
Evolution of Medical Students’ Perception of the Patient’s Right to Privacy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. Gathered Information
2.3. Ethical Issues
2.4. Statistical Analysis
3. Results
3.1. Students’ Experience When Rotating in Hospital
3.2. Students’ Opinion
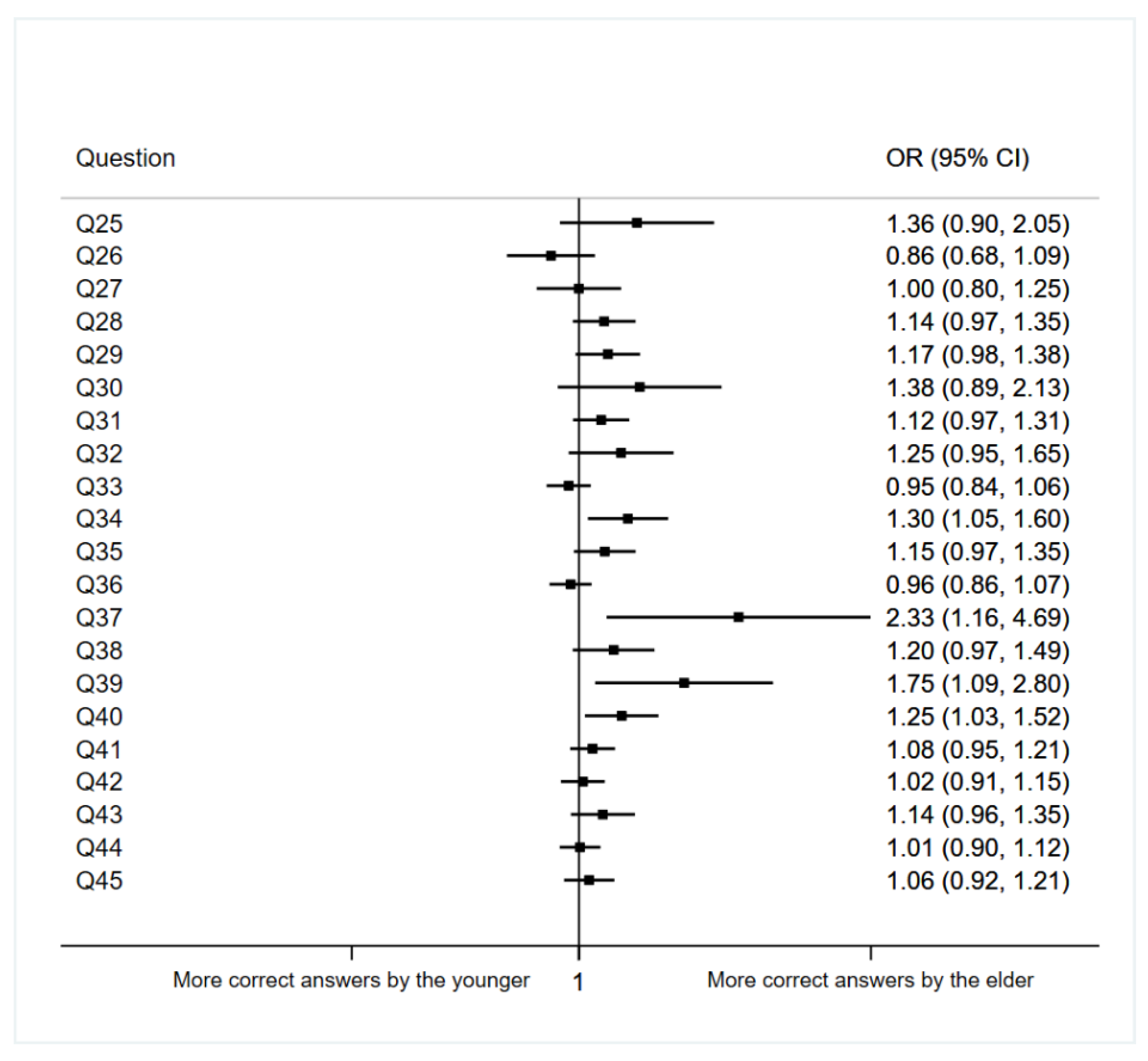
3.3. Association between Age and Knowledge about Ethical Issues
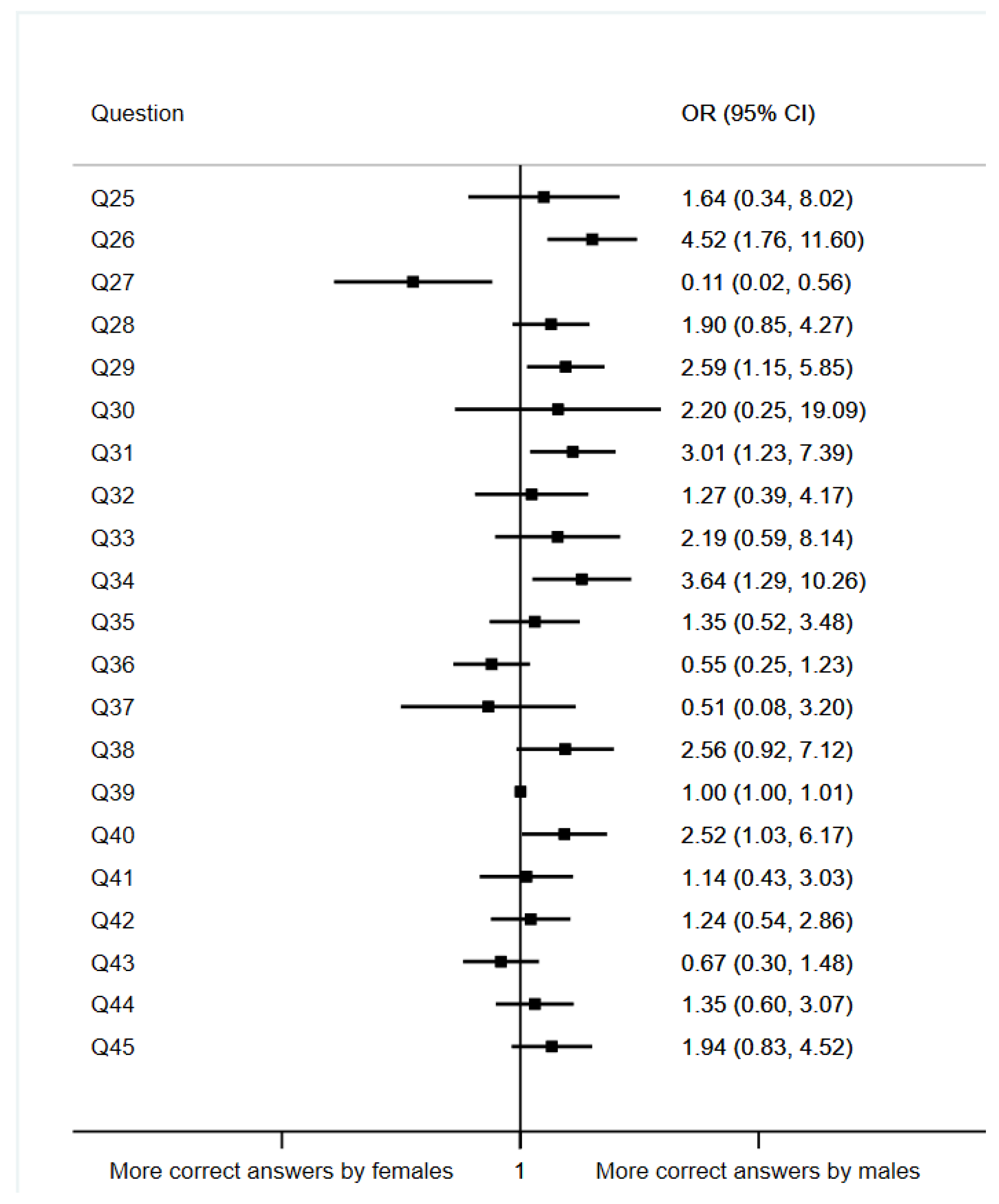
3.4. Association between Sex and Knowledge about Ethical Issues
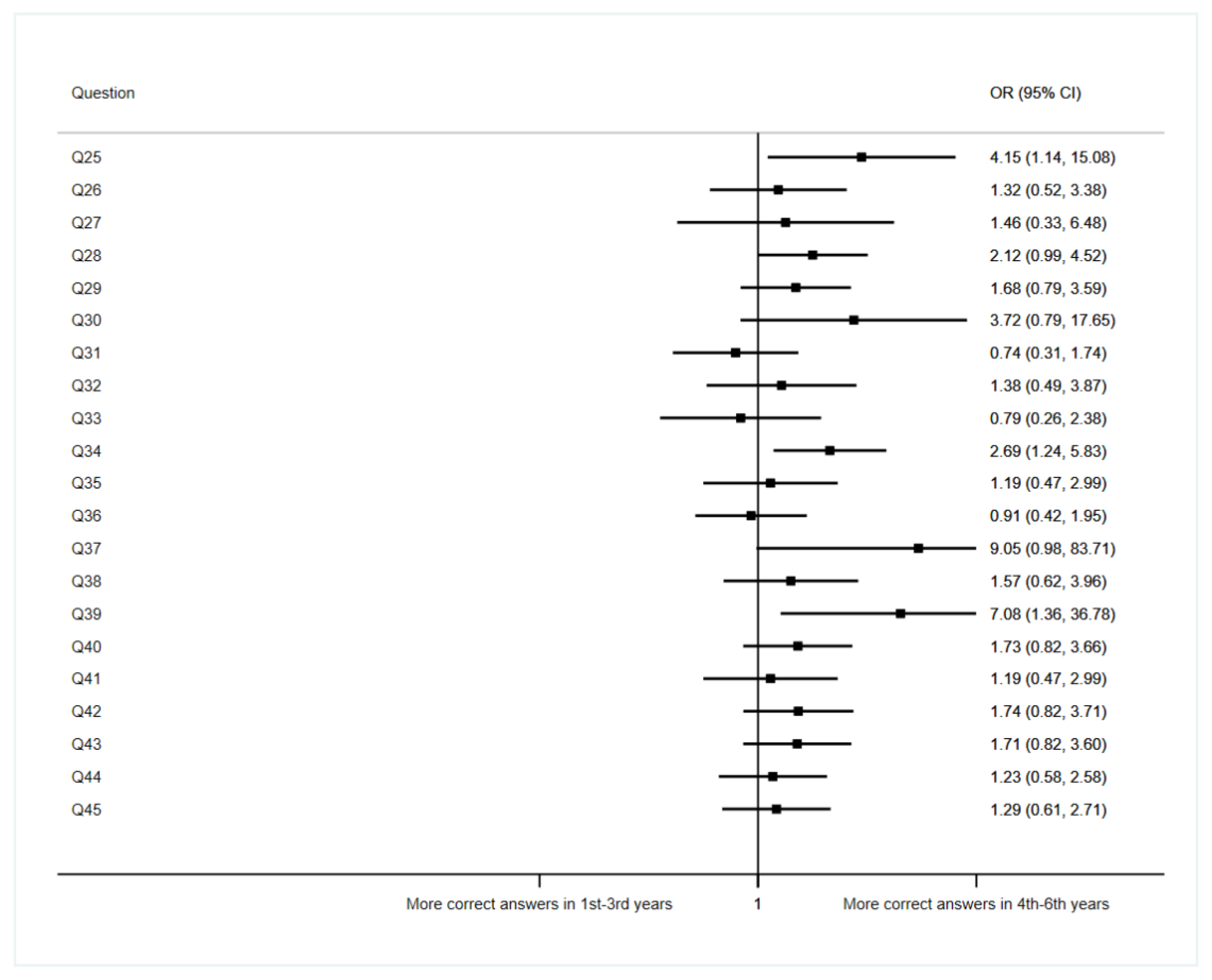
3.5. Association between Academic Year and Knowledge about Ethical Issues
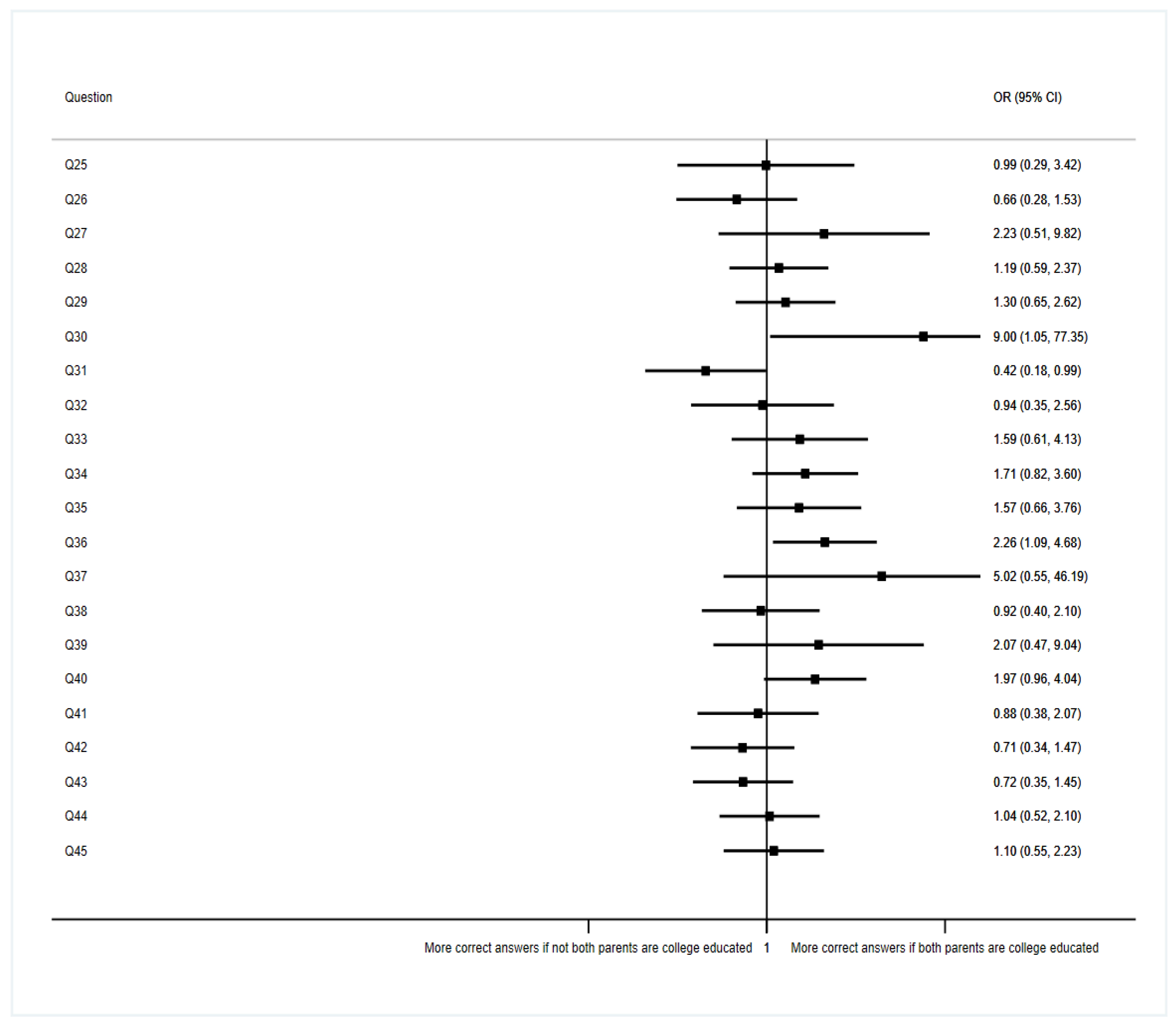
3.6. Association between Parents’ Educational Level and Knowledge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Véliz, C. Not the Doctor’s Business: Privacy, Personal Responsibility and Data Rights in Medical Settings. Bioethics 2020, 34, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.K.; Bhatia, A.C.; Callen, J.P. Protection of Patients’ Right to Privacy in Clinical Photographs, Video, and Detailed Case Descriptions. JAMA Dermatol. 2014, 150, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Beltran-Aroca, C.M.; Labella, F.; Font-Ugalde, P.; Girela-Lopez, E. Assessment of Doctors’ Knowledge and Attitudes Towards Confidentiality in Hospital Care. Sci. Eng. Ethics 2019, 25, 1531–1548. [Google Scholar] [CrossRef] [PubMed]
- Winton, R. The Declaration of Lisbon: Patients Have Rights, Too. Med. J. Aust. 1982, 1, 101. [Google Scholar] [CrossRef]
- Ramos-Brieva, J. Respect the privacy of the patient: The feminization of Medicine requires a paradigm shif. J. Healthc. Qual. Res. 2019, 34, 275–276. [Google Scholar] [CrossRef]
- Jefatura del Estado. Ley Orgánica 10/1995, de 23 de Noviembre, Del Código Penal; 1995; Volume BOE-A-1995-25444, pp. 33987–34058. Available online: https://www.boe.es/eli/es/lo/1995/11/23/10/con (accessed on 20 July 2022).
- Rosagemma, C.; Ilaria, B.; Fabio, G.; Sara, P.; Francesco, D.S.; Alessandro, B. Physicians’ Perception of the Importance of Ethical and Deontological Issues in a Major Italian Province: Pilot Questionnaire and Its Validation. Acta Biomed. 2019, 90, 56–67. [Google Scholar] [CrossRef]
- Kapp, M.; Turner, G.; Baker, D. Medicine, Law, Ethics: Teaching versus Learning. Clin. Teach. 2012, 9, 338–342. [Google Scholar] [CrossRef]
- Faulk, C.E.; Mali, J.; Mendoza, P.M.; Musick, D.; Sembrano, R. Impact of a Required Fourth-Year Medical Student Rotation in Physical Medicine and Rehabilitation. Am. J. Phys. Med. Rehabil. 2012, 91, 442–448. [Google Scholar] [CrossRef]
- Yilmaz, N.D.; Velipasaoglu, S.; Ozan, S.; Basusta, B.U.; Midik, O.; Mamakli, S.; Karaoglu, N.; Tengiz, F.; Durak, H.İ.; Sahin, H. A Multicenter Study: How Do Medical Students Perceive Clinical Learning Climate? Med. Educ. Online 2016, 21, 30846. [Google Scholar] [CrossRef]
- Kandiah, D.A. Perception of Educational Value in Clinical Rotations by Medical Students. Adv. Med. Educ. Pract. 2017, 8, 149–162. [Google Scholar] [CrossRef] [Green Version]
- Hassidim, A.; Korach, T.; Shreberk-Hassidim, R.; Thomaidou, E.; Uzefovsky, F.; Ayal, S.; Ariely, D. Prevalence of Sharing Access Credentials in Electronic Medical Records. Healthc. Inform. Res. 2017, 23, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Zucco, L.; Desmond, G.; Carpenter, B. Identity Cards Help Patients Identify Their Doctors. BMJ Qual. Improv. Rep. 2014, 2, u539.w574. [Google Scholar] [CrossRef] [PubMed]
- Coleman, D.; McLaughlin, D. Using Simulated Patients as a Learning Strategy to Support Undergraduate Nurses to Develop Patient-Teaching Skills. Br. J. Nurs. 2019, 28, 1300–1306. [Google Scholar] [CrossRef] [PubMed]
- Hishikawa, S.; Kawano, M.; Tanaka, H.; Konno, K.; Yasuda, Y.; Kawano, R.; Kobayashi, E.; Lefor, A.T. Mannequin Simulation Improves the Confidence of Medical Students Performing Tube Thoracostomy: A Prospective, Controlled Trial. Am. Surg. 2010, 76, 73–78. [Google Scholar] [CrossRef]
- Lavanya, S.H.; Kalpana, L.; Veena, R.M.; Bharath Kumar, V.D. Role-Play as an Educational Tool in Medication Communication Skills: Students’ Perspectives. Indian J. Pharmacol. 2016, 48, S33–S36. [Google Scholar] [CrossRef] [PubMed]
- Nair, B.T. Role Play–An Effective Tool to Teach Communication Skills in Pediatrics to Medical Undergraduates. J. Educ. Health Promot. 2019, 8, 18. [Google Scholar] [CrossRef]
- Rønning, S.B.; Bjørkly, S. The Use of Clinical Role-Play and Reflection in Learning Therapeutic Communication Skills in Mental Health Education: An Integrative Review. Adv. Med. Educ. Pract. 2019, 10, 415–425. [Google Scholar] [CrossRef]
- Malpas, P.J.; Bagg, W.; Yielder, J.; Merry, A.F. Medical Students, Sensitive Examinations and Patient Consent: A Qualitative Review. N. Z. Med. J. 2018, 131, 29–37. [Google Scholar]
- Campbell, A.T. Teaching Law in Medical Schools: First, Reflect. J. Law Med. Ethics 2012, 40, 301–310. [Google Scholar] [CrossRef]
- Parker, M.; Willmott, L.; White, B.; Williams, G.; Cartwright, C. Medical Education and Law: Withholding/Withdrawing Treatment from Adults without Capacity. Intern. Med. J. 2015, 45, 634–640. [Google Scholar] [CrossRef]
- Wong, R.S.Y.; Balasingam, U. Teaching Medical Law in Medical Education. J. Acad. Ethics 2013, 11, 121–138. [Google Scholar] [CrossRef]
- Mou, D.; Sarma, A.; Sethi, R.; Merryman, R. The State of Health Policy Education in U.S. Medical Schools. N. Engl. J. Med. 2011, 364, e19. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.S.; Davis, M.M.; Lypson, M.L. Advancing Medical Education by Teaching Health Policy. N. Engl. J. Med. 2011, 364, 695–697. [Google Scholar] [CrossRef] [PubMed]
- Backović, D.V.; Zivojinović, J.I.; Maksimović, J.; Maksimović, M. Gender Differences in Academic Stress and Burnout among Medical Students in Final Years of Education. Psychiatr. Danub. 2012, 24, 175–181. [Google Scholar]
- Gao, W.; Ping, S.; Liu, X. Gender Differences in Depression, Anxiety, and Stress among College Students: A Longitudinal Study from China. J. Affect. Disord. 2020, 263, 292–300. [Google Scholar] [CrossRef]
- Van Wyk, J.M.; Naidoo, S.S.; Moodley, K.; Higgins-Opitz, S.B. Perceptions of Final-Year Medical Students towards the Impact of Gender on Their Training and Future Practice. Adv. Med. Educ. Pract. 2016, 7, 541–550. [Google Scholar] [CrossRef]
- Faisal, R.; Shinwari, L.; Hussain, S.S. Academic Performance of Male in Comparison with Female Undergraduate Medical Students in Pharmacology Examinations. J. Pak. Med. Assoc. 2017, 67, 204–208. [Google Scholar]
- O’Dea, R.E.; Lagisz, M.; Jennions, M.D.; Nakagawa, S. Gender Differences in Individual Variation in Academic Grades Fail to Fit Expected Patterns for STEM. Nat. Commun. 2018, 9, 3777. [Google Scholar] [CrossRef]
- Fadem, B.; Schuchman, M.; Simring, S.S. The Relationship between Parental Income and Academic Performance of Medical Students. Acad. Med. 1995, 70, 1142–1144. [Google Scholar] [CrossRef]
- Fan, A.P.C.; Chen, C.-H.; Su, T.-P.; Shih, W.-J.; Lee, C.-H.; Hou, S.-M. The Association between Parental Socioeconomic Status (SES) and Medical Students’ Personal and Professional Development. Ann. Acad. Med. Singap. 2007, 36, 735–742. [Google Scholar]
- Padilla-Moledo, C.; Ruiz, J.R.; Castro-Piñero, J. Parental Educational Level and Psychological Positive Health and Health Complaints in Spanish Children and Adolescents. Child Care Health Dev. 2016, 42, 534–543. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Total |
|---|---|---|
| Age (years) mean ± standard deviation | 22.1 ± 3.5 | |
| Gender | Man | 33 (25.6) |
| Woman | 94 (72.9) | |
| NA | 2 (1.5) | |
| Parents with college education | Not both parents college-educated | 59 (45.7) |
| Both parents college-educated | 70 (54.3) | |
| Current academic year | From 1st to 3rd | 42 (32.6) |
| From 4th to 6th | 87 (67.4) | |
| Subjects from previous academic years | No | 102 (79) |
| Yes | 27 (21) | |
| Current average grade * | 5–6.9 | 29 (22.5) |
| 7–8.9 | 83 (64.3) | |
| ≥9 | 6 (4.7) | |
| NA | 11 (8.5) | |
| Number of hospital services the student has rotated at | 0 services | 21 (16.3) |
| From 1 to 9 services | 82 (63.6) | |
| 10 or more services | 26 (20.1) | |
| Question | Statements | Category | Number of Students from 3rd to 6th Year |
|---|---|---|---|
| Q1 | During my clinical rotation, I am constantly supervised and accompanied by my doctor. | Rarely | 2 (1.9) |
| Sometimes | 18 (16.7) | ||
| Quite often | 57 (52.8) | ||
| Always | 29 (26.9) | ||
| N/A | 2 (1.9) | ||
| Q2 | At the beginning of my rotations, I signed a confidentiality commitment provided by the health center where I carry out the practice. | No | 65 (60.2) |
| Yes | 33 (30.6) | ||
| N/A | 10 (9.3) | ||
| Q3 | During my clinical rotation, the doctor provides me his/her username and password for the hospital’s intranet. | Always | 2 (1.9) |
| Quite often | 1 (0.9) | ||
| Sometimes | 4 (3.7) | ||
| Rarely | 16 (14.8) | ||
| Never | 83 (76.9) | ||
| N/A | 2 (1.9) | ||
| Q4 | When I am at the hospital, I wear the identification card (name and surname, photograph and “student in training”), and carry it in a visible place. | Never | 3 (2.8) |
| Rarely | 12 (11.1) | ||
| Sometimes | 6 (5.6) | ||
| Quite often | 20 (18.5) | ||
| Always | 66 (61.1) | ||
| N/A | 1 (0.9) | ||
| Q5 | The health-care center (not the medical school) takes charge of providing me with a student identification card for the rotation. | No | 52 (48.2) |
| Yes | 52 (48.2) | ||
| N/A | 4 (3.7) | ||
| Q6 | When the academic year is finished, I am obligated to give my student identification card back. | No | 86 (79.6) |
| Yes | 2 (1.9) | ||
| N/A | 20 (18.5) | ||
| Q7 | When assigning the clinical rotations, the faculty informs me of what hospital service I am assigned to. In addition, they also inform me of which doctor will be responsible for my rotation. | Never | 1 (0.9) |
| Rarely | 2 (1.9) | ||
| Sometimes | 8 (7.4) | ||
| Quite often | 31 (28.7) | ||
| Always | 65 (60.2) | ||
| N/A | 1 (0.9) | ||
| Q8 | On the first day of each rotation, my assigned tutor already knew how many students we were and our names, our schedule and timetable, etc. | Never | 32 (29.6) |
| Rarely | 47 (43.5) | ||
| Sometimes | 15 (13.9) | ||
| Quite often | 12 (11.1) | ||
| Always | 1 (0.9) | ||
| N/A | 1 (0.9) | ||
| Q9 | In preclinical years (mainly 1st and 2nd) we have used mannequins, simulated patients and/or roleplays, in order to acquire skills for the “patient-student” relationship in subsequent clinical courses. | No | 46 (42.6) |
| Yes | 58 (53.7) | ||
| N/A | 4 (3.7) | ||
| Q10 | I have got nervous on some occasion during a health care process in my rotation, and I have missed not having practiced before with a mannequin, simulated patient, using roleplays, etc. | Yes | 81 (75) |
| No | 25 (23.2) | ||
| N/A | 2 (1.9) | ||
| Q11 | During my rotation, I have access to the patient’s medical history and I could have modified it. | Always | 11 (10.2) |
| Quite often | 20 (18.5) | ||
| Sometimes | 25 (23.2) | ||
| Rarely | 26 (24.1) | ||
| Never | 25 (23.2) | ||
| N/A | 1 (0.9) | ||
| Q12 | I do clinical interviews with patients and read their medical reports without the presence of my responsible doctor. | Always | 3 (2.8) |
| Quite often | 28 (25.9) | ||
| Sometimes | 44 (40.7) | ||
| Rarely | 22 (20.4) | ||
| Never | 11 (10.2) | ||
| N/A | 0 (0.0) | ||
| Q13 | During my rotation, the doctor knocks at the door and greets the patients when entering their rooms. | Never | 1 (0.9) |
| Rarely | 2 (1.9) | ||
| Sometimes | 8 (7.4) | ||
| Quite often | 47 (43.5) | ||
| Always | 49 (45.4) | ||
| N/A | 1 (0.9) | ||
| Q14 | More than 3 students have been present at the same time in some health-care process of a patient. | Always | 2 (1.9) |
| Quite often | 29 (26.9) | ||
| Sometimes | 49 (45.4) | ||
| Rarely | 16 (14.8) | ||
| Never | 12 (11.1) | ||
| N/A | 0 (0.0) | ||
| Q15 | I have sent a patient’s medical history to my personal email, without expressly asking the patient for permission. | Yes | 3 (2.8) |
| No | 104 (96.3) | ||
| N/A | 1 (0.9) | ||
| Q16 | I have used my personal mobile phone during a patient’s care process for things unrelated to learning (WhatsApp, social networks, etc.) | Quite often | 2 (1.9) |
| Sometimes | 18 (16.7) | ||
| Rarely | 33 (30.6) | ||
| Never | 55 (50.9) | ||
| N/A | 0 (0.0) | ||
| Q17 | My assigned doctor informs me about patients’ rights and corrects me in case of not acting correctly on issues of personal treatment, ethics, privacy, dignity, etc. | Never | 15 (13.9) |
| Rarely | 24 (22.2) | ||
| Sometimes | 28 (25.9) | ||
| Quite often | 20 (18.5) | ||
| Always | 12 (11.1) | ||
| N/A | 9 (8.3) | ||
| Q18 | Before a patient’s care process, my assigned doctor informs him/her (or his/her representative) of the presence of students and asks him/her for verbal consent for the students to witness the clinical act. | Never | 4 (3.7) |
| Rarely | 25 (23.2) | ||
| Sometimes | 33 (30.6) | ||
| Quite often | 34 (31.5) | ||
| Always | 12 (11.1) | ||
| N/A | 0 (0.0) | ||
| Q19 | If the doctor considers it appropriate for me to carry out some type of exploration or procedure, he/she again asks for the verbal consent of the patient (or his/her representative). | Never | 3 (2.8) |
| Rarely | 16 (14.8) | ||
| Sometimes | 26 (24.1) | ||
| Quite often | 37 (34.3) | ||
| Always | 26 (24.1) | ||
| Q20 | Some doctor told me private aspects about a patient without any clinical interest (e.g., “she is the mother of the mayor”, “she is the sister of the hospital manager”, “he likes to go to certain places”, etc.). | Yes | 63 (58.3) |
| No | 38 (35.2) | ||
| N/A | 7 (6.5) | ||
| Q21 | The management of the health centers in which I carry out my training rotations (medical director, hospital manager, etc.) are responsible for explaining the ethical principles and basic rules of action in the patient care process. | Never | 55 (50.9) |
| Rarely | 25 (23.2) | ||
| Sometimes | 16 (14.8) | ||
| Quite often | 5 (4.6) | ||
| Always | 3 (2.8) | ||
| N/A | 4 (3.7) | ||
| Q22 | During my rotations, the doctor introduces and identifies him/herself when entering the patients’ rooms, as well as introduces me and identifies me as a student. | Never | 4 (3.7) |
| Rarely | 17 (15.7) | ||
| Sometimes | 35 (32.4) | ||
| Quite often | 39 (36.1) | ||
| Always | 12 (11.1) | ||
| N/A | 1 (0.9) | ||
| Q23 | During my rotations, I have access to patients’ identification data, such as name, surname, age, address, etc. (I see it in medical record or report, my assigned doctor tells me, etc.), not only purely clinical data. | Always | 38 (35.2) |
| Quite often | 38 (35.2) | ||
| Sometimes | 25 (23.2) | ||
| Rarely | 4 (3.7) | ||
| Never | 2 (1.9) | ||
| N/A | 1 (0.9) | ||
| Q24 | The health-care centers in which I carry out my rotations have systems that allow students to read clinical reports about patients without being able to see their identification data (name, address, profession, etc.). | No | 66 (61.1) |
| Yes | 11 (10.2) | ||
| N/A | 31 (28.7) |
| Question | Statements | Category | Total | Current Academic Year | p | |
|---|---|---|---|---|---|---|
| From 1st to 3rd | From 4th to 6th | |||||
| Q25 | Being a student and not a doctor, I am legally not compelled to keep medical secrecy. | Incorrect answer | 11 | 7 (63.64) | 4 (36.36) | 0.021 |
| Correct answer | 118 | 35 (29.66) | 83 (70.34) | |||
| Q26 | If a patient gives his/her consent, the doctor is legally allowed to “break” medical secrecy. | Incorrect answer | 77 | 25 (32.47) | 52 (67.53) | 0.556 |
| Correct answer | 30 | 8 (26.67) | 22 (73.33) | |||
| N/A | 22 | 9 (40.91) | 13 (59.09) | |||
| Q27 | If a patient dies, medical secrecy disappears with him/her. | Incorrect answer | 8 | 3 (37.50) | 5 (62.50) | 0.063 |
| Correct answer | 110 | 32 (29.09) | 78 (70.91) | |||
| N/A | 11 | 7 (63.64) | 4 (36.36) | |||
| Q28 | During my rotation in the hospital, a patient wants me not to be in his care process because I am a student. I refuse, since it is a “university hospital”. | Incorrect answer | 67 | 27 (40.30) | 40 (59.70) | 0.051 |
| Correct answer | 62 | 15 (24.19) | 47 (75.81) | |||
| Q29 | During your rotation in cardiology, a neighbor of yours gets hospitalized in your wards. When you get home, you tell your parents/friends about it. | Incorrect answer | 72 | 27 (37.50) | 45 (62.50) | 0.178 |
| Correct answer | 57 | 15 (26.32) | 42 (73.68) | |||
| Q30 | If a doctor diagnoses a patient with a disease of public health significance (for example, cholera), the doctor is legally allowed to “break” medical secrecy and report to health authorities. | Incorrect answer | 7 | 4 (57.14) | 3 (42.86) | 0.001 |
| Correct answer | 110 | 29 (26.36) | 81 (73.64) | |||
| N/A | 12 | 9 (75.00) | 3 (25.00) | |||
| Q31 | I take a photograph of a patient’s admission report, which would be useful for preparing some assignment. I will not share it with anyone, I will simply store it in the phone’s photo gallery. | Incorrect answer | 100 | 31 (31.00) | 69 (69.00) | 0.483 |
| Correct answer | 29 | 11 (37.93) | 18 (62.07) | |||
| Q32 | During your rotation in psychiatry, a patient suspected of domestic violence addresses you because he wants some medication to calm his headache. You are alone. You ignore it and don’t tell your doctor. | Incorrect answer | 18 | 7 (38.89) | 11 (61.11) | 0.537 |
| Correct answer | 111 | 35 (31.53) | 76 (68.47) | |||
| Q33 | If a doctor diagnoses a patient with a severe contagious disease, the doctor is legally allowed to “break” medical secrecy and tell the patient’s partner, even if the patient does not want it to be told, in order to avoid potential damage of the partner’s health. | Incorrect answer | 21 | 5 (23.81) | 16 (76.19) | 0.016 |
| Correct answer | 88 | 25 (28.41) | 63 (71.59) | |||
| N/A | 20 | 12 (60.00) | 8 (40.00) | |||
| Q34 | During my rotation, I see a patient with Fournier’s gangrene. This disease is not seen every day, so I send a WhatsApp group with class friends a photo of the perineal necrosis, without informing the patient, but without giving information about his identity. | Incorrect answer | 42 | 20 (47.62) | 22 (52.38) | 0.011 |
| Correct answer | 87 | 22 (25.29) | 65 (74.71) | |||
| Q35 | In case of a patient who is expected to stay in hospital more than 15 days, if the doctor has already asked the patient for his verbal consent for me to be present at the clinical events and even perform physical examinations, it is not necessary to ask again the patient for his verbal consent during the rest of his stay. | Incorrect answer | 102 | 34 (33.33) | 68 (66.67) | 0.715 |
| Correct answer | 27 | 8 (29.63) | 19 (70.37) | |||
| Q36 | During your emergency room rotation, a patient is continuously shouting and insulting the staff because he has been waiting to be attended for quite some time. For this reason, you attend before to other patients who have arrived later than him. | Incorrect answer | 48 | 15 (31.25) | 33 (68.75) | 0.807 |
| Correct answer | 81 | 27 (33.33) | 54 (66.67) | |||
| Q37 | During your rotation through the internal medicine wards, you perform a physical examination of a terminally ill patient. After finishing, you go with your doctor to the wards to continue visiting patients. However, when you leave the patient’s room you realize that you have exposed the patient’s genitalia and you tell the doctor. The patient has dementia and has no family/friends who could complain. The doctor tells you “it is not necessary; nobody comes to see him”. | Incorrect answer | 5 | 4 (80.00) | 1 (20.00) | 0.021 |
| Correct answer | 124 | 38 (30.65) | 86 (69.35) | |||
| Q38 | If a judge requests a doctor to testify at a trial, the doctor is legally allowed to “break” medical secrecy regarding that patient. | Incorrect answer | 36 | 11 (30.56) | 25 (69.44) | 0.002 |
| Correct answer | 64 | 14 (21.88) | 50 (78.13) | |||
| N/A | 29 | 17 (58.62) | 12 (41.38) | |||
| Q39 | I upload to Instagram a photo in which I am auscultating a patient. I do not expressly ask the patient for permission. The patient has a characteristic tattoo on the sternum area (visible in the photo), but his face cannot be seen. | Incorrect answer | 8 | 6 (75.00) | 2 (25.00) | 0.008 |
| Correct answer | 121 | 36 (29.75) | 85 (70.25) | |||
| Q40 | I upload to Instagram a photo in which I am auscultating a patient. I do not expressly ask the patient for permission, but her face cannot be seen, so there is no way to know her identity. | Incorrect answer | 50 | 20 (40.00) | 30 (60.00) | 0.151 |
| Correct answer | 79 | 22 (27.85) | 57 (72.15) | |||
| Q41 | During your rotation in traumatology, the surgeon photographs with her personal mobile phone anatomic areas of patients with large cosmetic defects. After the operation, she photographs the area again to make a comparison. In order to know which patient the image belongs to, she labels images with medical record numbers. | Incorrect answer | 102 | 34 (33.33) | 68 (66.67) | 0.715 |
| Correct answer | 27 | 8 (29.63) | 19 (70.37) | |||
| Q42 | In case of an under-18 patient, the doctor must ask the patient’s legal representative for verbal consent about my presence as a student in the health care process. | Incorrect answer | 47 | 19 (40.43) | 28 (59.57) | 0.149 |
| Correct answer | 82 | 23 (28.05) | 59 (71.95) | |||
| Q43 | In the previous case (under-18 patient), once verbal consent has been asked, the legal representative decides on his/her own, and has no obligation to listen to what the minor thinks about what has been reported. | Incorrect answer | 56 | 22 (39.29) | 34 (60.71) | 0.153 |
| Correct answer | 73 | 20 (27.40) | 53 (72.60) | |||
| Q44 | In case of a patient with limited decision-making capacity, the doctor must ask the family/partner/legal representative of the patient for verbal consent about my presence as a student in the care process. | Incorrect answer | 54 | 19 (35.19) | 35 (64.81) | 0.589 |
| Correct answer | 75 | 23 (30.67) | 52 (69.33) | |||
| Q45 | In case of an incapacitated patient (with a judicial sentence), the doctor must ask the family/partner/legal representative of the patient for verbal consent about my presence as a student in the care process. | Incorrect answer | 53 | 19 (35.85) | 34 (64.15) | 0.505 |
| Correct answer | 76 | 23 (30.26) | 53 (69.74) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terán, A.Á.; Palazuelos, C.; Dierssen-Sotos, T.; Alonso-Molero, J.; Llorca, J.; Gómez-Acebo, I. Evolution of Medical Students’ Perception of the Patient’s Right to Privacy. Int. J. Environ. Res. Public Health 2022, 19, 11067. https://doi.org/10.3390/ijerph191711067
Terán AÁ, Palazuelos C, Dierssen-Sotos T, Alonso-Molero J, Llorca J, Gómez-Acebo I. Evolution of Medical Students’ Perception of the Patient’s Right to Privacy. International Journal of Environmental Research and Public Health. 2022; 19(17):11067. https://doi.org/10.3390/ijerph191711067
Chicago/Turabian StyleTerán, Alberto Álvarez, Camilo Palazuelos, Trinidad Dierssen-Sotos, Jessica Alonso-Molero, Javier Llorca, and Inés Gómez-Acebo. 2022. "Evolution of Medical Students’ Perception of the Patient’s Right to Privacy" International Journal of Environmental Research and Public Health 19, no. 17: 11067. https://doi.org/10.3390/ijerph191711067
APA StyleTerán, A. Á., Palazuelos, C., Dierssen-Sotos, T., Alonso-Molero, J., Llorca, J., & Gómez-Acebo, I. (2022). Evolution of Medical Students’ Perception of the Patient’s Right to Privacy. International Journal of Environmental Research and Public Health, 19(17), 11067. https://doi.org/10.3390/ijerph191711067