
A Simple Resident Need-for-Physical-Assistance Scale in Eldercare: Validation Using 4716 Observation Sequences of Caring Activities

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Population
2.2.1. Observational Data
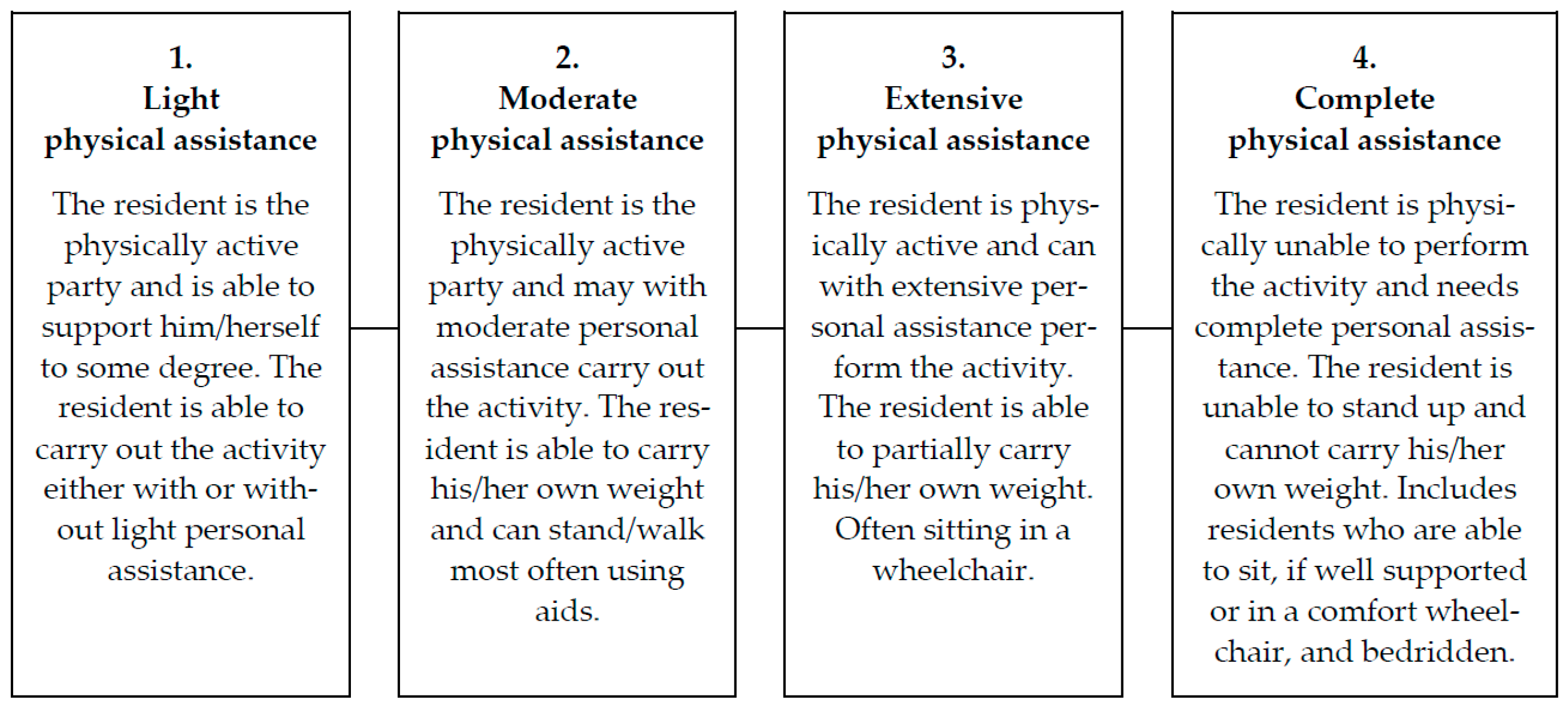
2.2.2. Development of the Scale and Classification of Residents
2.3. Validation Process and Statistical Analysis
3. Results
3.1. Criterion Validity
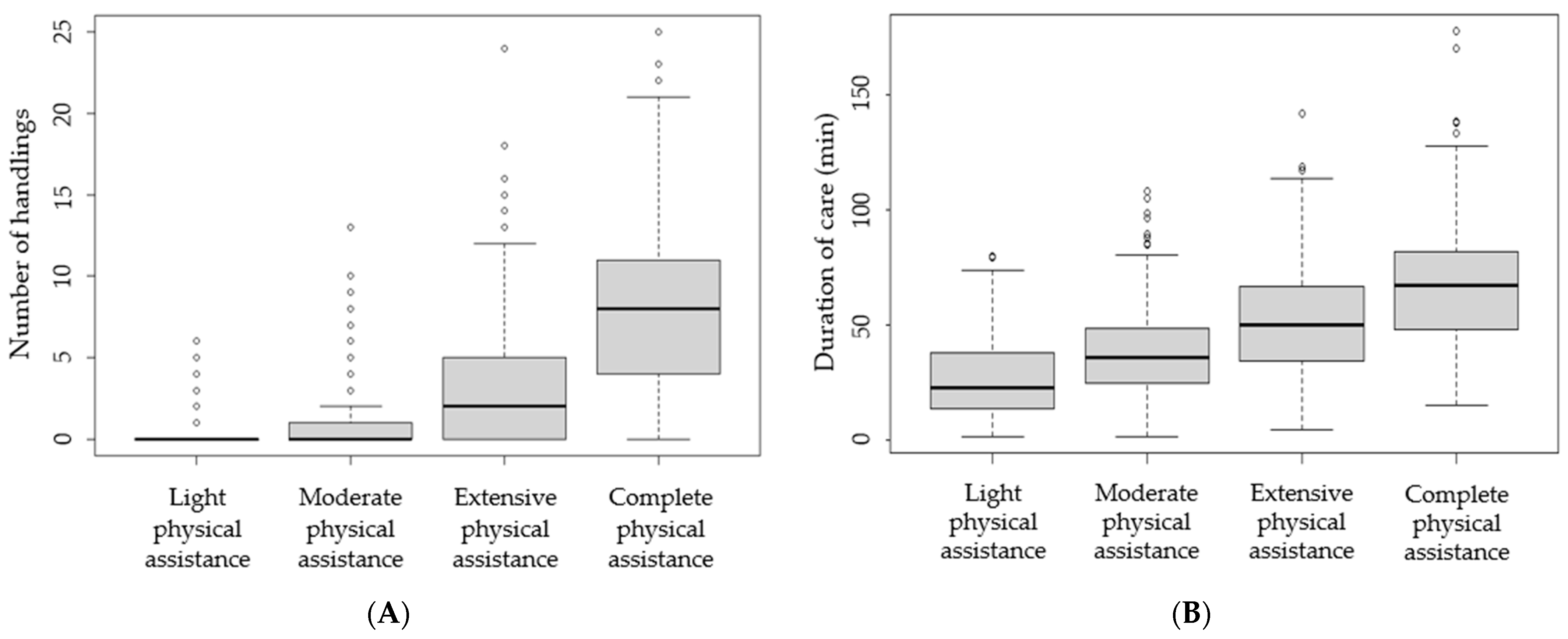
3.2. Discriminative Ability
4. Discussion
4.1. Strength and Limitations
4.2. Practical Implications for Eldercare Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Resident Need-for-Assistance Classification | |||||
|---|---|---|---|---|---|
| All Residents Mean ± SD | Light Physical Assistance Mean ± SD | Moderate Physical Assistance Mean ± SD | Extensive Physical Assistance Mean ± SD | Complete Physical Assistance Mean ± SD | |
| n = 1456 | n = 290 | n = 453 | n = 262 | n = 312 | |
| Day shift | |||||
| Total number of handling activities | 1.9 ± 3.1 | 0.1 ± 0.6 | 0.50 ± 1.3 | 1.9 ± 2.7 | 5.3 ± 3.9 |
| Number of lifting activities | 0.6 ± 1.1 | 0.0 ± 0.2 | 0.2 ± 0.6 | 0.7 ± 1.1 | 1.5 ± 1.3 |
| Number of repositioning activities | 0.64 ± 1.32 | 0.1 ± 0.4 | 0.3 ± 0.7 | 0.7 ± 1.6 | 1.7 ± 2.0 |
| Number of turning activities | 0.7 ± 1.6 | 0.01 ± 0.1 | 0.1 ± 0.4 | 0.5 ± 1.3 | 2.2 ± 2.3 |
| Number of handlings without support from the resident | 1.33 ± 2.77 | 0.1 ± 0.5 | 0.2 ± 0.8 | 1.1 ± 2.4 | 4.33 ± 3.8 |
| Duration of care (min) | 32.0 ± 21.5 | 17.6 ± 15.6 | 25.7 ± 15.6 | 36.9 ± 20.9 | 48.7 ± 21.3 |
| Evening shift | |||||
| Total number of handling activities | 1.1 ± 1.8 | 0.1 ± 0.4 | 0.4 ± 0.9 | 1.2 ± 1.7 | 2.6 ± 2.1 |
| Number of lifting activities | 0.4 ± 0.7 | 0.0 ± 0.1 | 0.1 ± 0.4 | 0.5 ± 0.9 | 0.8 ± 0.9 |
| Number of repositioning activities | 0.4 ± 0.9 | 0.1 ± 0.3 | 0.2 ± 0.6 | 0.5 ± 1.0 | 0.8 ± 1.0 |
| Number of turning activities | 0.4 ± 1.0 | 0.0 ± 0.0 | 0.1 ± 0.3 | 0.2 ± 0.7 | 1.1 ± 1.5 |
| Number of handlings without support from the resident | 0.8 ± 1.5 | 0.0 ± 0.2 | 0.2 ± 0.7 | 0.7 ± 1.3 | 2.1 ± 2.1 |
| Duration of care (min) | 12.7 ± 10.1 | 6.3 ± 6.6 | 10.3 ± 8.4 | 14.3 ± 9.4 | 18.7 ± 11.0 |
| Spearman’s Rho (95% CI) | ROC-AUC * | |
|---|---|---|
| Day shift | ||
| Total number of handling activities | 0.69 (0.65–0.72) | 0.78 |
| Number of lifting activities | 0.60 (0.56–0.64) | 0.72 |
| Number of repositioning activities | 0.48 (0.43–0.52) | 0.68 |
| Number of turning activities | 0.57 (0.53–0.60) | 0.68 |
| Number of handlings without support from the resident | 0.67 (0.64–0.71) | 0.75 |
| Duration of care (min) | 0.54 (0.50–0.59) | 0.75 |
| Evening shift | ||
| Total number of handling activities | 0.61 (0.57–0.65) | 0.74 |
| Number of lifting activities | 0.50 (0.46–0.54) | 0.66 |
| Number of repositioning activities | 0.35 (0.30–0.40) | 0.62 |
| Number of turning activities | 0.49 (0.44–0.53) | 0.64 |
| Number of handlings without support from the resident | 0.61 (0.57–0.64) | 0.72 |
| Duration of care (min) | 0.47 (0.42–0.52) | 0.72 |
References
- Andersen, L.L.; Clausen, T.; Mortensen, O.S.; Burr, H.; Holtermann, A. A prospective cohort study on musculoskeletal risk factors for long-term sickness absence among healthcare workers in eldercare. Int. Arch. Occup. Environ. Health 2012, 85, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.G.; Kotowski, S.E. Prevalence of Musculoskeletal Disorders for Nurses in Hospitals, Long-Term Care Facilities, and Home Health Care: A Comprehensive Review. Hum. Factors 2015, 57, 754–792. [Google Scholar] [CrossRef] [PubMed]
- Bláfoss, R.; Vinstrup, J.; Skovlund, S.V.; López-Bueno, R.; Calatayud, J.; Clausen, T.; Andersen, L.L. Musculoskeletal pain intensity in different body regions and risk of disability pension among female eldercare workers: Prospective cohort study with 11-year register follow-up. BMC Musculoskelet. Disord. 2021, 22, 771. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Clausen, T.; Jørgensen, M.B.; Burdorf, A.; Andersen, L.L. Patient handling and risk for developing persistent low-back pain among female healthcare workers. Scand. J. Work Environ. Health 2013, 39, 164–169. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, T.; Serranheira, F.; Loureiro, H. Work related musculoskeletal disorders in primary health care nurses. Appl. Nurs. Res. ANR 2017, 33, 72–77. [Google Scholar] [CrossRef]
- Coenen, P.; Gouttebarge, V.; van der Burght, A.S.; van Dieën, J.H.; Frings-Dresen, M.H.; van der Beek, A.J.; Burdorf, A. The effect of lifting during work on low back pain: A health impact assessment based on a meta-analysis. Occup. Environ. Med. 2014, 71, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Kyriakidis, S.; Stevens, M.L.; Karstad, K.; Søgaard, K.; Holtermann, A. The Influence of Nursing Home, Ward, and Eldercare Workers on the Number of Resident Handlings Performed per Shift in Eldercare. Int. J. Environ. Res. Public Health 2021, 18, 11040. [Google Scholar] [CrossRef]
- Jørgensen, L.M.; el Kholy, K.; Damkjaer, K.; Deis, A.; Schroll, M. “RAI”—Et internationalt system til vurdering af beboere på plejehjem [“RAI”—An international system for assessment of nursing home residents]. Ugeskr. Laeger 1997, 159, 6371–6376. [Google Scholar]
- Knibbe, J.J.; Friele, R.D. The use of logs to assess exposure to manual handling of patients, illustrated in an intervention study in home care nursing. Int. J. Ind. Ergon. 1999, 24, 445–454. [Google Scholar] [CrossRef] [Green Version]
- Knibbe, J.J.; Knibbe, N.E. An international validation study of the care thermometer: A tool supporting the quality of ergonomic policies in health care. Work 2012, 41 (Suppl. S1), 5639–5641. [Google Scholar] [CrossRef] [Green Version]
- Cantarella, C.; Stucchi, G.; Menoni, O.; Consonni, D.; Cairoli, S.; Manno, R.; Tasso, M.; Galinotti, L.; Battevi, N. MAPO Method to Assess the Risk of Patient Manual Handling in Hospital Wards: A Validation Study. Hum. Factors 2020, 62, 1141–1149. [Google Scholar] [CrossRef]
- Karhula, K.; Rönnholm, T.; Sjögren, T. A method for evaluating the load of patient transfers. Occup. Saf. Health Publ. 2009, 83. Available online: https://www.av.se/globalassets/filer/arbetsmiljoarbete-och-inspektioner/method-for-evaluating–the-load-of-patient-transfers.pdf (accessed on 15 July 2021).
- Karstad, K.; Jørgensen, A.; Greiner, B.A.; Burdorf, A.; Søgaard, K.; Rugulies, R.; Holtermann, A. Danish Observational Study of Eldercare work and musculoskeletal disorderS (DOSES): A prospective study at 20 nursing homes in Denmark. BMJ Open 2018, 8, e019670. [Google Scholar] [CrossRef]
- Koppelaar, E.; Knibbe, J.J.; Miedema, H.S.; Burdorf, A. The influence of individual and organisational factors on nurses’ behaviour to use lifting devices in healthcare. Appl. Ergon. 2013, 44, 532–537. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, L.M.; Jorgensen, A.F.; Thomsen, B.L.; Albertsen, K.; Greiner, B.A.; Rugulies, R. Emotion work within eldercare and depressive symptoms: A cross-sectional multi-level study assessing the association between externally observed emotion work and self-reported depressive symptoms among Danish eldercare workers. Int. J. Nurs. Stud. 2016, 62, 183–192. [Google Scholar] [CrossRef]
- Jakobsen, L.M.; Jorgensen, A.F.; Thomsen, B.L.; Greiner, B.A.; Rugulies, R. A multilevel study on the association of observer-assessed working conditions with depressive symptoms among female eldercare workers from 56 work units in 10 care homes in Denmark. BMJ Open 2015, 5, e008713. [Google Scholar] [CrossRef] [Green Version]
- Park, J.K.; Boyer, J.; Tessler, J.; Casey, J.; Schemm, L.; Gore, R.; Punnett, L. Inter-rater reliability of PATH observations for assessment of ergonomic risk factors in hospital work. Ergonomics 2009, 52, 820–829. [Google Scholar] [CrossRef]
- Johnsson, C.; Kjellberg, K.; Kjellberg, A.; Lagerström, M. A direct observation instrument for assessment of nurses’ patient transfer technique (DINO). Appl. Ergon. 2004, 35, 591–601. [Google Scholar] [CrossRef]
- Warming, S.; Juul-Kristensen, B.; Ebbehøj, N.E.; Schibye, B. An observation instrument for the description and evaluation of patient transfer technique. Appl. Ergon. 2004, 35, 603–614. [Google Scholar] [CrossRef]
- Karstad, K.; Rugulies, R.; Skotte, J.; Munch, P.K.; Greiner, B.A.; Burdorf, A.; Søgaard, K.; Holtermann, A. Inter-rater reliability of direct observations of the physical and psychosocial working conditions in eldercare: An evaluation in the DOSES project. Appl. Ergon. 2018, 69, 93–103. [Google Scholar] [CrossRef]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, C.M.; Athanasiou, T. Summary receiver operating characteristic curve analysis techniques in the evaluation of diagnostic tests. Ann. Thorac. Surg. 2005, 79, 16–20. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Wickham, H.; Miller, E. haven: Import and Export ‘SPSS’, ‘Stata’ and ‘SAS’ Files; R Package Version 2.4.0; 2021; Available online: https://CRAN.R-project.org/package=haven. (accessed on 15 July 2021).
- Wickham, H.; François, R.; Henry, L.; Müller, K. dplyr: A Grammar of Data Manipulation; R Package Version 1.0.5; 2021; Available online: https://CRAN.R-project.org/package=dplyr (accessed on 15 July 2021).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Hervé, M. RVAideMemoire: Testing and Plotting Procedures for Biostatistics; R Package Version 0.9-79; 2021; Available online: https://CRAN.R-project.org/package=RVAideMemoire (accessed on 15 July 2021).
- Clausen, T.; Tufte, P.; Borg, V. Why are they leaving? Causes of actual turnover in the Danish eldercare services. J. Nurs. Manag. 2014, 22, 583–592. [Google Scholar] [CrossRef]
- National Labour Market Board. Rekruttering. 1. Halvår 2009 [Recruitment. 1st. Half of the Year 2009]; Arbejdsmarkedsstyrelsen [The National Labour Market Board]: Copenhagen, Denmark, 2009; Available online: https://star.dk/media/1367/rekruttering-foraar-2009.pdf (accessed on 15 July 2021).
- Januario, L.B.; Mathiassen, S.E.; Stevens, M.L.; Holtermann, A.; Bergström, G.; Rugulies, R.; Karstad, K.; Hallman, D.M. Are resident handlings in eldercare wards associated with musculoskeletal pain and sickness absence among the workers? A prospective study based on onsite observations. Scand. J. Work Environ. Health 2021, 47, 609–618. [Google Scholar] [CrossRef]

| Resident Need-for-Assistance Classification | |||||
|---|---|---|---|---|---|
| All Residents Mean ± SD | Light Physical Assistance Mean ± SD | Moderate Physical Assistance Mean ± SD | Extensive Physical Assistance Mean ± SD | Complete Physical Assistance Mean ± SD | |
| n = 1456 | n = 290 | n = 453 | n = 262 | n = 312 | |
| Resident body weight (kg) | 65.46 ± 15.14 | 66.49 ± 15.49 | 64.85 ± 14.56 | 66.20 ± 15.86 | 64.78 ± 15.05 |
| Whole day | |||||
| Total number of handling activities | 3.2 ± 4.5 | 0.3 ± 0.9 | 0.9 ± 1.9 | 3.1 ± 3.7 | 8.1 ± 5.0 |
| Number of lifting activities | 1.0 ± 1.6 | 0.1 ± 0.3 | 0.3 ± 0.8 | 1.2 ± 1.6 | 2.3 ± 1.8 |
| Number of repositioning activities | 1.1 ± 1.8 | 0.2 ± 0.7 | 0.5 ± 1.0 | 1.2 ± 1.6 | 2.4 ± 3.4 |
| Number of turning activities | 1.1 ± 2.3 | 0.0 ± 0.2 | 0.2 ± 0.7 | 0.8 ± 1.8 | 3.3 ± 3.1 |
| Number of handlings without support from the resident | 2.3 ± 4.0 | 0.1 ± 0.6 | 0.4 ± 1.3 | 1.8 ± 3.2 | 6.5 ± 5.0 |
| Duration of care (min) | 46.9 ± 26.8 | 27.1 ± 18.5 | 36.9 ± 19.4 | 51.7 ± 24.2 | 67.8 ± 25.5 |
| Spearman’s Rho (95% CI) | ROC-AUC * | |
|---|---|---|
| Whole day | ||
| Total number of handling activities | 0.71 (0.67–0.74) | 0.81 |
| Number of lifting activities | 0.63 (0.59–0.66) | 0.74 |
| Number of repositioning activities | 0.52 (0.47–0.57) | 0.71 |
| Number of turning activities | 0.61 (0.57–0.65) | 0.71 |
| Number of handlings without support from the resident | 0.71 (0.67–0.73) | 0.78 |
| Duration of care (min) | 0.57 (0.52–0.61) | 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacobsen, S.S.; Stevens, M.L.; Karstad, K.; Rasmussen, C.D.N.; Kühnel, A.B.; Holtermann, A. A Simple Resident Need-for-Physical-Assistance Scale in Eldercare: Validation Using 4716 Observation Sequences of Caring Activities. Int. J. Environ. Res. Public Health 2022, 19, 10488. https://doi.org/10.3390/ijerph191710488
Jacobsen SS, Stevens ML, Karstad K, Rasmussen CDN, Kühnel AB, Holtermann A. A Simple Resident Need-for-Physical-Assistance Scale in Eldercare: Validation Using 4716 Observation Sequences of Caring Activities. International Journal of Environmental Research and Public Health. 2022; 19(17):10488. https://doi.org/10.3390/ijerph191710488
Chicago/Turabian StyleJacobsen, Sandra Schade, Matthew Leigh Stevens, Kristina Karstad, Charlotte Diana Nørregaard Rasmussen, Alexander Bork Kühnel, and Andreas Holtermann. 2022. "A Simple Resident Need-for-Physical-Assistance Scale in Eldercare: Validation Using 4716 Observation Sequences of Caring Activities" International Journal of Environmental Research and Public Health 19, no. 17: 10488. https://doi.org/10.3390/ijerph191710488
APA StyleJacobsen, S. S., Stevens, M. L., Karstad, K., Rasmussen, C. D. N., Kühnel, A. B., & Holtermann, A. (2022). A Simple Resident Need-for-Physical-Assistance Scale in Eldercare: Validation Using 4716 Observation Sequences of Caring Activities. International Journal of Environmental Research and Public Health, 19(17), 10488. https://doi.org/10.3390/ijerph191710488