Abstract
Background: Conventional and newly emerged intravesical modalities have demonstrated prophylactic effectiveness that may improve quality of life (QoL) in non-muscle invasive bladder cancer. The purpose of this study is to analyze existing QoL evidence in patients receiving any form of intravesical therapy. Methods: A PubMed search without time restriction was conducted to identify all relevant studies in accordance with the PICOT question. Additionally, a search was also performed in the Cochrane library database, Internet, and citation. The CONSORT 2010 checklist and STROBE statement checklist were used to evaluate the risk of bias of the included studies. Results: A total of 24 eligible articles were included, which consisted of 11 interventional and 13 observational studies. Intravesical therapy with Bacillus Calmette–Guérin (BCG) or certain chemotherapeutic agents worsens symptom burdens and functional performance during the initial induction phase while continuous improved is observed throughout the maintenance treatment and beyond. Hyperthermia has shown a positive trend in enhancing QoL of patients receiving intravesical chemotherapy, which requires more investigations. However, QoL data were unavailable for other forms of immunotherapy, immune checkpoint inhibitors, electromotive drug administration, and photodynamic therapy. Conclusions: Limited studies suggested the long-term positive impact of intravesical BCG immunotherapy and chemotherapy. However, existing evidence was lacking to clarify the impact of many emerging intravesical therapies that have suggested to be effective and safe, which demands treatment-specific QoL studies.
1. Introduction
Bladder cancer ranked the 10th most common cancer with 573,000 newly diagnosed cases worldwide in 2020, which is dominated by men at approximately 4 times higher prevalence than women [1]. Non-muscle invasive bladder cancer (NMIBC) accounts for approximately 70% of new cases of bladder cancer, which consists of three early-stage diseases: papillary transition carcinoma (Ta), flat carcinoma in situ (CIS), and cancer confined to the submucosa (T1) [2]. Despite having transurethral resection of bladder tumor (TURBT) as a curative-intent treatment, the 1-year and 5-year recurrence rates remain high at 15–61% and 31–78%, respectively [3], whilst 20–25% of initially NMIBC would progress to muscle-invasive stages during the lifetime, which is indicative for radical cystectomy resulting in urinary diversion to impair patients’ quality of life (QoL) [4,5]. Adjuvant prophylactic chemo- or immunotherapy is often provided to NMIBC patients following TURBT [6]. A recent survey conducted in Brazil reported that almost 79% and 35% of urologists utilized adjuvant intravesical therapy in their patients with high-risk and low-risk bladder cancer [7]. Frequent relapses of the disease require long-term surveillance follow-up accompanied with protracted course of treatment and care that compromises patients’ QoL [8].
Many researchers [6,8,9,10,11] have reviewed QoL during the NMIBC trajectory, but existing treatment-specific QoL studies were mainly restricted to muscle-invasive progression [10,12] or cystectomy [10]. Efficacies of various intravesical agents used for NMIBC were evaluated in systematic reviews, whereas QoL outcomes were usually missing [13]. Intravesical instillation maximizes lesions exposure to the therapeutic agent at lower dosage since it does not involve absorption and systematic metabolism [14]. Despite numerous receptors expressed on the surface bladder urothelium also facilitating some of the therapeutic actions to take place, treatment efficacy is largely dependent on effective drug penetration into bladder tumors prevented by the distinctive tight junction and negatively charged glycosaminoglycan (GAG) layer [14,15]. Chemical and physical strategies such as electromotive drug administration (EMDA) are trending modalities used for improving the permeability of instilled drugs [14,15]. However, lacking data of disease-specific QoL has restricted quantitative analysis in other systematic reviews reporting individual intravesical treatment modalities, including chemotherapy [16,17], immunotherapy [18,19,20,21], and EMDA [22]. The critical review by Botteman et al. [23] summarized the findings of two prospective cohort studies and concluded that post-TURBT intravesical BCG instillation has no serious impact on life satisfaction with NMIBC patients, notwithstanding some unpleasant micturition symptoms experienced at the initial stage while these symptoms were improved into the maintenance phase. The latest systematic review [8] shared the same insight while inconclusive evidence has suggested alternative intravesical treatment for better QoL. Furthermore, two phase III effectiveness trials that reported patient experience during intravesical instillation were identified in another systematic review [24], which only summarized the QoL instruments and methods instead of the outcomes.
Even though Bacillus Calmette–Guérin (BCG) remains as an effective intravesical agent for treating NMIBC after 40 years of practice, new modalities have emerged demonstrating at least comparable prophylactic effectiveness but fewer toxicities, and circumvent the need for radical cystectomy in progressed cases that may improve patients’ QoL [25,26]. Aside from modifying the treatment schedule and dosage of current intravesical agents, current boosting strategies include sequential and combination therapy [19,20], hyperthermia [27,28,29], and EMDA [22,30] that required devices to assisted drug delivery, priming immune checkpoint blockade [31], and novel photodynamic approaches [32,33]. However, the QoL impact of these effective intravesical treatments has not been addressed. The current systematic review is conducted to gather such information.
2. Materials and Methods
This systematic review methodology followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines [34]. The PICOT question ‘Are NMIBC patients (P) who have received intravesical therapy (I) compared with those without or received other treatments (C) experiencing better quality of life (O) throughout the cancer trajectory (T)?’ was used to guide the search strategy and evidence acquisition process.
In May 2022, a PubMed search without time restriction was conducted using the formulated search terms algorithm developed from Medical Subject Headings (MeSH) to identify all relevant studies in accordance with the PICOT components:
- Population (P): (“carcinoma, transitional cell” [MeSH Terms] OR (“urinary bladder neoplasms/drug therapy” [MeSH Terms] OR “urinary bladder neoplasms/prevention and control” [MeSH Terms] OR “urinary bladder neoplasms/therapy” [MeSH Terms]) OR “Bladder cancer” [All Fields] OR “urothelial cancer” [All Fields] OR “Non-muscle invasive bladder cancer” [All Fields] OR “NMIBC” [All Fields] OR “urinary bladder neoplasm*” [All Fields])
- Intervention (I) and (C): (“Immunotherapy” [MeSH Terms] OR “chemotherapy, adjuvant” [MeSH Terms] OR “Drug therapy” [MeSH Terms] OR “intravesical therap*” [All Fields] OR “immunotherap*” [All Fields] OR “chemotherap*” [All Fields] OR “drug therap*” [All Fields] OR “electromotive drug administration” [All Fields] OR “EMDA” [All Fields] OR “Photochemotherapy” [MeSH Terms] OR “Aminolevulinic Acid” [MeSH Terms] OR “5-ALA” [All Fields] OR “ALA” [All Fields] OR “Photodynamic” [All Fields] OR “PDT” [All Fields] OR “PDD” [All Fields] OR “thermochemother*” [All Fields] OR “Hyperthermia” [MeSH Terms] OR “hyperthermia, induced” [MeSH Terms] OR “hyperther*” [All Fields])
- Outcome (O): (“Quality of life” [Title/Abstract] OR “Quality of life” [MeSH Terms]”)
Search terms for (I) and (C) included all existing intravesical therapeutic approaches and were identical because studies may compare between different forms of intravesical therapies. No search terms for the time (T) component were created for maximizing the outcome to cover the whole caner trajectory period. The Boolean operator “AND” was used to combine the sets of search terms between PICOT components. The Cochrane library database, Internet, and citation searching was also conducted.
Two independent reviewers (J.W.Y. and R.W.W.) carried out the two-step process: (1) title/abstract screening and (2) further full-text assessment following duplication removal, according to the eligibility criteria. Any disagreements were resolved through discussion among the reviewers and team consensus. The same procedure also applied to the quality assessment and data extraction of selected studies. The eligibility criteria were:
- Original research articles reporting full or part of interventional and observational studies (e.g., pilot clinical trial, baseline profile of cohort study) encompassed at least one arm of intravesical therapy in analysis,
- Involved NMIBC patients at stage of T0-1 and CIS of any tumor grades,
- Operationization of main QoL variables, and
- Studies in English language.
In contrast, studies reported a mixed population of NMIBC and advanced stage patients were excluded.
2.1. Assessment of Quality and Risk of Bias
Quality of the selected studies was assessed using the CONSORT 2010 checklist for interventional studies and the STROBE statement checklist for observational studies. Risk of bias results of each individual study were charted.
2.2. Data Extraction and Synthesis
One reviewer (J.W.Y.) extracted data, which was cross-checked by a second reviewer (S.S.C.). The following information was recorded: first author, publication year, study design, cancer stage and grade condition, intravesical agents used, comparison groups and sample size, QoL instruments variables used, time points of measurement, and main findings. The main findings recorded outcomes of general and bladder cancer treatment-specific QoL variables, numeric (e.g., percentage, mean scores, standard deviations) or categorical (e.g., Likert, satisfaction level) expressions, significance levels, changes, and trends among study groups and time points of measurement. Relevant information was also extracted from the supplementary documents of individual studies.
3. Results
3.1. Search Results and Study Selection
3.1.1. Characteristics of Included Studies
As summarized in the PRISMA flow diagram (Figure 1), the literature search conducted in May 2022 identified 585 records following removal of duplicates. Among the 91 full-text records retrieved and assessed against the eligibility criteria, 66 of them were excluded with 48 due to lacking QoL outcome measures, 11 for not including a study arm of intravesical therapy or NMIBC in the reports, and 8 were not original studies. All eligible studies were in quantitative research design, except for one cross-sectional that used a mixed method approach including a quantitative survey and qualitative interview [35].
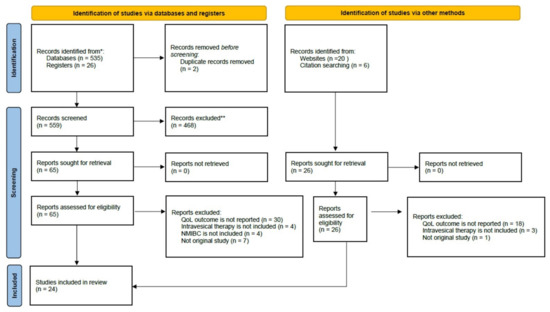
Figure 1.
The process of literature screening and selection presented using the PRISMA 2020 flow diagram. * PubMed and the Cochrane library database; ** Studies did not involve NMIBC patients, did not include quality-of-life as outcome measures, and non-English publications.
Table 1 summarizes the detailed characteristics of the 24 studies. They were published from 1996 to 2022, and consist of 11 interventional and 13 observational in design. A total of 2098 patients of any NMIBC stages and grades who received any forms of intravesical therapy were involved and distributed in the 4 cross-sectional (N = 620), 9 prospective cohort (N = 762), 2 single-arm clinical trial (N = 70), and 9 randomized controlled trial (RCT) studies (N = 646). Particularly, literature by Hayne et al. [36] is a protocol article that is embedded with the pilot RCT results. Regarding the intravesical agents assessed, almost 60% of the studies involved BCG (14 out of 24) with 6 of them having a design to compare the effects with a chemotherapeutic agent. While 4 studies did not specify the intravesical agent used, which were all cross-sectional surveys, 10 studies involved chemotherapeutic agents (including cisplatin, gemcitabine, mitomycin C, and pirarubicin) with 3 of them assisted by hyperthermia and 1 in combination with hyaluronic acid. Additionally, a single study evaluated the effects of an immunotherapeutic agent, interleukin-2, on QoL.

Table 1.
A summary of the characteristics and main findings of the eligible studies included in this systematic review.
3.1.2. Risk of Bias
Overall quality of the interventions included in this systematic review was poor because the majority of these studies carried high or unclear risk of bias in at least half of the 7 evaluated components (Figure 2a). The risk for performance bias (91%) and detection bias (100%) were exceptionally high due to lacking evidence of blinding procedures (Figure 2a,b). Blinding of patients but not the outcome data was performed in the study of Bosschieter et al. [51] while Tan et al., 2019 [52] fulfilled all remaining components except blinding. The performance regarding selection bias was moderately poor, because 7 and 9 trials were rated high or unclear risk for random sequence generation and allocation concealment, respectively, including the 2 single-arm interventions [42,58] in which such procedures are completely lacked by default (Figure 2a). Risk of attrition bias by analyzing incomplete outcome data was rated as low in 82% (Figure 2a,b). In contrast, approximately one-third (36%) of the included studies carried unclear risk of reporting bias due to selective reporting of outcome results for further analysis (Figure 2a,b). However, other unclear forms of bias were identified in most of the included interventions (Figure 2a,b).
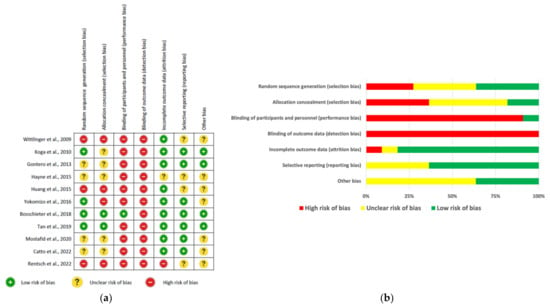
Figure 2.
Summary of risk of bias results evaluated by using the CONSORT 2010 checklist for interventional studies: (a) The risk of bias levels of key RCT components rated in every included study; (b) the percentage of each risk of bias level of the key components [36,42,43,44,48,51,52,53,55,58].
For observational studies, quality assessment results were summarized in Figure 3a and grouped into 6 areas for reporting publications in Figure 3b. Almost all included studies have adequately explained the scientific background, rationale for investigation, and specific objectives or hypothesis; however, approximately one-third (39%) of them failed in indicating the study design in the title or abstract (Figure 3a,b). Regarding the methods, none of the studies has described any efforts to address potential source of bias; in addition, 85% and 77% of the included studies inadequately explained ‘how the sample size was arrived at’ and ‘statistical approach for addressing missing data’, respectively (Figure 3a,b). When reporting the results, 77% of studies fulfilled the requirement of indicating the numbers of individuals at each stage but reasons for non-participation were not given in half of them. Participant characteristics, exposure information, or missing data per each variable of interest were not reported in 85% of studies, whereas only 54% adequately reported the main finding with unadjusted estimates and their precision and 69% did not perform other analyses such as subgroup analyses and sensitivity (Figure 3a,b). Key results and cautious overall interpretation were adequately discussed in general, but only 7 (54%) and 1 (7.7%) of the included studies addressed the study limitations and generalization of the results, respectively (Figure 3a,b). However, up to 70% of the studies did not report the source of funding and the role of the funders (Figure 3b). Overall, the cohort study conducted by Schmidt et al. [47] was rated as a high-quality report which fulfilled almost all 22 STROBE reporting items. In the remaining studies included in this review, 7–18 items were inadequately reported (Figure 3a).
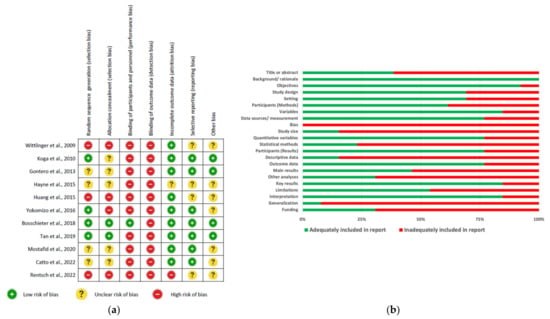
Figure 3.
Summary of risk of bias results evaluated by using the STROBE Statement checklist for interventional studies: (a) The risk of bias levels of items rated in every included study; (b) the percentage of each risk of bias level of the items [36,42,43,44,48,51,52,53,54,58].
3.2. QoL Measures and Instruments
3.2.1. General QoL
Earlier research asked general QoL questions using self-constructed scales to measure satisfaction to life and health status [37], overall QoL [38], and satisfaction of general QoL and affecting daily life [35]. William-Cox [35] also measured particularly QoL related to physical condition using a 7-point scale in addition to qualitative interviews. Other researchers also measured multiple additional aspects related general QoL, which included sexual activity, symptoms, daily activity levels [38], working activity relations, sexual couple life, and self-esteem [39]. Huang et al. [46] used the Visual Analogue Scale (VAS) to measure pain intensity while Miyake et al. [57] measured sleep quality using the MotionWatch8 mobile application.
The EORTC QLQ-C30 questionnaire was identified as the most frequently adopted validated instrument for measuring the global health status [43,44,45,48,50,53,54,55,57,58]. Three other studies measured health states of participants using the EQ-5D questionnaire [52,54,55], while general health was measured in two studies using the SF-36 heath survey [47,51] and SF-8 which is the abbreviated version of an original 36-item [57]. Within the context of generic QoL, these instruments also cover functioning and symptoms of physical, mental, and social health in certain extents:
- EORTC QLQ-C30: Contains 30 items to measure Global health status, functioning QoL (5 subscales), symptom QoL (8 subscales), and financial difficulties [59].
- EQ-5D: Severity levels of 5 dimensions including mobility, self-care, usual activities, pain & discomfort, and anxiety and depression [60].
- SF-36: Contains 36 items to measure 8 domains including physical functioning, role limitations due to physical problems, role limitations due to emotional problems, general health, bodily pain, vitality, social functioning, and mental health [61].
- SF-8: Contains 8 items to measure the same 8 domains of SF-36 [62].
3.2.2. Disease- and Treatment-Specific QoL
Numerous researchers measured the QoL more comprehensively using combination of a general QoL instrument with one or more other disease- or treatment-specific tools. The EORTC-BLS24 is a NMIBC-specific module of the QLQ-C30 for assessing health-related QoL that they were commonly coupled together and used in some studies [36,44,50,51,58]. Danielsson et al. [49] developed their own 17-item questionnaire to measure the urinary bladder symptoms and burdens in NMIBC patients treated with BCG instillation. Moreover, two other bladder cancer-specific instruments were identified from the studies included in this review, they are BCI [40,47] and FACT-BI [56,57]. The domains of the three bladder cancer-specific instruments are listed:
- EORTC QLQ-BLS24: Modular questionnaire specific for NMIBC which contains 24 items grouped into 6 scales to measure the QoL affected by urinary symptoms, malaise, intravesical treatment issues, future worries, bloating and flatulence, and sexual function. Later in 2014, it was updated to QLQ-NMIBC24 which has maintenance but added 5 sexual function subscales [63].
- BCI: Contains 36 items assessing QoL in urinary, bowel and sexual health domains function among patients with bladder cancer [64].
- FACT-BI: Contains 39 items to measure 5 domains including physical, social, emotional, functional well-being, and a bladder cancer subscale [65].
The BCI was used alone in one study [40] while it was used to supplement the general QoL measured by using the SF-36 questionnaire in the study Schmidt et al. [47]. Other researchers measured how QoL is affected by urinary symptoms and sexual functions by adopting instruments commonly used in urology other than bladder cancer, they are:
- IPSS: Contains 8 items to measure severity of urinary symptoms with the last item (IPSS-8) asking the QoL living with the urinary symptoms [66].
- IIEF-5: Contains 5 items to measure erectile function with the last item addressing intercourse satisfaction [67].
- ICSI: Contains 4 items measuring voiding and pain without asking any QoL aspects [68].
- CLSS: Contains 10 items addressing the frequency of lower urinary tract symptoms, and additional 2 single items asking the single symptom which had the greatest impact and the feeling of living with the urinary condition for the rest of life [69].
Although it was first established for addressing lower urinary tract symptom secondary to benign prostatic hyperplasia, the IPSS is frequently adopted by urologist to measure urinary symptoms and burdens of patients with different urological diseases [66]. Two studies used IPSS together with FACT-BI [56,57]. Particularly, Miyake et al. [57] also measured the general QoL using QLQ-C30 and SF-8 as well as sleep quality using the MotionWatch8 mobile application, in addition to IPSS and FACT-BI but a bladder cancer-specific QoL measurement was missing. On the other hand, the RCT conducted by Hayne et al. [36] has comprehensively evaluated the effect of a new chemotherapeutic modality by using a set of instruments including QLQ-C30, QLQ-BLS24, IPSS, and ICSI. One study used IPSS in addition to IIEF-5 which is a simplified version of the International Index of Erectile Function [70] to address in particular the effect of intravesical BCG therapy on QoL associated with urinary symptoms and erectile function [41]. Wittlinger et al. [42] only reported the results of IPSS-8 as a summary of how the patients living with urinary symptoms upon an intravesical treatment. The CLSS was identified in a single study and used in addition to QLQ-C30 to evaluate the effect of an intravesical chemotherapy on general QoL and QoL living with lower urinary tract condition in intermediate- or high-risk NMIBC patients.
3.3. Impact of Intravesical Therapies on QoL
3.3.1. Is Intravesical Therapy Better Than Other Treatments?
Four cross-sectional studies did not specify the intravesical agents that were exposed to the surveyed patients. When compared with patients without receiving TURBT alone or other non-specified treatments, consistent findings suggested that intravesical therapy caused some degrees of burdens on sexual functions especially in men [39,40,54]. Apart from sexual/couple life, Abbona et al. [39] indicated the alteration of working activity/relations and self-esteem by intravesical therapy in a quite significant number of patients when reporting their baseline measurements before recruiting them into a psychosexual support therapy. Pain and discomfort were also more frequently reported in patients who received intravesical instillation following TURBT, but an overall better emotional quality as compared with TURBT alone [54]. When compared with surgical treatment, intravesical chemotherapy with MMC resulted in constant deteriorations in urinary symptoms and global health status throughout the 12-month follow-up period [53]. The benefit of intravesical therapy on mental health over TURBT was coherent with the findings of a cohort study [47]. In a recent RCT study [55], when compared with radical cystectomy (RC), intravesical BCG therapy was shown to have negative impacts on urinary symptoms and sexual functioning without demonstrating remarkable improvement in general QoL, especially during the initial 3–6 month treatment period. However, the negative impacts of intravesical therapy seemed to be associated with the induction period but improved after the maintenance [35], resulting in a possible better global QoL state over time along the treatment [35,54]. Such pattern of improvements observed in various symptom and functioning parameters following the induction were consistent with another cohort study [50].
3.3.2. BCG Immunotherapy
Intravesical BCG instillation exhibited long term benefits in reducing emotional burdens caused by urinary and sexual symptoms as soon as at 1 month [41] and up to 5 years after completing the treatment [49]. Patients who received BCG therapy maintained stable health status in general over time [41,49]. In the RCT conducted by Catto et al. [55], as measured by the QLQ- NIMIBC24, worsening of urinary symptoms and concerns about contaminating a partner were observed in the first 3–6 months upon commencing the treatment schedule, but restored to the baseline levels with small reductions in future worry scores in the next 6 months. This is consistent with the findings indicated deterioration of health-related QoL during the induction period [57,58] while improvements were observed during the maintenance schedules [38,43,58].
Induction was shown to worsen cognitive functioning and insomnia with stable emotional functioning [57], physical functioning and fatigue with improved emotional functioning, urinary symptoms, future worries, and sexual functioning [58]. Regarding insomnia, 60–70% of patients rated their sleep quality poor resulting from decreased sleep efficacy with increases of mobile time, immobile bouts ≤ 1 min, and fragmentation index [57], which was consistent with the higher insomnia scores reported by the cross-sectional study conducted by Catto et al. [54]. The negative impact on sleep quality was believed to be caused by transient increase of voiding frequency, intermittency, and nocturia [57]. In a RCT study [48], induction treatment using half-dose of BCG resulted in better symptom QoL with almost all symptom scores decreased but a poorer function QoL when compared with the standard dose, which partially explained the stable global health and QoL states observed in other studies. However, in another RCT study, a 1/3 dose of BCG displayed negative impacts on general functioning and symptom QoL scales, and positive impacts on NMIBC-specific QoL scales but negative impacts on sexual functioning measured, when the measurements after the induction and end of maintenance treatment cycles were compared with the baseline values before the first instillation [44].
During and after the maintenance period, progressive improvements were observed in sexual activity, micturition problems, and activity levels [38] and different functioning dimensions and most of the symptoms [43] resulting in better global health status and overall QoL. In the RCT study conducted by Koga et al. [43], positive QoL impact was not observed in the observational group without receiving the maintenance treatment. Contradictorily, a single-arm clinical trial of BCG maintenance exhibited continuous deterioration in various functioning dimensions but improvement in a few non-specific symptom scores (nausea/vomiting, appetite loss, constipation) in addition to deteriorated insomnia and diarrhea, despite urinary symptoms and sexual function being improved together with a slightly improved global health status [58].
3.3.3. Immunotherapy
Inclusive outcomes were reported in a small sampled RCT study was designed to compare the effects of intravesical IL-2 following incomplete TURBT with complete TURBT alone, although statistically insignificant positive and negative changes were observed in certain general- and NMIBC-specific QoL parameters in both arms [51].
3.3.4. Chemotherapy
Among the 10 included studies involving chemotherapeutic agents, only 2 RCT [46,53] and 1 cohort [45] studies investigated the effects of chemotherapy on QoL in 3 different treatment protocols involving 2 drugs. Intravesical treatment schedule with MMC resulted in constant deteriorations in urinary symptoms and global health status throughout the 12-month follow-up period. Similarly, worsening of social function and global health status that were associated with local urinary symptoms in addition to increased fatigue, pain, appetite loss, and diarrhea were observed in the patient cohort receiving intravesical instillation with pirarubicin [45]. However, Huang et al. [53] demonstrated the positive impact of adding HA to the pirarubicin regimen on relieving the pelvic pain and urinary symptoms up to the 2-year follow-up period. The remaining studies involving chemotherapy that compared with BCG [36,44,47,50] and assisted the drug delivery using hyperthermia [42,52,56] will be discussed in the following two sections.
3.3.5. Comparison between Intravesical BCG and Chemotherapy
Limited evidence suggested intravesical therapy with BCG or chemotherapeutic agents has its own pros and cons. A cohort study suggested that BCG was good in reducing pains over MMC while MMC performed better in problems with cystoscopy over BCG, despite both having a similar impact on QoL [50]. In a RCT study, GEM was shown to be superior to BCG for general QoL while BCG performed better in the bladder cancer-specific QoL than BCG, despite both exhibiting comparable negative impacts on sexual QoL [44]. When administered intravesically following TURBT, MMC demonstrated the improvement on sexual QoL which was contradictory to the negative impact of BCG, while BCG was shown to be beneficial to bowel symptoms over MMC, despite MMC resulting in a poorer BCI urinary summary score at 6 months but restored to score level equivalent to BCG [47]. Pilot results of a RCT study suggested the potential benefits of combining BCG with MMC on QoL related to local urinary symptoms [36].
3.3.6. Hyperthermia
Post-trial measurement of a quadrimodal treatment that incorporated hyperthermia with cisplatin indicated that the vast majority of patients were satisfied with the QoL associated with urinary symptoms while only 3% of them rated themselves unhappy [42]. Patients treated with radiofrequency-induced thermo-chemotherapy with MMC were shown to have a slight increasing trend of health status from 3 to 9 months after instillation and rated higher health status than those treated with BCG, although statistically insignificantly [52]. Chemohyperthermia with MMC exhibited comparable effects with MMC instillation but superior effects over BCG on overall functioning QoL at the 4th week of induction treatment [56].
4. Discussion
The primary objective of this study was to review the existing scientific evidence on the impact of intravesical therapy towards QoL in NMIBC patients. To answer the PICOT question, the selected literatures comprised 6 studies allowing the comparison between intravesical therapy and TURBT, 14 studies having the focus on immunotherapy with 13 of them investigated BCG, and 10 studies focusing on chemotherapy with 4 of them were comparing with BCG with another 3 studies have adopted hyperthermia.
Adjuvant intravesical therapy following TURBT was not just a standard of care effective for preventing the recurrence of NMIBC [2], evidence collated in this current review supports its long-term positive impact on general and mental general QoL over TURBT alone. This is inconsistent with the findings of recent systematic reviews on bladder cancer surveillance that have suggested the negative impact on QoL due to the length and frequency of repeat intravesical therapy and cystoscopy [8,12]. There are two possible reasons for such inconsistency in the current review: first, because the actual effects were determined by comparing different time points to observe the long-term improvement of QoL; and second, the effects of follow-up and diagnosis in patients were ignored when determining the outcomes. Without a doubt, it is well known that the QOL of patients could be largely impacted by the protracted course of surveillance follow-up and care, whereas new diagnostic technologies such as the magnetic resonance imaging (MRI) without the need for contrast injection may be beneficial to improve the QoL [71]. In-depth analysis of the reviewed studies revealed similar positive QoL effects between BCG and certain chemotherapeutic drugs (for instance MMC, pirarubicin, and gemcitabine) over time, even though some symptom and functioning burdens were evidenced. The intravesical treatment protocol for high-risk NMIBC patients could last for more than 3 years [6]. During the induction period, BCG worsened the local urinary symptoms and sexual dysfunctions that resulted from TURBT, but continuous improvements were observed after beginning the maintenance period and remained stable afterwards. This is aligned with the early literature review published in 2003 [23]. In contrast, intravesical chemotherapy was more prone to being associated with non-specific symptoms such as pain and fatigue throughout the treatment period, although deteriorations in urinary symptoms and global health status could also occur. Interestingly, hyaluronic acid helped to ease the pain and urinary symptoms associated with pirarubicin for up to 2 years follow-up period, but no other QoL parameters were measured [46]. QoL data regarding chemotherapy remain limited [16]. On the other hand, hyperthermia has shown a positive trend in enhancing the QoL of patients receiving intravesical chemotherapy, which requires more investigations.
Owing to the reason of most interventions conducted on intravesical therapy being focused on evaluating effectiveness and toxicities without measuring QoL [13,14,15,16,19,22,61], the current systematic review collected more comprehensively a mixture of interventional and observational studies. In fact, the number of eligible studies included was still limited to cover existing intravesical modalities that are known to be effective. Regarding immunotherapy, aside from BCG, only a single study investigating the effects of interleukin-2 on QoL was identified which was insufficient to draw any conclusions [51], whilst many other agents such as interferon-alpha [19,20] and immune checkpoint inhibitors [72] were not addressed. Except for three identified studies on hyperthermia, other device-assisted modalities intravesical drug delivery such as EMDA [22,30] were completely lacking. Nothing has been updated from the systematic reviews on interferon-alpha [19] and EMDA [22] published 5 years ago, both reported no data related to disease-specific QoL was found. Moreover, the emerging photodynamic therapy has been shown to be highly effective and safe [32,33], whilst none of the studies have addressed the QoL in patients. No doubt, QoL outcomes of intravesical therapy were understudied in terms of both volume and coverage of different modalities. However, two-thirds of the eligible studies were published in the past 10 years which has projected an increasing trend of using QoL measures in recent interventions. With the identification of registered trials that have incorporated QoL outcome measures in their protocol while results were yet to be available, a more comprehensive outlook for QoL impacted by novel and effective intravesical therapies will be available in the 5–10 years. This aligns with the call for uncovering patient-report outcomes in bladder cancer [73].
Regarding the outcome measures, a total of 11 well-validated questionnaires or scales in addition to other self-developed instruments were among the 24 eligible studies for measuring different aspects of general and disease specific QoL. Since the literature review published by Bottemen et al. [23], the combination use of multiple QoL instruments for evaluating intravesical therapy has become a common practice that also resulted in generating heterogeneous outcome to hinder the effect size estimation to proceed for meta-analysis. The same phenomenon was concluded from another systematic review on NMIBC effectiveness trials that led to the recommendation of using the core set of QoL outcomes to reduce heterogeneity [24]. In addition to heterogeneity, another limitation of current review is the publication quality of the included studies. Quality assessment has determined that the majority of studies under review were poorly conducted or reported, which concurred with many other systematic reviews on effectiveness of intravesical therapies [16,17,19,22].
5. Conclusions
Existing evidence was insufficient to provide a conclusive answer to the PICOT question of this systematic review because data were not found to uncover the impact of many emerging intravesical therapies that have been suggested to be effective and safe. Limited studies revealed the long-term positive impact of intravesical immunotherapy with BCG or chemotherapy with certain drugs, irrespective of the worsening symptom burdens and functional performance observed during the induction treatment. However, treatment-specific QoL studies are required for newly emerging intravesical modalities that have displayed effectiveness.
Author Contributions
Conceptualization, J.W.Y. and C.-F.N.; methodology, J.W.Y.; systematic search of literature: J.W.Y.; formal analysis: J.W.Y., R.W.W. and S.S.C.; writing—original draft preparation, J.W.Y.; writing—review and editing, S.S.C. and C.-F.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this systematic review article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Anderson, B. Bladder cancer: Overview and disease management. Part 1: Non-muscle-invasive bladder cancer. Br. J. Nurs. 2018, 27, S27–S37. [Google Scholar] [CrossRef]
- Van der Heijden, A.G.; Witjes, J.A. Recurrence, Progression, and Follow-Up in Non–Muscle-Invasive Bladder Cancer. Eur. Urol. Suppl. 2009, 8, 556–562. [Google Scholar] [CrossRef]
- Langbein, S.; Lehmann, J.; Harder, A.; Steidler, A.; Michel, M.S.; Alken, P.; Badawi, J.K. Protein profiling of bladder cancer using the 2D-PAGE and SELDI-TOF-MS technique. Technol. Cancer Res. Treat. 2006, 5, 67–72. [Google Scholar] [CrossRef]
- Boustani, J.; Bertaut, A.; Galsky, M.D.; Rosenberg, J.E.; Bellmunt, J.; Powles, T.; Recine, F.; Harshman, L.C.; Chowdhury, S.; Niegisch, G.; et al. Retrospective International Study of Cancers of the Urothelial Tract (RISC) Investigators. Radical cystectomy or bladder preservation with radiochemotherapy in elderly patients with muscle-invasive bladder cancer: Retrospective International Study of Cancers of the Urothelial Tract (RISC) Investigators. Acta Oncol. 2018, 57, 491–497. [Google Scholar] [CrossRef]
- McConkey, R.W.; Dowling, M. Supportive Care Needs of Patients on Surveillance and Treatment for Non-Muscle-Invasive Bladder Cancer. Semin. Oncol. Nurs. 2021, 37, 151105. [Google Scholar] [CrossRef] [PubMed]
- Reis, L.O.; Moro, J.C.; Ribeiro, L.F.; Voris, B.R.; Sadi, M.V. Are we following the guidelines on non-muscle invasive bladder cancer? Int. Braz. J. Urol. 2016, 42, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Nayak, A.; Cresswell, J.; Mariappan, P. Quality of life in patients undergoing surveillance for non-muscle invasive bladder cancer-a systematic review. Transl. Androl. Urol. 2021, 10, 2737–2749. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.; Nielsen, M.E.; Crandell, J.L.; Palmer, M.H.; Smith, S.K.; Bryant, A.L.; Mayer, D.K. Health-related quality of life among non-muscle-invasive bladder cancer survivors: A population-based study. BJU Int. 2020, 125, 38–48. [Google Scholar] [CrossRef]
- Singer, S.; Ziegler, C.; Schwalenberg, T.; Hinz, A.; Götze, H.; Schulte, T. Quality of life in patients with muscle invasive and non-muscle invasive bladder cancer. Support Care Cancer 2013, 21, 1383–1393. [Google Scholar] [CrossRef]
- Mohamed, N.E.; Gilbert, F.; Lee, C.T.; Sfakianos, J.; Knauer, C.; Mehrazin, R.; Badr, H.; Wittmann, D.; Downs, T.; Berry, D.; et al. Pursuing Quality in the Application of Bladder Cancer Quality of Life Research. Bladder Cancer 2016, 2, 139–149. [Google Scholar] [CrossRef]
- Taarnhøj, G.A.; Johansen, C.; Pappot, H. Quality of life in bladder cancer patients receiving medical oncological treatment; a systematic review of the literature. Health Qual. Life Outcomes 2019, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Selph, S.; Buckley, D.I.; Fu, R.; Griffin, J.C.; Grusing, S.; Gore, J.L. Intravesical Therapy for the Treatment of Nonmuscle Invasive Bladder Cancer: A Systematic Review and Meta-Analysis. J. Urol. 2017, 197, 1189–1199. [Google Scholar] [CrossRef]
- Wang, S.; Jin, S.; Shu, Q.; Wu, S. Strategies to Get Drugs across Bladder Penetrating Barriers for Improving Bladder Cancer. Ther. Pharm. 2021, 13, 166. [Google Scholar] [CrossRef]
- Tyagi, P.; Kashyap, M.; Hensley, H.; Yoshimura, N. Advances in intravesical therapy for urinary tract disorders. Expert Opin. Drug Deliv. 2016, 13, 71–84. [Google Scholar] [CrossRef]
- Schmidt, S.; Kunath, F.; Coles, B.; Draeger, D.L.; Krabbe, L.M.; Dersch, R.; Kilian, S.; Jensen, K.; Dahm, P.; Meerpohl, J.J. Intravesical Bacillus Calmette-Guérin versus mitomycin C for Ta and T1 bladder cancer. Cochrane Database Syst. Rev. 2020, 1, CD011935. [Google Scholar] [CrossRef]
- Han, M.A.; Maisch, P.; Jung, J.H.; Hwang, J.E.; Narayan, V.; Cleves, A.; Hwang, E.C.; Dahm, P. Intravesical gemcitabine for non-muscle invasive bladder cancer. Cochrane Database Syst. Rev. 2021, 6, CD009294. [Google Scholar] [CrossRef]
- Galsky, M.D.; Balar, A.V.; Black, P.C.; Campbell, M.T.; Dykstra, G.S.; Grivas, P.; Gupta, S.; Hoimes, C.J.; Lopez, L.P.; Meeks, J.J.; et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of urothelial cancer. J. Immunother. Cancer 2021, 9, e002552. [Google Scholar] [CrossRef]
- Shepherd, A.R.; Shepherd, E.; Brook, N.R. Intravesical Bacillus Calmette-Guérin with interferon-alpha versus intravesical Bacillus Calmette-Guérin for treating non-muscle-invasive bladder cancer. Cochrane Database Syst. Rev. 2017, 3, CD012112. [Google Scholar] [CrossRef]
- Lamm, D.; Brausi, M.; O’Donnell, M.A.; Witjes, J.A. Interferon alfa in the treatment paradigm for non-muscle-invasive bladder cancer. Urol. Oncol. 2014, 32, e21–e30. [Google Scholar] [CrossRef] [PubMed]
- Braasch, M.R.; Böhle, A.; O’Donnell, M.A. Risk-adapted use of intravesical immunotherapy. BJU Int. 2008, 102, 1254–1264. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Gudeloglu, A.; Kiziloz, H.; Kuntz, G.M.; Miller, A.; Konety, B.R.; Dahm, P. Intravesical electromotive drug administration for non-muscle invasive bladder cancer. Cochrane Database Syst. Rev. 2017, 9, CD011864. [Google Scholar] [CrossRef] [PubMed]
- Botteman, M.F.; Pashos, C.L.; Hauser, R.S.; Laskin, B.L.; Redaelli, A. Quality of life aspects of bladder cancer: A review of the literature. Qual. Life Res. 2003, 12, 675–688. [Google Scholar] [CrossRef] [PubMed]
- Veskimae, E. A Systematic Review of Outcome Reporting, Definition and Measurement Heterogeneity in Non-Muscle Invasive Bladder Cancer Effectiveness Trials of Adjuvant, Prophylactic Treatment After Transurethral Resection. Bladder Cancer 2021, 7, 221–241. [Google Scholar] [CrossRef]
- Guallar-Garrido, S.; Julián, E. Bacillus Calmette-Guérin (BCG) Therapy for Bladder Cancer: An Update. Immunotargets Ther. 2020, 9, 1–11. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Gunjur, A.; Weickhardt, A.; Papa, N.; Bolton, D.; Lawrentschuk, N.; Perera, M. Adjuvant therapies for non-muscle-invasive bladder cancer: Advances during BCG shortage. World J. Urol. 2022, 40, 1111–1124. [Google Scholar] [CrossRef]
- van der Heijden, A.G.; Dewhirst, M.W. Effects of hyperthermia in neutralising mechanisms of drug resistance in non-muscle-invasive bladder cancer. Int. J. Hyperth. 2016, 32, 434–445. [Google Scholar] [CrossRef]
- Multhoff, G.; Habl, G.; Combs, S.E. Rationale of hyperthermia for radio(chemo)therapy and immune responses in patients with bladder cancer: Biological concepts, clinical data, interdisciplinary treatment decisions and biological tumour imaging. Int. J. Hyperth. 2016, 32, 455–463. [Google Scholar] [CrossRef]
- Van Valenberg, F.J.P.; Kajtazovic, A.; Canepa, G.; Lüdecke, G.; Kilb, J.I.; Aben, K.K.H.; Nativ, O.; Madaan, S.; Ayres, B.; Issa, R.; et al. Intravesical Radiofrequency-Induced Chemohyperthermia for Carcinoma In Situ of the Urinary Bladder: A Retrospective Multicentre Study. Bladder Cancer 2018, 4, 365–376. [Google Scholar] [CrossRef]
- Slater, S.E.; Patel, P.; Viney, R.; Foster, M.; Porfiri, E.; James, N.D.; Montgomery, B.; Bryan, R.T. The effects and effectiveness of electromotive drug administration and chemohyperthermia for treating non-muscle invasive bladder cancer. Ann. R. Coll. Surg. Engl. 2014, 96, 415–419. [Google Scholar] [CrossRef][Green Version]
- Audisio, A.; Buttigliero, C.; Delcuratolo, M.D.; Parlagreco, E.; Audisio, M.; Ungaro, A.; Di Stefano, R.F.; Di Prima, L.; Turco, F.; Tucci, M. New Perspectives in the Medical Treatment of Non-Muscle-Invasive Bladder Cancer: Immune Checkpoint Inhibitors and Beyond. Cells 2022, 11, 357. [Google Scholar] [CrossRef] [PubMed]
- Devere White, R.W. Transurethral resection of superficial bladder cancer using 5-aminolevulinic acid: Are there any long-term benefits? Nat. Clin. Pract. Urol. 2006, 3, 254–255. [Google Scholar] [CrossRef]
- Inoue, K. 5-Aminolevulinic acid-mediated photodynamic therapy for bladder cancer. Int. J. Urol. 2017, 24, 97–101. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Williams-Cox, D. A mixed-method study into quality of life for bladder cancer patients. Prof. Nurse 2004, 19, 343–347. [Google Scholar]
- Hayne, D.; Stockler, M.; McCombie, S.P.; Chalasani, V.; Long, A.; Martin, A.; Sengupta, S.; Davis, I.D. BCG+MMC trial: Adding mitomycin C to BCG as adjuvant intravesical therapy for high-risk, non-muscle-invasive bladder cancer: A randomised phase III trial (ANZUP 1301). BMC Cancer 2015, 15, 432. [Google Scholar] [CrossRef]
- Bohle, A.; Balck, F.; von Weitersheim, J.; Jocham, D. The quality of life during intravesical bacillus Calmette-Guerin therapy. J. Urol. 1996, 155, 1221–1226. [Google Scholar] [CrossRef]
- Mack, D.; Frick, J. Quality of life in patients undergoing bacille Calmette-Guérin therapy for superficial bladder cancer. Br. J. Urol. 1996, 78, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Abbona, A.; Morabito, F.; Rossi, R.; Billia, M.; Liberale, F.; Ferrando, U. Quality of life in patients undergone oncopreventive intravesical treatment for superficial bladder cancer. Arch. Ital. Urol. Androl. 2007, 79, 143–146. [Google Scholar] [PubMed]
- Gilbert, S.M.; Wood, D.P.; Dunn, R.L.; Weizer, A.Z.; Lee, C.T.; Montie, J.E.; Wei, J.T. Measuring health-related quality of life outcomes in bladder cancer patients using the Bladder Cancer Index (BCI). Cancer 2007, 109, 1756–1762. [Google Scholar] [CrossRef]
- Sighinolfi, M.C.; Micali, S.; De Stefani, S.; Mofferdin, A.; Ferrari, N.; Giacometti, M.; Bianchi, G. Bacille Calmette-Guérin intravesical instillation and erectile function: Is there a concern? Andrologia 2007, 39, 51–54. [Google Scholar] [CrossRef]
- Wittlinger, M.; Rödel, C.M.; Weiss, C.; Krause, S.F.; Kühn, R.; Fietkau, R.; Sauer, R.; Ott, O.J. Quadrimodal treatment of high-risk T1 and T2 bladder cancer: Transurethral tumor resection followed by concurrent radiochemotherapy and regional deep hyperthermia. Radiother. Oncol. 2009, 93, 358–363. [Google Scholar] [CrossRef]
- Koga, H.; Ozono, S.; Tsushima, T.; Tomita, K.; Horiguchi, Y.; Usami, M.; Hirao, Y.; Akaza, H.; Naito, S.; BCG Tokyo Strain Study Group. Maintenance intravesical bacillus Calmette-Guérin instillation for Ta, T1 cancer and carcinoma in situ of the bladder: Randomized controlled trial by the BCG Tokyo Strain Study Group. Int. J. Urol. 2010, 17, 759–766. [Google Scholar] [CrossRef]
- Gontero, P.; Oderda, M.; Mehnert, A.; Gurioli, A.; Marson, F.; Lucca, I.; Rink, M.; Schmid, M.; Kluth, L.A.; Pappagallo, G.; et al. The impact of intravesical gemcitabine and 1/3 dose Bacillus Calmette-Guérin instillation therapy on the quality of life in patients with nonmuscle invasive bladder cancer: Results of a prospective, randomized, phase II trial. J. Urol. 2013, 190, 857–862. [Google Scholar] [CrossRef]
- Wei, L.; Li, Q.; Liang, H.; Jianbo, L. The quality of life in patients during intravesical treatment and correlation with local symptoms. J. Chemother. 2014, 26, 165–168. [Google Scholar] [CrossRef]
- Huang, W.; Wang, F.; Wu, C.; Hu, W. Efficacy and safety of pirarubicin combined with hyaluronic acid for non-muscle invasive bladder cancer after transurethral resection: A prospective, randomized study. Int. Urol. Nephrol. 2015, 47, 631–636. [Google Scholar] [CrossRef]
- Schmidt, S.; Francés, A.; Lorente Garin, J.A.; Juanpere, N.; Lloreta Trull, J.; Bonfill, X.; Martinez-Zapata, M.J.; Morales Suarez-Varela, M.; de la Cruz, J.; Emparanza, J.I.; et al. Quality of life in patients with non-muscle-invasive bladder cancer: One-year results of a multicentre prospective cohort study. Urol. Oncol. 2015, 33, e7–e19. [Google Scholar] [CrossRef]
- Yokomizo, A.; Kanimoto, Y.; Okamura, T.; Ozono, S.; Koga, H.; Iwamura, M.; Tanaka, H.; Takahashi, S.; Tsushima, T.; Kanayama, H.O.; et al. Randomized Controlled Study of the Efficacy, Safety and Quality of Life with Low Dose bacillus Calmette-Guérin Instillation Therapy for Nonmuscle Invasive Bladder Cancer. J. Urol. 2016, 195, 41–46. [Google Scholar] [CrossRef]
- Danielsson, G.; Malmström, P.U.; Jahnson, S.; Wijkström, H.; Nyberg, T.; Thulin, H. Bladder health in patients treated with BCG instillations for T1G2-G3 bladder cancer—A follow-up five years after the start of treatment. Scand. J. Urol. 2018, 52, 377–384. [Google Scholar] [CrossRef]
- Siracusano, S.; Silvestri, T.; Bassi, S.; Porcaro, A.B.; Cerruto, M.A.; Talamini, R.; Artibani, W. Health-related quality of life after BCG or MMC induction for non-muscle invasive bladder cancer. Can. J. Urol. 2018, 25, 9480–9485. [Google Scholar]
- Bosschieter, J.; Nieuwenhuijzen, J.A.; Hentschel, A.; Vis, A.N.; Lissenberg-Witte, B.I.; den Otter, W.; van Moorselaar, R.J.A. Value of a Marker Lesion in Non-Muscle-Invasive Bladder Cancer Patients Treated with Interleukin-2 Instillations: A Randomized Controlled Multicentre Trial. Urol. Int. 2019, 102, 69–76. [Google Scholar] [CrossRef]
- Tan, W.S.; Panchal, A.; Buckley, L.; Devall, A.J.; Loubière, L.S.; Pope, A.M.; Feneley, M.R.; Cresswell, J.; Issa, R.; Mostafid, H.; et al. Radiofrequency-induced Thermo-chemotherapy Effect Versus a Second Course of Bacillus Calmette-Guérin or Institutional Standard in Patients with Recurrence of Non-muscle-invasive Bladder Cancer Following Induction or Maintenance Bacillus Calmette-Guérin Therapy (HYMN): A Phase III, Open-label, Randomised Controlled Trial. Eur. Urol. 2019, 75, 63–71. [Google Scholar] [CrossRef]
- Mostafid, A.H.; Porta, N.; Cresswell, J.; Griffiths, T.R.L.; Kelly, J.D.; Penegar, S.R.; Davenport, K.; McGrath, J.S.; Campain, N.; Cooke, P.; et al. CALIBER: A phase II randomized feasibility trial of chemoablation with mitomycin-C vs surgical management in low-risk non-muscle-invasive bladder cancer. BJU Int. 2020, 125, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Catto, J.W.F.; Downing, A.; Mason, S.; Wright, P.; Absolom, K.; Bottomley, S.; Hounsome, L.; Hussain, S.; Varughese, M.; Raw, C.; et al. Quality of Life After Bladder Cancer: A Cross-sectional Survey of Patient-reported Outcomes. Eur. Urol. 2021, 79, 621–632. [Google Scholar] [CrossRef] [PubMed]
- Catto, J.W.F.; Gordon, K.; Collinson, M.; Poad, H.; Twiddy, M.; Johnson, M.; Jain, S.; Chahal, R.; Simms, M.; Dooldeniya, M.; et al. Radical Cystectomy Against Intravesical BCG for High-Risk High-Grade Nonmuscle Invasive Bladder Cancer: Results from the Randomized Controlled BRAVO-Feasibility Study. J. Clin. Oncol. 2021, 39, 202–214. [Google Scholar] [CrossRef] [PubMed]
- González-Padilla, D.A.; González-Díaz, A.; Guerrero-Ramos, F.; Rodríguez-Serrano, A.; García-Jarabo, E.; Corona-laPuerta, M.; Rodríguez-Antolín, A.; Villacampa-Aubá, F. Quality of life and adverse events in patients with nonmuscle invasive bladder cancer receiving adjuvant treatment with BCG, MMC, or chemohyperthermia. Urol. Oncol. 2021, 39, e9–e76. [Google Scholar] [CrossRef]
- Miyake, M.; Nishimura, N.; Oda, Y.; Owari, T.; Hori, S.; Morizawa, Y.; Gotoh, D.; Nakai, Y.; Anai, S.; Torimoto, K.; et al. Intravesical Bacillus Calmette-Guerin treatment-induced sleep quality deterioration in patients with non-muscle invasive bladder cancer: Functional outcome assessment based on a questionnaire survey and actigraphy. Support Care Cancer 2022, 30, 887–895. [Google Scholar] [CrossRef]
- Rentsch, C.A.; Thalmann, G.N.; Lucca, I.; Kwiatkowski, M.; Wirth, G.J.; Strebel, R.T.; Engeler, D.; Pedrazzini, A.; Hüttenbrink, C.; Schultze-Seemann, W.; et al. A Phase 1/2 Single-arm Clinical Trial of Recombinant Bacillus Calmette-Guérin (BCG) VPM1002BC Immunotherapy in Non-muscle-invasive Bladder Cancer Recurrence after Conventional BCG Therapy: SAKK 06/14. Eur. Urol. Oncol. 2022, 5, 195–202. [Google Scholar] [CrossRef]
- Fayers, P.; Bottomley, A.; EORTC Quality of Life Group; Quality of Life Unit. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur. J. Cancer. 2002, 38, S125–S133. [Google Scholar] [CrossRef]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 2050312116671725. [Google Scholar] [CrossRef] [PubMed]
- Hashine, K.; Kusuhara, Y.; Miura, N.; Shirato, A.; Sumiyoshi, Y.; Kataoka, M. Health-related quality of life using SF-8 and EPIC questionnaires after treatment with radical retropubic prostatectomy and permanent prostate brachytherapy. Jpn. J. Clin. Oncol. 2009, 39, 502–508. [Google Scholar] [CrossRef]
- Blazeby, J.M.; Hall, E.; Aaronson, N.K.; Lloyd, L.; Waters, R.; Kelly, J.D.; Fayers, P. Validation and reliability testing of the EORTC QLQ-NMIBC24 questionnaire module to assess patient-reported outcomes in non-muscle-invasive bladder cancer. Eur. Urol. 2014, 66, 1148–1156. [Google Scholar] [CrossRef]
- Gilbert, S.M.; Dunn, R.L.; Hollenbeck, B.K.; Montie, J.E.; Lee, C.T.; Wood, D.P.; Wei, J.T. Development and validation of the Bladder Cancer Index: A comprehensive, disease specific measure of health related quality of life in patients with localized bladder cancer. J. Urol. 2010, 183, 1764–1769. [Google Scholar] [CrossRef]
- Brady, M.J.; Cella, D.F.; Mo, F.; Bonomi, A.E.; Tulsky, D.S.; Lloyd, S.R.; Deasy, S.; Cobleigh, M.; Shiomoto, G. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J. Clin. Oncol. 1997, 15, 974–986. [Google Scholar] [CrossRef]
- Kok, E.T.; McDonnell, J.; Stolk, E.A.; Stoevelaar, H.J.; Busschbach, J.J.; Triumph Research Group; Pan-European Expert Panel. The valuation of the International Prostate Symptom Score (IPSS) for use in economic evaluations. Eur. Urol. 2002, 42, 491–497. [Google Scholar] [CrossRef]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Peña, B.M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot. Res. 1999, 11, 319–326. [Google Scholar] [CrossRef]
- Humphrey, L.; Arbuckle, R.; Moldwin, R.; Nordling, J.; van de Merwe, J.P.; Meunier, J.; Crook, T.; Abraham, L. The bladder pain/interstitial cystitis symptom score: Development, validation, and identification of a cut score. Eur. Urol. 2012, 61, 271–279. [Google Scholar] [CrossRef]
- Homma, Y.; Yoshida, M.; Yamanishi, T.; Gotoh, M. Core Lower Urinary Tract Symptom score (CLSS) questionnaire: A reliable tool in the overall assessment of lower urinary tract symptoms. Int. J. Urol. 2008, 15, 816–820. [Google Scholar] [CrossRef]
- Rosen, R.C.; Cappelleri, J.C.; Gendrano, N. The International Index of Erectile Function (IIEF): A state-of-the-science review. Int. J. Impot. Res. 2002, 14, 226–244. [Google Scholar] [CrossRef]
- Afonso, J.; Santos, L.L.; Longatto-Filho, A.; Baltazar, F. Competitive glucose metabolism as a target to boost bladder cancer immunotherapy. Nat. Rev. Urol. 2020, 17, 77–106. [Google Scholar] [CrossRef] [PubMed]
- Delli Pizzi, A.; Mastrodicasa, D.; Marchioni, M.; Primiceri, G.; Di Fabio, F.; Cianci, R.; Seccia, B.; Sessa, B.; Mincuzzi, E.; Romanelli, M.; et al. Bladder cancer: Do we need contrast injection for MRI assessment of muscle invasion? A prospective multi-reader VI-RADS approach. Eur. Radiol. 2021, 31, 3874–3883. [Google Scholar] [CrossRef] [PubMed]
- Abu-Salha, Y.; Smith, A.B. Seeing the Unseen: Uncovering Patient-reported Outcomes in Bladder Cancer. Eur. Urol. 2021, 79, 633–634. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).