Abstract
Objective: This study aimed to describe neurodevelopment in fetal growth restriction children at the age of six. Secondly, we tried to demonstrate influencing factors that can improve or exacerbate this development, as well as predictive factors that might select a population at risk to assist with early childhood support. Method: It was a study of 70 children affected with FGR. FGR was based on these definitions: birth weight below the 3rd percentile or birth weight below the 10th percentile with an abnormal hemodynamic Doppler study. Neurodevelopment was assessed at 6 years old by means of Batelle Development Inventory. A global development quotient under a 100 score was considered a neurodevelopment delay. All variables regarding pregnancy care, delivery episode, postpartum, neonatal care, sociodemographic issues, and the need for support in the first years were studied. Results: The mean gestational age at diagnosis was 33.14 weeks (standard deviation (SD = 4.31), with 32.9% of early-onset diagnoses. The mean gestational age at delivery was 35.61 (SD = 3.21), and the cesarean rate was 64.3%. The average age of the children at the moment of the evaluation was 76.20-month-old (SD = 3.70). The mean global development quotient was 97.28 (SD = 13.97). We were able to record a 57.1% of global development delay. In the cases of cognition, only 17.1% of the children registered a delay. Motor and communication skills were the most frequently affected. We discovered that socioeconomic status was positively related to the global development quotient, as well as both gestational age at delivery and middle cerebral artery pulsatility index was positively related to the global development quotient. Conclusions: We found a higher neurodevelopment delay rate (57.1%). We could relate a higher gestational age at delivery and a higher MCA percentile with better global neurodevelopment quotients.
1. Introduction
Fetal growth restriction (FGR) is a pregnancy complication that occurs in approximately 10% of pregnancies worldwide. In this complication, fetuses cannot reach their predestinated genetic weight. Its multiple causes could be divided into two groups: due to placental insufficiency supply and non-placental origin (genetics or chromosomal disorders, congenital infections, or metabolic disorders). The classical definition of FGR was a fetus whose estimated weight was below the 10th percentile. Doppler study incorporation allows for differentiation between genetic small for gestational age fetuses and real FGR due to insufficiency of placental supply [1,2].
FGR could be divided into two groups depending on its onset, placental ischemic degree, and chronicity: early-onset and late-onset. Early-onset FGR is associated with early and severe ischemic placental involvement. It is associated with a high uterine artery pulsatility index measurement [3] and an elevated rate of early-onset preeclampsia, close to 70% [4]. Usually, umbilical artery (UA) Doppler is pathological at diagnosis, and associated with elevated severe neonatal outcomes [5]. Induced prematurity is a frequent outcome due to fetal deterioration, with high morbidity and mortality rates. Late-onset FGR has the same etiopathogenic basis, although it is a minor, late, and acute condition [6]. Its association with preeclampsia is less frequent, close to 8–15% [4,7]. UA usually is normal at diagnosis, even if they have circulation redistribution as a middle cerebral artery (MCA) or the ratio measurement is abnormal [7,8]. Commonly, neonatal morbidity rates are lower, but stillbirth and mortality are higher [7].
Adverse neonatal outcome in FGR has been exhaustively researched. TRUFFLE study described short-term outcomes in a cohort of fetuses with FGR. Prematurity was strongly associated with adverse neonatal outcomes, being more frequent neonatal sepsis and bronchopulmonary dysplasia. Adverse outcomes were more frequent at a lower gestational age at delivery or associated with hypertensive states [2].
Childhood and adulthood development could be affected by FGR [9]. Recently, interest in long-term outcomes is increasing. Specifically, cognitive and motor development, as well as brain structure development, is a primary field of study. The fetal period and early childhood are sensitive stages where genomic interactions with the environment occur as organs and systems acquire their long-term functions. Induced prematurity is a risk factor for adverse neurological outcomes. Those children could be affected by visual and auditory disabilities, coordination disorders, cognitive, and behavioral conditions and, in extreme cases, cerebral palsy [10]. Adverse neurological outcomes could be due to prematurity or as a consequence of FGR, although this connection is complex to link. In both cases, motor, cognitive and behavioral development could be affected by a hostile environment.
Multiple studies in animal models have demonstrated changes in brain structure. More precisely, induced hypoxia in animals has shown a reduction in neuron quantity [11] and a significant modification of dendritic arbors [12]. Other studies have demonstrated a delay in myelin production that could affect normal nervous conduction in the early stages [13,14]. This process is crucial to cognitive development in childhood. Furthermore, those changes have been appreciated in different concentrations of metabolites and neurotransmitters [15,16,17]. Studies in human models have also demonstrated a decrease in brain volume [18,19,20], a reduction in grey matter volume [18,21,22], as well as differences in white matter [23,24] and gyrification patterns [25] in FGR children. These modifications could affect cognitive, motor, and behavior development.
Poor cognitive development, behavioral disabilities, and academic difficulties have been related to FGR. Different studies have shown a higher incidence of neurodevelopmental disabilities in premature infants with FGR compared with preterm infants with adequate growth [26,27,28,29]. Late-onset FGR has also been related to cognitive disabilities and academic difficulties, but published data are contradictory and differences between groups tend to be minimal [30,31,32,33,34].
Even though the relationship between Doppler alterations and neonatal outcomes has been well established, the relationship with neurodevelopment has not been yet elucidated. Different studies have tried to link umbilical and middle cerebral artery alterations to cognitive and motor disabilities in childhood [35,36,37]. Classically, brain sparing has been associated with adaptative phenomena, but more recent studies have associated this process with poor cognitive and behavioral development [38,39,40,41,42,43,44]. In a recent systematic review, we were able to connect poor intelligence quotient results in children with brain sparing, but an association with motor or behavioral disabilities was difficult to link. These could be due to heterogeneity in the studies analyzed, great variety in both specific tests and ages of assessment, different definitions of brain sparing and lack of control of confounders [45]. In severe cases, the deleterious consequences of brain sparing on neurodevelopment could overpass the benefits of the sparing, leading to a wide spectrum of clinical manifestations [45].
We believe that FGR causes development disabilities in adaptative, motor, communication, and cognitive spheres during childhood. This study aimed to describe neurodevelopment in FGR children at six years of age. Secondly, we tried to demonstrate influencing factors that can improve or exacerbate this development, as well as predictive factors that might help us select a population at risk to assist with early childhood support.
2. Materials and Methods
2.1. Design and Population
This study was designed as a retrospective cohort study, in which we selected a group of children with fetal growth restriction born in 2015 at University Hospital Carlos Haya, Málaga, Spain. Inclusion criteria were based on FGR definition: less than the 3rd percentile birth weight or less than the 10th percentile birth weight with abnormal hemodynamic Doppler study. The abnormal hemodynamic study was defined as a pulsatility index (PI) of umbilical artery (UA) above the 95th percethe ntile, PI of middle cerebral artery (MCA) below the 5th percentile, cerebroplacental ratio (CPR) below the 5th percentile, or PI of uterine arteries above the 95th percentile. The CPR was calculated by dividing the PI of the MCA by the PI of the UA. A CPR below the 5th percentile was defined as brain sparing effect. Exclusion criteria were structural and chromosomal abnormalities, multiple pregnancies and small for gestational age. Once approval was obtained from the regional ethics committee, recruitment started in 2021. Parental consent was obtained before starting the procedure. Data were collected from clinical records, parents’ reports, and individually assessed children with Battelle Developmental Inventory (screening test).
2.2. Neurodevelopment Follow-Up at 6 Years Old
At the age of six, a Batelle Developmental Inventory (BDI) screening test (Spanish Edition) was performed prospectively [46]. We selected this screening test because it has a good correlation with the total inventory. The correlation level was 0.96 on all scales, except for the cognitive scale which was 0.92 [47]. This battery includes 96 items divided into five scales: personal-social, adaptive, motor, communicative and cognitive scale. Finally, a global score was obtained and converted into an equivalent developmental age on each scale. The items are presented in a standardized format, specifying the behavior or characteristic to be evaluated. This evaluation was performed individually and the average time to complete the test was approximately one hour. Information was obtained by means of direct observation, parental interviews, and direct children assessment. The global development quotient was obtained using Moraleda’s formula as follows: dividing the equivalent developmental age by the real age multiplied by 100 [47]. We considered the upper limit of the range at the final equivalent age of the BDI to calculate this ratio. Children were considered to have a developmental delay if their score was lower than 100 [48].
2.3. Parent Reports
At the same time that the children were assessed, a questionary was provided to the parents. In this report, they were requested to provide information about sociodemographic items and children’s issues during the first years of life (necessity of early child support, academic difficulties, and illnesses during childhood). Completion of the questionary required circa 15 min.
2.4. Data Collection
Medical records were searched for data about pregnancy and neonatal care during the first days of life. We registered variables about pregnancy care, delivery episode, postpartum, as well as weight, length, and head circumference of the neonate. We recorded the days of neonatal intensive care unit (NICU) admission and adverse neonatal outcomes if this was the case. NICU admission was considered when newborns required invasive care or close monitoring by neonatal pediatricians. Those children who remained with their mothers in the maternity ward were not considered in this group.
2.5. Statistical Analysis
Firstly, we carried out a descriptive analysis to detail the frequency distribution of the different variables in the cohort, as well as the frequency distribution of the developmental delay on each scale and global scale. Secondly, we explored the association between global development quotient and sociodemographic, pregnancy, Doppler measurement, delivery, and neonatal variables using the Student’s t-test or ANOVA test analysis.
Thirdly, multivariate analysis was accomplished to analyze moderating factors. Linear regression analyses were performed to examine the effect of (1) sociodemographic factors, (2) Doppler measurements, birth weight and age at delivery, and (3) postnatal factors. We incorporated all sociodemographic factors (maternal and paternal studies level, socioeconomic status, maternal and paternal occupational status, and separated parent status) in the first model. In the second model we included doppler measurements of UA, MCA, and CPR, birth weight and gestational age at delivery. In the third model, we included gestational age at delivery, gender, adverse neonatal outcomes, early childcare, academic difficulties, and nursery assistance. For all analyses, a p-value below 0.05 was considered significant. Data were processed and analyzed using the Statistical Package for the Social Sciences (SPSS), Version 22.0 (SPSS Inc., Chicago, IL, USA).
3. Results
3.1. Population
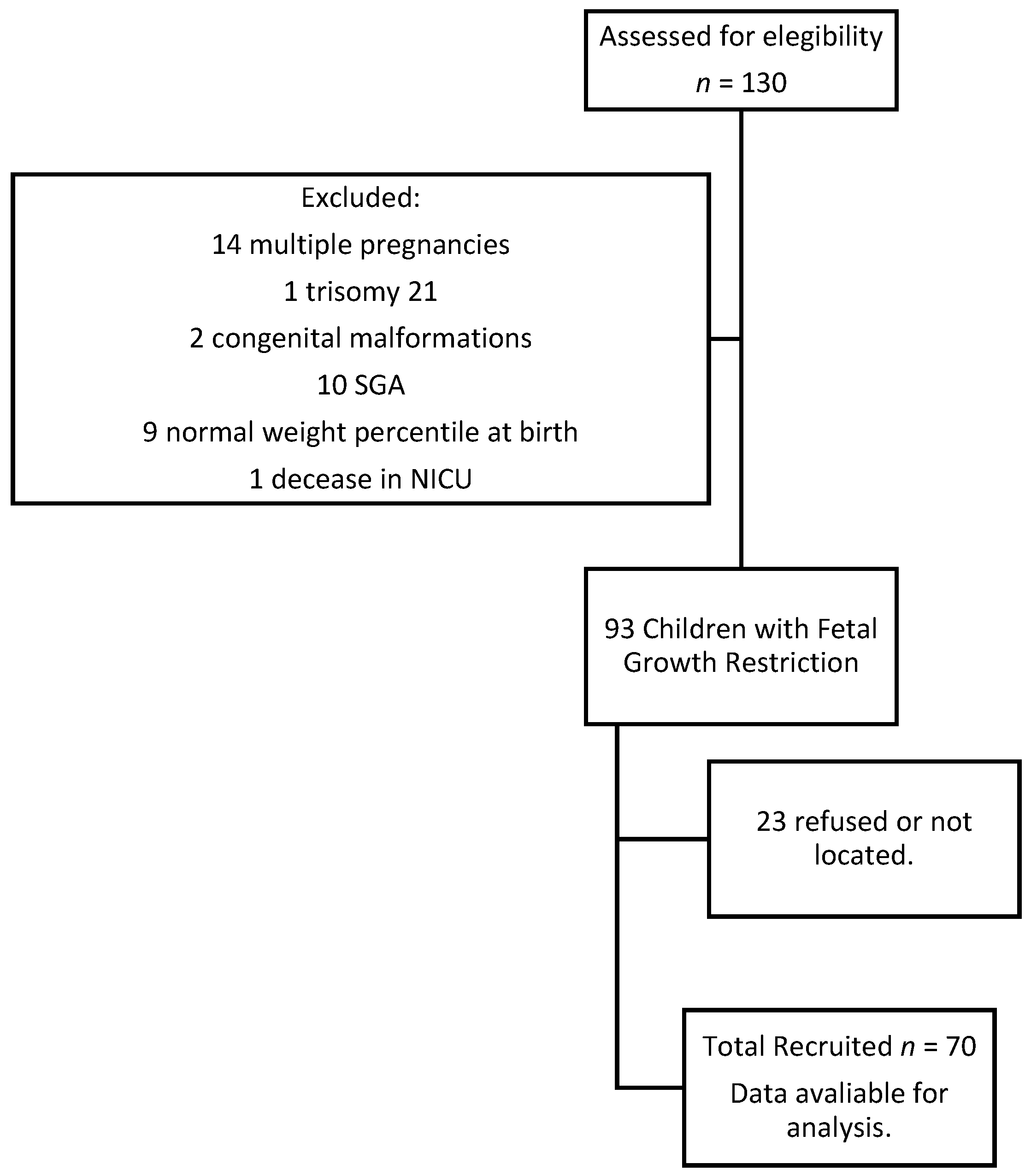
Initially, 130 patients with growth difficulties during pregnancy and born in 2015 were located in our documentary system. After applying exclusion criteria, a total of 37 children were excluded (14 multiple pregnancies, one trisomy 21, 2 congenital malformations, 10 small for gestational age, 9 children with a birth weight above the 10th percentile, and one newborn deceased during his NICU admission). Of the remaining 93 children, 70 parents agreed to carry out the neuropsychological assessment and consented to the revision of the medical records (Figure 1). Children were found to be between 70–84 months old during the evaluation. The remaining 23 children could not be assessed and BID was unavailable. Recruitment was laborious because some parents could not be located and some refused the interview due to lack of time or interest. All the cases of FGR diagnosed in our hospital that met the inclusion criteria were considered for the aim of this study. Being a single-center study no case sampling was performed. All eligible cases were thus included. Finally, we recruited seventy 6-year-old children. The group was representative of the initial population with a confidence level of 95%, a type II error of 0.6, and a statistical power of 94%.
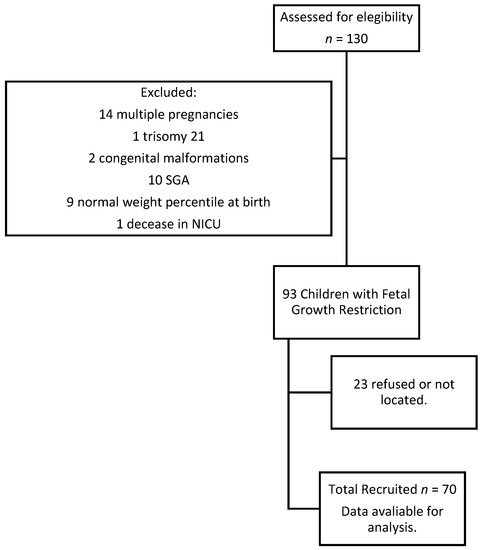
Figure 1.
Flow-diagram: Participants in the study.
3.2. Characteristics of Population Participants
Table 1 summarizes sociodemographic and delivery characteristics. The most frequent maternal and paternal educational level was secondary degree (54.3% and 51.4%). One mother and father declared no studies, but we did not reference them in the table. The most frequent socioeconomic status was medium (77.1%) and most parents were active workers. The mean gestational age at diagnosis was 33.14 weeks (SD = 4.31), with 32.9% of early-onset diagnoses. The mean fetal weight at diagnosis was 1616.38 g (SD = 660.25). The preeclampsia rate was 34.3%. In early-onset FGR, the preeclampsia rate was 60.9%, while in late-onset FGR was 21.7%. AU Doppler was registered in 65 cases, of which 20% were above the 95th percentile. In the case of MCA, only 56 were recorded and 41.4% were below the 5th percentile. CPR was calculated in 61 children, with pathological results in 50%.

Table 1.
Sociodemographic and delivery characteristics.
The mean gestational age at delivery was 35.61 (SD = 3.21) and the cesarean rate was 64.3%. Arterial blood cord pH only was registered in cesarean section deliveries and the mean was 7.27 (SD = 0.09). In 23.5% of cases, this determination was less than 7.24. The average birth weight was 1848.30 g (SD = 589.74). The mean NICU admission was 15.57 days (2–127 days). Forty-one-point-four percent of the children did not require intensive care. Table 2 summarizes adverse neonatal outcomes, being neonatal respiratory distress syndrome and neonatal sepsis were the most frequently registered. No cases of intraventricular hemorrhage, periventricular leukomalacia, or other neurological complications were recorded.
Table 2.
Adverse neonatal outcome frequencies.
3.3. Neurodevelopmental Outcome at 6 Years of Age
The average age of the children at the moment of the evaluation was 76.20-month-old (SD = 3.70). Non-major health problems or neurosensory disabilities were reported by parents, except for a child with bronchopulmonary dysplasia. Two cases of conditions encompassed within autism spectrum disorder (ASD) were disclosed. One of these children had difficulties regarding adaptative skills, and the other had poor global development. Thirty-six-point-eight percent of children needed early child support, during an average period of 3.39 years. Sixteen-point-seven percent of the children are currently following this stimulation program. Parents reported that 27.1% of children with learning disabilities.
Table 3 and Table 4 summarizes the mean quotient and the percentages of children with developmental delay in the different scales. The mean global development quotient was 97.28 (SD = 13.97). We were able to record a 57.1% of global development delay. In the cases of cognition, only 17.1% of the children registered a delay. Motor and communication skills were the most frequently affected.
Table 3.
Mean of Quotient reached in each development scale for children.
Table 4.
Percentage of children with developmental delay in each of the scales.
3.4. Bivariant Analyses
Table 5 summarizes the mean value and standard deviation for the global development quotient for each variable studied. We were able to find a higher quotient in children whose mothers had completed secondary or university studies (p < 0.05), as well as in the case of active employment status (p < 0.05). Similar results were accounted regarding the father study level and employment status but this finding did not reach the level of statistical significance. Socioeconomic status was also significantly associated with the mean of the quotient, being the case that which middle and high levels reach better quotients (p < 0.05).
Table 5.
Mean values and standard deviations of global development coefficient in each variable studied.
Early-onset FGR were linked to a lower quotient than late-onset (91.51 versus 99.92), reaching this data statistical significance (p < 0.05). When UA Doppler was studied, we found a significantly lower quotient in the cases with pathological measurement (98.30 in normal measurement versus 89.90 in pathological measurement, p < 0.05). These results were similar in the case of pathological MCA or CPR, but this did not reach statistical significance. We found a better quotient in the case of the feminine gender (p < 0.05).
Table 6 summarizes the mean and standard deviation for each variable in the subgroup of neurodevelopment delay. Lower gestational age and fetal weight at diagnosis were observed in the case of neurodevelopment delay (p < 0.001). In the same way, we found a higher UA measurement and lower MCA and CPR measurements in the neurodevelopment delay group (p < 0.05). At the moment of delivery, we found a lower mean gestational age, birth weight, length, and head circumference in the neurodevelopmental delay group with statistical significance (p < 0.001). We could not find a difference in the quotient regarding the type of delivery, arterial/venous blood cord pH, or cardiotocographic register. Although the children that received breastfeeding obtained a better quotient value, this result did not reach statistical significance.
Table 6.
Mean values and standard deviations in neurodevelopment delay subgroups.
Among the neurodevelopmental delay group, children required more days of NICU care. Table 7 summarizes the mean quotient in case of adverse neonatal outcomes. Children that underwent neonatal respiratory distress syndrome (NRDS), neonatal sepsis, or bronchopulmonary dysplasia (BPD) obtained significantly lower quotients (p < 0.05). The worst outcomes were related to children needing intubation or developed BPD. Children with other conditions achieved lower quotient values, but this result was not significant. We should notice that these were pathologies with a low incidence among the studied subject.
Table 7.
Mean values and standard deviations of global development coefficient in each neonatal outcome studied.
Table 8 summarizes the results obtained when children required early child support or had any learning disability. The poorest outcomes were accounted for in case they needed any support therapy or had academic difficulties, reaching statistical significance in case of early child support, physiotherapy support, or learning disabilities (p < 0.001). Better results were achieved when nursery school was attended (no significance).
Table 8.
Mean values and standard deviations of the global development coefficient in each childcare variable studied.
3.5. Multivariate Analyses
A linear regression analysis was performed to control the mediator factors. In the first model sociodemographic factors were included. We detected that socioeconomic status was positively related to global development quotient (F(1,62) = 9.41, p = 0.003). The R2 value was 0.132, showing that 13% of the effect is explained by differences in socioeconomic status.
The second model included Doppler variables, birthweight, and gestational age at delivery as parameters. We could find that both gestational ages at delivery and MCA pulsatility index were positively related to the global development quotient (F(2,56) = 8.45, p = 0.001). The R2 value was 0.232, so both variables could explain the 23% of the effect.
In the third model, we included postnatal variables. We were able to find that both learning disabilities and the need for early child support were negatively related to the global development quotient (F(2,58) = 15.33, p = 0.0001). These findings could be explained by higher rates of severe FGR and extreme prematurity among these children. These features make them more prone to receive early stimulation support than children with non-severe FGR or non-extreme prematurity. In the same way, they are more susceptible to academic difficulties. Table 9 sums up these models.
Table 9.
Best fit linear regression models of different variables.
4. Discussion
We performed a study to assess the neurodevelopment of children with FGR at 6 years of age. We have demonstrated higher neurodevelopment delay rates in these children. At the same time, we have proved a positive relationship between gestational age at delivery and MCA percentile with the global development quotient.
The relationship between hemodynamics disturbances, prematurity in FGR, and adverse neonatal outcomes has been well established. Assessing neurodevelopment in children with a history of FGR is more intricate. Neurodevelopment is a continuous process with different stages that can be influenced by multiple postnatal factors, both protective and risk factors. In the same way, the severity of hemodynamic alterations in FGR, as well as in prematurity, could involve a deleterious effect in the process. Our global developmental delay was 57.1%, higher than that found in other studies (close to 10–20%) [35,49,50]. This divergence could be due to different ages and methods of assessment. We evaluated the children at a late age (6 years old) by means of BDI, which assesses completely all neurodevelopment areas.
Baschat et al. (2009) found an increased risk of global retardation, cerebral palsy, and neurosensory abnormalities among FGR children with the reverse flow of the UA. They also determined that birthweight, gestational age at delivery, and neonatal adverse outcomes were strong predictors of adverse neurodevelopment [35]. In our bivariate analysis, similar results were found. A significantly lower gestational age and birth weight were found in children with developmental delays. Length of stay in the NICU was longer in children with developmental delays. We only could find a relationship between NRDS, neonatal sepsis, and BPD with worse scores in the global development coefficient. However, we could not associate perinatal outcomes with the global neurodevelopment coefficient in the multivariate analysis. This finding could be due to the low perinatal morbidity rates recorded in our study cohort.
We found that prematurity and brain sparing could be risk factors for impaired neurodevelopment. We saw a statistical association between global development quotient and gestational age at delivery and MCA pulsatility index percentile. Previous studies have related prematurity with poor neurodevelopment. In the GRIT study, the investigators evaluated the possibility of immediate or late delivery, always under safety conditions for the fetus. They found similar mortality rates in both groups. When they assessed neurodevelopment at 2 years of age, they observed comparable rates of neurodevelopment disabilities. However, when they evaluated extreme prematurity (24–30 weeks) they encountered higher rates of neurodevelopment disabilities in the immediate delivery group than in the late delivery one (13% versus 5%), as well as a poorer development quotient. A tendency to reduce morbidity and mortality in late delivery was noted [51]. When they assessed children at 6–13 years of age, they could not find differences in motor, cognitive development, or behavioral disturbances [52].
Therefore, in early-onset FGR, prematurity plays a role in neurodevelopment, mainly in psychomotor development, independently of the severity of the FGR and hemodynamic disturbances [49]. The impact on psychomotor development is more important in extreme prematurity (before 28–29 weeks of gestation) [50,53]. Besides cerebral palsy rate is between 4–18% before 32 weeks of gestational age, being higher in early prematurity [35,53]. In the same manner, Guellec et al. (2011) found a higher impact on cognitive development in FGR fetuses born before 28 weeks (37.5%) than in older fetuses. However, the result was similar to fetuses with adequate weight born before 28 weeks of gestation (38.2%). This result was non-significant [53]. Our percentage of cognitive delay was 17.1% across the entire cohort. For us, psychomotor and cognitive consequences are difficult to demonstrate because our prematurity rate before the 28th week of gestation was 2.9%.
Contrary, in late-onset FGR, gestational age is not a determinant for neurodevelopment. The DIGITAT study found that birthweight below the 2.3rd percentile is the strongest predictor for abnormal neurodevelopment in fetuses born between 36–41 weeks. They conclude that expectant management could deteriorate birthweight and neurodevelopment at 2 years of age [54].
The brain sparing effect is more controversial. Classically, brain sparing has been defined as a protective phenomenon by means of which the brain obtains nutrients and oxygen for the maintenance of its proper function. Recent studies have demonstrated the contrary. Brain sparing is a risk factor for brain development, specifically for adaptative, motor, communicative and cognitive development. Brain sparing has been related to smaller head circumferences [43] and smaller brain volume at delivery [55,56]. We could not find this relationship in our cohort, in which head circumference was similar to non-brain-sparing FGR fetuses at delivery (data not shown).
Scherjon’s group study could not relate the umbilical-cerebral ratio (UCR) with cognitive disabilities at 12 months and three years of age. However, these children had higher hyperactivity disorder rates and fewer words in their vocabulary. When children were assessed at five years of age, they could find visual potentials suggesting worse maturation profile and slower responses, as well as poor cognitive development with lower scores in intelligence quotient [41,42,43]. They only could find differences in behavior at the age of 11 [44].
Other studies have shown cognitive disturbances in brain sparing group at early ages: lower scores in habituation, motor, social interaction, and attention areas at birth [57]; poorest cognitive development at 2 years old [55] and at 3 years of age [40]. Monteith et al. (2019) could demonstrate that FGR with brain sparing resulted in lower scores in motor development tests than FGR without this condition [40].
In our systematic review, published the last year, we could connect poor intelligence quotient results to brain sparing in children with FGR. The relationship between brain sparing and motor or behavioral disabilities was difficult to assess. A good reason for that lies in methodological differences as children were assessed at different ages, when disabilities might not have yet appeared or may have already improved. On the other hand, the lack of control of the confounder could affect the results [45]. Our findings in this cohort are consistent with this trend. We have found that the MCA pulsatility index is positively related to the global development quotient.
Beukers et al. (2017) and Richter et al. (2020) could not find any association between brain sparing and cognitive development. They could not find differences in intelligence quotient either [58,59]. Specifically, the umbilico-cerebral ratio was not associated with adverse outcomes, and birth weight and sociodemographic variables seemed to take a more important role [58]. Although we reached a relationship between MCA and the global neurodevelopment quotient, our cognitive delay rate was low (17.1%).
We noted a worse quotient in those children with an AU pulsatility index above the 95th percentile. However, we could not link the AU percentile to this quotient in the multivariate analysis. This could be due to fetuses with AU pathological measurements usually being preterm, with significant deterioration. Prematurity could be more decisive for neurodevelopment than the measurement of the UA pulsatility index itself. Studies have shown controversy about this connection. Some studies determine that it is a good predictor of early neurological complications or cerebral palsy but not for adverse cognitive outcomes [37,60,61]. Other studies relate it to worse cognitive development and motor outcomes, as well as an increased rate of cerebral palsy, especially in cases where diastolic flow is absent or reversed [36,62]. We could not prove it. We only had 12 cases of absent end diastolic flow velocity in the umbilical artery. At the same time, non-cerebral palsy was found in our cohort. A larger sample size would be necessary to demonstrate an association between the measurement of UA PI and its characteristics and neurodevelopmental outcomes.
Despite the importance of fetal maturation, neurodevelopment is a complex and continuous process in which multiple factors could influence the progress. In our study, we have associated higher socioeconomic status with better global development quotients. Other studies identified a higher parental educational level [63,64] and socioeconomic status [58,65] as linked to better cognitive results. These findings could be due to higher implications and knowledge of the neurological stimulation process by parents.
On the other hand, we could not identify early stimulation in early child support as a protective factor in this group of children. Initially, we have recognized a negative association between early child support, academic disabilities, and global development quotient. These findings could be due to children attending early stimulation being a group with severe FGR and prematurity with worse results. But finally, early stimulation is a protective factor for this subgroup of children in a certain way. Other studies could identify early stimulation as a protective factor [64].
We could not relate breastfeeding as a protective factor or postpartum depression as a risk factor against other studies that succeeded to do so. Breastfeeding has been associated with better cognitive development in term and preterm infants, specifically when its use is prolonged. However, this effect is moderate when confounders are adjusted [66]. Nevertheless, breastfeeding improves neurological development, being the effect more powerful in low-birth-weight children [67] and children with lower cognitive test scores [68]. A systematic review has shown worse cognitive, language, and behavioral development in children with mothers affected by postpartum depression [69]. Postpartum depression is usually associated with worse caregiving, affecting thus neurodevelopment. Its implications for motor development are more controversial. We could not find any link between these variables and global development. Although children with breastfeeding or non-depression postpartum had better scores, this difference was minimal and non-significant. Further studies and larger sample sizes are necessary to demonstrate these associations.
5. Strengths and Limitations
Our study has some strengths. First, we assessed children at 6 years of age, when most of the motor, cognitive, and communication maturing processes are already well established. Therefore, we could accurately appraise the overall development of these children. Second, we assessed them using a complete test; the Batelle Developmental Inventory (screening test). This test allowed us to attain a global conception of the child’s development on all scales. It also allowed for considering children with disabilities, thus rendering them suitable to participate in our study. In addition, the test had a good correlation with its diagnostic modality.
Our main limitation was the sample size. Despite testing most children, a moderate number of parents were not reached or refused to participate. Although we found associations in multiple respects, we were unable to reach statistical significance. On the other hand, we could not assess a control group of children without growth restriction, to evaluate significant differences between them. Despite this, we could find a high percentage of global developmental delay. A larger sample size and a control group could be necessary to reach significance.
6. Conclusions
We found a high neurodevelopment delay rate (57.1%), specifically in motor and communicative skills. Cognitive skills have been preserved in most cases, with a low rate of delay (17.1%). Based on the results of our study, we can link gestational age at delivery and MCA percentile to the global development quotient, in the way that a higher gestational age at delivery and a higher MCA percentile is related to better quotients. Brain sparing could be a not fully protective phenomenon. In severe cases, it could surpass its protective effect becoming a harmful event for development. More studies are necessary to determine the percentile cut-off in which this effect stops being protective.
Author Contributions
Conceptualization, M.J.B.M. and E.G.M.; methodology, M.J.B.M., J.M.C., J.J.L., D.M.L.L. and E.G.M.; software, M.J.B.M.; validation, E.G.M.; formal analysis, M.J.B.M. and E.G.M.; investigation, M.J.B.M. and E.G.M.; resources, J.J.L.; data curation, M.J.B.M. and E.G.M.; writing—original draft preparation, M.J.B.M.; writing—review and editing, M.J.B.M., J.M.C., J.A.B.E. and E.G.M.; visualization, M.J.B.M., J.M.C. and E.G.M.; supervision, E.G.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of “Comité de Etica de Investigación Provincial de Málaga” (28/01/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank all of the authors included in this original paper. This research contributes to the doctoral work of M.J.B.M. We would like to thank all the participants in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Figueras, F.; Gratacós, E. Update on the Diagnosis and Classification of Fetal Growth Restriction and Proposal of a Stage-Based Management Protocol. Fetal Diagn. Ther. 2014, 36, 86–98. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.; Marlow, N.; Arabin, B.; Bilardo, C.M.; Brezinka, C.; Derks, J.B.; Duvekot, J.; Frusca, T.; Diemert, A.; Ferrazzi, E.; et al. Perinatal morbidity and mortality in early-onset fetal growth restriction: Cohort outcomes of the trial of randomized umbilical and fetal flow in Europe (TRUFFLE). Ultrasound Obstet. Gynecol. 2013, 42, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Ferrazzi, E.; Bulfamante, G.; Mezzopane, R.; Barbera, A.; Ghidini, A.; Pardi, G. Uterine Doppler Velocimetry and Placental Hypoxic-ischemic Lesion in Pregnancies with Fetal Intrauterine Growth Restriction. Placenta 1999, 20, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Crovetto, F.; Crispi, F.; Scazzocchio, E.; Mercade, I.; Meler, E.; Figueras, F.; Gratacos, E. First-trimester screening for early and late small-for-gestational-age neonates using maternal serum biochemistry, blood pressure and uterine artery Doppler. Ultrasound Obstet. Gynecol. 2014, 43, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Spinillo, A.; Gardella, B.; Bariselli, S.; Alfei, A.; Silini, E.; Dal Bello, B. Placental histopathological correlates of umbilical artery Doppler velocimetry in pregnancies complicated by fetal growth restriction. Prenat. Diagn. 2012, 32, 1263–1272. [Google Scholar] [CrossRef]
- Mifsud, W.; Sebire, N.J. Placental Pathology in Early-Onset and Late-Onset Fetal Growth Restriction. Fetal Diagn. Ther. 2014, 36, 117–128. [Google Scholar] [CrossRef]
- Figueras, F.; Caradeux, J.; Crispi, F.; Eixarch, E.; Peguero, A.; Gratacos, E. Diagnosis and surveillance of late-onset fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S790–S802.e1. [Google Scholar] [CrossRef]
- Oros, D.; Figueras, F.; Cruz-Martinez, R.; Meler, E.; Munmany, M.; Gratacos, E. Longitudinal changes in uterine, umbilical and fetal cerebral Doppler indices in late-onset small-for-gestational age fetuses. Ultrasound Obstet. Gynecol. 2011, 37, 191–195. [Google Scholar] [CrossRef]
- Simeoni, U.; Armengaud, J.-B.; Siddeek, B.; Tolsa, J.-F. Perinatal Origins of Adult Disease. Neonatology 2018, 113, 393–399. [Google Scholar] [CrossRef]
- Arpino, C.; Compagnone, E.; Montanaro, M.L.; Cacciatore, D.; De Luca, A.; Cerulli, A.; Di Girolamo, S.; Curatolo, P. Preterm birth and neurodevelopmental outcome: A review. Childs Nerv. Syst. 2010, 26, 1139–1149. [Google Scholar] [CrossRef]
- Mallard, C.; Loeliger, M.; Copolov, D.; Rees, S. Reduced number of neurons in the hippocampus and the cerebellum in the postnatal guinea-pig following intrauterine growth-restriction. Neuroscience 2000, 100, 327–333. [Google Scholar] [CrossRef]
- Dieni, S.; Rees, S. Dendritic morphology is altered in hippocampal neurons following prenatal compromise. J. Neurobiol. 2003, 55, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Eixarch, E.; Batalle, D.; Illa, M.; Muñoz-Moreno, E.; Arbat-Plana, A.; Amat-Roldan, I.; Figueras, F.; Gratacos, E. Neonatal Neurobehavior and Diffusion MRI Changes in Brain Reorganization Due to Intrauterine Growth Restriction in a Rabbit Model. PLoS ONE 2012, 7, e31497. [Google Scholar] [CrossRef]
- Tolcos, M.; Bateman, E.; O’Dowd, R.; Markwick, R.; Vrijsen, K.; Rehn, A.; Rees, S. Intrauterine growth restriction affects the maturation of myelin. Exp. Neurol. 2011, 232, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Andrade, E.; Cortés-Camberos, A.J.; Díaz, N.F.; Flores-Herrera, H.; García-López, G.; González-Jiménez, M.; Santamaría, A.; Molina-Hernández, A. Altered levels of brain neurotransmitter from new born rabbits with intrauterine restriction. Neurosci. Lett. 2015, 584, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Simões, R.V.; Muñoz-Moreno, E.; Carbajo, R.J.; González-Tendero, A.; Illa, M.; Sanz-Cortés, M.; Pineda-Lucena, A.; Gratacós, E. In Vivo Detection of Perinatal Brain Metabolite Changes in a Rabbit Model of Intrauterine Growth Restriction (IUGR). PLoS ONE 2015, 10, e0131310. [Google Scholar] [CrossRef] [PubMed]
- van Vliet, E.; Eixarch, E.; Illa, M.; Arbat-Plana, A.; González-Tendero, A.; Hogberg, H.T.; Zhao, L.; Hartung, T.; Gratacos, E. Metabolomics Reveals Metabolic Alterations by Intrauterine Growth Restriction in the Fetal Rabbit Brain. PLoS ONE 2013, 8, e64545. [Google Scholar]
- Tolsa, C.B.; Zimine, S.; Warfield, S.K.; Freschi, M.; Rossignol, A.S.; Lazeyras, F.; Hanquinet, S.; Pfizenmaier, M.; Hüppi, P.S. Early Alteration of Structural and Functional Brain Development in Premature Infants Born with Intrauterine Growth Restriction. Pediatr. Res. 2004, 56, 132–138. [Google Scholar] [CrossRef]
- Padilla, N.; Perapoch, J.; Carrascosa, A.; Acosta-Rojas, R.; Botet, F.; Gratacós, E. Twelve-month neurodevelopmental outcome in preterm infants with and without intrauterine growth restriction. Acta Paediatr. 2010, 99, 1498–1503. [Google Scholar] [CrossRef]
- Samuelsen, G.B.; Pakkenberg, B.; Bogdanović, N.; Gundersen, H.J.G.; Larsen, J.F.; Græm, N.; Laursen, H. Severe cell reduction in the future brain cortex in human growth–restricted fetuses and infants. Am. J. Obstet. Gynecol. 2007, 197, e1–e56. [Google Scholar] [CrossRef]
- Bruno, C.J.; Bengani, S.; Gomes, W.A.; Brewer, M.; Vega, M.; Xie, X.; Kim, M.; Fuloria, M. MRI Differences Associated with Intrauterine Growth Restriction in Preterm Infants. Neonatology 2017, 111, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Lodygensky, G.A.; Seghier, M.L.; Warfield, S.K.; Tolsa, C.B.; Sizonenko, S.; Lazeyras, F.; Hüppi, P.S. Intrauterine Growth Restriction Affects the Preterm Infant’s Hippocampus. Pediatr. Res. 2008, 63, 438–443. [Google Scholar] [CrossRef]
- Fischi-Gómez, E.; Vasung, L.; Meskaldji, D.-E.; Lazeyras, F.; Borradori-Tolsa, C.; Hagmann, P.; Barisnikov, K.; Thiran, J.-P.; Hüppi, P.S. Structural Brain Connectivity in School-Age Preterm Infants Provides Evidence for Impaired Networks Relevant for Higher Order Cognitive Skills and Social Cognition. Cereb. Cortex 2015, 25, 2793–2805. [Google Scholar] [CrossRef] [PubMed]
- Padilla, N.; Junqué, C.; Figueras, F.; Sanz-Cortes, M.; Bargalló, N.; Arranz, A.; Donaire, A.; Figueras, J.; Gratacos, E. Differential vulnerability of gray matter and white matter to intrauterine growth restriction in preterm infants at 12 months corrected age. Brain Res. 2014, 1545, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dubois, J.; Benders, M.; Borradori-Tolsa, C.; Cachia, A.; Lazeyras, F.; Ha-Vinh Leuchter, R.; Sizonenko, S.V.; Warfield, S.K.; Mangin, J.F.; Hüppi, P.S. Primary cortical folding in the human newborn: An early marker of later functional development. Brain 2008, 131, 2028–2041. [Google Scholar] [CrossRef]
- Geva, R.; Eshel, R.; Leitner, Y.; Fattal-Valevski, A.; Harel, S. Memory functions of children born with asymmetric intrauterine growth restriction. Brain Res. 2006, 1117, 186–194. [Google Scholar] [CrossRef]
- Geva, R.; Eshel, R.; Leitner, Y.; Valevski, A.F.; Harel, S. Neuropsychological Outcome of Children With Intrauterine Growth Restriction: A 9-Year Prospective Study. Pediatrics 2006, 118, 91–100. [Google Scholar] [CrossRef]
- Korzeniewski, S.J.; Allred, E.N.; Joseph, R.M.; Heeren, T.; Kuban, K.C.K.; O’Shea, T.M.; Leviton, A. Neurodevelopment at Age 10 Years of Children Born <28 Weeks With Fetal Growth Restriction. Pediatrics 2017, 140, e20170697. [Google Scholar]
- Morsing, E.; Åsard, M.; Ley, D.; Stjernqvist, K.; Maršál, K. Cognitive Function After Intrauterine Growth Restriction and Very Preterm Birth. Pediatrics 2011, 127, e874–e882. [Google Scholar] [CrossRef]
- Kulseng, S.; Jennekens-Schinkel, A.; Naess, P.; Romundstad, P.; Indredavik, M.; Vik, T.; Brubakk, A.-M. Very-low-birthweight and term small-for-gestational-age adolescents: Attention revisited. Acta Paediatr. 2007, 95, 224–230. [Google Scholar] [CrossRef]
- Paz, I.; Gale, R.; Laor, A.; Danon, Y.; Stevenson, D.; Seidman, D. The cognitive outcome of full-term small for gestational age infants at late adolescence. Obstet. Gynecol. 1995, 85, 452–456. [Google Scholar] [PubMed]
- Paz, I.; Laor, A.; Gale, R.; Harlap, S.; Stevenson, D.K.; Seidman, D.S. Term infants with fetal growth restriction are not at increased risk for low intelligence scores at age 17 years. J. Pediatr. 2001, 138, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Sommerfelt, K. Cognitive development of term small for gestational age children at five years of age. Arch. Dis. Child. 2000, 83, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Theodore, R.F.; Thompson, J.M.D.; Waldie, K.E.; Becroft, D.M.O.; Robinson, E.; Wild, C.J.; Clark, P.M.; Mitchell, E.A. Determinants of cognitive ability at 7 years: A longitudinal case–control study of children born small-for-gestational age at term. Eur. J. Pediatr. 2009, 168, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Baschat, A.A.; Viscardi, R.M.; Hussey-Gardner, B.; Hashmi, N.; Harman, C. Infant neurodevelopment following fetal growth restriction: Relationship with antepartum surveillance parameters. Ultrasound Obstet. Gynecol. 2009, 33, 44–50. [Google Scholar] [CrossRef]
- Schreuder, A.M. Outcome at school age following antenatal detection of absent or reversed end diastolic flow velocity in the umbilical artery. Arch. Dis. Child.-Fetal Neonatal Ed. 2002, 86, F108–F114. [Google Scholar] [CrossRef] [PubMed]
- Valcamonico, A.; Accorsi, P.; Battaglia, S.; Soregaroli, M.; Beretta, D.; Frusca, T. Absent or reverse end-diastolic flow in the umbilical artery: Intellectual development at school age. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 114, 23–28. [Google Scholar] [CrossRef]
- Cruz-Martinez, R.; Figueras, F.; Oros, D.; Padilla, N.; Meler, E.; Hernandez-Andrade, E.; Gratacos, E. Cerebral blood perfusion and neurobehavioral performance in full-term small-for-gestational-age fetuses. Am. J. Obstet. Gynecol. 2009, 201, 474.e1–474.e7. [Google Scholar] [CrossRef]
- Eixarch, E.; Meler, E.; Iraola, A.; Illa, M.; Crispi, F.; Hernandez-Andrade, E.; Gratacos, E.; Figueras, F. Neurodevelopmental outcome in 2-year-old infants who were small-for-gestational age term fetuses with cerebral blood flow redistribution. Ultrasound Obstet. Gynecol. 2008, 32, 894–899. [Google Scholar] [CrossRef]
- Monteith, C.; Flood, K.; Pinnamaneni, R.; Levine, T.A.; Alderdice, F.A.; Unterscheider, J.; McAuliffe, F.M.; Dicker, P.; Tully, E.C.; Malone, F.D.; et al. An abnormal cerebroplacental ratio (CPR) is predictive of early childhood delayed neurodevelopment in the setting of fetal growth restriction. Am. J. Obstet. Gynecol. 2019, 221, 273.e1–273.e9. [Google Scholar] [CrossRef]
- Scherjon, S.; Briet, J.; Oosting, H.; Kok, J. The Discrepancy Between Maturation of Visual-Evoked Potentials and Cognitive Outcome at Five Years in Very Preterm Infants With and Without Hemodynamic Signs of Fetal Brain-Sparing. Pediatrics 2000, 105, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Scherjon, S.A.; Oosting, H.; Smolders-DeHaas, H.; Zondervan, H.A.; Kok, J.H. Neurodevelopmental outcome at three years of age after fetal ‘brain-sparing’. Early Hum. Dev. 1998, 52, 67–79. [Google Scholar] [CrossRef]
- Scherjon, S.A.; Smolders-DeHaas, H.; Kok, J.H.; Zondervan, H.A. The “brain-sparing” effect: Antenatal cerebral Doppler findings in relation to neurologic outcome in very preterm infants. Am. J. Obstet. Gynecol. 1993, 169, 169–175. [Google Scholar] [CrossRef]
- van den Broek, A.J.M.; Kok, J.H.; Houtzager, B.A.; Scherjon, S.A. Behavioural problems at the age of eleven years in preterm-born children with or without fetal brain sparing: A prospective cohort study. Early Hum. Dev. 2010, 86, 379–384. [Google Scholar] [CrossRef]
- Benítez-Marín, M.J.; Marín-Clavijo, J.; Blanco-Elena, J.A.; Jiménez-López, J.; González-Mesa, E. Brain Sparing Effect on Neurodevelopment in Children with Intrauterine Growth Restriction: A Systematic Review. Children 2021, 8, 745. [Google Scholar] [CrossRef]
- Newborg, J.; Guidubaldi, J.; Wnek, L.; Svinicki, J.; Stock, J.R.; de la Cruz López, M.V.; Criado, M.G. Battelle: Inventario del Desarrollo, 2nd ed.; TEA: Madrid, Spain, 2009. [Google Scholar]
- Moraleda-Barreno, E.; Romero-López, M.; Cayetano-Menéndez, M.J. La prueba de cribado del inventario de desarrollo de Battelle para la detección precoz de alteraciones del desarrollo en parálisis cerebral. An. Pediatría 2011, 75, 372–379. [Google Scholar] [CrossRef]
- González-Valenzuela, M.J.; García-Fortea, P.; Delgado-Ríos, M.; Cazorla-Granados, O.; Blasco-Alonso, M.; González-Mesa, E. Effects of oxytocin used during delivery on development: A retrospective cohort study. J. Clin. Exp. Neuropsychol. 2014, 36, 680–690. [Google Scholar] [CrossRef]
- Stampalija, T.; Arabin, B.; Wolf, H.; Bilardo, C.M.; Lees, C.; Brezinka, C.; Derks, J.B.; Diemert, A.; Duvekot, J.J.; Ferrazzi, E.; et al. Is middle cerebral artery Doppler related to neonatal and 2-year infant outcome in early fetal growth restriction? Am. J. Obstet. Gynecol. 2017, 216, 521.e1–521.e13. [Google Scholar] [CrossRef]
- Torrance, H.L.; Bloemen, M.C.T.; Mulder, E.J.H.; Nikkels, P.G.J.; Derks, J.B.; De Vries, L.S.; Visser, G.H.A. Predictors of outcome at 2 years of age after early intrauterine growth restriction. Ultrasound Obstet. Gynecol. 2010, 36, 171–177. [Google Scholar] [CrossRef]
- GRIT Study Group. Infant wellbeing at 2 years of age in the Growth Restriction Intervention Trial (GRIT): Multicentred randomised controlled trial. Lancet 2004, 364, 513–520. [Google Scholar] [CrossRef]
- Walker, D.-M.; Marlow, N.; Upstone, L.; Gross, H.; Hornbuckle, J.; Vail, A.; Wolke, D.; Thornton, J.G. The Growth Restriction Intervention Trial: Long-term outcomes in a randomized trial of timing of delivery in fetal growth restriction. Am. J. Obstet. Gynecol. 2011, 204, 34.e1–34.e9. [Google Scholar] [CrossRef] [PubMed]
- Guellec, I.; Lapillonne, A.; Renolleau, S.; Charlaluk, M.-L.; Roze, J.-C.; Marret, S.; Vieux, R.; Monique, K.; Ancel, P.-Y. Neurologic Outcomes at School Age in Very Preterm Infants Born With Severe or Mild Growth Restriction. Pediatrics 2011, 127, e883–e891. [Google Scholar] [CrossRef] [PubMed]
- van Wyk, L.; Boers, K.E.; van der Post, J.A.M.; van Pampus, M.G.; van Wassenaer, A.G.; van Baar, A.L.; Spaanderdam, M.E.A.; Becker, J.H.; Kwee, A.; Duvekot, J.J.; et al. Effects on (neuro)developmental and behavioral outcome at 2 years of age of induced labor compared with expectant management in intrauterine growth-restricted infants: Long-term outcomes of the DIGITAT trial. Am. J. Obstet. Gynecol. 2012, 206, 406.e1–406.e7. [Google Scholar] [CrossRef] [PubMed]
- Leppänen, M.; Ekholm, E.; Palo, P.; Maunu, J.; Munck, P.; Parkkola, R.; Matomäki, J.; Lapinleimu, H.; Haataja, L.; Lehtonen, L.; et al. Abnormal antenatal Doppler velocimetry and cognitive outcome in very-low-birth-weight infants at 2 years of age. Ultrasound Obstet. Gynecol. 2009, 36, 178–185. [Google Scholar] [CrossRef]
- Maunu, J.; Ekholm, E.; Parkkola, R.; Palo, P.; Rikalainen, H.; Lapinleimu, H.; Haataja, L.; Lehtonen, L. Antenatal Doppler Measurements and Early Brain Injury in Very Low Birth Weight Infants. J. Pediatr. 2007, 150, 51–56.e1. [Google Scholar]
- Figueras, F.; Cruz-Martinez, R.; Sanz-Cortes, M.; Arranz, A.; Illa, M.; Botet, F.; Costas-Moragas, C.; Gratacos, E. Neurobehavioral outcomes in preterm, growth-restricted infants with and without prenatal advanced signs of brain-sparing. Ultrasound Obstet. Gynecol. 2011, 38, 288–294. [Google Scholar] [CrossRef]
- Beukers, F.; Aarnoudse-Moens, C.S.H.; van Weissenbruch, M.M.; Ganzevoort, W.; van Goudoever, J.B.; van Wassenaer-Leemhuis, A.G. Fetal Growth Restriction with Brain Sparing: Neurocognitive and Behavioral Outcomes at 12 Years of Age. J. Pediatr. 2017, 188, 103–109.e2. [Google Scholar] [CrossRef]
- Richter, A.E.; Salavati, S.; Kooi, E.M.W.; den Heijer, A.E.; Foreman, A.B.; Schoots, M.H.; Bilardo, C.M.; Scherjon, S.A.; Tanis, J.C.; Bos, A.F. Fetal Brain-Sparing, Postnatal Cerebral Oxygenation, and Neurodevelopment at 4 Years of Age Following Fetal Growth Restriction. Front. Pediatr. 2020, 8, 225. [Google Scholar] [CrossRef]
- Eger, S.H.W.; Sommerfelt, K.; Kiserud, T.; Markestad, T. Foetal umbilical artery Doppler in small preterms: (IQ) Neurocognitive outcome at 5 years of age. Acta Paediatr. 2013, 102, 403–409. [Google Scholar] [CrossRef]
- Kirsten, G.F.; van Zyl, J.I.; van Zijl, F.; Maritz, J.S.; Odendaal, H.J. Infants of Women With Severe Early Pre-Eclampsia: The Effect of Absent End-Diastolic Umbilical Artery Doppler Flow Velocities on Neurodevelopmental Outcome. Obstet. Gynecol. Surv. 2001, 56, 124–125. [Google Scholar] [CrossRef]
- Voßbeck, S.; de Camargo, O.K.; Grab, D.; Bode, H.; Pohlandt, F. Neonatal and neurodevelopmental outcome in infants born before 30 weeks of gestation with absent or reversed end-diastolic flow velocities in the umbilical artery. Eur. J. Pediatr. 2001, 160, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Aarnoudse-Moens, C.S.H.; Weisglas-Kuperus, N.; van Goudoever, J.B.; Oosterlaan, J. Meta-Analysis of Neurobehavioral Outcomes in Very Preterm and/or Very Low Birth Weight Children. Pediatrics 2009, 124, 717–728. [Google Scholar] [CrossRef] [PubMed]
- Candel Pau, J.; Perapoch López, J.; Castillo Salinas, F.; Sánchez Garcia, O.; Pérez Hoyos, S.; Llurba Olivé, E. Neurodevelopment in preterm infants with and without placenta-related intrauterine growth restriction and its relation to perinatal and postnatal factors. J. Matern. Neonatal Med. 2016, 29, 2268–2274. [Google Scholar] [CrossRef] [PubMed]
- González, L.; Cortés-Sancho, R.; Murcia, M.; Ballester, F.; Rebagliato, M.; Rodríguez-Bernal, C.L. The role of parental social class, education and unemployment on child cognitive development. Gac. Sanit. 2020, 34, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.A.; Hockley, C.; Carson, C.; Kelly, Y.; Renfrew, M.J.; Sacker, A. Breastfeeding is Associated with Improved Child Cognitive Development: A Population-Based Cohort Study. J. Pediatr. 2012, 160, 25–32. [Google Scholar] [CrossRef]
- Anderson, J.W.; Johnstone, B.M.; Remley, D.T. Breast-feeding and cognitive development: A meta-analysis. Am. J. Clin. Nutr. 1999, 70, 525–535. [Google Scholar] [CrossRef]
- Koh, K. Maternal breastfeeding and children’s cognitive development. Soc. Sci. Med. 2017, 187, 101–108. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.-Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Womens Health 2019, 15, 174550651984404. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).