

Leadership Effectiveness in Healthcare Settings: A Systematic Review and Meta-Analysis of Cross-Sectional and Before–After Studies

 ,
, 
 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
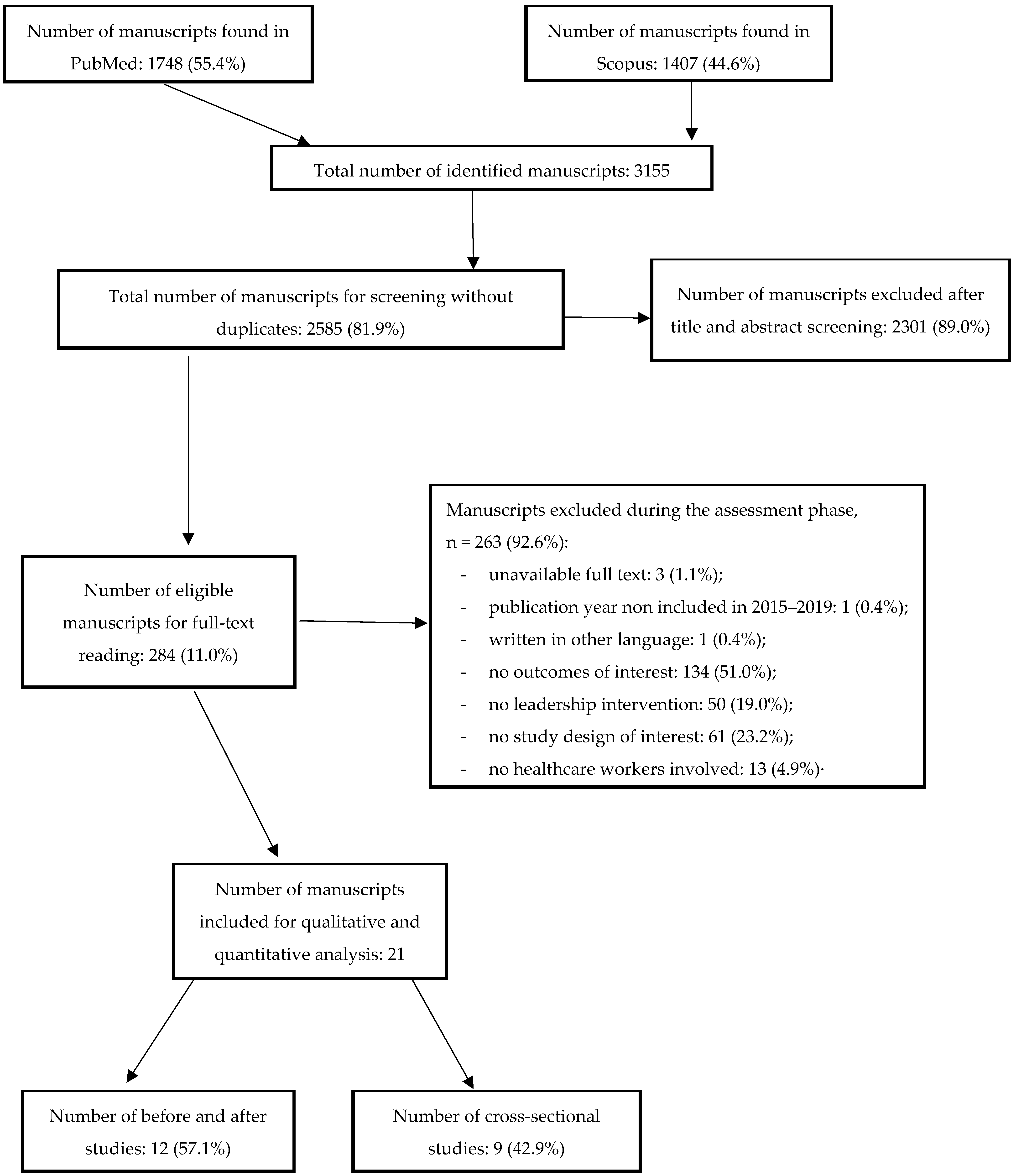
2.1. Data Sources and Search Strategy
2.2. Study Selection and Data Extraction
2.3. Statistical Data Analysis
- for cross-sectional studies, the outcome of interest was the correlation between leadership improvement and guideline adherence or healthcare performance;
- the outcome derived from before–after studies or the trial was the percentage of leadership improvement intervention in guideline adherence or healthcare performance;
- the incidence occurrence of improved results among exposed and not exposed healthcare workers of leadership interventions and the relative risks (RR) were the outcomes in cohort studies;
- the odds ratio (OR) between the case of healthcare workers who had received a leadership intervention and the control group for case-control studies.
3. Results
3.1. Studies Characteristics
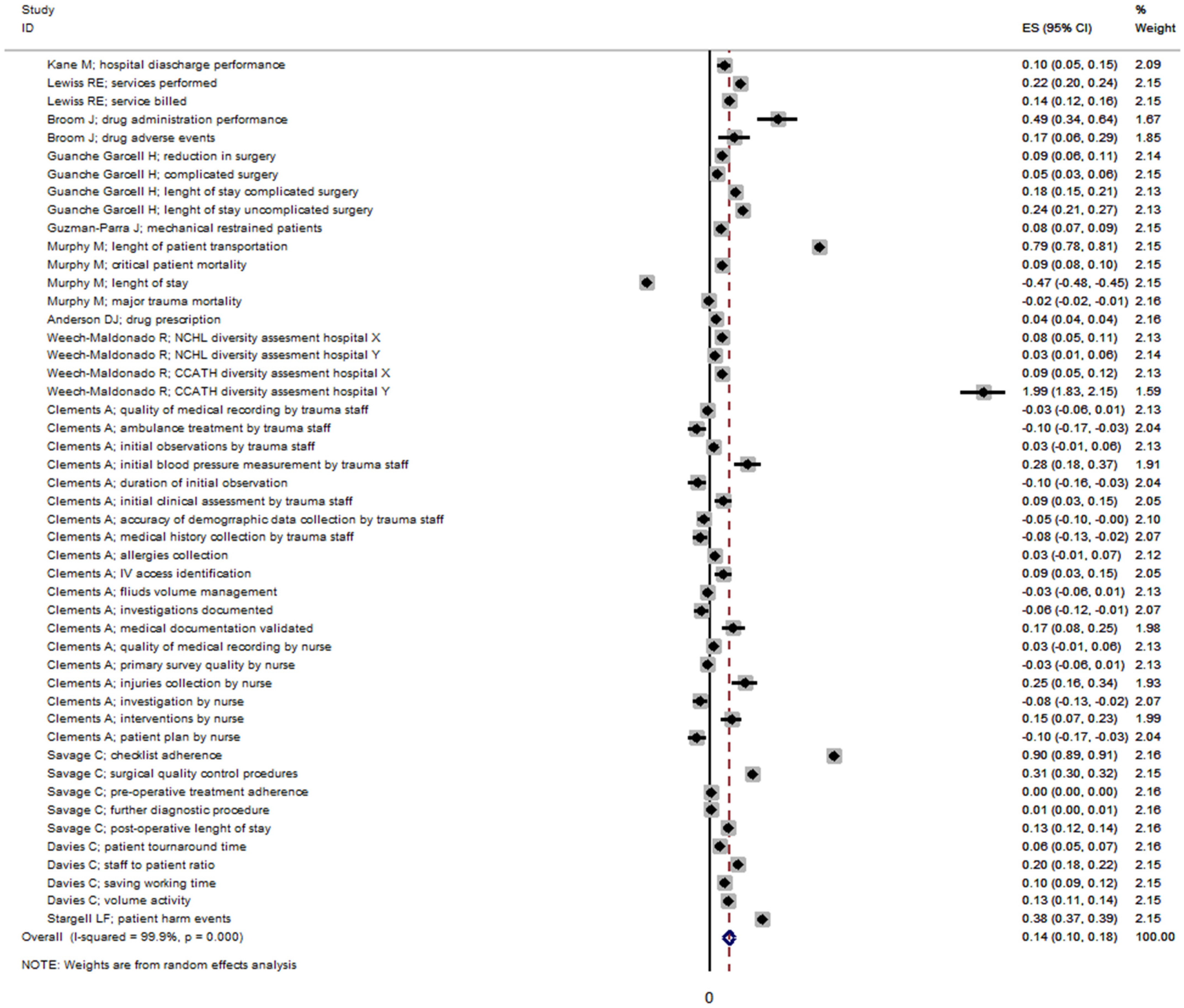
3.2. Leadership Effectiveness in before–after Studies
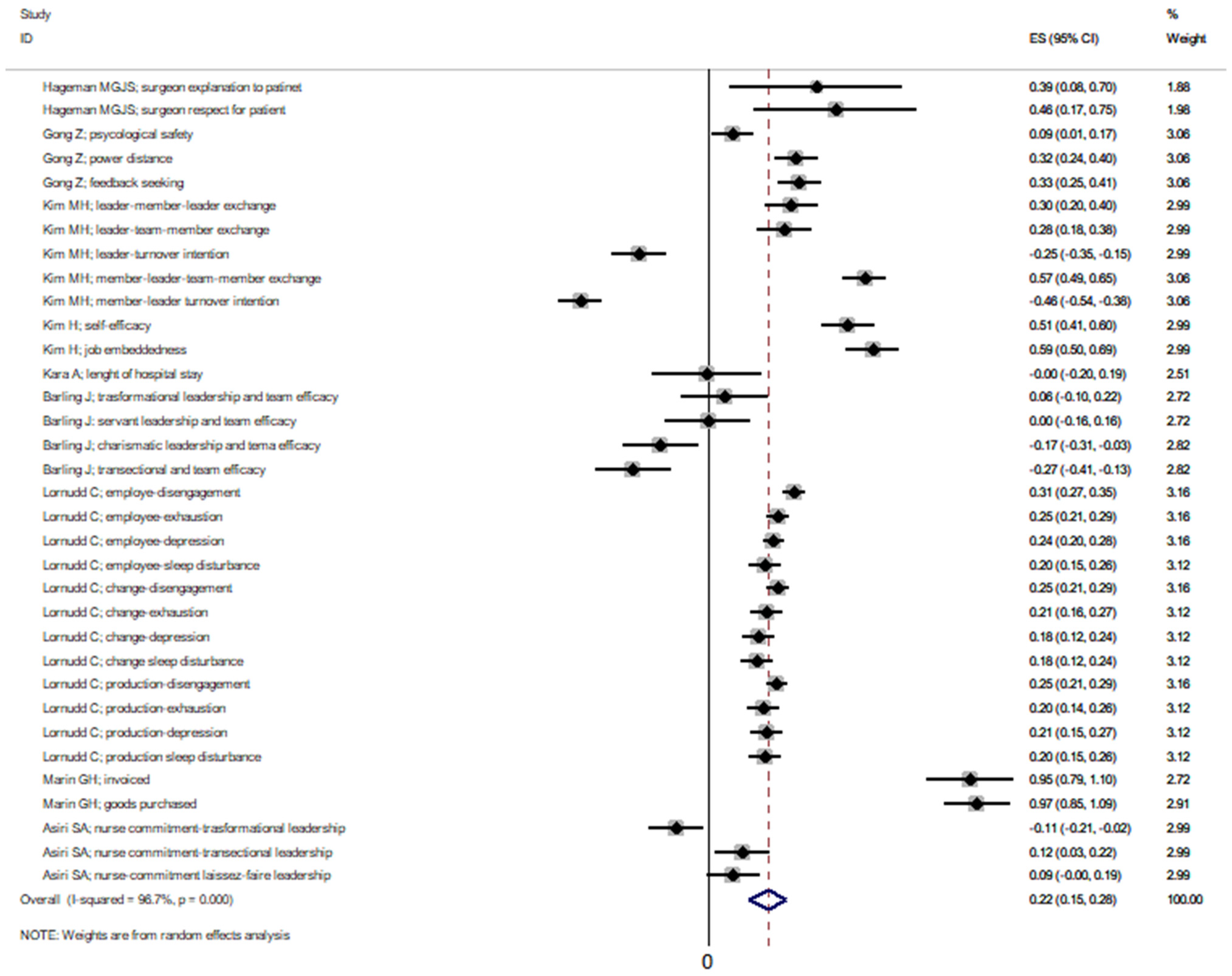
3.3. Leadership Effectiveness in Cross Sectional Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solà, G.J.I.; Badia, J.G.I.; Hito, P.D.; Osaba, M.A.C.; Del Val García, J.L. Self-Perception of Leadership Styles and Behaviour in Primary Health Care. BMC Health Serv. Res. 2016, 16, 572. [Google Scholar] [CrossRef]
- Flodgren, G.; O’Brien, M.A.; Parmelli, E.; Grimshaw, J.M. Local Opinion Leaders: Effects on Professional Practice and Healthcare Outcomes. Cochrane Database Syst. Rev. 2019, 6, CD000125. [Google Scholar] [CrossRef]
- Galaviz, K.I.; Narayan, K.M.V.; Manders, O.C.; Torres-Mejía, G.; Goenka, S.; McFarland, D.A.; Reddy, K.S.; Lozano, R.; Valladares, L.M.; Prabhakaran, D.; et al. The Public Health Leadership and Implementation Academy for Noncommunicable Diseases. Prev. Chronic. Dis. 2019, 16, E49. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.D.C.; Khiljee, N. Leadership in Healthcare. Anaesth. Intensive Care Med. 2016, 17, 63–65. [Google Scholar] [CrossRef]
- Chigudu, S.; Jasseh, M.; d’Alessandro, U.; Corrah, T.; Demba, A.; Balen, J. The Role of Leadership in People-Centred Health Systems: A Sub-National Study in The Gambia. Health Policy Plan. 2014, 33, e14–e25. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.-S. Leadership Styles and Organization Structural Configurations. J. Hum. Resour. Adult Learn. 2006, 2, 39–46. [Google Scholar]
- Denis, J.-L.; van Gestel, N. Medical Doctors in Healthcare Leadership: Theoretical and Practical Challenges. BMC Health Serv. Res. 2016, 16, 158. [Google Scholar] [CrossRef]
- Mutale, W.; Vardoy-Mutale, A.-T.; Kachemba, A.; Mukendi, R.; Clarke, K.; Mulenga, D. Leadership and Management Training as a Catalyst to Health System Strengthening in Low-Income Settings: Evidence from Implementation of the Zambia Management and Leadership Course for District Health Managers in Zambia. PLoS ONE 2017, 12, e0174536. [Google Scholar] [CrossRef]
- Braun, S.; Kark, R.; Wisse, B. Editorial: Fifty Shades of Grey: Exploring the Dark Sides of Leadership and Followership. Front. Psychol. 2018, 9, 1877. [Google Scholar] [CrossRef]
- Fatima, T.; Majeed, M.; Shah, S.Z.A. Jeopardies of Aversive Leadership: A Conservation of Resources Theory Approach. Front. Psychol. 2018, 9, 1935. [Google Scholar] [CrossRef]
- Abraham, T.H.; Stewart, G.L.; Solimeo, S.L. The Importance of Soft Skills Development in a Hard Data World: Learning from Interviews with Healthcare Leaders. BMC Med. Educ. 2021, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ovretveit, J. Improvement Leaders: What Do They and Should They Do? A Summary of a Review of Research. Qual. Saf. Health Care 2010, 19, 490–492. [Google Scholar] [CrossRef]
- Saxena, A.; Desanghere, L.; Stobart, K.; Walker, K. Goleman’s Leadership Styles at Different Hierarchical Levels in Medical Education. BMC Med. Educ. 2017, 17, 169. [Google Scholar] [CrossRef]
- Ford, K.; Menchine, M.; Burner, E.; Arora, S.; Inaba, K.; Demetriades, D.; Yersin, B. Leadership and Teamwork in Trauma and Resuscitation. West. J. Emerg. Med. 2016, 17, 549–556. [Google Scholar] [CrossRef]
- Dubinsky, I.; Feerasta, N.; Lash, R. A Model for Physician Leadership Development and Succession Planning. Healthc. Q. Tor. Ont 2015, 18, 38–42. [Google Scholar] [CrossRef]
- Stahlhut, R.W.; Porterfield, D.S.; Grande, D.R.; Balan, A. Characteristics of Population Health Physicians and the Needs of Healthcare Organizations. Am. J. Prev. Med. 2021, 60, 198–204. [Google Scholar] [CrossRef]
- Quince, T.; Abbas, M.; Murugesu, S.; Crawley, F.; Hyde, S.; Wood, D.; Benson, J. Leadership and Management in the Undergraduate Medical Curriculum: A Qualitative Study of Students’ Attitudes and Opinions at One UK Medical School. BMJ Open 2014, 4, e005353. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Sertel, G.; Karadag, E.; Ergin-Kocatürk, H. Effects of Leadership on Performance: A Cross-Cultural Meta-Analysis. Int. J. Cross Cult. Manag. 2022, 22, 59–82. [Google Scholar] [CrossRef]
- Hunziker, S.; Johansson, A.C.; Tschan, F.; Semmer, N.K.; Rock, L.; Howell, M.D.; Marsch, S. Teamwork and Leadership in Cardiopulmonary Resuscitation. J. Am. Coll. Cardiol. 2011, 57, 2381–2388. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis; ScienceOpen, Inc.: Burlington, MA, USA, 2000. [Google Scholar]
- Quality Assessment Tool for Studies with No Control Group. Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 March 2021).
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Fleiss, J.L. The Statistical Basis of Meta-Analysis. Stat. Methods Med. Res. 1993, 2, 121–145. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel Plots for Detecting Bias in Meta-Analysis: Guidelines on Choice of Axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Palmer, T.M.; Sterne, J.A.C. (Eds.) Meta-Analysis in Stata: An Updated Collection from the Stata Journal, 2nd ed.; StataCorp LLC: College Station, TX, USA, 2015. [Google Scholar]
- Clements, A.; Curtis, K.; Horvat, L.; Shaban, R.Z. The Effect of a Nurse Team Leader on Communication and Leadership in Major Trauma Resuscitations. Int. Emerg. Nurs. 2015, 23, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Lornudd, C.; Tafvelin, S.; von Thiele Schwarz, U.; Bergman, D. The Mediating Role of Demand and Control in the Relationship between Leadership Behaviour and Employee Distress: A Cross-Sectional Study. Int. J. Nurs. Stud. 2015, 52, 543–554. [Google Scholar] [CrossRef]
- Savage, C.; Gaffney, F.A.; Hussain-Alkhateeb, L.; Olsson Ackheim, P.; Henricson, G.; Antoniadou, I.; Hedsköld, M.; Pukk Härenstam, K. Safer Paediatric Surgical Teams: A 5-Year Evaluation of Crew Resource Management Implementation and Outcomes. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2017, 29, 853–860. [Google Scholar] [CrossRef]
- Kane, M.; Weinacker, A.; Arthofer, R.; Seay-Morrison, T.; Elfman, W.; Ramirez, M.; Ahuja, N.; Pickham, D.; Hereford, J.; Welton, M. A Multidisciplinary Initiative to Increase Inpatient Discharges Before Noon. J. Nurs. Adm. 2016, 46, 630–635. [Google Scholar] [CrossRef]
- Lewiss, R.E.; Cook, J.; Sauler, A.; Avitabile, N.; Kaban, N.L.; Rabrich, J.; Saul, T.; Siadecki, S.D.; Wiener, D. A Workflow Task Force Affects Emergency Physician Compliance for Point-of-Care Ultrasound Documentation and Billing. Crit. Ultrasound. J. 2016, 8, 5. [Google Scholar] [CrossRef]
- Broom, J.; Tee, C.L.; Broom, A.; Kelly, M.D.; Scott, T.; Grieve, D.A. Addressing Social Influences Reduces Antibiotic Duration in Complicated Abdominal Infection: A Mixed Methods Study. ANZ J. Surg. 2019, 89, 96–100. [Google Scholar] [CrossRef] [Green Version]
- Guanche Garcell, H.; Valle Gamboa, M.E.; Guelmes Dominguez, A.A.; Hernández Hernandez, E.; Bode Sado, A.; Alfonso Serrano, R.N. Effect of a Quality Improvement Intervention to Reduce the Length of Stay in Appendicitis. J. Healthc. Qual. Res. 2019, 34, 228–232. [Google Scholar] [CrossRef]
- Guzman-Parra, J.; Aguilera Serrano, C.; García-Sánchez, J.A.; Pino-Benítez, I.; Alba-Vallejo, M.; Moreno-Küstner, B.; Mayoral-Cleries, F. Effectiveness of a Multimodal Intervention Program for Restraint Prevention in an Acute Spanish Psychiatric Ward. J. Am. Psychiatr. Nurses Assoc. 2016, 22, 233–241. [Google Scholar] [CrossRef]
- Murphy, M.; McCloughen, A.; Curtis, K. The Impact of Simulated Multidisciplinary Trauma Team Training on Team Performance: A Qualitative Study. Australas. Emerg. Care 2019, 22, 1–7. [Google Scholar] [CrossRef]
- Anderson, D.J.; Watson, S.; Moehring, R.W.; Komarow, L.; Finnemeyer, M.; Arias, R.M.; Huvane, J.; Bova Hill, C.; Deckard, N.; Sexton, D.J.; et al. Feasibility of Core Antimicrobial Stewardship Interventions in Community Hospitals. JAMA Netw. Open 2019, 2, e199369. [Google Scholar] [CrossRef]
- Weech-Maldonado, R.; Dreachslin, J.L.; Epané, J.P.; Gail, J.; Gupta, S.; Wainio, J.A. Hospital Cultural Competency as a Systematic Organizational Intervention: Key Findings from the National Center for Healthcare Leadership Diversity Demonstration Project. Health Care Manag. Rev. 2018, 43, 30–41. [Google Scholar] [CrossRef]
- Davies, C.; Lyons, C.; Whyte, R. Optimizing Nursing Time in a Day Care Unit: Quality Improvement Using Lean Six Sigma Methodology. Int. J. Qual. Health Care 2019, 31 (Suppl. S1), 22–28. [Google Scholar] [CrossRef]
- Stargell, L.F.; Heatherly, S.L. Managing What Is Measured: A Rural Hospital’s Experience in Reducing Patient Harm. J. Healthc. Qual. Off. Publ. Natl. Assoc. Healthc. Qual. 2018, 40, 172–176. [Google Scholar] [CrossRef]
- Hageman, M.G.J.S.; Ring, D.C.; Gregory, P.J.; Rubash, H.E.; Harmon, L. Do 360-Degree Feedback Survey Results Relate to Patient Satisfaction Measures? Clin. Orthop. 2015, 473, 1590–1597. [Google Scholar] [CrossRef]
- Gong, Z.; Van Swol, L.; Xu, Z.; Yin, K.; Zhang, N.; Gul Gilal, F.; Li, X. High-Power Distance Is Not Always Bad: Ethical Leadership Results in Feedback Seeking. Front. Psychol. 2019, 10, 2137. [Google Scholar] [CrossRef]
- Kim, M.-H.; Yi, Y.-J. Impact of Leader-Member-Exchange and Team-Member-Exchange on Nurses’ Job Satisfaction and Turnover Intention. Int. Nurs. Rev. 2019, 66, 242–249. [Google Scholar] [CrossRef]
- Kim, H.; Kim, K. Impact of Self-Efficacy on the Self-Leadership of Nursing Preceptors: The Mediating Effect of Job Embeddedness. J. Nurs. Manag. 2019, 27, 1756–1763. [Google Scholar] [CrossRef]
- Kara, A.; Johnson, C.S.; Nicley, A.; Niemeier, M.R.; Hui, S.L. Redesigning Inpatient Care: Testing the Effectiveness of an Accountable Care Team Model. J. Hosp. Med. 2015, 10, 773–779. [Google Scholar] [CrossRef]
- Barling, J.; Akers, A.; Beiko, D. The Impact of Positive and Negative Intraoperative Surgeons’ Leadership Behaviors on Surgical Team Performance. Am. J. Surg. 2018, 215, 14–18. [Google Scholar] [CrossRef]
- Marin, G.H.; Silberman, M.; Colombo, M.V.; Ozaeta, B.; Henen, J. Manager’s Leadership Is the Main Skill for Ambulatory Health Care Plan Success. J. Ambul. Care Manag. 2015, 38, 59–68. [Google Scholar] [CrossRef]
- Asiri, S.A.; Rohrer, W.W.; Al-Surimi, K.; Da’ar, O.O.; Ahmed, A. The Association of Leadership Styles and Empowerment with Nurses’ Organizational Commitment in an Acute Health Care Setting: A Cross-Sectional Study. BMC Nurs. 2016, 15, 38. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; deBeer, H.; et al. GRADE Guidelines: 1. Introduction—GRADE Evidence Profiles and Summary of Findings Tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Correlation Coefficient | Beta Coefficient | 95% CI | |
|---|---|---|---|---|
| Studies conducted between 2012–2019 vs. 2005–2011 years | −0.26 | −0.09 | −0.42 | 0.24 |
| North American continent vs. others | 0.27 | −0.04 | −0.82 | 0.75 |
| Oceanian continent vs. others | −0.26 | −0.33 | −1.25 | 0.59 |
| European continent vs. others | 0.07 | −0.27 | −1.12 | 0.58 |
| Public hospital vs. private hospital | 0.01 | |||
| Surgical specialty vs. non-surgical specialty | −0.21 | −0.05 | −0.85 | 0.75 |
| Leadership style transformational vs. other styles | 0.12 | 0.32 | −0.47 | 1.11 |
| Leadership style charismatic vs. other styles | −0.23 | 0.24 | −0.69 | 1.17 |
| Leadership style transactional vs. other styles | 0.25 | 0.25 | −0.40 | 0.91 |
| Variables | Correlation Coefficient | Beta Coefficient | 95% CI | |
|---|---|---|---|---|
| Studies conducted between 2012–2019 vs. 2005–2011 years | −0.31 | −0.09 | −0.27 | 0.10 |
| South American continent vs. others | 0.63 | 0.56 * | 0.13 | 0.99 |
| Private hospital vs. public hospital | 0.17 | 0.60 * | 0.14 | 1.06 |
| Surgical specialty vs. non-surgical specialty | −0.22 | −0.28 * | −0.54 | −0.02 |
| Leadership style transformational vs. other styles | 0.41 | 0.16 | −0.14 | 0.46 |
| Leadership style charismatic vs. other styles | −0.14 | −0.04 | −0.26 | 0.18 |
| Leadership style transactional vs. other styles | −0.11 | 0.01 | −0.21 | 0.23 |
| Multiprofessional team vs. single professional team | 0.04 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restivo, V.; Minutolo, G.; Battaglini, A.; Carli, A.; Capraro, M.; Gaeta, M.; Odone, A.; Trucchi, C.; Favaretti, C.; Vitale, F.; et al. Leadership Effectiveness in Healthcare Settings: A Systematic Review and Meta-Analysis of Cross-Sectional and Before–After Studies. Int. J. Environ. Res. Public Health 2022, 19, 10995. https://doi.org/10.3390/ijerph191710995
Restivo V, Minutolo G, Battaglini A, Carli A, Capraro M, Gaeta M, Odone A, Trucchi C, Favaretti C, Vitale F, et al. Leadership Effectiveness in Healthcare Settings: A Systematic Review and Meta-Analysis of Cross-Sectional and Before–After Studies. International Journal of Environmental Research and Public Health. 2022; 19(17):10995. https://doi.org/10.3390/ijerph191710995
Chicago/Turabian StyleRestivo, Vincenzo, Giuseppa Minutolo, Alberto Battaglini, Alberto Carli, Michele Capraro, Maddalena Gaeta, Anna Odone, Cecilia Trucchi, Carlo Favaretti, Francesco Vitale, and et al. 2022. "Leadership Effectiveness in Healthcare Settings: A Systematic Review and Meta-Analysis of Cross-Sectional and Before–After Studies" International Journal of Environmental Research and Public Health 19, no. 17: 10995. https://doi.org/10.3390/ijerph191710995
APA StyleRestivo, V., Minutolo, G., Battaglini, A., Carli, A., Capraro, M., Gaeta, M., Odone, A., Trucchi, C., Favaretti, C., Vitale, F., & Casuccio, A. (2022). Leadership Effectiveness in Healthcare Settings: A Systematic Review and Meta-Analysis of Cross-Sectional and Before–After Studies. International Journal of Environmental Research and Public Health, 19(17), 10995. https://doi.org/10.3390/ijerph191710995