
Validation of the Short Food Literacy Questionnaire in the Representative Sample of Polish Internet Users


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
2.2. Questionnaire
2.3. The Polish Version of the SFLQ
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
3.2. Internal Consistency
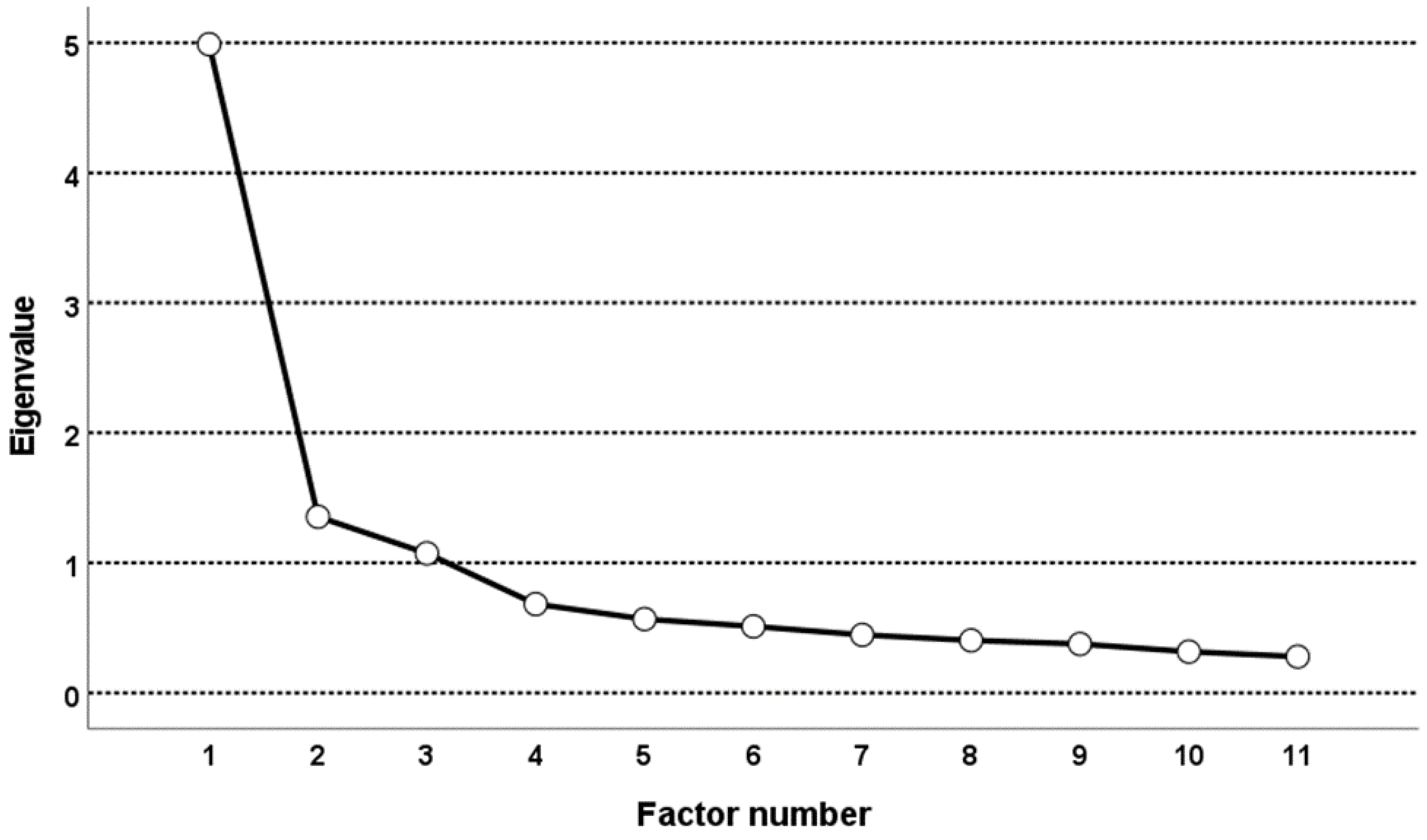
3.3. Exploratory Factor Analysis
3.4. Confirmatory Factory Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nutbeam, D. Health Promotion Glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Sørensen, S.K.; Stephan Van den Broucke, J.F.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health Literacy and Public Health: A Systematic Review and Integration of Definitions and Models. BMC Public Health 2012, 12, 12–80. [Google Scholar] [CrossRef] [Green Version]
- Berkman, N.D.; Donahue, K.; Halpern, D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Evid. Rep./Technol. Assess. 2011, 199, 1–141. [Google Scholar] [CrossRef] [PubMed]
- Humphrys, E.; Burt, J.; Rubin, G.; Emery, J.D.; Walter, F.M. The Influence of Health Literacy on the Timely Diagnosis of Symptomatic Cancer: A Systematic Review. Eur. J. Cancer Care 2019, 28, e12920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaben, K.; Khalil, A. Health Literacy, Self-Care Behavior and Quality of Life in Acute Coronary Syndrome Patients: An Integrative Review. Open J. Nurs. 2019, 9, 383–395. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Pelikan, J.J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health Literacy in Europe: Comparative Results of the European Health Literacy Survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [Green Version]
- Krause, C.; Sommerhalder, K.; Beer-Borst, S.; Abel, T. Just a Subtle Difference? Findings from a Systematic Review on Definitions of Nutrition Literacy and Food Literacy. Health Promot. Int. 2018, 33, 378–389. [Google Scholar] [CrossRef] [Green Version]
- Yuen, E.Y.N.; Thomson, M.; Gardiner, H. Measuring Nutrition and Food Literacy in Adults: A Systematic Review and Appraisal of Existing Measurement Tools. Health Lit. Res. Pract. 2018, 2, e134–e160. [Google Scholar] [CrossRef] [Green Version]
- Silk, K.J.; Sherry, J.; Winn, B.; Keesecker, N.; Horodynski, M.A.; Sayir, A. Increasing Nutrition Literacy: Testing the Effectiveness of Print, Web Site, and Game Modalities. J. Nutr. Educ. Behav. 2008, 40, 3–10. [Google Scholar] [CrossRef]
- Guttersrud, O.; Dalane, J.O.; Pettersen, S. Improving Measurement in Nutrition Literacy Research Using Rasch Modelling: Examining Construct Validity of Stage-Specific “critical Nutrition Literacy” Scales. Public Health Nutr. 2014, 17, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Fordyce-Voorham, S. Identification of Essential Food Skills for Skill-Based Healthful Eating Programs in Secondary Schools. J. Nutr. Educ. Behav. 2011, 43, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Sumner, J. Food Literacy and Adult Education: Learning to Read the World by Eating. Can. J. Study Adult Educ. (Online) Supl. Explor. Soc. Influ. Learn. 2013, 25, 79. [Google Scholar]
- Nutbeam, D. Health Literacy as a Public Health Goal: A Challenge for Contemporary Health Education and Communication Strategies into the 21st Century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Perry, E.A.; Thomas, H.; Samra, H.R.; Edmonstone, S.; Davidson, L.; Faulkner, A.; Petermann, L.; Manafò, E.; Kirkpatrick, S.I. Identifying Attributes of Food Literacy: A Scoping Review. Public Health Nutr. 2017, 20, 2406–2415. [Google Scholar] [CrossRef] [Green Version]
- Colatruglio, S.; Slater, J. Challenges to Acquiring and Utilizing Food Literacy: Perceptions of Young Canadian Adults. Can. Food Stud./Rev. Can. Études L’alimentation 2016, 3, 96–118. [Google Scholar] [CrossRef] [Green Version]
- Diamond, J.J. Development of a Reliable and Construct Valid Measure of Nutritional Literacy in Adults. Nutr. J. 2007, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, H.D.; Ellerbeck, E.F.; Gajewski, B.; Zhang, C.; Sullivan, D.K. The Nutrition Literacy Assessment Instrument Is a Valid and Reliable Measure of Nutrition Literacy in Adults with Chronic Disease. J. Nutr. Educ. Behav. 2018, 50, 247–257.e1. [Google Scholar] [CrossRef]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick Assessment of Literacy in Primary Care: The Newest Vital Sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Ringland, E.M.; Gifford, J.A.; Denyer, G.S.; Thai, D.; Franklin, J.L.; Stevenson, M.M.; Prvan, T.; O’connor, H.T. Evaluation of an Electronic Tool to Assess Food Label Literacy in Adult Australians: A Pilot Study. Nutr. Diet. 2016, 73, 482–489. [Google Scholar] [CrossRef]
- Krause, C.G.; Beer-Borst, S.; Sommerhalder, K.; Hayoz, S.; Thomas, A. A Short Food Literacy Questionnaire (SFLQ) for Adults: Findings from a Swiss Validation Study. Appetite 2018, 1, 275–280. [Google Scholar] [CrossRef]
- Durmus, H.; Gökler, M.E.; Havlioglu, S. Reliability and Validity of the Turkish Version of the Short Food Literacy Questionnaire among University Students. Prog. Nutr. 2019, 21, 333–338. [Google Scholar] [CrossRef]
- Gökler, M.E.; Durmuş, H.; Havlioǧlu, S. Food Literacy Can Described Adequate? Optimizing Cut-off Scores for the Short Food Literacy Questionnaire (SFLQ). Med. J. Nutr. Metab. 2020, 13, 119–126. [Google Scholar] [CrossRef]
- Trieste, L.; Bazzani, A.; Amato, A.; Faraguna, U.; Turchetti, G. Food Literacy and Food Choice–a Survey-Based Psychometric Profiling of Consumer Behaviour. Br. Food J. 2021, 123, 124–141. [Google Scholar] [CrossRef]
- Itzkovitz, A.; Maggio, V.; Roy-Fleming, A.; Legault, L.; Brazeau, A.-S. Nutrition and Food Literacy among Young Canadian Adults Living with Type 1 Diabetes. Diabet. Med. 2022, e14921. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Process of Translation and Adaptation of Instruments. Available online: http://www.who.int/substance_abuse/research_tools/translation/en (accessed on 25 May 2022).
- Ogólnopolski Panel Badawczy Sp. z Ogólnopolski Panel Badawczy Ariadna. Available online: https://panelariadna.pl/ (accessed on 10 July 2022).
- Guiné, R.P.F.; Duarte, J.; Ferrão, A.C.; Ferreira, M.; Correia, P.; Cardoso, A.P.; Bartkiene, E.; Szucs, V.; Nemes, L.; Ljubičić, M.; et al. The Eating Motivations Scale (EATMOT): Development and Validation by Means of Confirmatory Factor Analysis (CFA) and Structural Equation Modelling (SEM). Zdr. Varst. 2021, 60, 4–9. [Google Scholar] [CrossRef]
- The European Health Literacy Project. Comparative Report On Health Literacy in Eight EU Member States; The European Health Literacy Survey HLS-EU. 2012. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiHkKmVjLH5AhVD2DgGHcHtAVgQFnoECAoQAQ&url=https%3A%2F%2Fcdn1.sph.harvard.edu%2Fwp-content%2Fuploads%2Fsites%2F135%2F2015%2F09%2Fneu_rev_hls-eu_report_2015_05_13_lit.pdf&usg=AOvVaw0ubJDA16x5Fw0gleh_dCU9 (accessed on 25 May 2022).
- Wolnicka, K. Talerz Zdrowego Żywienia. Available online: https://ncez.pzh.gov.pl/abc-zywienia/talerz-zdrowego-zywienia/ (accessed on 29 May 2022).
- Hutcheson, G.; Sofroniou, N. The Multivariate Social Scientist. Introductory Statistics Using Generalized Linear Models; Sage Publications: Thousand Oaks, CA, USA, 1999; ISBN 9780761952008. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 4th ed.; SAGE: London, UK, 2013. [Google Scholar]
- Child, D. The Essentials of Factor Analysis, 3rd ed.; Continuum: New York, NY, USA, 2006. [Google Scholar]
- Guadagnoli, E.; Velicer, W.F. Relation of Sample Size to the Stability of Component Patterns. Psychol. Bull. 1988, 103, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L. Figuring out Factors: The Use and Misuse of Factor Analysis. Can. J. Psychiatry 1994, 39, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.-T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hatcher, L.; O’Rourke, N. A Step-by-Step Approach to Using SAS for Factor Analysis and Structural Equation Modeling, 2nd ed.; SAS Institute Inc.: Cary, NC, USA, 2013; ISBN 978-1599942308. [Google Scholar]
- Tennant, A.; Pallant, J. The Root Mean Square Error of Approximation (RMSEA). Rasch Meas. Trans. 2012, 25, 1348–1349. [Google Scholar]
- Kline, P. An Easy Guide to Factor Analysis, 1st ed.; Routledge: London, UK, 1994; ISBN 9781315788135. [Google Scholar]
- Hurley, A.E.; Scandura, T.A.; Schriesheim, C.A.; Brannick, M.T.; Seers, A.; Vandenberg, R.J.; Williams, L.J. Exploratory and Confirmatory Factor Analysis: Guidelines, Issues, and Alternatives. J. Organ. Behav. 1997, 18, 667–683. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. EHEALS: The EHealth Literacy Scale. J. Med. Internet Res. 2006, 8, e507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soellner, R.; Huber, S.; Reder, M. The Concept of Ehealth Literacy and Its Measurement: German Translation of the EHEALS. J. Media Psychol. 2014, 26, 29–38. [Google Scholar] [CrossRef]
- Hyde, L.L.; Boyes, A.W.; Evans, T.J.; Mackenzie, L.J.; Sanson-Fisher, R. Three-Factor Structure of the EHealth Literacy Scale Among Magnetic Resonance Imaging and Computed Tomography Outpatients: A Confirmatory Factor Analysis. JMIR Hum. Factors 2018, 5, e9039. [Google Scholar] [CrossRef] [PubMed]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural Equation Modelling: Guidelines for Determining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Babyak, M.A.; Green, S.B. Confirmatory Factor Analysis: An Introduction for Psychosomatic Medicine Researchers. Psychosom. Med. 2010, 72, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Chi-Square for Model Fit in Confirmatory Factor Analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | Variable Categories | All Respondents (n = 1286) | Subset 1 (n = 628) | Subset 2 (n = 658) | |||
|---|---|---|---|---|---|---|---|
| % | n | % | n | % | n | ||
| Gender | Female | 49.53 | 637 | 48.73 | 306 | 50.30 | 331 |
| Male | 50.47 | 649 | 51.27 | 322 | 49.70 | 327 | |
| Place of residence | Rural | 38.34 | 493 | 36.46 | 229 | 40.12 | 264 |
| urban below 20,000 inhabitants | 13.30 | 171 | 12.42 | 78 | 14.13 | 93 | |
| urban 20,000–100,000 inhabitants | 19.60 | 252 | 20.06 | 126 | 19.15 | 126 | |
| urban 100,000–200,000 inhabitants | 8.24 | 106 | 8.12 | 51 | 8.36 | 55 | |
| urban 200,000–500,000 inhabitants | 9.33 | 120 | 9.55 | 60 | 9.12 | 60 | |
| urban above 500,000 inhabitants | 11.20 | 144 | 13.38 | 84 | 9.12 | 60 | |
| Education | lower than secondary | 11.90 | 153 | 10.67 | 67 | 13.07 | 86 |
| secondary vocational | 22.24 | 286 | 23.09 | 145 | 21.43 | 141 | |
| secondary | 38.34 | 493 | 39.17 | 246 | 37.54 | 247 | |
| University | 27.53 | 354 | 27.07 | 170 | 27.96 | 184 | |
| Net monthly household income | not more than 1000 PLN | 5.37 | 69 | 5.10 | 32 | 5.62 | 37 |
| 1001–1500 PLN | 9.80 | 126 | 8.12 | 51 | 11.40 | 75 | |
| 1501–2000 PLN | 11.12 | 143 | 11.46 | 72 | 10.79 | 71 | |
| 2001–3000 PLN | 21.85 | 281 | 22.61 | 142 | 21.12 | 139 | |
| 3001–5000 PLN | 10.50 | 135 | 10.51 | 66 | 10.49 | 69 | |
| 5001–7000 PLN | 13.92 | 179 | 15.76 | 99 | 12.16 | 80 | |
| more than 7000 PLN | 5.52 | 71 | 4.94 | 31 | 6.08 | 40 | |
| not revealed | 21.93 | 282 | 21.50 | 135 | 22.34 | 147 | |
| Vocational status | employee | 64.54 | 830 | 66.88 | 420 | 62.31 | 410 |
| self-employed or farmer | 12.60 | 162 | 12.10 | 76 | 13.07 | 86 | |
| retired or on disability pension | 5.13 | 66 | 5.10 | 32 | 5.17 | 34 | |
| high school or university student | 8.79 | 113 | 7.64 | 48 | 9.88 | 65 | |
| vocationally passive incl. unemployed | 16.02 | 206 | 15.13 | 95 | 16.87 | 111 | |
| Marital status | single | 28.46 | 366 | 27.87 | 175 | 29.03 | 191 |
| married | 47.74 | 614 | 49.04 | 308 | 46.50 | 306 | |
| in partnership | 16.10 | 207 | 15.45 | 97 | 16.72 | 110 | |
| widowed | 2.18 | 28 | 2.23 | 14 | 2.13 | 14 | |
| divorced or in separation | 5.52 | 71 | 5.41 | 34 | 5.62 | 37 | |
| SFLQ Item | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| item 2 | 0.47 | ||||||||||
| item 3 | 0.40 | 0.33 | |||||||||
| item 4 | 0.33 | 0.32 | 0.62 | ||||||||
| item 5 | 0.28 | 0.28 | 0.54 | 0.70 | |||||||
| item 6 | 0.45 | 0.31 | 0.36 | 0.35 | 0.34 | ||||||
| item 7 | 0.23 | 0.20 | 0.19 | 0.12 | 0.11 | 0.14 | |||||
| item 8 | 0.53 | 0.53 | 0.47 | 0.42 | 0.39 | 0.44 | 0.31 | ||||
| item 9 | 0.36 | 0.30 | 0.33 | 0.34 | 0.29 | 0.34 | 0.03 | 0.34 | |||
| item 10 | 0.32 | 0.28 | 0.36 | 0.35 | 0.32 | 0.36 | 0.08 | 0.37 | 0.67 | ||
| item 11 | 0.38 | 0.32 | 0.34 | 0.31 | 0.30 | 0.38 | 0.03 | 0.39 | 0.58 | 0.61 | |
| item 12 | 0.37 | 0.29 | 0.34 | 0.36 | 0.32 | 0.37 | −0.001 | 0.38 | 0.45 | 0.58 | 0.60 |
| Factor | Initial Eigenvalues | Sum of Squared Loading after Extraction | Sums of Squared Loading after Rotation | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | % of Variance | Cumulated % of Variance | Total | % of Variance | Cumulated % of Variance | Total | % of Variance | Cumulated % of Variance | |
| 1 | 4.99 | 45.35 | 45.35 | 4.53 | 41.20 | 41.20 | 2.35 | 21.32 | 21.32 |
| 2 | 1.35 | 12.31 | 57.67 | 0.99 | 9.03 | 50.23 | 1.94 | 17.66 | 38.99 |
| 3 | 1.07 | 9.75 | 67.42 | 0.66 | 5.97 | 56.20 | 1.89 | 17.22 | 56.20 |
| 4 | 0.68 | 6.21 | 73.63 | ||||||
| 5 | 0.57 | 5.16 | 78.79 | ||||||
| 6 | 0.51 | 4.65 | 83.44 | ||||||
| 7 | 0.45 | 4.06 | 87.50 | ||||||
| 8 | 0.40 | 3.67 | 91.17 | ||||||
| 9 | 0.38 | 3.42 | 94.59 | ||||||
| 10 | 0.32 | 2.88 | 97.47 | ||||||
| 11 | 0.28 | 2.53 | 100.00 | ||||||
| Item | Factor 1 | Factor 2 | Factor 3 |
|---|---|---|---|
| item 1 | 0.652 | 0.168 | 0.245 |
| item 2 | 0.610 | 0.168 | 0.179 |
| item 3 | 0.350 | 0.604 | 0.223 |
| item 4 | 0.223 | 0.818 | 0.200 |
| item 5 | 0.190 | 0.761 | 0.180 |
| item 6 | 0.439 | 0.250 | 0.302 |
| item 8 | 0.682 | 0.284 | 0.231 |
| item 9 | 0.205 | 0.172 | 0.718 |
| item 10 | 0.173 | 0.190 | 0.792 |
| item 11 | 0.286 | 0.141 | 0.704 |
| item 12 | 0.276 | 0.213 | 0.589 |
| Information Accessing | Knowledge | Information Appraisal | Food Literacy Score | |
|---|---|---|---|---|
| Descriptive statistics | ||||
| Mean (SD) | 11.36 (4.02) | 8.19 (2.79) | 11.34 (2.40) | 30.89 (7.66) |
| Median (IQR) | 12.00 (4.40) | 9.00 (4.00) | 12.00 (2.00) | 31.60 (8.80) |
| Range | 0–18.00 | 2.00–13.00 | 4.00–16.00 | 6–47 |
| Range of possible scores | 0–19 | 2–13 | 4–16 | 6–48 |
| Correlations | ||||
| HL score | 0.54 ** | 0.22 ** | 0.42 ** | 0.46 ** |
| Frequency of the consumption of food categories | ||||
| Fruit and vegetables | 0.26 ** | 0.24 ** | 0.17 ** | 0.28 ** |
| Meat | 0.05 | 0.09 * | 0.01 | 0.02 |
| Fish | 0.15 ** | 0.17 ** | 0.10 ** | 0.17 ** |
| Industrial sugar products | −0.01 | −0.04 | 0.03 | −0.01 |
| Wholemeal bread | 0.22 ** | 0.20 ** | 0.14 ** | 0.23 ** |
| Nutritional habits | ||||
| Omitting breakfast | −0.14 ** | −0.07 | −0.08 * | −0.12 * |
| Irregular meals | −0.13 ** | −0.12 * | −0.09 * | −0.14 ** |
| Late supper | −0.07 | −0.13 ** | −0.04 | −0.10 * |
| Supper as the most caloric meal | −0.16 ** | −0.11 * | −0.15 ** | −0.20 ** |
| Indexes | Threshold Levels of Indexes | Three-Factor Model (11 Items without Item 7) | One-Factor Model (11 Items without Item 7) |
|---|---|---|---|
| CDFR | <2.0 (p > 0.05) | 3.154 (<0.001) | 15.831 (<0.001) |
| CFI | Acceptable 0.90–0.95, good: 0.97 | 0.972 | 0.775 |
| GFI | Acceptable: ≥0.90 to <0.95, good: ≥0.95 | 0.963 | 0.794 |
| AGFI | Acceptable: ≥0.90 to <0.95, good: ≥0.95 | 0.940 | 0.692 |
| NFI | Acceptable: ≥0.90 to <0.95, good: ≥0.95 | 0.959 | 0.765 |
| RMSEA (90%CI) | Acceptable: <0.08 to 0.05, good: <0.05 | 0.059 (0.047–0.070) | 0.154 (0.144–0.164) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwierczyk, U.; Kobryn, M.; Duplaga, M. Validation of the Short Food Literacy Questionnaire in the Representative Sample of Polish Internet Users. Int. J. Environ. Res. Public Health 2022, 19, 9710. https://doi.org/10.3390/ijerph19159710
Zwierczyk U, Kobryn M, Duplaga M. Validation of the Short Food Literacy Questionnaire in the Representative Sample of Polish Internet Users. International Journal of Environmental Research and Public Health. 2022; 19(15):9710. https://doi.org/10.3390/ijerph19159710
Chicago/Turabian StyleZwierczyk, Urszula, Mateusz Kobryn, and Mariusz Duplaga. 2022. "Validation of the Short Food Literacy Questionnaire in the Representative Sample of Polish Internet Users" International Journal of Environmental Research and Public Health 19, no. 15: 9710. https://doi.org/10.3390/ijerph19159710