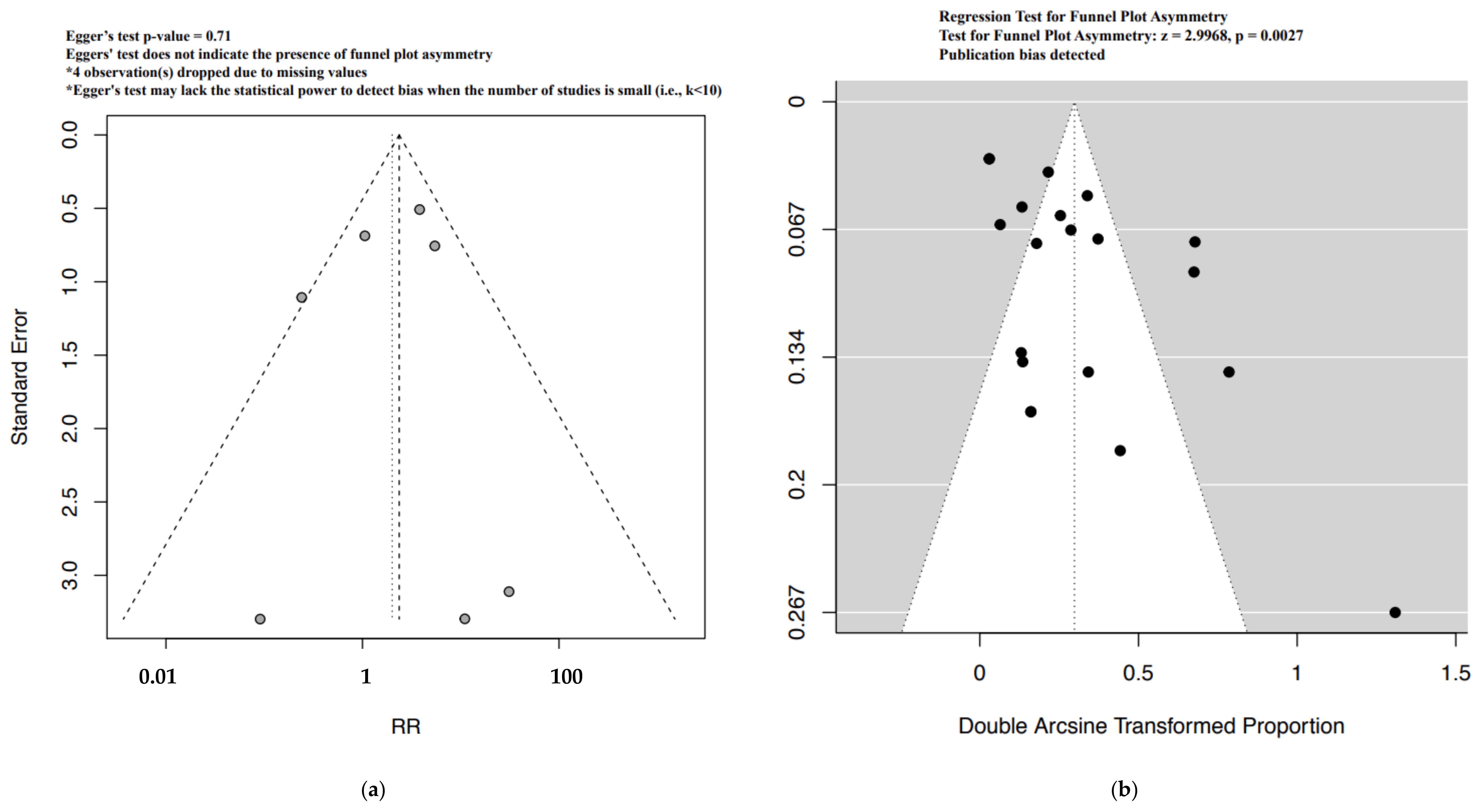
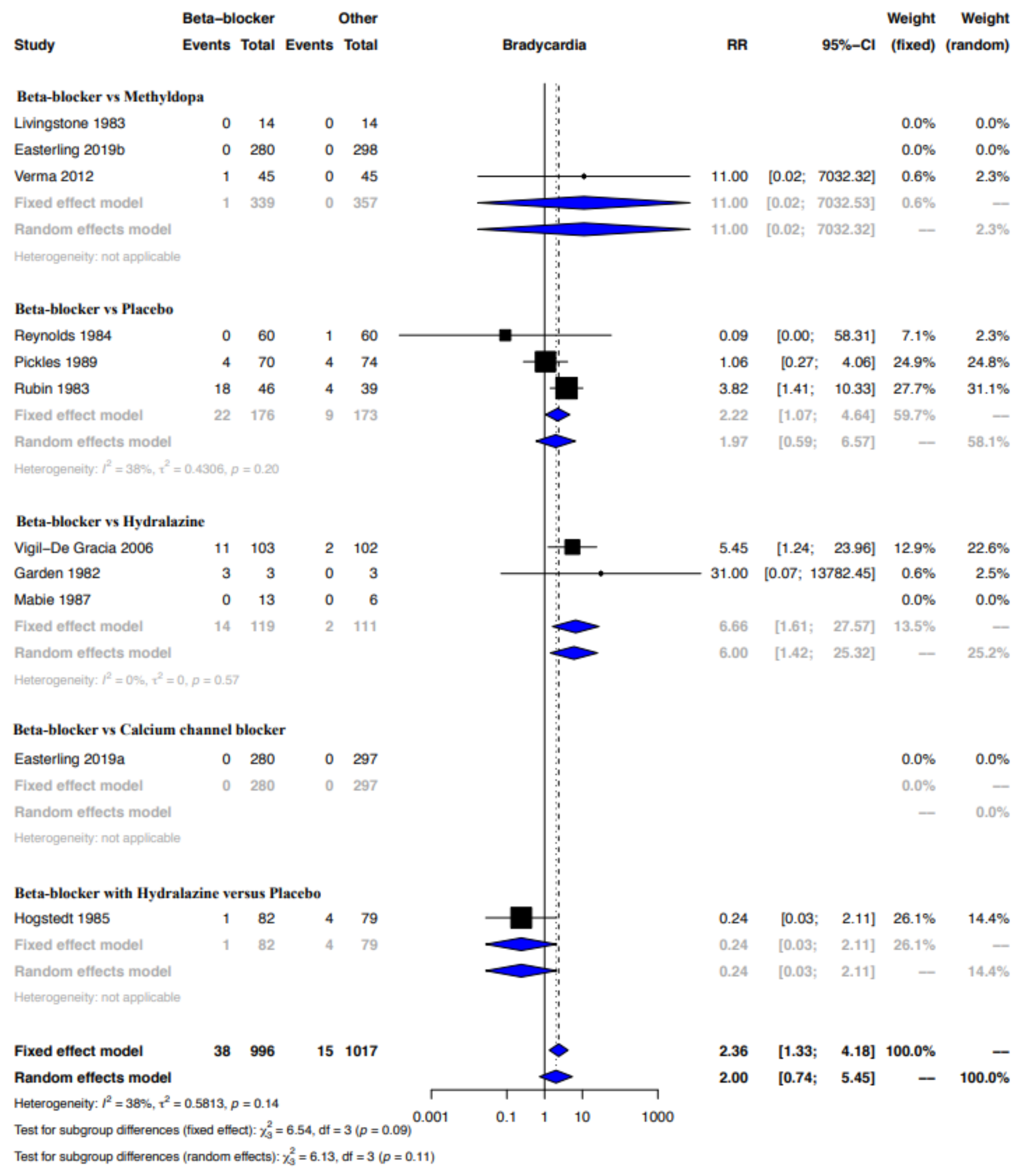
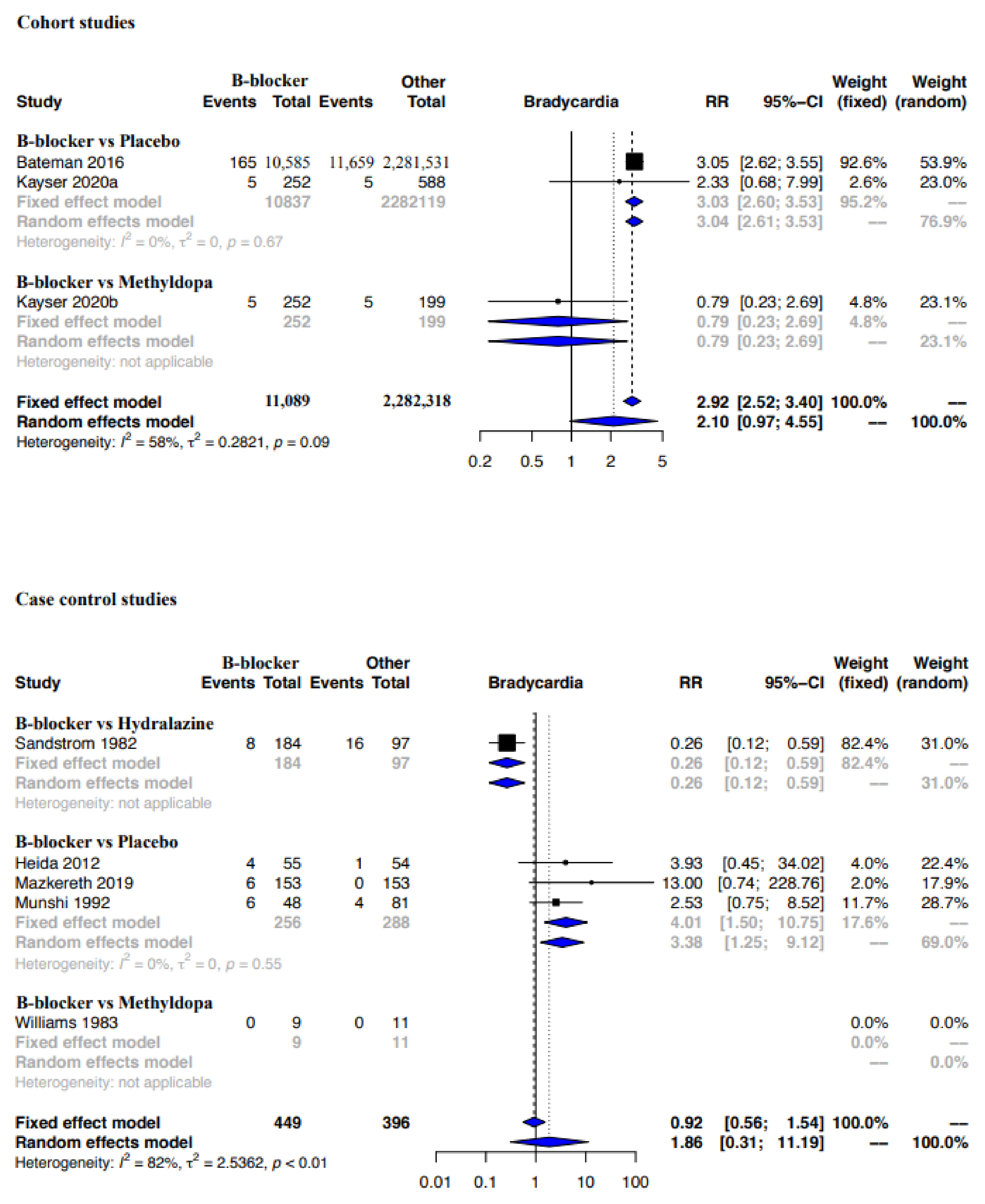
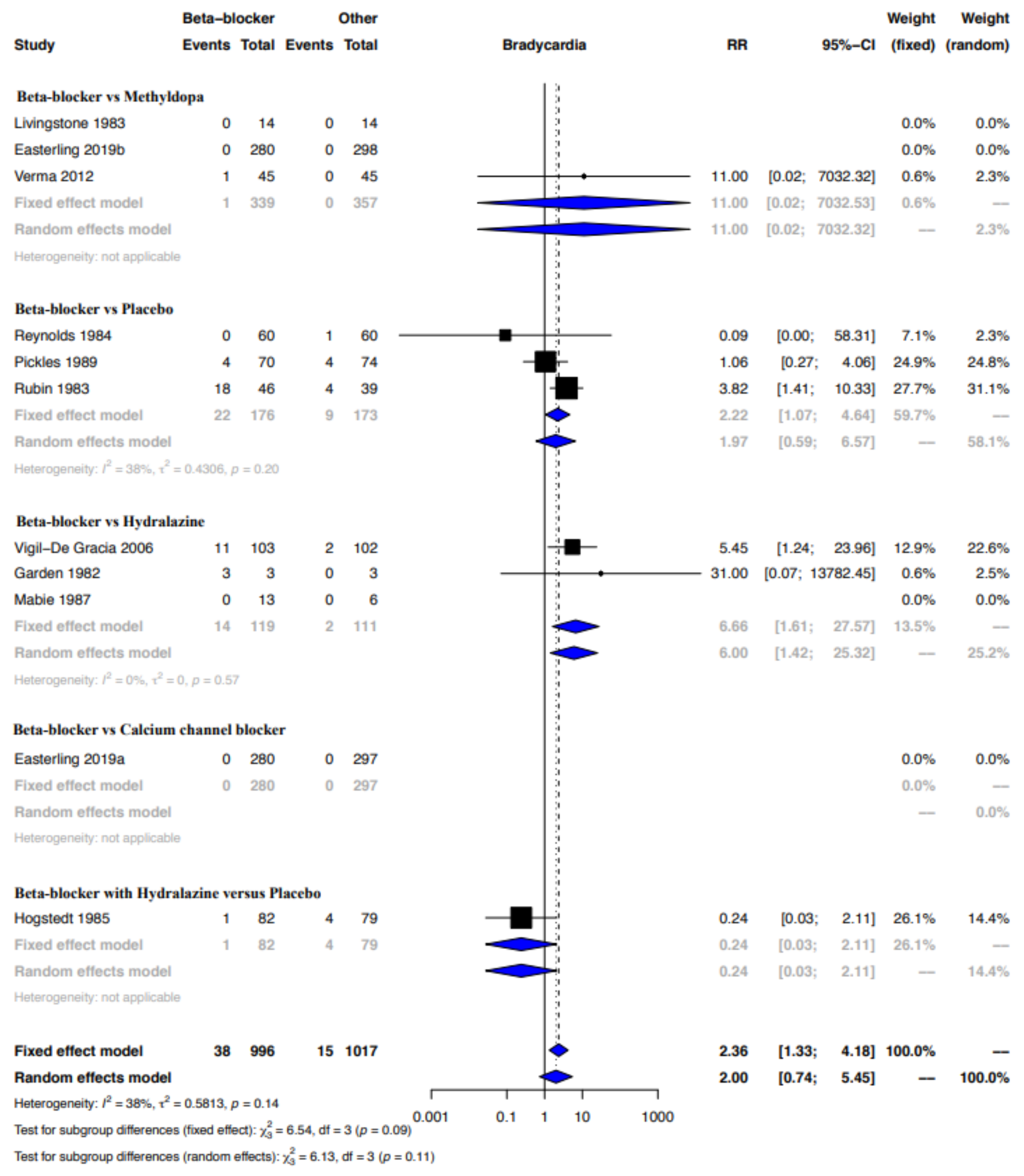
3.3.6. Meta-Analyses for the Outcome Bradycardia
3.4. Hypoglycemia
3.4.1. Beta-Blocker vs. Control Group without a Beta-Blocker
3.4.2. Beta-Blocker vs. Placebo
3.4.3. Beta-Blocker vs. Methyldopa
3.4.4. Beta-Blocker vs. Hydralazine
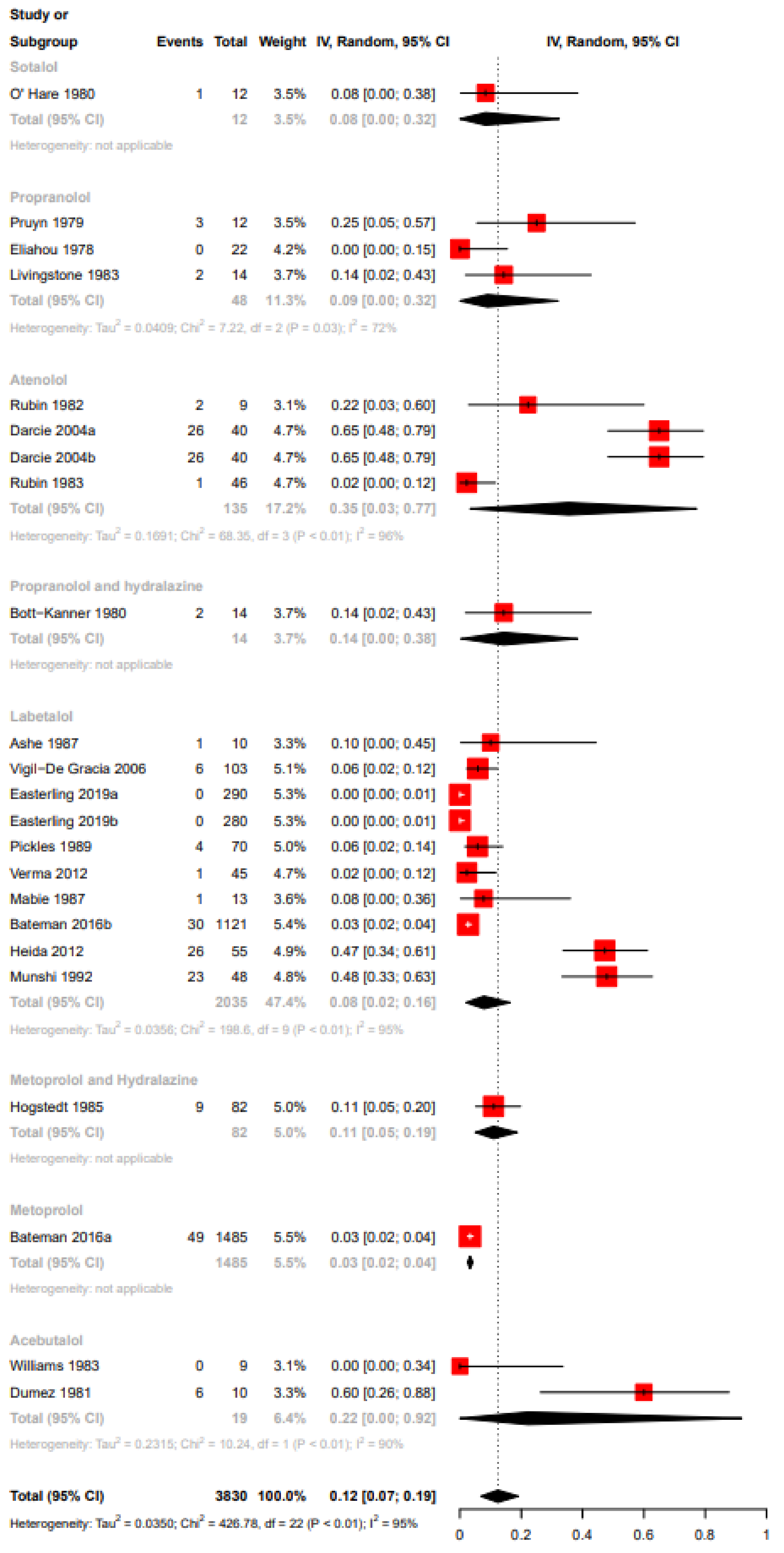
3.4.5. No Control Group
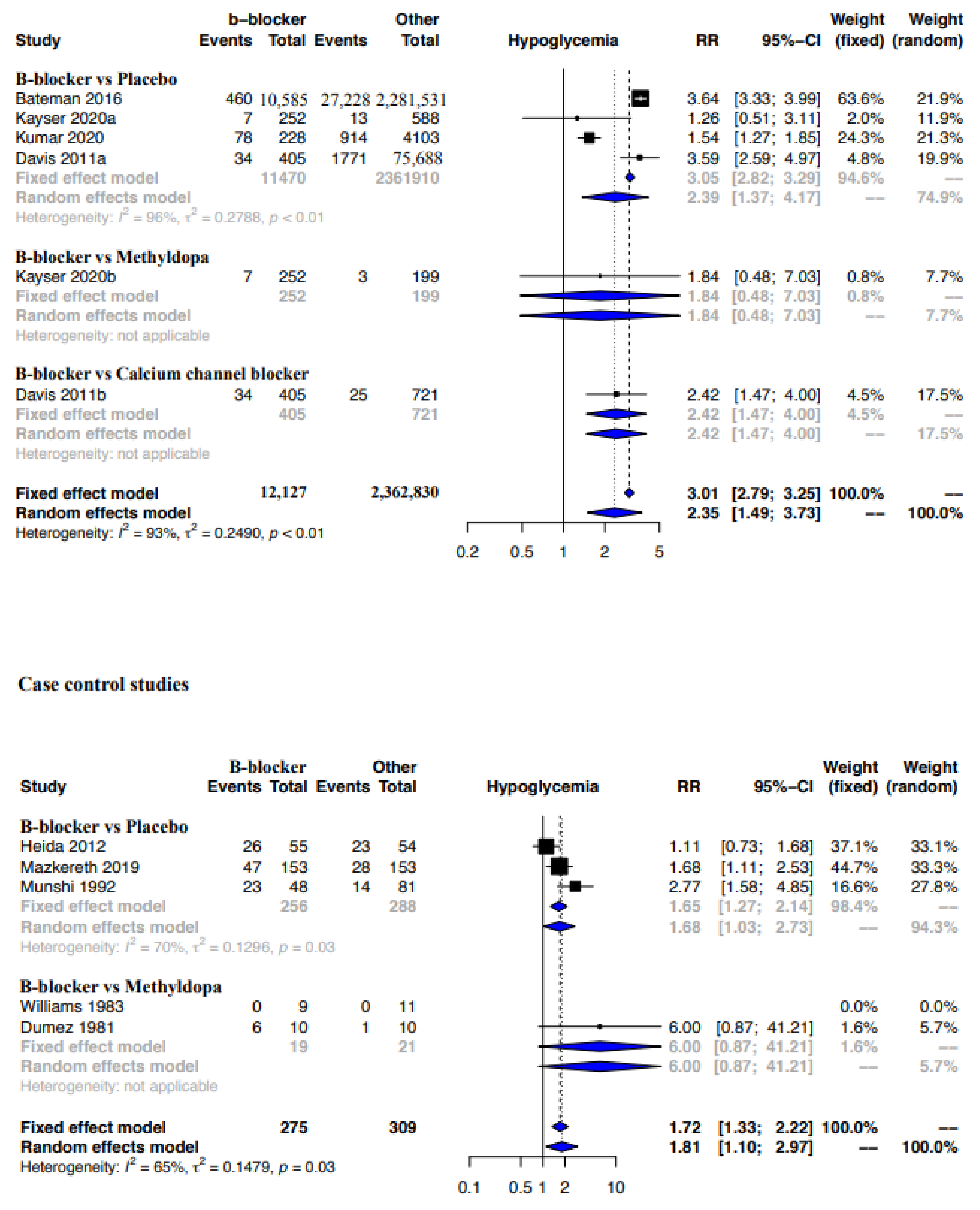
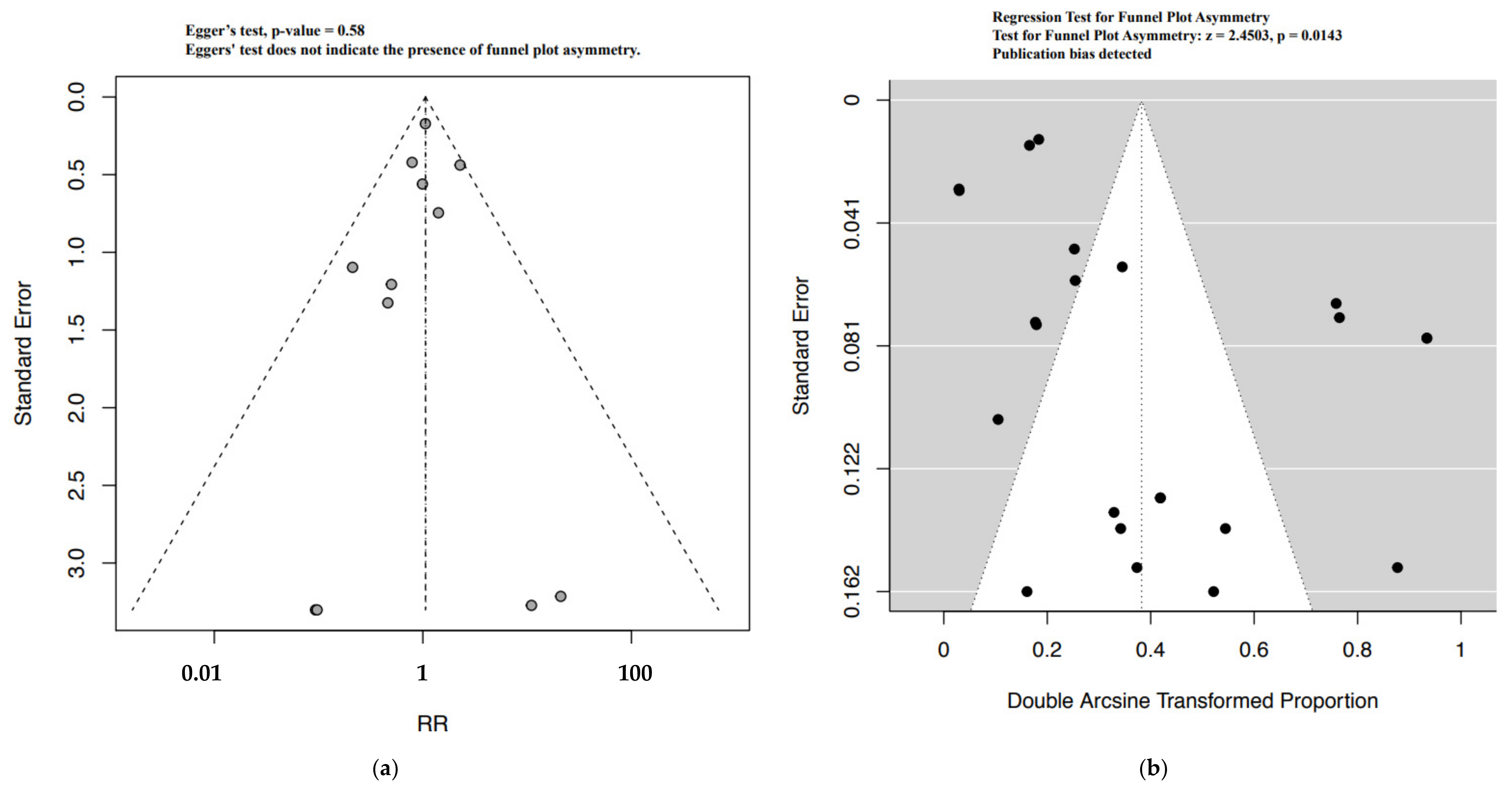
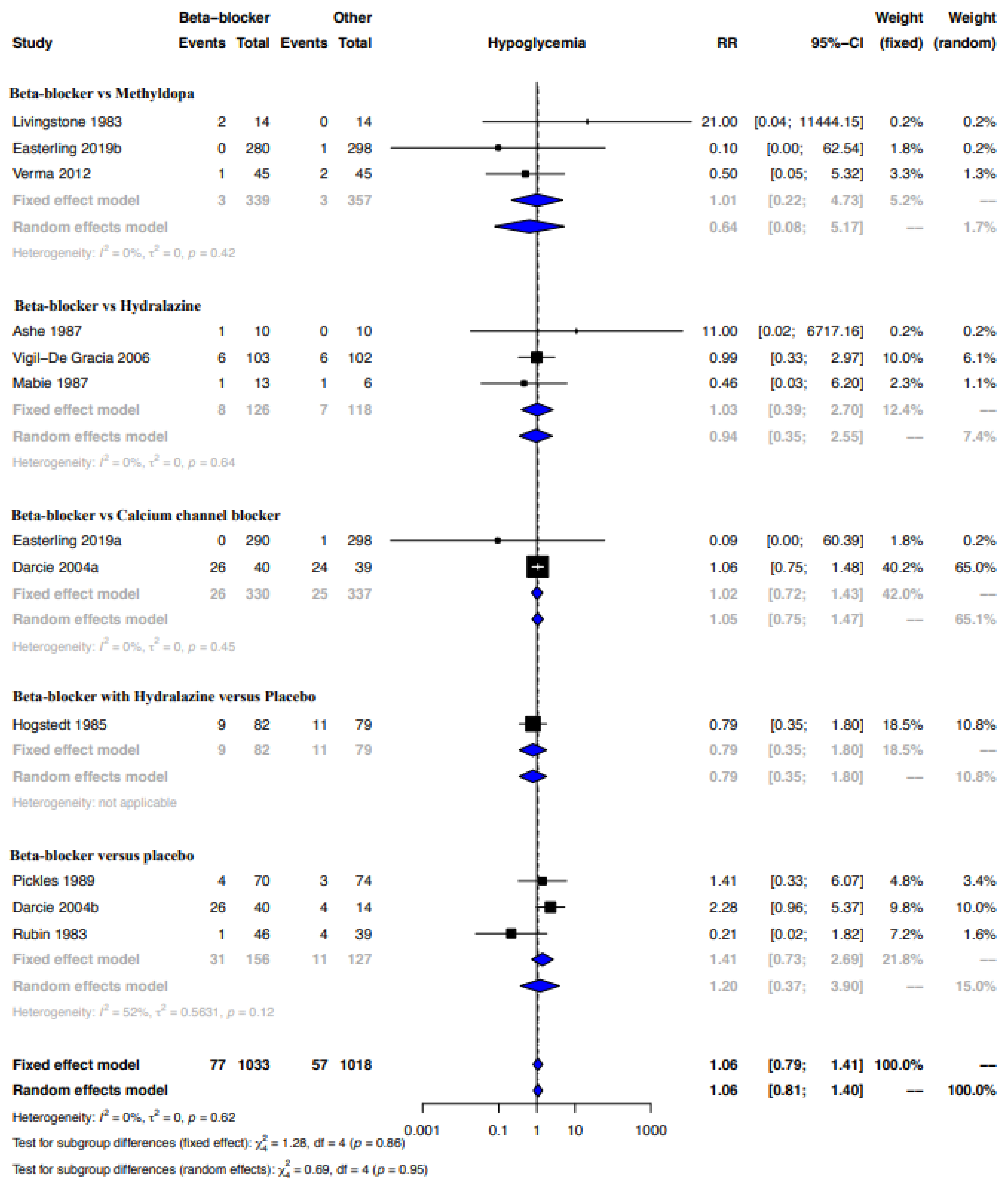
3.4.6. Meta-Analyses for the Outcome Hypoglycemia
3.5. Lactation
3.6. Case Reports
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cea Soriano, L.; Bateman, B.T.; García Rodríguez, L.A.; Hernández-Díaz, S. Prescription of antihypertensive medications during pregnancy in the UK. Pharmacoepidemiol. Drug Saf. 2014, 23, 1051–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, H.; Proegler, M. Placental transfer of beta-adrenergic antagonists studied in an in vitro perfusion system of human placental tissue. Am. J. Obstet. Gynecol. 1988, 159, 42–47. [Google Scholar] [CrossRef]
- Erkkola, R.; Lammintausta, R.; Liukko, P.; Anttila, M. Transfer of propranolol and sotalol across the human placenta. Their effect on maternal and fetal plasma renin activity. Acta Obstet. Gynecol. Scand. 1982, 61, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Bateman, B.T.; Heide-Jørgensen, U.; Einarsdóttir, K.; Engeland, A.; Furu, K.; Gissler, M.; Hernandez-Diaz, S.; Kieler, H.; Lahesmaa-Korpinen, A.M.; Mogun, H.; et al. β-Blocker Use in Pregnancy and the Risk for Congenital Malformations: An International Cohort Study. Ann. Intern. Med. 2018, 169, 665–673. [Google Scholar] [CrossRef]
- Duan, L.; Ng, A.; Chen, W.; Spencer, H.T.; Nguyen, J.; Shen, A.Y.; Lee, M.S. β-Blocker Exposure in Pregnancy and Risk of Fetal Cardiac Anomalies. JAMA Intern. Med. 2017, 177, 885–887. [Google Scholar] [CrossRef] [Green Version]
- Kaye, A.B.; Bhakta, A.; Moseley, A.D.; Rao, A.K.; Arif, S.; Lichtenstein, S.J.; Aggarwal, N.T.; Volgman, A.S.; Sanghani, R.M. Review of Cardiovascular Drugs in Pregnancy. J. Womens Health 2019, 28, 686–697. [Google Scholar] [CrossRef]
- Shannon, M.E.; Malecha, S.E.; Cha, A.J. Beta blockers and lactation: An update. J. Hum. Lact. 2000, 16, 240–245. [Google Scholar] [CrossRef]
- Lunell, N.O.; Kulas, J.; Rane, A. Transfer of labetalol into amniotic fluid and breast milk in lactating women. Eur. J. Clin. Pharmacol. 1985, 28, 597–599. [Google Scholar] [CrossRef]
- Smith, M.T.; Livingstone, I.; Hooper, W.D.; Eadie, M.J.; Triggs, E.J. Propranolol, propranolol glucuronide, and naphthoxylactic acid in breast milk and plasma. Ther. Drug Monit. 1983, 5, 87–93. [Google Scholar] [CrossRef]
- Lwin, E.M.P.; Gerber, C.; Leggett, C.; Song, Y.; Ritchie, U.; Turner, S.; Hague, W.; Upton, R.; Garg, S. Estimation of Atenolol Transfer Into Milk and Infant Exposure During Its Use in Lactating Women. J. Hum. Lact. 2018, 34, 592–599. [Google Scholar] [CrossRef]
- Farmacotherapeutisch Compas. Bètablokkers, Systemisch. Available online: https://www.farmacotherapeutischkompas.nl/bladeren/groepsteksten/betablokkers__systemisch (accessed on 5 October 2021).
- Stomnaroska, O.; Petkovska, E.; Jancevska, S.; Danilovski, D. Neonatal Hypoglycemia: Risk Factors and Outcomes. Pril. (Makedon. Akad. Nauk. Umet. Odd. Med. Nauki.) 2017, 38, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Burns, C.M.; Rutherford, M.A.; Boardman, J.P.; Cowan, F.M. Patterns of cerebral injury and neurodevelopmental outcomes after symptomatic neonatal hypoglycemia. Pediatrics 2008, 122, 65–74. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. Bmj 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. Bmj 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.M.Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; Mu, P.-F. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Schünemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef]
- Santesso, N.; Glenton, C.; Dahm, P.; Garner, P.; Akl, E.A.; Alper, B.; Brignardello-Petersen, R.; Carrasco-Labra, A.; De Beer, H.; Hultcrantz, M.; et al. GRADE guidelines 26: Informative statements to communicate the findings of systematic reviews of interventions. J. Clin. Epidemiol. 2020, 119, 126–135. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 10 March 2022).
- Bansal, S.; Pawar, M. Haemodynamic responses to laryngoscopy and intubation in patients with pregnancy-induced hypertension: Effect of intravenous esmolol with or without lidocaine. Int. J. Obstet. Anesth. 2002, 11, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Molvi, S.N.; Mir, S.; Rana, V.S.; Jabeen, F.; Rauoof Malik, A. Role of antihypertensive therapy in mild to moderate pregnancy-induced hypertension: A prospective randomized study comparing labetalol with alpha methyldopa. Arch. Gynecol. Obstet. 2012, 285, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Dubois, D.; Petitcolas, J.; Temperville, B. Beta blocker therapy in 125 cases of hypertension during pregnancy. Clin. Exp. Hypertension. Part B Hypertens. Pregnancy 1983, 2, 41–59. [Google Scholar] [CrossRef] [PubMed]
- Liedholm, H. Transplacental passage and breast milk accumulation of atenolol in humans. Drugs 1983, 25, 217–218. [Google Scholar] [CrossRef]
- Ramanathan, J.; Sibai, B.M.; Mabie, W.C.; Chauhan, D.; Ruiz, A.G. The use of labetalol for attenuation of the hypertensive response to endotracheal intubation in preeclampsia. Am. J. Obstet. Gynecol. 1988, 159, 650–654. [Google Scholar] [CrossRef]
- Bigelow, C.A.; Pan, S.; Overbey, J.R.; Stone, J. Propranolol for Induction of Labor in Nulliparas trial a double-blind, randomized, placebo-controlled trial. American J. Obstet. Gynecol. MFM 2021, 3, 100301. [Google Scholar] [CrossRef]
- Kayser, A.; Beck, E.; Hoeltzenbein, M.; Zinke, S.; Meister, R.; Weber-Schoendorfer, C.; Schaefer, C. Neonatal effects of intrauterine metoprolol/bisoprolol exposure during the second and third trimester: A cohort study with two comparison groups. J. Hypertens. 2020, 38, 354–361. [Google Scholar] [CrossRef]
- Kumar, N.; Kumar, P.; Harris, N.; Monga, R.; Sampath, V. Impact of Maternal HbA1c Levels ≤6% and Race in Nondiabetic Pregnancies on Birthweight and Early Neonatal Hypoglycemia. J. Pediatr. 2020, 227, 121–127.e123. [Google Scholar] [CrossRef]
- Mazkereth, R.; Maayan-Metzger, A.; Leibovitch, L.; Schushan-Eisen, I.; Morag, I.; Straus, T. Short-term neonatal outcome among term infants after in-utero exposure to beta blockers. Isr. Med. Assoc. J. 2019, 21, 724–727. [Google Scholar]
- Easterling, T.; Mundle, S.; Bracken, H.; Parvekar, S.; Mool, S.; Magee, L.A.; von Dadelszen, P.; Shochet, T.; Winikoff, B. Oral antihypertensive regimens (nifedipine retard, labetalol, and methyldopa) for management of severe hypertension in pregnancy: An open-label, randomised controlled trial. Lancet 2019, 394, 1011–1021. [Google Scholar] [CrossRef] [Green Version]
- Thewissen, L.; Pistorius, L.; Baerts, W.; Naulaers, G.; Van Bel, F.; Lemmers, P. Neonatal haemodynamic effects following foetal exposure to labetalol in hypertensive disorders of pregnancy. J. Matern.-Fetal Neonatal Med. 2017, 30, 1533–1538. [Google Scholar] [CrossRef] [Green Version]
- Bateman, B.T.; Patorno, E.; Desai, R.J.; Seely, E.W.; Mogun, H.; Maeda, A.; Fischer, M.A.; Hernandez-Diaz, S.; Huybrechts, K.F. Late pregnancy β blocker exposure and risks of neonatal hypoglycemia and bradycardia. Pediatrics 2016, 138, e20160731. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Singh, S.; Singh, S.; Agarwal, M.; Anand, S.; Yadav, N.K. Comparative study of efficacy and safety of intravenous labetalol and intravenous hydralazine in managing hypertensive emergencies in pregnancy. J Safog. 2016, 8, 185–188. [Google Scholar] [CrossRef] [Green Version]
- Heida, K.Y.; Zeeman, G.G.; Van Veen, T.R.; Hulzebos, C.V. Neonatal side effects of maternal labetalol treatment in severe preeclampsia. Early Hum. Dev. 2012, 88, 503–507. [Google Scholar] [CrossRef]
- Verma, R.; Lahon, K.; Tonpay, S.D.; Kale, V.J. A comparative randomised controlled parallel group study of maternal, fetal and neonatal outcomes of labetalol versus methyldopa in the treatment of new onset hypertension during pregnancy. Int. J. Pharma. Bio. Sci. 2012, 3, P201–P211. [Google Scholar]
- Davis, R.L.; Eastman, D.; McPhillips, H.; Raebel, M.A.; Andrade, S.E.; Smith, D.; Yood, M.U.; Dublin, S.; Platt, R. Risks of congenital malformations and perinatal events among infants exposed to calcium channel and beta-blockers during pregnancy. Pharmacoepidemiol. Drug Saf. 2011, 20, 138–145. [Google Scholar] [CrossRef]
- Vigil-De Gracia, P.; Lasso, M.; Ruiz, E.; Vega-Malek, J.C.; de Mena, F.T.; López, J.C. Severe hypertension in pregnancy: Hydralazine or labetalol. A randomized clinical trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 128, 157–162. [Google Scholar] [CrossRef]
- Darcie, S.; Leone, C.R.; Calil, V.M.; Prescinotti, E.P.; Kahhale, S.; Zugaib, M. Glycemia in newborns of hypertensive mothers according to maternal treatment. Rev. Hosp Clin. 2004, 59, 244–250. [Google Scholar] [CrossRef]
- Paran, E.; Holzberg, G.; Mazor, M.; Zmora, E.; Insler, V. β-adrenergic blocking agents in the treatment of pregnancy-induced hypertension. Int. J. Clin. Pharmacol. Ther. 1995, 33, 119–123. [Google Scholar]
- Munshi, U.K.; Deorari, A.K.; Paul, V.K.; Singh, M. Effects of maternal labetalol on the newborn infant. Indian Pediatr. 1992, 29, 1507–1512. [Google Scholar]
- Bott-Kanner, G.; Hirsch, M.; Friedman, S.; Boner, G.; Ovadia, J.; Merlob, P.; Mor, N.; Modan, M.; Galai, N.; Rosenfeld, J.B. Antihypertensive therapy in the management of hypertension in pregnancy: A clinical double-blind study of pindolol. Clin. Exp. Hypertension. Part B Hypertens. Pregnancy 1992, 11, 207–220. [Google Scholar] [CrossRef]
- Pickles, C.J.; Symonds, E.M.; Broughton Pipkin, F. The fetal outcome in a randomized double-blind controlled trial of labetalol versus placebo in pregnancy-induced hypertension. Br. J. Obstet. Gynaecol. 1989, 96, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ashe, R.G.; Moodley, J.; Richards, A.M.; Philpott, R.H. Comparison of labetalol and dihydrallazine in hypertensive emergencies of pregnancy. S. Afr. Med. J. 1987, 71, 354–356. [Google Scholar] [PubMed]
- Mabie, W.C.; Gonzalez, A.R.; Sibai, B.M.; Amon, E. A comparative trial of labetalol and hydralazine in the acute management of severe hypertension complicating pregnancy. Obstet. Gynecol. 1987, 70, 328–333. [Google Scholar]
- Boutroy, M.J.; Bianchetti, G.; Dubruc, C. To nurse when receiving acebutolol: Is it dangerous for the neonate? Eur. J. Clin. Pharmacol. 1986, 30, 737–739. [Google Scholar] [CrossRef]
- Macpherson, M.; Broughton Pipkin, F.; Rutter, N. The effect of maternal labetalol on the newborn infant. Br. J. Obstet. Gynaecol. 1986, 93, 539–542. [Google Scholar] [CrossRef]
- Hogstedt, S.; Lindeberg, S.; Axelsson, O. A prospective controlled trial of metoprolol–Hydralazine treatment in hypertension during pregnancy. Acta Obstet. Gynecol. Scand. 1985, 64, 505–510. [Google Scholar] [CrossRef]
- Reynolds, B.; Butters, L.; Evans, J. First year of life after the use of atenolol in pregnancy associated hypertension. Arch. Dis. Child. 1984, 59, 1061–1063. [Google Scholar] [CrossRef]
- Williams, E.R.; Morrissey, J.R. A comparison of acebutolol with methyldopa in hypertensive pregnancy. Pharmatherapeutica 1983, 3, 487–491. [Google Scholar]
- Rubin, P.C.; Clark, D.M.; Butters, L. Placebo controlled trial of atenolol in treatment of pregnancy associated hypertension. Lancet 1983, 1, 431–434. [Google Scholar]
- Liedholm, H. Atenolol in the treatment of hypertension of pregnancy. Drugs 1983, 25, 206–211. [Google Scholar] [CrossRef]
- Livingstone, I.; Craswell, P.W.; Bevan, E.B. Propranolol in pregnancy three year prospective study. Clin. Exp. Hypertension. Part B Hypertens. Pregnancy 1983, 2, 341–350. [Google Scholar] [CrossRef]
- Boutroy, M.J.; Vert, P.; Bianchetti, G.; Dubrucq, C.; Morselli, P.L. Infants born to hypertensive mothers treated by acebutolol. Pharmacological studies in the perinatal period. Dev. Pharmacol. Ther. 1982, 4, 109–115. [Google Scholar] [CrossRef]
- Rubin, P.C.; Butters, L.; Low, R.A.; Reid, J.L. Atenolol in the treatment of essential hypertension during pregnancy. Br. J. Clin. Pharmacol. 1982, 14, 279–281. [Google Scholar] [CrossRef] [Green Version]
- Sandstrom, B. Adrenergic beta-receptor blockers in hypertension of pregnancy. Clin. Exp. Hypertension. Part B Hypertens. Pregnancy 1982, 1, 127–141. [Google Scholar]
- Garden, A.; Davey, D.A.; Dommisse, J. Intravenous labetalol and intravenous dihydralazine in severe hypertension in pregnancy. Clin. Exp. Hypertens. B 1982, 1, 371–383. [Google Scholar] [CrossRef]
- Dumez, Y.; Tchobroutsky, C.; Hornych, H.; Amiel-Tison, C. Neonatal effects of maternal administration of acebutolol. Br. Med. J. 1981, 283, 1077–1079. [Google Scholar] [CrossRef] [Green Version]
- Bott-Kanner, G.; Schweitzer, A.; Reisner, S.H. Propranolol and hydrallazine in the management of essential hypertension in pregnancy. Br. J. Obstet. Gynaecol. 1980, 87, 110–114. [Google Scholar] [CrossRef]
- O’Hare, M.F.; Murnaghan, G.A.; Russell, C.J.; Leahey, W.J.; Varma, M.P.; McDevitt, D.G. Sotalol as a hypotensive agent in pregnancy. Br J Obstet Gynaecol 1980, 87, 814–820. [Google Scholar] [CrossRef]
- Gallery, E.D.M.; Saunders, D.M.; Hunyor, S.N.; Gyory, A.Z. Randomised comparison of methyldopa and oxprenolol for treatment of hypertension in pregnancy. Br. Med. J. 1979, 1, 1591–1594. [Google Scholar] [CrossRef] [Green Version]
- Pruyn, S.C.; Phelan, J.P.; Buchanan, G.C. Long-term propranolol therapy in pregnancy: Maternal and fetal outcome. Am. J. Obstet. Gynecol. 1979, 135, 485–489. [Google Scholar] [CrossRef]
- Eliahou, H.E.; Silverberg, D.S.; Reisin, E. Propranolol for the treatment of hypertension in pregnancy. Br. J. Obstet. Gynaecol. 1978, 85, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Sullo, M.G.; Perri, D.; Sibilio, M.; Rafaniello, C.; Fucile, A.; Rossi, F.; Capuano, A. Hypoglycemia, polycythemia and hyponatremia in a newborn exposed to nebivolol during pregnancy. J. Pharmacol. Pharmather. 2015, 6, 45–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, T.P.; Guillet, R. Use of glucagon to treat neonatal low-output congestive heart failure after maternal labetalol therapy. J. Pediatr. 1995, 127, 151–153. [Google Scholar] [CrossRef]
- Klarr, J.M.; Bhatt-Mehta, V.; Donn, S.M. Neonatal adrenergic blockade following single dose maternal labetalol administration. Am. J. Perinatol. 1994, 11, 91–93. [Google Scholar] [CrossRef]
- Haraldsson, A.; Geven, W. Severe adverse effects of maternal labetalol in a premature infant. Acta Paediatr. Scand. 1989, 78, 956–958. [Google Scholar] [CrossRef]
- Haraldsson, A.; Geven, W. Half-life of maternal labetalol in a premature infant. Pharm. Weekbl. Sci. 1989, 11, 229–231. [Google Scholar] [CrossRef]
- Schmimmel, M.S.; Eidelman, A.J.; Wilschanski, M.A.; Shaw Jr, D.; Ogilvie, R.J.; Koren, G. Toxic effects of atenolol consumed during breast feeding. J. Pediatr. 1989, 114, 476–478. [Google Scholar] [CrossRef]
- Fox, R.E.; Marx, C.; Stark, A.R. Neonatal effects of maternal nadolol therapy. Am. J. Obstet. Gynecol. 1985, 152, 1045–1046. [Google Scholar] [CrossRef]
- Woods, D.L.; Morrell, D.F. Atenolol: Side effects in a newborn infant. Br. Med. J. 1982, 285, 691–692. [Google Scholar] [CrossRef] [Green Version]
- Bott-Kanner, G.; Schweitzer, A.; Schoenfeld, A. Treatment with propranolol and hydralazine throughout pregnancy in a hypertensive patient. A case report. Isr. J. Med. Sci. 1978, 14, 466–468. [Google Scholar]
- Sabom, M.B.; Curry, R.C., Jr.; Wise, D.E. Propranolol therapy during pregnancy in a patient with idiopathic hypertrophic subaortic stenosis: Is it safe? South Med. J. 1978, 71, 328–329. [Google Scholar] [CrossRef]
- Datta, S.; Kitzmiller, J.L.; Ostheimer, G.W.; Schoenbaum, S.C. Propranolol and parturition. Obstet. Gynecol. 1978, 51, 577–581. [Google Scholar] [CrossRef]
- Habib, A.; McCarthy, J.S. Effects on the neonate of propranolol administered during pregnancy. J. Pediatr. 1977, 91, 808–811. [Google Scholar] [CrossRef]
- Cottrill, C.M.; McAllister Jr, R.G.; Gettes, L.; Noonan, J.A. Propranolol therapy during pregnancy, labor, and delivery: Evidence for transplacental drug transfer and impaired neonatal drug disposition. J. Pediatr. 1977, 91, 812–814. [Google Scholar] [CrossRef]
- Gladstone, G.R.; Hordof, A.; Gersony, W.M. Propranolol administration during pregnancy: Effects on the fetus. J. Pediatr. 1975, 86, 962–964. [Google Scholar] [CrossRef]
- Fiddler, G.I. Propranolol and pregnancy. Lancet 1974, 2, 722–723. [Google Scholar] [CrossRef]
- Datapharm Ltd. Methyldopa 500 mg Tablets BP. Available online: https://www.medicines.org.uk/emc/product/5879/smpc (accessed on 6 June 2022).
- Ryu, R.J.; Eyal, S.; Easterling, T.R.; Caritis, S.N.; Venkataraman, R.; Hankins, G.; Rytting, E.; Thummel, K.; Kelly, E.J.; Risler, L.; et al. Pharmacokinetics of metoprolol during pregnancy and lactation. J. Clin. Pharmacol. 2016, 56, 581–589. [Google Scholar] [CrossRef]
- Eyal, S.; Kim, J.D.; Anderson, G.D.; Buchanan, M.L.; Brateng, D.A.; Carr, D.; Woodrum, D.E.; Easterling, T.R.; Hebert, M.F. Atenolol pharmacokinetics and excretion in breast milk during the first 6 to 8 months postpartum. J. Clin. Pharmacol. 2010, 50, 1301–1309. [Google Scholar] [CrossRef]
- Aizman, L.; Van Den Anker, J.; Tender, J.; Krishnan, A.; Kirkorian, A.Y. Special management considerations for propranolol use in breastfed infants of mothers taking antihypertensives. Pediatr. Dermatol. 2020, 37, 537–540. [Google Scholar] [CrossRef]








| Descriptor | Criteria |
|---|---|
| Clinical benefit/harm | Statistically significant result High certainty evidence Biological mechanism(s) well established Point estimates of underlying studies are consistently in one direction Optimal information size reached |
| Probable clinical benefit/harm | Statistically significant result Moderate or high certainty evidence Evidence of biological plausibility Point estimates of underlying studies are predominantly in one direction Close to optimal information size or summary confidence interval is sufficiently narrow to give confidence that the true effect would be clinically meaningful if it is only in the ballpark of the summary estimate |
| Possible clinical benefit/harm | Statistically significant result Low or very low certainty evidence Few studies, wide summary confidence interval or effect is driven by one or two heavily weighted studies |
| Improbable benefit/harm | Statistically non-significant result Moderate or high certainty evidence Point estimates of underlying studies are close to and on both sides of the line of null effect |
| No clinical benefit/harm | Statistically non-significant result High certainty evidence Point estimates of underlying studies are close to and on either side of the line of null effect Majority of underlying studies are adequately powered for outcome of interest Optimal information size reached |
| Clinical benefit/harm cannot be excluded | Statistically non-significant result Low or very low certainty evidence Few studies Wide confidence intervals |
| Article | Acebutolol | Atenolol | Bisoprolol | Carvedilol | Labetalol | Metoprolol | Nadolol | Oxprenolol | Pindolol | Propranolol | Sotalol |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bigelow CA, 2021 [29] | 2 mg | ||||||||||
| Kayser A, 2020 [30] | 1.25–10 mg/day | 12–400 mg/day | |||||||||
| Kumar N, 2020 1,2 [31] | |||||||||||
| Mazkereth R, 2019 2 [32] | X | X | X | ||||||||
| Easterling T, 2019 [33] | 200 mg/day (max. 600 mg/day) | ||||||||||
| Thewissen L, 2017 [34] | X | ||||||||||
| Bateman BT, 2016 2 [35] | X | X | X | X | X | X | X | X | X | X | |
| Singh R, 2016 3 [36] | X | ||||||||||
| Heida KY,2012 4 [37] | X | ||||||||||
| Verma R, 2012 [38] | 100–300 mg three times per day | ||||||||||
| Davis RL, 2011 5 [39] | |||||||||||
| Vigil-De Gracia P, 2006 6 [40] | Max. 300 mg | ||||||||||
| Darcie S, 2004 [41] | 50 mg two times per day | ||||||||||
| Paran E, 1995 [42] | 5–15 mg | 40–120 mg | |||||||||
| Munshi UK, 1992 2 [43] | X | ||||||||||
| Bott-Kanner G, 1992 [44] | 5–10 mg two or three times per day | ||||||||||
| Pickles CJ, 1989 [45] | 100–200 mg three times per day | ||||||||||
| Ramanathan J, 1988 7 [28] | X | ||||||||||
| Ashe RG, 1987 [46] | 200 mg | ||||||||||
| Mabie WC, 1987 [47] | 20–80 mg | ||||||||||
| Boutroy MJ, 1986 [48] | 200–1200 mg per day | ||||||||||
| Macpherson M, 1986 [49] | 100–300 mg three times per day | ||||||||||
| Högstedt S, 1985 [50] | 50 mg two times per day (200 mg maximum per day) | ||||||||||
| Reynolds B, 1984 [51] | Max. 200 mg per day | ||||||||||
| Williams ER, 1983 [52] | 300–600 mg per day | ||||||||||
| Rubin PC, 1983 [53] | 100 mg per day | ||||||||||
| Liedholm H, 1983 [54] | 50–200 mg per day | X | |||||||||
| Liedholm H, 1983 2 [27] | X | ||||||||||
| Livingstone I, 1983 [55] | 30–160 mg per day | ||||||||||
| Dubois D, 1983 [26] | 200 mg | 100 mg | 5 mg | ||||||||
| Boutroy MJ, 1982 [56] | 200–800 mg per day | ||||||||||
| Rubin PC, 1982 [57] | 100 or 200 mg per day | ||||||||||
| Sandström B, 1982 [58] | 100–400 mg | ||||||||||
| Garden A, 1982 [59] | 200 mg | ||||||||||
| Dumez Y, 1981 [60] | 200–800 mg/day | ||||||||||
| Bott-Kanner G, 1980 [61] | 30–240 mg per day | ||||||||||
| O’Hare MF, 1980 [62] | 200 mg per day | ||||||||||
| Gallery ED, 1979 8 [63] | X | ||||||||||
| Pruyn SC, 1979 [64] | 10–80 mg per day | ||||||||||
| Eliahou HE, 1978 [65] | 40–120 mg per day |
| Source | Domain 1. Risk of Bias from the Randomization Process | Domain 2. Risk of Bias Due to Deviations from the Intended Interventions | Domain 3. Missing Outcome Data | Domain 4. Risk of Bias in Measurement of the Outcome | Domain 5. Risk of Bias in selection of the Reported Result | Overall Risk of Bias Judgement |
|---|---|---|---|---|---|---|
| Ashe RG, 1987 [46] | Some concerns | Low | Low | Low | Some concerns | High risk |
| Bigelow CA, 2021 [29] | Low | Low | Low | Low | Low | Low |
| Bott-Kanner G, 1992 [44] | Some concerns | Low | Low | Low | Some concerns | High risk |
| Darcie S, 2004 [41] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Easterling T, 2019 [33] | Low | Some concerns | Low | Low | Low | Some concerns |
| Gallery ED, 1979 [63] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Garden A, 1982 [59] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Högstedt S, 1985 [50] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Livingstone I, 1983 [55] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Mabie WC, 1987 [47] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Paran E, 1994 [42] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Pickles CJ, 1989 [45] | Some concerns | Low | Low | Low | Some concerns | High risk |
| Ramanathan J, 1988 [28] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Reynolds B, 1984 [51] | Some concerns | Low | Low | Low | Some concerns | High risk |
| Rubin PC, 1983 [53] | Some concerns | Low | Low | Low | Some concerns | High risk |
| Singh R, 2016 [36] | Some concerns | Some concerns | Low | Low | Some concerns | High risk |
| Verma R, 2012 [38] | Low | Some concerns | Low | Low | Some concerns | High risk |
| Vigil-De Graca P, 2006 [40] | Low | Low | Low | Low | Some concerns | Some concerns |
| Source | Bias Due to Confounding | Bias in Selecting Participants | Bias in Classification of the Interventions | Bias Due to Deviations from Intended Interventions | Bias Due To Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Bateman BT, 2016 [35] | Moderate | Moderate | Moderate | Low | Low | Low | Moderate | Moderate |
| Davis RL, 2011 [39] | Critical | Serious | Moderate | Low | NI | Low | Moderate | Critical |
| Dumez Y, 1981 [60] | Critical | NI | Low | Low | Low | Low | Moderate | Critical |
| Heida KY, 2012 [37] | NI | Low | Moderate | Low | Low | Low | Moderate | Moderate |
| Kayser A, 2020 [30] | Moderate | Moderate | Moderate | Low | Low | Low | Low | Moderate |
| Kumar N, 2020 [31] | Serious | Moderate | Moderate | Low | Low | Low | Moderate | Serious |
| Liedholm H, 1983 [54] | Critical | Moderate | Serious | Low | Low | Low | Moderate | Critical |
| Macpherson M, 1986 [49] | Serious | Serious | Low | Low | Low | Low | Moderate | Serious |
| Mazkereth R, 2019 [32] | Critical | Serious | Serious | Low | Low | Low | Moderate | Critical |
| Munshi UK, 1992 [43] | Moderate | Moderate | Serious | Low | Low | Low | Moderate | Serious |
| Sandstrom B, 1982 [58] | Serious | Moderate | NI | Low | Low | Low | Moderate | Serious |
| Thewissen L, 2017 [34] | Serious | Serious | Serious | Low | Low | Low | Moderate | Serious |
| Williams ER, 1983 [52] | Serious | Moderate | Low | Low | Low | Low | Low | Serious |
| Source | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Boutroy MJ, 1986 [48] | Y | Y | Y | N | N | N | N | Y | N | N/A |
| Liedholm, 1983 [27] | Y | Y | Y | Y | Y | N | N | Y | N | N/A |
| Dubois, 1983 [26] | Y | Y | Y | Y | U | N | Y | Y | N | N/A |
| Boutroy MJ, 1982 [56] | Y | Y | Y | N | N | N | N | Y | N | Y |
| Rubin PC, 1982 [57] | Y | Y | Y | U | U | N | N | Y | N | Y |
| Bott-Kanner G, 1980 [61] | N | Y | Y | N | N | N | Y | Y | N | N/A |
| O’hare MF, 1980 [62] | Y | Y | Y | N | N | Y | Y | Y | N | Y |
| Pruyn SC, 1979 [64] | N | Y | N | Y | Y | N | Y | Y | N | Y |
| Eliahou HE, 1978 [65] | Y | Y | Y | Y | Y | N | Y | Y | N | N/A |
| Source | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 |
|---|---|---|---|---|---|---|---|---|
| Sullo MG, 2015 [66] | N/A 1 | N/A 2 | Y | Y | Y | Y | Y | Y |
| Stevens TP, 1995 [67] | N | N | Y | Y | Y | Y | Y | Y |
| Klarr JM, 1994 [68] | Y | N | Y | U | Y | Y | Y | Y |
| Haraldsson A, 1989 [69] | N/A 1 | N/A 2 | Y | Y | Y | Y | Y | Y |
| Haraldsson A, 1989 [70] | N/A 1,3 | N/A 2 | Y | Y | U | Y | Y | Y |
| Schmimmel MS, 1989 [71] | N/A 1 | N/A 2 | Y | Y | Y | Y | Y | Y |
| Fox RE, 1985 [72] | Y | N | Y | Y | Y | Y | Y | Y |
| Woods DL, 1982 [73] | N/A 1 | N/A 2 | Y | Y | Y | Y | Y | Y |
| Bott-Kanner G, 1978 [74] | U | Y | Y | Y | Y | U | Y | Y |
| Sabom MB, 1978 [75] | N | N | Y | Y | Y | Y | Y | Y |
| Datta S, 1978 [76] | Y | Y | Y | Y | Y | Y | Y | Y |
| Habib A, 1977 [77] | N | N | Y | Y | Y | Y | Y | Y |
| Cottrill CM, 1977 [78] | N | N | U | Y | Y | Y | Y | Y |
| Gladstone GR, 1975 [79] | N/A 1,3 | N/A 2 | Y | Y | Y | Y | Y | Y |
| Fiddler GI, 1974 [80] | N | N | Y | Y | Y | Y | Y | Y |
| Certainty Assessment | Summary of Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants (Studies)Follow-up | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Certainty of Evidence | Study Event Rates (%) | Relative Effect (95% CI) | Anticipated Absolute Effects | ||
| With Other Antihypertensive Drugs or Placebo | With Beta-Blockers | Risk with Other Antihypertensive Drugs or Placebo | Risk Difference with Beta-Blockers | ||||||||
| Bradycardia (Cohort studies) | |||||||||||
| 2,293,407 (3 observational studies) | Serious a | Serious b | not serious | Serious c | strong association | ⨁⨁◯◯ Low | 11,669/2,282,318 (0.5%) | 175/11089 (1.6%) | RR 2.10 (0.97 to 4.55) | 5 per 1000 | 6 more per 1000 (from 0 fewer to 18 more) |
| Bradycardia (Case control studies) | |||||||||||
| 45 cases 800 controls (5 observational studies) | very serious d | very serious e | not serious | very serious f | none | ⨁◯◯◯ Very low | 45 cases 800 controls | RR 1.86 (0.31 to 11.19) | Low | ||
| 0 per 1000 | 0 fewer per 1000 (from 0 fewer to 0 fewer) | ||||||||||
| Bradycardia (RCTs) | |||||||||||
| 2013 (11 RCTs) | very serious g | not serious | not serious | not serious | none | ⨁⨁◯◯ Low | 15/1017 (1.5%) | 38/996 (3.8%) | RR 2.36 (1.33 to 4.18) | 15 per 1000 | 20 more per 1000 (from 5 more to 47 more) |
| Hypoglycemia (Cohort studies) | |||||||||||
| 2,374,957 (6 observational studies) | Serious h | serious i | not serious | not serious | strong association | ⨁⨁⨁◯ Moderate | 29,954/2,362,830 (1.3%) | 620/12,127 (5.1%) | RR 3.01 (2.79 to 3.25) | 13 per 1000 | 25 more per 1000 (from 23 more to 29 more) |
| Hypoglycemia (Case control studies) | |||||||||||
| 168 cases 416 controls (5 observational studies) | very serious j | not serious i | not serious | Serious k | none | ⨁◯◯◯ Very low | 168 cases 416 controls | RR 1.72 (1.33 to 2.22) | Low | ||
| 0 per 1000 | 0 fewer per 1000 (from 0 fewer to 0 fewer) | ||||||||||
| Hypoglycemia (RCTs) | |||||||||||
| 2051 (12 RCTs) | Serious l | not serious | not serious | serious c | none | ⨁⨁◯◯ Low | 57/1018 (5.6%) | 77/1033 (7.5%) | RR 1.06 (0.79 to 1.41) | 56 per 1000 | 3 more per 1000 (from 12 fewer to 23 more) |
| Article | Study Groups | Hypoglycemia | Blood Glucose (mmol/L) | Definition of Hypoglycemia | Time of Control of Hypoglycemia |
|---|---|---|---|---|---|
| Bigelow CA, 2021 [29] | Propranolol vs. placebo | 11/45 (24.4%) vs. 8/49 (16.3%) (p = 0.33) | Blood sugar < 40 md/dL | N | |
| Kayser A, 2020 [30] | ß-blocker vs. methyldopa ß-blocker vs. non-hypertensive mother | 7/252 (2.8%) vs. 3/199 (1.5%) (NS) 7/252 (2.8%) vs. 13/588 (2.2%) (NS) | Blood glucose < 35 mg/dl at the first day of life or <45 mg/dL after the first day of life | N | |
| Kumar N, 2020 [31] | ß-blocker vs. no disease | 78/228 (34.6%) vs. 914/4103 (22.2%) (p < 0.01) | Blood glucose < 40 mg/dL | At least 30 min after feeding. Feeding was initiated as soon as possible after delivery. For at least 24 h in late preterm and small for gestational age (SGA), and for the first 12 h in LGA infants and infants of mothers with diabetes | |
| Mazkereth R, 2019 [32] | ß-blocker vs. control | 47/153 (30.7%) vs. 28/153 (18.3%) p = 0.016 | Glucose < 40 mg/dL on the first day of life | Hours 1, 2, 4 and 6 of life and every 8 h thereafter (to complete a 48-h follow-up) | |
| Easterling T, 2019 [33] | Labetalol vs. nifedipine Labetalol vs. methyldopa | 0/290 (0%) vs. 1/298 (<1%) 0/290 (0%) vs. 0/294 (0%) | N | N | |
| Bateman BT, 2016 [35] | ß-blocker vs. control Labetalol vs. control Metoprolol vs. control Atenolol vs. control Propensity-score 1 corrected available | 460/10,585 (4.3%) vs. 27,228/2,281,531 (1.2%) 345/6748 (5.1%) vs. 27,228/2,281,531 (1.2%) 49/1485 (3.3%) vs. 27,228/2,281,531 (1.2%) 30/1121 (2.7%) vs. 27,228/2,281,531 (1.2%) | Glucose ≤ 35 mg/dL | N | |
| Singh R, 2016 [36] | Labetalol vs. hydralazine | NS | N | N | |
| Heida KY, 2012 [37] | Labetalol vs. control Labetalol i.v. vs. labetalol oral | 26/55 (47.3%) vs. 23/54 (42.6%) p = 0.62 43.2 vs. 55.6% p = 0.45 | Glucose < 2.7 mmol/L | In the first 48 postnatal hours | |
| Verma R, 2012 [38] | Labetalol vs. methyldopa | 1/45 (2.22%) vs. 2/45 (4.44%) (NS) | N | N | |
| Davis RL, 2011 2 [39] | ß-blocker vs. control ß-blocker vs. calcium channel blockers | 34/405 (8.4%) vs. 1771/75,688 (2.3%) 34/405 (8.4%) vs. 25/721 (3.5%) | N | N | |
| Vigil-De Gracia P, 2006 [40] | Labetalol vs. hydralazine | 6/103 (5.8%) vs. 6/102 (5.8%) | Plasma glucose < 35 mg/dL | N | |
| Darcie S, 2004 [41] | Atenolol vs. isradipine Atenolol vs. control | 26/40 (65%) vs. 24/39 (61.5%) (p = 0.818) 26/40 (65%) vs. 4/14 (28.5%) (p < 0.05) | Blood glycemia levels < 40 mg/dL | 1, 3, 6, 12 and 24 h after birth | |
| Paran E, 1995 [42] | Hydralazine vs. hydralazine and propranolol Hydralazine vs. hydralazine and pindolol | 76.4 ± 16.5 vs. 62.6 ± 14.0 mg% (p < 0.02) 76.4 ± 16.5 vs. 78.6 ± 15.7 mg% (p < 0.02) | N | In the first 48 postnatal hours | |
| Munshi UK, 1992 [43] | Labetalol vs. control | 23/48 (47.9%) vs. 14/81 (17.2%) (p < 0.01) | Blood glucose value of <30 mg/dL irrespective of gestational age, within the first 72 h of life and below 40 mg/dL thereafter | First at 1–2 h of age and again at 4–6 h of age, thereafter 2–6 hourly depending on the previous blood glucose results. The monitoring was stopped once at least two blood glucose values were above 40 mg on an oral feeding alone | |
| Bott-Kanner G, 1992 [44] | Pindolol vs. placebo | 3 | Blood glucose < 25 mg/dL | During the first 24 h of life | |
| Pickles CJ, 1989 [45] | Labetalol vs. placebo | 4/70 (5.7%) vs. 3/74 (4.1%) | Blood glucose < 1.4 nmol/L | N | |
| Ramanathan J, 1988 [28] | Labetalol vs. control | 0/15 (0%) vs. 0/10 (0%) | 53.4 ± 2.8 vs. 50 ± 3.1 (NS) | N | Within 10 to 20 min of delivery |
| Ashe RG, 1987 [46] | Labetalol vs. hydralazine | 1/10 (10%) vs. 0/10 (0%) | N | Every 4 h, for 1 day | |
| Mabie WC, 1987 [47] | Labetalol vs. hydralazine | 1/13 (7.7%) vs. 1/6 (16.7%) | Blood glucose < 35 mg/dL | N | |
| Macpherson M, 1986 [49] | Labetalol vs. control | 4 | <35 mg/dL | At 2, 4, 8,16, 24, 48 and 72 h after birth | |
| Högstedt S, 1985 [50] | Metoprolol and hydralazine vs. control (intended-to-treat) 5 Metoprolol and hydralazine vs. control (cause-effect) | 9/82 (11.0%) vs. 11/79 (13.9%) 8/69 (11.6%) vs. 10/66 (15.2%) | Blood glucose ≤ 1.7 mmol/L | N | |
| Williams ER, 1983 [52] | Acebutolol vs. methyldopa | 0/9 vs. 0/11 | N | N | |
| Rubin PC, 1983 [53] | Atenolol vs. placebo | 1/46 (2.2%) vs. 4/39 (10.3%) (NS) | Confirmed serum glucose < 1.4 nmol/L | At 1, 4, 6, 12 and 24 h | |
| Liedholm H, 1983 [54] | Atenolol or metoprolol (no control group) | 4/95 (4.2%) | N | N | |
| Livingstone I, 1983 [55] | Propranolol vs. methyldopa | 2/14 (14.3%) vs. 0/14 (0%) | N | For 48 h after delivery | |
| Dubois D, 1983 [26] | Beta blocker (no control group) | 1/125 (0.8%) | N | At birth | |
| Rubin PC, 1982 [57] | Atenolol (no control group) | 2/9 (22%) | N | During the first 24 h of life | |
| Sanström B, 1982 [58] | Bendroflumethiazide + metoprolol vs. metoprolol + hydralazine vs. Bendroflumethiazide + hydralazine | 6 | N | N | |
| Dumez Y, 1981 [60] | Acebutolol vs. methyldopa | 6/10 vs. 1/10 | Day 1: 1.60 mmol/L ± 0.99 vs. 2.55 mmol/L ± 0.42 (NS), Day 2: 2.63 mmol/L ± 0.50 vs. 2.47 mmol/L ± 0.63 (NS), Day 3: 3.29 mmol/L ± 1.53 vs. 2.72 mmol/L ± 1.19 (NS) | N | Daily within the 3 first days of life, for the first time at about three hours of life and on the second and third days of life two hours after feeding |
| Bott-Kanner G, 1980 [61] | Propranolol (no control group) | 2/14 (14.3%) | Blood glucose < 35 mg/dL | Frequently In the first few hours of life | |
| O’Hare MF, 1980 [62] | Sotalol (no control group) | 1/12 (8.33%) | N | Four-hourly | |
| Gallery ED, 1979 [63] | Oxprenolol vs. methyldopa | 3.8 ± 0.27 vs. 2.8 ± 0.36 mmol/L p < 0.05 | N | N | |
| Pruyn SC, 1979 [64] | Propranolol (no control group) | 3/12 (25%) | N | N | |
| Eliahou HE, 1978 [65] | Propranolol (no control group) | 0/22 (0%) | N | N |
| Source | Country | Treatment Indication | Beta-Blocker Type | Dosage | Blood Glucose | Heart Rate (Beats per Minute) |
|---|---|---|---|---|---|---|
| Sullo MG, 2015 [66] | Italy | Unspecified tachycardia | Nebivolol | 5 mg per day | 30 mg/dL | x |
| Stevens TP, 1995 [67] | United States | Hypertension | Labetalol | 150 mg two times per day | 1.7 mmol/L (30 mg/dL) | 111 after birth 100 in transit to tertiary referral center 100–120 (resting heart rate) |
| Klarr JM, 1994 [68] | United States | Hypertension prior to cesarean section | Labetalol | Single 30 mg dosage | 31 mg/dL (twin A) 37 mg/dL (twin B) | <80 (both twins) |
| Haraldsson A, 1989 [69] | The Netherlands | Hypertension prior to cesarean section | Labetalol | 50 mg/hour | Not described in article, but intravenous glucose was given | Severe bradycardia immediately after delivery. On admission the heart rate was 140 |
| Haraldsson A, 1989 [70] | The Netherlands | Pregnancy induced hypertension | Labetalol | 600 mg (200 mg 3 times per day) | 1.2 mmol/l | <80 after delivery, 148 later |
| Schmimmel MS, 1989 [71] | Israel | Postpartum hypertension | Atenolol | 100 mg daily (50 mg two times per day) | x | 80 |
| Fox RE, 1985 [72] | United States | Hypertension | Nadolol | 20 mg once per day | 20 mg/dl | 136 after birth 112 at 4.5 h of age 1 >135 at 4 days of age |
| Woods DL, 1982 [73] | South Africa | Uncontrolled hypertension | Atenolol | 100 mg daily | 2–5 mmol/L (45 mg/100 mL) | 138 |
| Bott-Kanner G,1978 [74] | Israel | Chronic hypertension | Propranolol | 160 --> 60 mg/day 2 (first pregnancy) 120 --> stop (second pregnancy) | 37 mg/dL (first pregnancy) 75 mg/dL after birth, 87 mg/dL next day (second pregnancy) | 150 (first pregnancy) 140 (second pregnancy) |
| Sabom MB, 1978 [75] | United States | Idiopathic Hypertrophic subaortic stenosis | Propranolol | 60 mg 4 times per day, discontinued upon admission | 25–45 mg/100 ml | Sinus bradycardia (heart rate not mentioned) |
| Datta S, 1978 [76] | United States | Idiopathic Hypertrophic subaortic stenosis | Propranolol | 80 mg daily | No hypoglycemia | 110–120, with a short period of 80 during sleep |
| Habib A, 1977 [77] | United States | Hyperthyroidism and congestive heart failure (case 1), supraventricular tachycardia (case 2 and 3) and hyperthyroidism (case 4) | Propranolol | 10 mg 4 times per day (case 1, 2 and 3), 10 mg two times per day (case 4) 3 | 20 mg/dL (case 1) 30 mg/dL (case 2) 25 mg/dL at one hour of age and 5 mg/dL at two hours of age (case 3) 25–45 mg/dL (case 4) | 80 within one hour of delivery (case 1) 4 80–90 5 (case 2) 100–120 6 (case 3) 80–90, frequently during first 24 h of life (case 4) |
| Cottrill CM, 1977 [78] | United States | Chronic atrial tachycardia | Propranolol | 160 mg per day (40 mg 4 times per day) 7 | Too low to be detected by the Dextrostix method | 40 at birth, later it varied between 100 and 165 |
| Gladstone GR, 1975 [79] | United States | Essential hypertension | Propranolol | 240 mg per Day decreased to 160 mg per Day 8 | 11 mg/dL | 70–90 during first day of life. Rose with stimulation to 120/minute. Was 120–130/minute on day 5 |
| Fiddler GI, 1974 [80] | Scotland | Hypertrophic Obstructive cardiomyopathy | Propranolol | 30 mg 3 times per day | 12 mg/100 mL | x |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Bruin, R.; van Dalen, S.L.; Franx, S.J.; Ramaswamy, V.V.; Simons, S.H.P.; Flint, R.B.; van den Bosch, G.E. The Risk for Neonatal Hypoglycemia and Bradycardia after Beta-Blocker Use during Pregnancy or Lactation: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9616. https://doi.org/10.3390/ijerph19159616
de Bruin R, van Dalen SL, Franx SJ, Ramaswamy VV, Simons SHP, Flint RB, van den Bosch GE. The Risk for Neonatal Hypoglycemia and Bradycardia after Beta-Blocker Use during Pregnancy or Lactation: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(15):9616. https://doi.org/10.3390/ijerph19159616
Chicago/Turabian Stylede Bruin, Rosalie, Sarah L. van Dalen, Shamaya J. Franx, Viraraghavan V. Ramaswamy, Sinno H. P. Simons, Robert B. Flint, and Gerbrich E. van den Bosch. 2022. "The Risk for Neonatal Hypoglycemia and Bradycardia after Beta-Blocker Use during Pregnancy or Lactation: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 15: 9616. https://doi.org/10.3390/ijerph19159616
APA Stylede Bruin, R., van Dalen, S. L., Franx, S. J., Ramaswamy, V. V., Simons, S. H. P., Flint, R. B., & van den Bosch, G. E. (2022). The Risk for Neonatal Hypoglycemia and Bradycardia after Beta-Blocker Use during Pregnancy or Lactation: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(15), 9616. https://doi.org/10.3390/ijerph19159616