
Secular Trends of Mortality and Years of Life Lost Due to Chronic Obstructive Pulmonary Disease in Wuhan, China from 2010 to 2019: Age-Period-Cohort Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
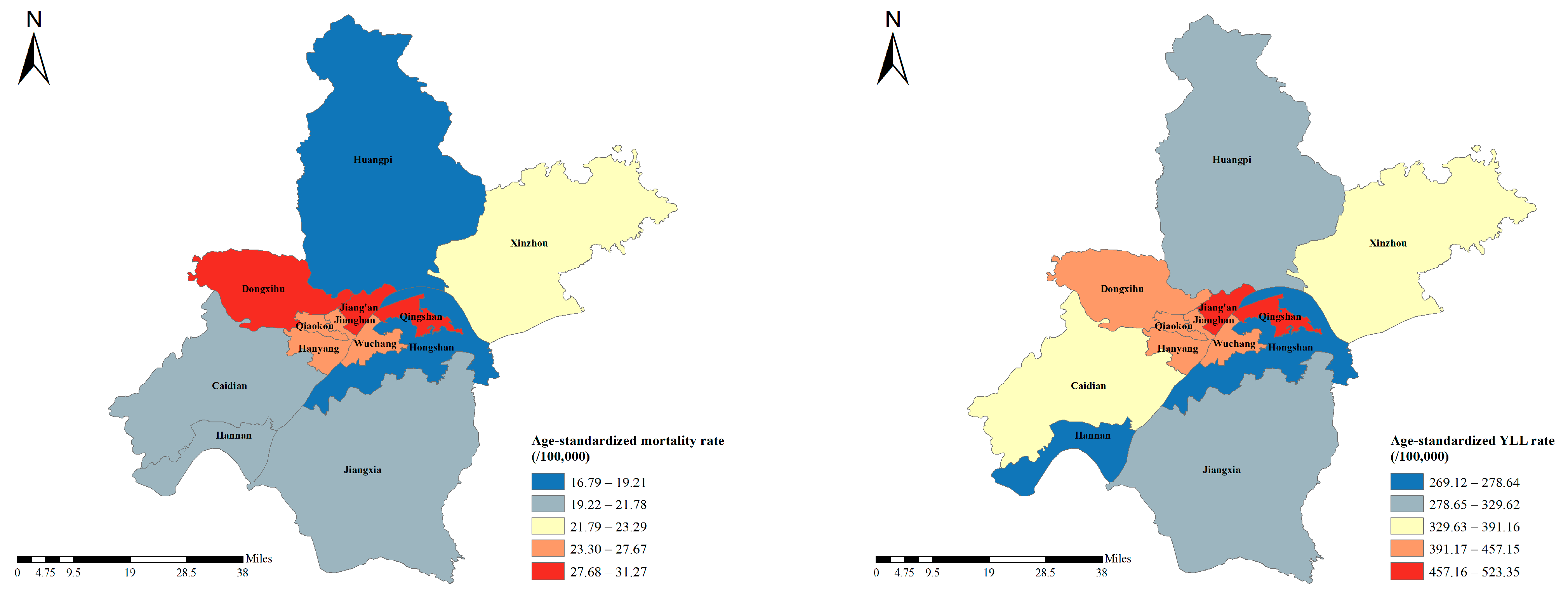
3.1. Spatial–Temporal Patterns of COPD Burden
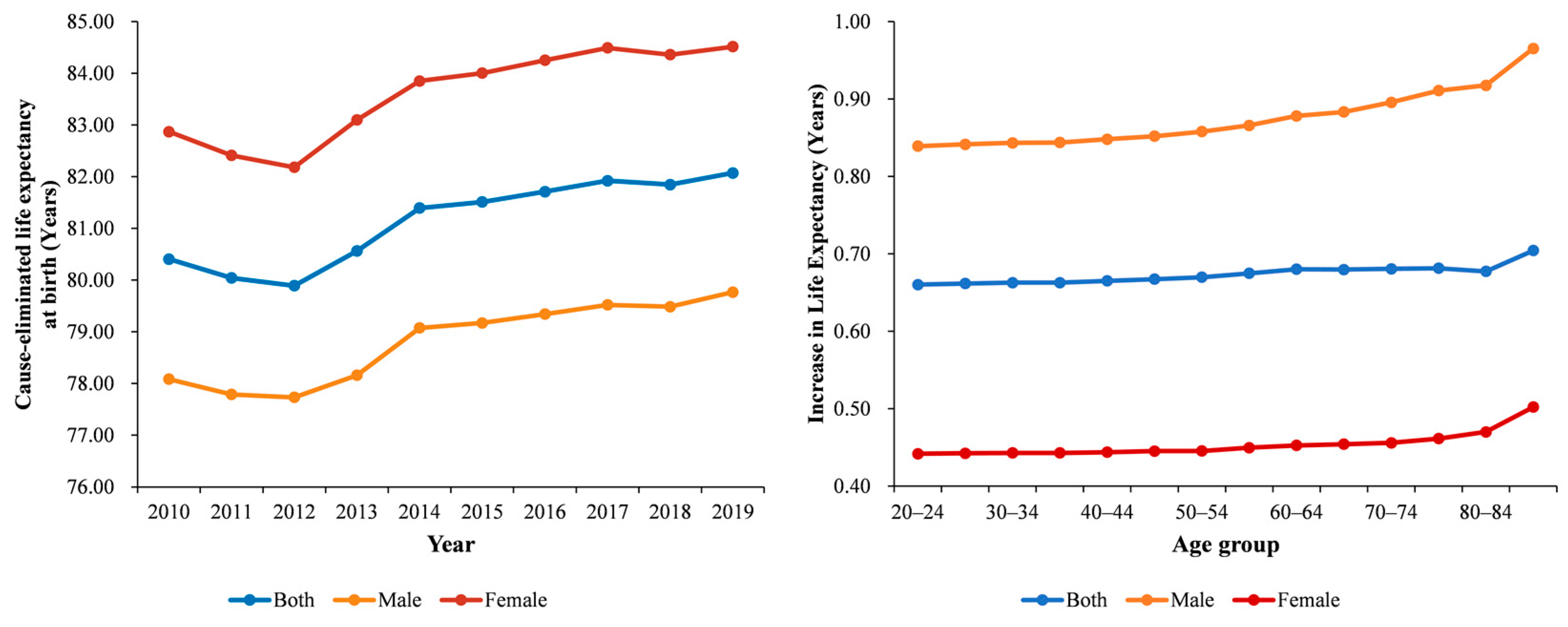
3.2. Life Expectancy and COPD Burden by Ages and Sex
3.3. The Age, Period, and Cohort Effects on COPD Mortality and YLL Rate
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diem, G.; Brownson, R.C.; Grabauskas, V.; Shatchkute, A.; Stachenko, S. Prevention and control of noncommunicable diseases through evidence-based public health: Implementing the NCD 2020 action plan. Glob. Health Promot. 2016, 23, 5–13. [Google Scholar] [CrossRef]
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- Adeloye, D.; Chua, S.; Lee, C.; Basquill, C.; Papana, A.; Theodoratou, E.; Nair, H.; Gasevic, D.; Sridhar, D.; Campbell, H.; et al. Global and regional estimates of COPD prevalence: Systematic review and meta-analysis. J. Glob. Health 2015, 5, 020415. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 394, 1145–1158. [Google Scholar] [CrossRef]
- Liu, W.; Wang, W.; Liu, J.; Liu, Y.; Meng, S.; Wang, F.; Long, Z.; Qi, J.; You, J.; Lin, L.; et al. Trend of Mortality and Years of Life Lost Due to Chronic Obstructive Pulmonary Disease in China and Its Provinces, 2005–2020. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 2973–2981. [Google Scholar] [CrossRef]
- Mubarik, S.; Yu, Y.; Wang, F.; Malik, S.S.; Liu, X.; Fawad, M.; Shi, F.; Yu, C. Epidemiological and sociodemographic transitions of female breast cancer incidence, death, case fatality and DALYs in 21 world regions and globally, from 1990 to 2017: An Age-Period-Cohort Analysis. J. Adv. Res. 2022, 37, 185–196. [Google Scholar] [CrossRef]
- Sun, L.; Zhou, Y.; Zhang, M.; Li, C.; Qu, M.; Cai, Q.; Meng, J.; Fan, H.; Zhao, Y.; Hu, D. Association of Major Chronic Noncommunicable Diseases and Life Expectancy in China, 2019. Healthcare 2022, 10, 296. [Google Scholar] [CrossRef]
- Yang, Y. Trends in U.S. adult chronic disease mortality, 1960–1999: Age, period, and cohort variations. Demography 2008, 45, 387–416. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.W. Age-Period-Cohort Analysis: New Models, Methods, and Empirical Applications. J. Am. Stat. Assoc. 2014, 109, 865. [Google Scholar]
- Wang, P.; Xu, C.; Yu, C. Age-period-cohort analysis on the cancer mortality in rural China: 1990–2010. Int. J. Equity Health 2014, 13, 1. [Google Scholar] [CrossRef]
- Jinhong, C.; Eshak, E.S.; Keyang, L.; Krisztina, G.; Zhiming, L.; Chuanhua, Y. Age-Period-Cohort Analysis of Stroke Mortality Attributable to High Sodium Intake in China and Japan. Stroke 2019, 50, 1648–1654. [Google Scholar] [CrossRef]
- Yin, P.; Wu, J.; Wang, L.; Luo, C.; Ouyang, L.; Tang, X.; Liu, J.; Liu, Y.; Qi, J.; Zhou, M.; et al. The Burden of COPD in China and Its Provinces: Findings from the Global Burden of Disease Study 2019. Front. Public Health 2022, 10, 859499. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xu, J.; Yang, L.; Xu, Y.; Zhang, X.; Bai, C.; Kang, J.; Ran, P.; Shen, H.; Wen, F.; et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): A national cross-sectional study. Lancet 2018, 391, 1706–1717. [Google Scholar] [CrossRef]
- Kokturk, N.; Kilic, H.; Baha, A.; Lee, S.D.; Jones, P.W. Sex Difference in Chronic Obstructive Lung Disease. Does it Matter? A Concise Review. COPD J. Chronic Obstr. Pulm. Dis. 2016, 13, 799–806. [Google Scholar] [CrossRef]
- Xie, L.; Qian, Y.; Liu, Y.; Li, Y.; Jia, S.; Yu, H.; Wang, C.; Qian, B.; Bao, P. Distinctive lung cancer incidence trends among men and women attributable to the period effect in Shanghai: An analysis spanning 42 years. Cancer Med. 2020, 9, 2930–2939. [Google Scholar] [CrossRef]
- Matera, M.G.; Ora, J.; Calzetta, L.; Rogliani, P.; Cazzola, M. Sex differences in COPD management. Expert Rev. Clin. Pharmacol. 2021, 14, 323–332. [Google Scholar] [CrossRef]
- Siegfried, J.M. Sex and Gender Differences in Lung Cancer and Chronic Obstructive Lung Disease. Endocrinology 2022, 163, bqab254. [Google Scholar] [CrossRef]
- Yan, Y.; She, L.; Guo, Y.; Zhao, Y.; Zhang, P.; Xiang, B.; Zeng, J.; Yang, M.; Wang, L. Association between ambient air pollution and mortality from chronic obstructive pulmonary disease in Wuhan, China: A population-based time-series study. Environ. Sci. Pollut. Res. Int. 2021, 28, 33698–33706. [Google Scholar] [CrossRef] [PubMed]
- Schikowski, T.; Mills, I.C.; Anderson, H.R.; Cohen, A.; Hansell, A.; Kauffmann, F.; Krämer, U.; Marcon, A.; Perez, L.; Sunyer, J.; et al. Ambient air pollution: A cause of COPD? Eur. Respir. J. 2014, 43, 250–263. [Google Scholar] [CrossRef]
- Liu, S.; Zhou, Y.; Liu, S.; Chen, X.; Zou, W.; Zhao, D.; Li, X.; Pu, J.; Huang, L.; Chen, J.; et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: Results from a cross-sectional study in China. Thorax 2017, 72, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Li, M.-H.; Fan, L.-C.; Mao, B.; Yang, J.-W.; Choi, A.M.K.; Cao, W.-J.; Xu, J.-F. Short-term Exposure to Ambient Fine Particulate Matter Increases Hospitalizations and Mortality in COPD: A Systematic Review and Meta-analysis. Chest 2016, 149, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef]
- Tao, F.; Gonzalez-Flecha, B.; Kobzik, L. Reactive oxygen species in pulmonary inflammation by ambient particulates. Free Radic. Biol. Med. 2003, 35, 327–340. [Google Scholar] [CrossRef]
- Liu, C.-W.; Lee, T.-L.; Chen, Y.-C.; Liang, C.-J.; Wang, S.-H.; Lue, J.-H.; Tsai, J.-S.; Lee, S.-W.; Chen, S.-H.; Yang, Y.-F.; et al. PM(2.5)-induced oxidative stress increases intercellular adhesion molecule-1 expression in lung epithelial cells through the IL-6/AKT/STAT3/NF-κB-dependent pathway. Part. Fibre Toxicol. 2018, 15, 4. [Google Scholar] [CrossRef]
- Zhao, J.; Li, M.; Wang, Z.; Chen, J.; Zhao, J.; Xu, Y.; Wei, X.; Wang, J.; Xie, J. Role of PM(2.5) in the development and progression of COPD and its mechanisms. Respir. Res. 2019, 20, 120. [Google Scholar] [CrossRef]
- Easter, M.; Bollenbecker, S.; Barnes, J.W.; Krick, S. Targeting Aging Pathways in Chronic Obstructive Pulmonary Disease. Int. J. Mol. Sci. 2020, 21, 6924. [Google Scholar] [CrossRef]
- Lahousse, L.; Seys, L.J.M.; Joos, G.F.; Franco, O.H.; Stricker, B.H.; Brusselle, G.G. Epidemiology and impact of chronic bronchitis in chronic obstructive pulmonary disease. Eur. Respir. J. 2017, 50, 1602470. [Google Scholar] [CrossRef]
- Fragoso, C.A. Epidemiology of Chronic Obstructive Pulmonary Disease (COPD) in Aging Populations. COPD J. Chronic Obstr. Pulm. Dis. 2016, 13, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Brandsma, C.A.; de Vries, M.; Costa, R.; Woldhuis, R.R.; Königshoff, M.; Timens, W. Lung ageing and COPD: Is there a role for ageing in abnormal tissue repair? Eur. Respir. Rev. 2017, 26, 170073. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Xu, X.; Jiang, L. A Preliminary Study on Planning Response to Population Aging in Wuhan City. Chin. Overseas Archit. 2012, 5, 99–100. [Google Scholar] [CrossRef]
- Zhang, L. Impact of Population Aging on Wuhan City Pension Fund. Ploneering Sci. Technol. Mon. 2015, 28, 56–58. [Google Scholar] [CrossRef]
- Li, J.; Zhao, H. Wuhan City Promotes “Five Combinations” of National Education on Population Aging. China Soc. Work. 2018, 20, 18–19. [Google Scholar]
- Zhu, B.; Wang, Y.; Ming, J.; Chen, W.; Zhang, L. Disease burden of COPD in China: A systematic review. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 1353–1364. [Google Scholar] [CrossRef]
- Bai, J.; Zhao, Y.; Yang, D.; Ma, Y.; Yu, C. Secular trends in chronic respiratory diseases mortality in Brazil, Russia, China, and South Africa: A comparative study across main BRICS countries from 1990 to 2019. BMC Public Health 2022, 22, 91. [Google Scholar] [CrossRef]
- Lu, Y.; Li, J.; Huang, Y.; Li, Y.; Zhang, L.; Peng, L.; Mei, X.; Chen, M.; Deng, Z. Survey on tobacco prevalence among urban residents in Wuhan City. Chin. J. Health Educ. 2018, 34, 4. [Google Scholar] [CrossRef]
- Wu, C.; Deng, Z. Epidemiologic status survey on tobacco epidemic among residents aged 15 and above of Wuhan in 2015. Mod. Prev. Med. 2018, 45, 5. [Google Scholar]
- Ni, L.; Chuang, C.C.; Zuo, L. Fine particulate matter in acute exacerbation of COPD. Front. Physiol. 2015, 6, 294. [Google Scholar] [CrossRef]
- Cho, S.J.; Stout-Delgado, H.W. Aging and Lung Disease. Annu. Rev. Physiol. 2020, 82, 433–459. [Google Scholar] [CrossRef] [PubMed]
- Bush, A. Lung Development and Aging. Ann. Am. Thorac. Soc. 2016, 13 (Suppl. S5), S438–S446. [Google Scholar] [CrossRef]
- Rusconi, F.; Galassi, C.; Forastiere, F.; Bellasio, M.; De Sario, M.; Ciccone, G.; Brunetti, L.; Chellini, E.; Corbo, G.; La Grutta, S.; et al. Maternal complications and procedures in pregnancy and at birth and wheezing phenotypes in children. Am. J. Respir. Crit. Care Med. 2007, 175, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Wright, R.J. Prenatal stress and childhood asthma risk: Taking a broader view. Eur. Respir. J. 2016, 47, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Wen, H.; Xie, C.; Wang, L.; Wang, F.; Wang, Y.; Liu, X.; Yu, C. Difference in Long-Term Trends in COPD Mortality between China and the U.S.; 1992–2017: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1529. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | ASMR Per 100,000 No. (95% UI) | EAPC No. (95% CI) | ASYR Per 100,000 No. (95% UI) | EAPC No. (95% CI) | ||
|---|---|---|---|---|---|---|
| 2010 | 2019 | 2010 | 2019 | |||
| Overall | 25.65 (24.52, 26.82) | 24.74 (23.82, 25.72) | 0.31 (−1.14, 1.79) | 420.25 (415.55, 424.98) | 404.20 (400.29, 408.16) | 0.32 (−1.24, 1.92) |
| Sex | ||||||
| Male | 36.96 (34.95, 39.06) | 39.6 (37.87, 41.44) | 1.06 (0.13, 2.00) | 610.8 (602.51, 619.17) | 659.07 (909.03, 651.77) | 1.21 (0.12, 2.31) |
| Female | 16.32 (15.13, 17.59) | 12.18 (11.34, 13.16) | −1.67 (−4.26, 0.98) | 252.01 (247.08, 257.03) | 177.36 (319.25, 173.92) | −2.14 (−4.95, 0.74) |
| Regions | ||||||
| Caidian | 16.52 (12.87, 21.01) | 21.7 (17.87, 26.77) | 8.39 (−0.40, 17.95) | 291.83 (275.33, 309.12) | 364.39 (347.81, 382.07) | 8.28 (−1.07, 18.52) |
| Dongxihu | 49.27 (39.44, 60.92) | 30.66 (24.96, 38.58) | −0.50 (−7.31, 6.82) | 773.02 (732.51, 815.29) | 449.48 (426.53, 474.33) | −2.15 (−9.11, 5.35) |
| Hannan | 83.45 (70.05, 98.79) | 20.19 (15.26, 28.04) | −10.57 (−14.14, −6.87) | 1265.76 (1211.04, 1322.39) | 278.64 (259.08, 300.56) | −10.97 (−14.62, −7.15) |
| Hanyang | 30.36 (25.4, 36.20) | 26.05 (22.32, 31.73) | −0.08 (−2.68, 2.6) | 530.34 (508.55, 552.97) | 433.99 (417.72, 451.79) | −0.34 (−2.73, 2.12) |
| Hongshan | 34.90 (30.23, 40.36) | 16.79 (14.38, 19.69) | −5.84 (−10.19, −1.28) | 574.6 (554.79, 595.17) | 269.12 (258.75, 279.95) | −6.34 (−10.8, −1.65) |
| Huangpi | 15.56 (13.16, 18.29) | 19.21 (16.82, 22.01) | 3.92 (−0.39, 8.43) | 269.28 (258.81, 280.09) | 329.62 (319.19, 340.42) | 3.97 (−0.52, 8.65) |
| Jiang’an | 24.50 (21.32, 28.2) | 29.76 (26.72, 33.93) | 2.23 (−1.32, 5.9) | 401.61 (387.79, 415.95) | 501.97 (488.53, 516.34) | 2.77 (−0.49, 6.15) |
| Jianghan | 29.42 (24.92, 34.72) | 26.78 (23.18, 32.11) | −2.84 (−5.47, −0.13) | 485.59 (466.03, 505.94) | 457.15 (440.98, 474.71) | −2.58 (−5.03, −0.06) |
| Jiangxia | 36.37 (31.07, 42.36) | 21.78 (18.21, 26.1) | −4.02 (−7.2, −0.73) | 602.57 (580, 625.82) | 323.22 (308.67, 338.49) | −4.96 (−8.71, −1.06) |
| Qiaokou | 34.93 (30.7, 39.8) | 26.38 (23.05, 31.22) | −3.39 (−4.49, −2.27) | 502 (485.05, 519.58) | 433.38 (418.53, 449.46) | −2.98 (−4.8, −1.12) |
| Qingshan | 37.02 (31.47, 43.37) | 31.27 (27.53, 36.96) | 3.44 (−2.3, 9.53) | 573.58 (551.53, 596.4) | 523.35 (506.75, 541.47) | 4.66 (−1.47, 11.17) |
| Wuchang | 15.42 (13.1, 18.13) | 27.67 (25.1, 30.89) | 4.62 (1.93, 7.37) | 241.96 (232.3, 252.01) | 452.72 (441.42, 464.58) | 4.90 (1.58, 8.32) |
| Xinzhou | 9.48 (7.45, 11.92) | 23.29 (20.44, 26.59) | 4.38 (−4.08, 13.58) | 191.18 (181.62, 201.14) | 391.16 (379.11, 403.65) | 3.15 (−4.90, 11.88) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Bai, J.; Zhang, X.; Jin, Q.; Liu, Y.; Yu, C. Secular Trends of Mortality and Years of Life Lost Due to Chronic Obstructive Pulmonary Disease in Wuhan, China from 2010 to 2019: Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10685. https://doi.org/10.3390/ijerph191710685
Guo Y, Bai J, Zhang X, Jin Q, Liu Y, Yu C. Secular Trends of Mortality and Years of Life Lost Due to Chronic Obstructive Pulmonary Disease in Wuhan, China from 2010 to 2019: Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health. 2022; 19(17):10685. https://doi.org/10.3390/ijerph191710685
Chicago/Turabian StyleGuo, Yan, Jianjun Bai, Xiaoxia Zhang, Qiman Jin, Yijun Liu, and Chuanhua Yu. 2022. "Secular Trends of Mortality and Years of Life Lost Due to Chronic Obstructive Pulmonary Disease in Wuhan, China from 2010 to 2019: Age-Period-Cohort Analysis" International Journal of Environmental Research and Public Health 19, no. 17: 10685. https://doi.org/10.3390/ijerph191710685
APA StyleGuo, Y., Bai, J., Zhang, X., Jin, Q., Liu, Y., & Yu, C. (2022). Secular Trends of Mortality and Years of Life Lost Due to Chronic Obstructive Pulmonary Disease in Wuhan, China from 2010 to 2019: Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health, 19(17), 10685. https://doi.org/10.3390/ijerph191710685