
Psychometric Properties of the Emotional Eater Questionnaire in University Students

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials & Methods
2.1. Participants
2.2. Instrument
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Description of the Sample
3.2. Descriptive Analysis of Each Item
3.3. Validity
3.3.1. Convergent Validity
3.3.2. Exploratory Factor Analysis
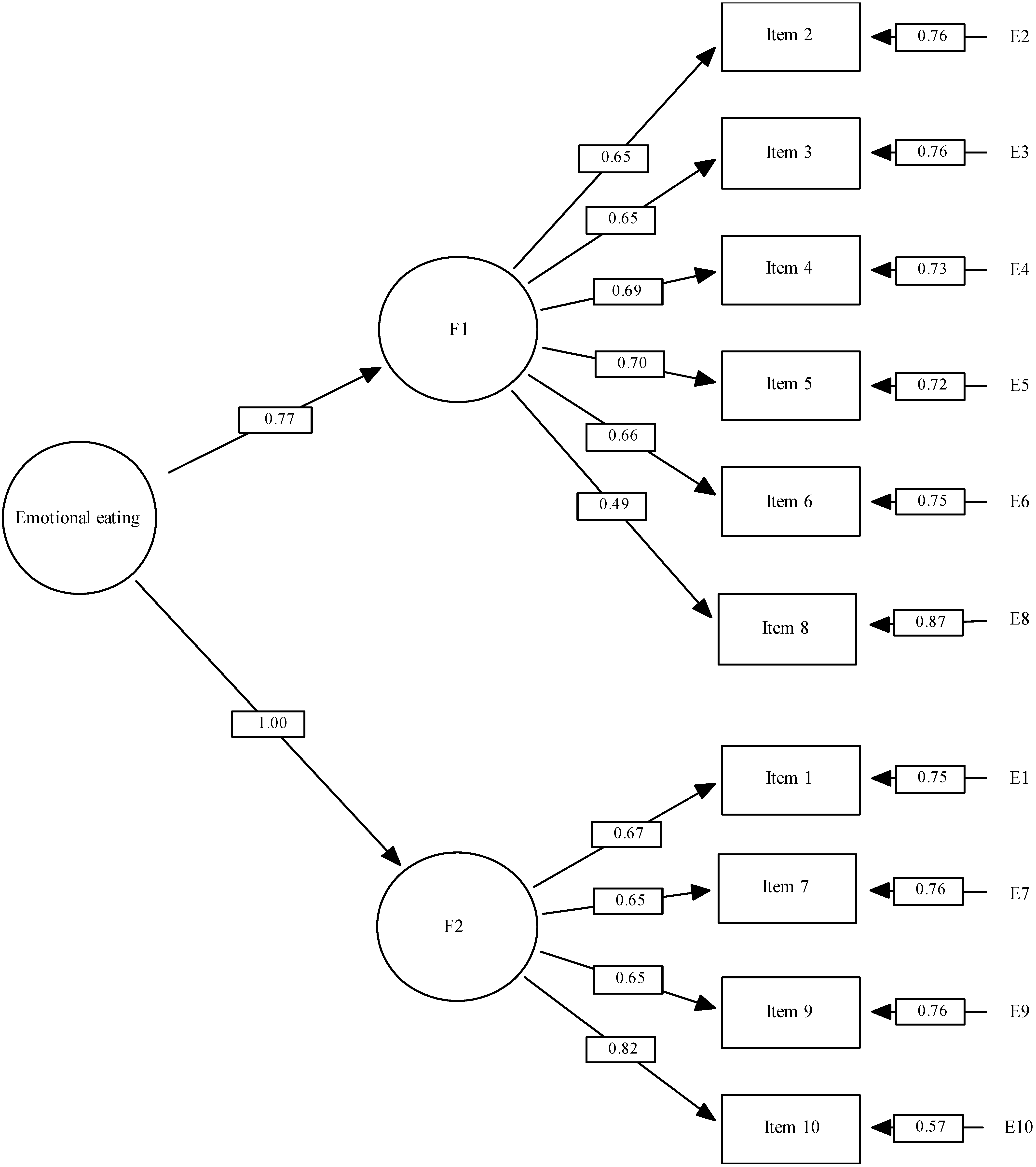
3.3.3. Confirmatory Factor Analysis
3.4. Reliability
3.4.1. Internal Consistency
3.4.2. Test-Retest
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Batty, G.D.; Hamer, M.; Gale, C.R. Life-course Psychological Distress and Total Mortality by Middle Age: The 1970 Birth Cohort Study. Epidemiology 2021, 32, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Cutillas, A.B.; Herrero, E.; de San Eustaquio, A.; Zamora, S.; Pérez-Llamas, F. Prevalencia de peso insuficiente, sobrepeso y obesidad, ingesta de energía y perfil calórico de la dieta de estudiantes universitarios de la Comunidad Autónoma de la Región de Murcia (España). Nutr. Hosp. 2013, 28, 683–689. [Google Scholar] [PubMed]
- González Sandoval, C.E.; Díaz Burke, Y.; Mendizabal-Ruiz, A.P.; Medina Díaz, E.; Alejandro Morales, J. Prevalence of obesity and altered lipid profile in university students. Nutr. Hosp. 2014, 29, 315–321. [Google Scholar]
- Mihalopoulos, N.L.; Auinger, P.; Klein, J.D. The Freshman 15: Is it Real? J. Am. Coll. Health 2010, 56, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Kemp, E.; Bui, M.; Grier, S. When food is more than nutrition: Understanding emotional eating and overconsumption. J. Consum. Behav. 2013, 12, 204–213. [Google Scholar] [CrossRef]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite 2021, 160, 105122. [Google Scholar] [PubMed]
- Zhang, J.; Zhang, Y.; Huo, S.; Ma, Y.; Ke, Y.; Wang, P.; Zhao, A. Emotional Eating in Pregnant Women during the COVID-19 Pandemic and Its Association with Dietary Intake and Gestational Weight Gain. Nutrients 2020, 12, 2250. [Google Scholar]
- Al-Musharaf, S. Prevalence and Predictors of Emotional Eating among Healthy Young Saudi Women during the COVID-19 Pandemic. Nutrients 2020, 12, 2923. [Google Scholar]
- Cardi, V.; Leppanen, J.; Treasure, J. The effects of negative and positive mood induction on eating behaviour: A meta-analysis of laboratory studies in the healthy population and eating and weight disorders. Neurosci. Biobehav. Rev. 2015, 57, 299–309. [Google Scholar]
- Bongers, P.; de Graaff, A.; Jansen, A. ‘Emotional’ does not even start to cover it: Generalization of overeating in emotional eaters. Appetite 2016, 96, 611–616. [Google Scholar]
- Sultson, H.; Kukk, K.; Akkermann, K. Positive and negative emotional eating have different associations with overeating and binge eating: Construction and validation of the Positive-Negative Emotional Eating Scale. Appetite 2017, 116, 423–430. [Google Scholar] [CrossRef]
- Evers, C.; Stok, F.; de Ridder, D.T.D. Feeding your feelings: Emotion regulation strategies and emotional eating. Pers. Soc. Psychol. Bull. 2010, 36, 792–804. [Google Scholar] [CrossRef]
- Bernabéu, E.; Marchena, C.; Iglesias, M.T. Factor Structure and Psychometric Properties of Emotional Eater Questionnaire (EEQ) in Spanish Colleges. Int. J. Environ. Res. Public. Health 2020, 17, 9090. Available online: https://www./pmc/articles/PMC7730267/ (accessed on 22 June 2021). [CrossRef]
- Alalwan, T.A.; Hilal, S.J.; Mahdi, A.M.; Ahmed, M.A.; Mandeel, Q.A. Emotional eating behavior among University of Bahrain students: A cross-sectional study. Arab. J. Basic. Appl. Sci. 2019, 26, 424–432. [Google Scholar]
- Sze, K.Y.P.; Lee, E.K.P.; Chan, R.H.W.; Kim, J.H. Prevalence of negative emotional eating and its associated psychosocial factors among urban Chinese undergraduates in Hong Kong: A cross-sectional study. BMC Public Health 2021, 21, 583. [Google Scholar] [CrossRef]
- WHO. Obesity and Overweight [Internet]. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 25 August 2022).
- Daubenmier, J.; Kristeller, J.; Hecht, F.M.; Maninger, N.; Kuwata, M.; Jhaveri, K.; Lustig, R.H.; Kemeny, M.; Karan, L.; Epel, E. Mindfulness intervention for stress eating to reduce cortisol and abdominal fat among overweight and obese women: An exploratory randomized controlled study. J. Obes. 2011, 2011, 651936. [Google Scholar] [CrossRef]
- Arnow, B.; Kenardy, J.; Agras, S. The emotional eating scale: The development of a measure to assess coping with negative affect by eating—Arnow—1995—International Journal of Eating Disorders—Wiley Online Library. Int. J. Eat. Disord. 1995, 18, 79–90. [Google Scholar] [CrossRef]
- Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior—van Strien—1986—International Journal of Eating Disorders—Wiley Online Library. Int. J. Eat. Disord. 1986, 5, 747–755. [Google Scholar]
- Framson, C.; Kristal, A.R.; Schenk, J.M.; Littman, A.J.; Zeliadt, S.; Benitez, D. Development and Validation of the Mindful Eating Questionnaire. J. Am. Diet. Assoc. 2009, 109, 1439–1444. [Google Scholar] [CrossRef]
- Masheb, R.M.; Grilo, C.M. Emotional overeating and its associations with eating disorder psychopathology among overweight patients with Binge eating disorder. Int. J. Eat. Disord. 2006, 39, 141–146. [Google Scholar]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Meule, A.; Reichenberger, J.; Blechert, J. Development and preliminary validation of the Salzburg Stress Eating Scale. Appetite 2018, 120, 442–448. [Google Scholar] [CrossRef]
- Garaulet, M. Validation of a questionnaire on emotional eating for use in cases of obesity: The Emotional Eater Questionnaire (EEQ). Nutr. Hosp. 2012, 27, 645–651. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem Med (Zagreb). Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- González, M. Validación del Cuestionario de Comedor Emocional (CCE) en Chile. Gen 2018, 72, 21–24. [Google Scholar]
- Ware, J.E.; Gandek, B. Methods for Testing Data Quality, Scaling Assumptions, and Reliability: The IQOLA Project Approach. J. Clin. Epidemiol. 1998, 51, 945–952. [Google Scholar] [CrossRef]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. El Cuestionario de Salud SF-36 español: Una década de experiencia y nuevos desarrollos. Gac. Sanit. 2005, 19, 135–150. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-91112005000200007&lng=es&nrm=iso&tlng=es (accessed on 26 August 2022). [CrossRef]
- EQ-5D User Guides—EQ-5D. Available online: https://euroqol.org/publications/user-guides/ (accessed on 26 August 2022).
- Ministerio de Sanidad–Portal Estadístico del SNS–Encuesta Europea de Salud en España. 2014. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/EncuestaEuropea/Enc_Eur_Salud_en_Esp_2014.htm (accessed on 26 August 2022).
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. Available online: https://pubmed.ncbi.nlm.nih.gov/6880820/ (accessed on 22 June 2021). [CrossRef]
- Carmen Terol-Cantero, M.; Cabrera-Perona, V.; Martín-Aragón, M. Revisión de estudios de la Escala de Ansiedad y Depresión Hospitalaria (HAD) en muestras españolas. An. Psicol. 2015, 31, 494–503. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-97282015000200013&lng=es&nrm=iso&tlng=es (accessed on 26 August 2022). [CrossRef]
- IBM Support. Available online: https://www.ibm.com/mysupport/s/?language=en_US (accessed on 25 August 2022).
- Bentler, P.M. EQS 6, Structural Equations Program Manual; Multivariate Software Inc.—References—Scientific Research Publishing: Encino, CA, USA, 2006. [Google Scholar]
- Kelloway, K.E. Using LISREL for Structural Equation Modeling: A Researcher’s Guide; Sage: Thousand Oaks, CA, USA, 1998; 160p. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling A Multidiscip. J. 2009, 6, 1–55. [Google Scholar] [CrossRef]
- EQS Download—Mvsoft. 2012. Available online: https://mvsoft.com/eqsdownload/ (accessed on 25 August 2022).
- Hooker, S.A. SF-36. Encyclopedia of Behavioral Medicine. 2013, pp. 1784–1786. Available online: https://link.springer.com/referenceworkentry/10.1007/978-1-4419-1005-9_1597 (accessed on 26 August 2022).
- Bongers, P.; Jansen, A. Emotional Eating Is Not What You Think It Is and Emotional Eating Scales Do Not Measure What You Think They Measure. Front. Psychol. 2016, 7, 1932. Available online: https://pmc/articles/PMC5143883/ (accessed on 30 March 2022). [CrossRef] [PubMed]
- Lin, C.J.; Deroo, L.A.; Jacobs, S.R.; Sandler, D.P. Accuracy and reliability of self-reported weight and height in the Sister Study. Public Health Nutr. 2012, 15, 989. Available online: https://pmc/articles/PMC3511620/ (accessed on 26 August 2022). [CrossRef] [PubMed]
- Edelen, M.O.; Reeve, B.B. Applying item response theory (IRT) modeling to questionnaire development, evaluation, and refinement. Qual. Life Res. 2007, 16 (Suppl. S1), 5–18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Males | Females | Chi-Square or t-Test p-Values | Total Sample |
|---|---|---|---|---|
| Age | 22.44 (sd = 5.40) | 21.76 (sd = 4.91) | 2.27 (0.024) | 22.00 (sd = 5.10) |
| BMI | 24.06 (sd = 5.75) | 23.16 (sd = 5.35) | 2.79 (0.005) | 23.59 (sd = 6.74) |
| Low weight | 4.46% | 6.83% | 6% (n = 77) | |
| Normoweight | 63.62% | 70.50 % | 68.2% (n = 874) | |
| Overweight | 26.56% | 14.51% | 18.7% (n = 240) | |
| Obesity I | 2.23% | 2.28% | 4.8% (n = 62) | |
| Obesity II | 4.24% | 5.76% | 2.3% (n = 29) | |
| EEQ | 6.96 (sd = 4.81) | 9.75 (sd = 5.85) | −8.64 (<0.001) | 8.77 (sd = 5.66) |
| Not emotional | 44.87% | 27.22% | 33.4% (n = 428) | |
| Somewhat emotional | 36.16% | 33.81% | 34.6% (n = 444) | |
| Emotional | 17.63% | 33.57% | 27.8% (n = 356) | |
| Highly emotional | 2.01% | 5.04% | 4.2% (n = 54) | |
| HADS-A | 6.75 (sd = 3.92) | 8.39 (sd = 4.42) | −6.60 (<0.001) | 7.81 (sd = 4.32) |
| No case | 64.29% | 48.08% | 53.7% (n = 689) | |
| Doubtful case | 19.20% | 19.30% | 19.3% (n = 247) | |
| Case | 16.52% | 32.61% | 27% (n = 346) | |
| HADS-D | 4.23 (sd = 3.33) | 4.49 (sd = 3.43) | −1.28 (0.202) | 4.40 (sd = 3.40) |
| No case | 83.48% | 88.01% | 82% (n = 1051) | |
| Doubtful case | 12.28% | 6.12% | 12.5% (n = 161) | |
| Case | 4.24% | 5.88% | 5.5% (n = 70) | |
| EQ-5D | 0.89 (sd = 0.15) | 0.85 (sd = 0.16) | 4.09 (<0.001) | 0.86 (sd = 0.16) |
| SF36 Total | 76.77 (sd = 12.20) | 71.05 (sd = 13.16) | 7.61 (<0.001) | 73.05 (sd = 13.11) |
| SF36PF | 96.15 (sd = 6.64) | 93.23(sd = 10.32) | 5.42 (<0.001) | 94.25 (sd = 9.31) |
| SF36RP | 85.46 (sd = 17.90) | 82.01 (sd = 18.61) | 3.21 (0.001) | 83.22 (sd = 18.43) |
| SF36BP | 80.15 (sd = 20.13) | 74.50 (sd = 21.53) | 4.58 (<0.001) | 76.47 (sd = 21.21) |
| SF36GH | 68.36 (sd = 16.39) | 62.34 (sd = 16.42) | 6.26 (<0.001) | 64.45 (sd = 16.65) |
| SF36VT | 61.13 (sd = 18.41) | 54.10 (sd = 19.03) | 6.47 (<0.001) | 56.50 (sd = 19.11) |
| SF36SF | 80.66 (sd = 21.62) | 73.88 (sd = 23.75) | 5.03 (<0.001) | 76.25 (sd = 23.24) |
| SF36RE | 73.87 (sd = 23.31) | 66.54 (sd = 22.32) | 5.52 (<0.001) | 69.10 (sd = 22.92) |
| SF36MH | 68.39 (sd = 18.79) | 61.89 (sd = 18.71) | 5.93 (<0.001) | 64.16 (sd = 18.98) |
| Item | SD | Asymmetry | Kurtosis | Floor | Ceiling | |
|---|---|---|---|---|---|---|
| 1 | 0.88 | 0.939 | 0.909 | −0.052 | 41.5% | 9.2% |
| 2 | 1.41 | 0.768 | 0.640 | −0.090 | 6.2% | 11.2% |
| 3 | 0.79 | 0.901 | 1.004 | −0.187 | 46.6% | 6.9% |
| 4 | 0.80 | 0.811 | 0.883 | −0.374 | 40.1% | 4.5% |
| 5 | 1.34 | 0.932 | 0.390 | −0.686 | 17.4% | 14.8% |
| 6 | 1.01 | 0.940 | 0.609 | −0.561 | 35.3% | 8.6% |
| 7 | 0.95 | 0.907 | 0.479 | −0.846 | 38.8% | 4.8% |
| 8 | 0.63 | 0.804 | 1.159 | −0.685 | 54.1% | 3.4% |
| 9 | 0.35 | 0.690 | 2.160 | 4.472 | 74.1% | 2.7% |
| 10 | 0.61 | 0.810 | 1.341 | 1.331 | 54.8% | 4.7% |
| Measures | EEQ | F1 (Items: 2, 3, 4, 5, 6, 8) | F2 (Items: 1, 7, 9, 10) |
|---|---|---|---|
| SF36 Total | −0.398 (p < 0.001) | −0.368 (p < 0.001) | −0.332 (p < 0.001) |
| SF36PF a | −0.204 (p < 0.001) | −0.179 (p < 0.001) | −0.165 (p < 0.001) |
| SF36RP b | −0.207 (p < 0.001) | −0.165 (p < 0.001) | −0.174 (p < 0.001) |
| SF36BP c | −0.196 (p < 0.001) | −0.202 (p < 0.001) | −0.140 (p < 0.001) |
| SF36GH d | −0.271 (p < 0.001) | −0.252 (p < 0.001) | −0.204 (p < 0.001) |
| SF36VT e | −0.326 (p < 0.001) | −0.310 (p < 0.001) | −0.291 (p < 0.001) |
| SF36SF f | −0.284 (p < 0.001) | −0.270 (p < 0.001) | −0.261 (p < 0.001) |
| SF36RE g | −0.306 (p < 0.001) | −0.305 (p < 0.001) | −0.247 (p < 0.001) |
| SF36MH h | −0.367 (p < 0.001) | −0.331 (p < 0.001) | −0.341 (p < 0.001) |
| EQ5D Coeff. i | −0.256 (p < 0.001) | −0.252 (p < 0.001) | −0.226 (p < 0.001) |
| HADS-anxiety j | 0.400 (p < 0.001) | 0.361 (p < 0.001) | 0.359 (p < 0.001) |
| HADS-depression k | 0.360 (p < 0.001) | 0.335 (p < 0.001) | 0.322 (p < 0.001) |
| BMI l | 0.204 (p < 0.001) | 0.127 (p < 0.001) | 0.227 (p < 0.001) |
| EEQ Items | Component 1 | Component 2 |
|---|---|---|
| 1. Does the scale have a great power over you? Is it able to change your mood? | 0.183 | 0.689 |
| 2. Do you tend to have a whim for certain foods? | 0.591 | 0.231 |
| 3. Do you find it difficult to stop eating sweet foods, especially chocolate? | 0.587 | 0.204 |
| 4. Do you have problems controlling the amounts of certain foods? | 0.557 | 0.388 |
| 5. Do you eat when you are stressed, angry, or bored? | 0.674 | 0.245 |
| 6. Do you eat more of your favourite foods, and eat more out of control, when you are alone? | 0.650 | 0.196 |
| 7. Do you feel guilty when you eat forbidden foods, i.e., foods that you think you should not eat, such as sweets or snacks? | 0.207 | 0.690 |
| 8. In the evening, when you come home tired from work, is it when you feel most out of control in your eating? | 0.403 | 0.326 |
| 9. You are on a diet, and for some reason you eat more than you should, so ¿do you think it is not worth it and, therefore, you eat in an uncontrolled way those foods that you think will make you gain weight? | 0.394 | 0.503 |
| 10. How often do you feel that food controls you instead of you controlling it? | 0.457 | 0.656 |
| Model | x2- | DF | X2/DF | CFI | IFI | RMSEA |
|---|---|---|---|---|---|---|
| Model 1 (Garaulet et al., 2012) [24] | 261.05 | 32 | 8.16 | 0.922 | 0.922 | 0.075 |
| Model 2 (Bernabéu et al., 2020) [13] | 119.42 | 33 | 3.62 | 0.970 | 0.971 | 0.045 |
| Model 3 (proposed) | 101.75 | 33 | 3.08 | 0.977 | 0.977 | 0.040 |
| Corrected Item-Total Correlation | Cronbach’s Alpha If the Item Has Been Removed | |
|---|---|---|
| 1. Does the scale have a great power over you? Is it able to change your mood? | 0.528 | 0.849 |
| 2. Do you tend to have a whim for certain foods? | 0.575 | 0.845 |
| 3. Do you find it difficult to stop eating sweet foods, especially chocolate? | 0.557 | 0.846 |
| 4. Do you have problems controlling the amounts of certain foods? | 0.623 | 0.841 |
| 5. Do you eat when you are stressed, angry, or bored? | 0.597 | 0.842 |
| 6. Do you eat more of your favourite foods, and eat more out of control, when you are alone? | 0.577 | 0.844 |
| 7. Do you feel guilty when you eat forbidden foods, i.e., Foods that you think you should not eat, such as sweets or snacks? | 0.525 | 0.849 |
| 8. In the evening, when you come home tired from work, is it when you feel most out of control in your eating? | 0.444 | 0.855 |
| 9. You are on a diet, and for some reason you eat more than you should, so ¿do you think it is not worth it and, therefore, you eat in an uncontrolled way those foods that you think will make you gain weight? | 0.580 | 0.845 |
| 10. How often do you feel that food controls you instead of you controlling it? | 0.687 | 0.835 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sosa-Cordobés, E.; García-Padilla, F.M.; Ortega-Galán, Á.M.; Sánchez-Alcón, M.; Garrido-Fernández, A.; Ramos-Pichardo, J.D. Psychometric Properties of the Emotional Eater Questionnaire in University Students. Int. J. Environ. Res. Public Health 2022, 19, 10965. https://doi.org/10.3390/ijerph191710965
Sosa-Cordobés E, García-Padilla FM, Ortega-Galán ÁM, Sánchez-Alcón M, Garrido-Fernández A, Ramos-Pichardo JD. Psychometric Properties of the Emotional Eater Questionnaire in University Students. International Journal of Environmental Research and Public Health. 2022; 19(17):10965. https://doi.org/10.3390/ijerph191710965
Chicago/Turabian StyleSosa-Cordobés, Elena, Francisca María García-Padilla, Ángela María Ortega-Galán, Miriam Sánchez-Alcón, Almudena Garrido-Fernández, and Juan Diego Ramos-Pichardo. 2022. "Psychometric Properties of the Emotional Eater Questionnaire in University Students" International Journal of Environmental Research and Public Health 19, no. 17: 10965. https://doi.org/10.3390/ijerph191710965
APA StyleSosa-Cordobés, E., García-Padilla, F. M., Ortega-Galán, Á. M., Sánchez-Alcón, M., Garrido-Fernández, A., & Ramos-Pichardo, J. D. (2022). Psychometric Properties of the Emotional Eater Questionnaire in University Students. International Journal of Environmental Research and Public Health, 19(17), 10965. https://doi.org/10.3390/ijerph191710965