
A Review of COVID-19 Response Challenges in Ethiopia

 ,
,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
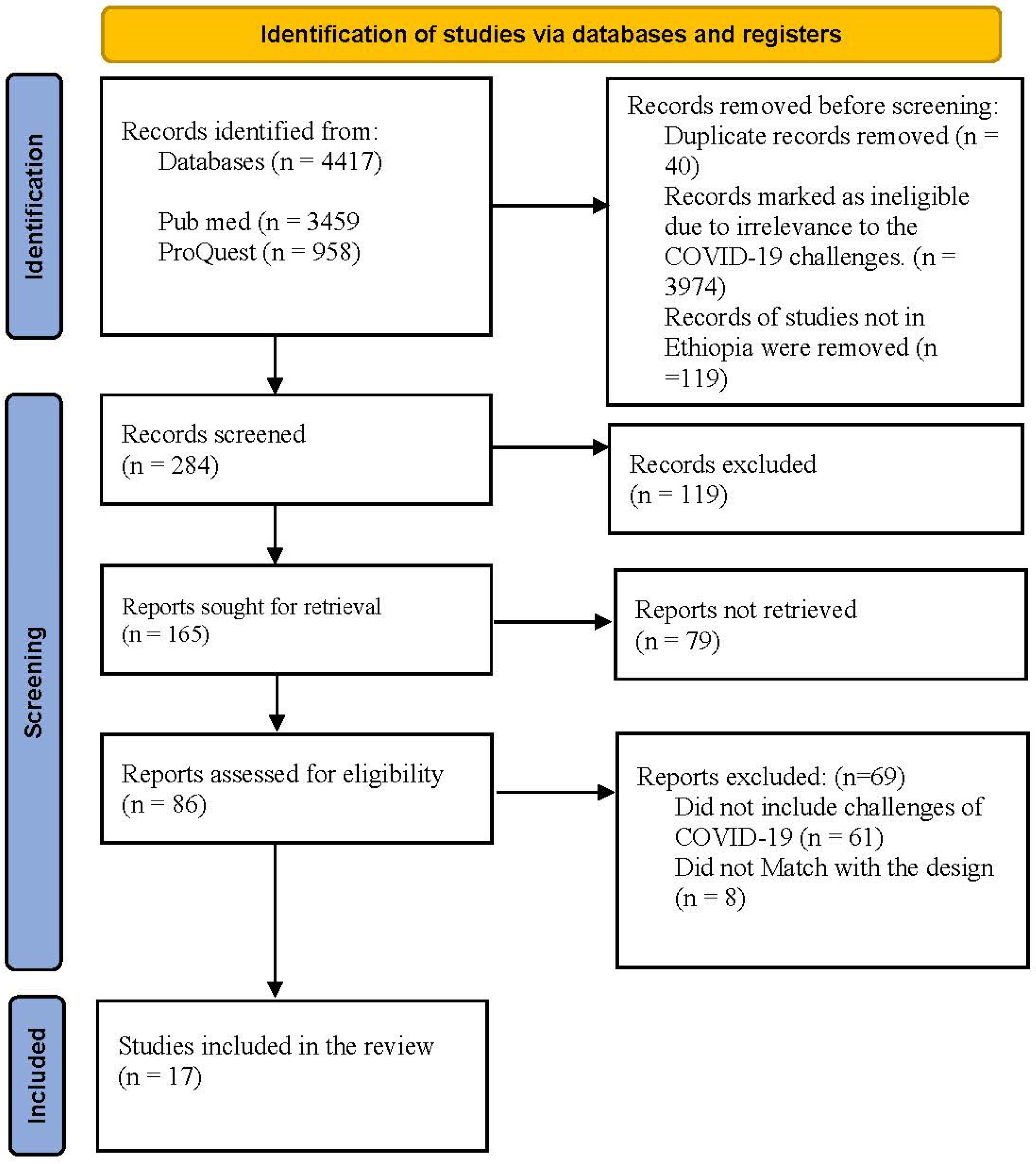
2.1. Search Strategy
2.2. Study Selection
2.3. Analysis and Reporting the Results
3. Results
3.1. COVID-19 Response Challenges to the Healthcare System in Ethiopia
3.2. Leadership and Governance
3.3. Health Financing
3.4. Health Workforce
3.5. Service Delivery
3.6. Essential Medicines
3.7. Information System
4. Discussion
4.1. Key Messages
- (a)
- The Ethiopian pandemic response saw good support from policymakers and Ministry of Health authorities;
- (b)
- No large-scale lockdown was enforced in Ethiopia, but preventive measures were privileged;
- (c)
- Shortage of medical personnel resulted in scarce testing capacity;
- (d)
- Ethiopia experienced disruption of routine health services, including MNCH services;
- (e)
- The pandemic impacted the pharmaceutical supply chain, leading to a shortage of emergency care supplies;
- (f)
- The private sector had an important role in supporting the health system in the response to the COVID-19 pandemic in Ethiopia.
4.2. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes—WHO’s Framework for Action; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Kruk, M.E.; Myers, M.; Varpilah, S.T.; Dahn, B.T. What is a resilient health system? Lessons from Ebola. Lancet 2015, 385, 1910–1912. [Google Scholar] [CrossRef]
- Heymann, D.L.; Chen, L.; Takemi, K.; Fidler, D.P.; Tappero, J.W.; Thomas, M.J.; Kenyon, T.A.; Frieden, T.R.; Yach, D.; Nishtar, S.; et al. Global health security: The wider lessons from the west African Ebola virus disease epidemic. Lancet 2015, 385, 1884–1901. [Google Scholar] [CrossRef]
- Bong, C.-L.; Brasher, C.; Chikumba, E.; McDougall, R.; Mellin-Olsen, J.; Enright, A. The COVID-19 Pandemic: Effects on Low- and Middle-Income Countries. Anesthesia Analg. 2020, 131, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Rahman, A.E.; Amole, T.G.; Galadanci, H.; Matjila, M.; Soma-Pillay, P.; Gillespie, B.M.; El Arifeen, S.; Anumba, D.O.C. The effect of COVID-19 on maternal newborn and child health (MNCH) services in Bangladesh, Nigeria and South Africa: Call for a contextualised pandemic response in LMICs. Int. J. Equity Health 2021, 20, 77. [Google Scholar] [CrossRef]
- Africa CDC. Africa Joint Continental Strategy for COVID-19 Outbreak. 2020. Available online: https://africacdc.org/download/africa-joint-continental-strategy-for-covid-19-outbreak/ (accessed on 15 March 2022).
- Bill & Melinda Gates Foundation. 2020. Available online: https://www.gatesfoundation.org/Media-Center/Press-Releases/2020/02/Bill-and-Melinda-Gates-Foundation-Dedicates-Additional-Funding-to-the-Novel-Coronavirus-Response (accessed on 17 March 2022).
- The World Bank’s Classification of Countries by Income. 2021. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 25 August 2022).
- Africa CDC. Africa CDC Receives Third Donation of Medical Supplies from Jack Ma Foundation, Co-Hosts Global MediXChange Webinar on COVID-19. 2020. Available online: https://africacdc.org/news-item/africa-cdc-receives-third-donation-of-medical-supplies-from-jack-ma-foundation-co-hosts-global-medixchange-webinar-on-covid-19/ (accessed on 22 April 2022).
- Worldometers, Coronavirus. Available online: www.worldometers.info/coronavirus (accessed on 26 July 2022).
- FMOH. National Comprehensive COVID-19 Management Handbook; Ethiopian Federal Ministry of Health: Addis Ababa, Ethiopia, 2020.
- Baye, K. COVID-19 Prevention Measures in Ethiopia: Current Realities and Prospects; ESSP Working Paper 141; International Food Policy Research Institute (IFPRI): Washington, DC, USA; Federal Democratic Republic of Ethiopia Policy Studies Institute: Addis Ababa, Ethiopia, 2020. [CrossRef]
- Zikargae, M.H. COVID-19 in Ethiopia: Assessment of How the Ethiopian Government has Executed Administrative Actions and Managed Risk Communications and Community Engagement. Risk Manag. Health Policy 2020, 13, 2803–2810. [Google Scholar] [CrossRef]
- Haldane, V.; Ong, S.-E.; Chuah, F.L.-H.; Legido-Quigley, H. Health systems resilience: Meaningful construct or catchphrase? Lancet 2017, 389, 1513. [Google Scholar] [CrossRef]
- Ozawa, S.; Paina, L.; Qiu, M. Exploring pathways for building trust in vaccination and strengthening health system resilience. BMC Health Serv. Res. 2016, 16, 131–141. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Monitoring the Building Blocks of the Health System; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Tolu, L.B.; Ezeh, A.; Feyissa, G.T. How Prepared Is Africa for the COVID-19 Pandemic Response? The Case of Ethiopia. Risk Manag. Health Policy 2020, 13, 771–776. [Google Scholar] [CrossRef]
- Mulu, G.B.; Kebede, W.M.; Worku, S.A.; Mittiku, Y.M.; Ayelign, B. Preparedness and Responses of Healthcare Providers to Combat the Spread of COVID-19 Among North Shewa Zone Hospitals, Amhara, Ethiopia, 2020. Infect. Drug Resist. 2020, 13, 3171–3178. [Google Scholar] [CrossRef]
- Shimels, T. The Trend of Health Service Utilization and Challenges Faced During the COVID-19 Pandemic at Primary Units in Addis Ababa: A Mixed-Methods Study. Health Serv. Res. Manag. Epidemiol. 2021, 8, 23333928211031119. [Google Scholar] [CrossRef]
- Mersha, A.; Shibiru, S.; Girma, M.; Ayele, G.; Bante, A.; Kassa, M.; Abebe, S.; Shewangizaw, M. Perceived barriers to the practice of preventive measures for COVID-19 pandemic among health professionals in public health facilities of the Gamo zone, southern Ethiopia: A phenomenological study. BMC Public Health 2021, 21, 199. [Google Scholar] [CrossRef]
- Abdela, S.G.; Berhanu, A.B.; Ferede, L.M.; Van Griensven, J. Essential Healthcare Services in the Face of COVID-19 Prevention: Experiences from a Referral Hospital in Ethiopia. Am. J. Trop. Med. Hyg. 2020, 103, 1198–1200. [Google Scholar] [CrossRef]
- Shimels, T.; Kassu, R.A.; Bogale, G.; Bekele, M.; Getnet, M.; Getachew, A.; Shewamene, Z.; Abraha, M. Magnitude and associated factors of poor medication adherence among diabetic and hypertensive patients visiting public health facilities in Ethiopia during the COVID-19 pandemic. PLoS ONE 2021, 16, e0249222. [Google Scholar] [CrossRef]
- Shigute, Z.; Mebratie, A.D.; Alemu, G.; Bedi, A.S. COVID-19 and balance in access to health care in Ethiopia. Clin. Epidemiol. Glob. Health 2021, 9, 1. [Google Scholar] [CrossRef]
- Abraha, H.E.; Gessesse, Z.; Gebrecherkos, T.; Kebede, Y.; Weldegiargis, A.W.; Tequare, M.H.; Welderufael, A.L.; Zenebe, D.; Gebremariam, A.G.; Dawit, T.C.; et al. Clinical Features and Risk Factors Associated with Morbidity and Mortality Among COVID-19 Patients in Northern Ethiopia. Int. J. Infect. Dis. 2021, 105, 776–783. [Google Scholar] [CrossRef]
- Miretu, D.G.; Asfaw, Z.A.; Addis, S.G. Impact of COVID-19 pandemic on vaccination coverage among children aged 15 to 23 months at Dessie town, Northeast Ethiopia, 2020. Hum. Vaccines Immunother. 2021, 17, 2427–2436. [Google Scholar] [CrossRef]
- Birihane, B.M.; Bayih, W.A.; Alemu, A.Y.; Belay, D.M. Perceived Barriers and Preventive Measures of COVID-19 Among Healthcare Providers in Debretabor, North Central Ethiopia, 2020. Risk Manag. Health Policy 2020, 13, 2699–2706. [Google Scholar] [CrossRef]
- Mekonen, E.; Shetie, B.; Muluneh, N. The Psychological Impact of COVID-19 Outbreak on Nurses Working in the Northwest of Amhara Regional State Referral Hospitals, Northwest Ethiopia. Psychol. Res. Behav. Manag. 2020, 13, 1353–1364. [Google Scholar] [CrossRef]
- Mohammed, H.; Oljira, L.; Roba, K.T.; Yimer, G.; Fekadu, A.; Manyazewal, T. Containment of COVID-19 in Ethiopia and implications for tuberculosis care and research. Infect. Dis. Poverty 2020, 9, 131. [Google Scholar] [CrossRef]
- Beyne, N.W.; Sitota, A.L.; Tegegn, B.; Bobobsha, K. The impact of COVID-19 on the tuberculosis control activities in Addis Ababa. Pan Afr. Med J. 2021, 38, 243. [Google Scholar] [CrossRef] [PubMed]
- Abdela, S.G.; van Griensven, J.; Seife, F.; Enbiale, W. Neglecting the effect of COVID-19 on neglected tropical diseases: The Ethiopian perspective. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 730–732. [Google Scholar] [CrossRef] [PubMed]
- Tiruneh, A.; Yetneberk, T.; Eshetie, D.; Chekol, B.; Gellaw, M. A cross-sectional survey of COVID-19 preparedness in governmental hospitals of North-West Ethiopia. SAGE Open Med. 2021, 9, 2050312121993292. [Google Scholar] [CrossRef] [PubMed]
- Boti Sidamo, N.; Hussen, S.; Shibiru, T.; Girma, M.; Shegaze, M.; Mersha, A.; Fikadu, T.; Gebru, Z.; Andarge, E.; Glagn, M.; et al. Exploring Barriers to Effective Implementation of Public Health Measures for Prevention and Control of COVID-19 Pandemic in Gamo Zone of Southern Ethiopia: Using a Modified Tanahashi Model. Risk Manag. Health Policy 2021, 14, 1219–1232. [Google Scholar] [CrossRef]
- Gudina, E.K.; Gobena, D.; Debela, T.; Yilma, D.; Girma, T.; Mekonnen, Z.; Woldie, M.; Abdena, D.; Shume, G.; Kenate, B.; et al. COVID-19 in Oromia Region of Ethiopia: A review of the first 6 months’ surveillance data. BMJ Open 2021, 11, e046764. [Google Scholar] [CrossRef]
- Ayanore, M.A.; Amuna, N.; Aviisah, M.; Awolu, A.; Kipo-Sunyehzi, D.D.; Mogre, V.; Ofori-Asenso, R.; Gmanyami, J.M.; Kugbey, N.; Gyapong, M. Towards Resilient Health Systems in Sub-Saharan Africa: A Systematic Review of the English Language Literature on Health Workforce, Surveillance, and Health Governance Issues for Health Systems Strengthening. Ann. Glob. Health 2019, 85, 113. [Google Scholar] [CrossRef]
- Birhanu, Z.; Ambelu, A.; Fufa, D.; Mecha, M.; Zeynudin, A.; Abafita, J.; Belay, A.; Doyore, F.; Oljira, L.; Bacha, E.; et al. Risk perceptions and attitudinal responses to COVID-19 pandemic: An online survey in Ethiopia. BMC Public Health 2021, 21, 981. [Google Scholar] [CrossRef]
- Africa Union. Country Case Studies of the Impact of COVID-19 in Ethiopia, Kenya, Somalia and Sudan Vol II; Africa Union: Addis Ababa, Ethiopia, 2020. [Google Scholar]
- Biadgilign, S.; Yigzaw, M. COVID-19 in Ethiopia: Current situation, missed opportunities, and the risk of health system disruptions. Pan Afr. Med J. 2020, 35 (Suppl. S2), 66. [Google Scholar] [CrossRef]
- United Nations International Children’s Emergency Fund (UNICEF) Ethiopia. Public Investment in Health in the COVID-19 Pandemic Era Budget Brief/2020/21; UNICEF Ethiopia: Addis Ababa, Ethiopia, 2021. [Google Scholar]
- Teklu, S.; Sultan, M.; Azazh, A.; Worku, A.; Redae, B.; Walelegn, M.; Tefera, M.; Argaw, R.; Waganew, W.; Yifru, S.; et al. Clinical and Socio-demographic Profile of the First 33 COVID-19 Cases Treated at Dedicated Treatment Center in Ethiopia. Ethiop. J. Health Sci. 2020, 30, 645–652. [Google Scholar]
- Memirie, S.T.; Yigezu, A.; Zewdie, S.A.; Mirkuzie, A.H.; Bolongaita, S.; Verguet, S. Hospitalization costs for COVID-19 in Ethiopia: Empirical data and analysis from Addis Ababa’s largest dedicated treatment center. PLoS ONE 2022, 17, e0260930. [Google Scholar] [CrossRef]
- Buseh, A.G.; Stevens, P.E.; Bromberg, M.; Kelber, S.T. The Ebola epidemic in West Africa: Challenges, opportunities, and policy priority areas. Nurs. Outlook 2015, 63, 30–40. [Google Scholar] [CrossRef]
- Nagesh, S.; Chakraborty, S. Saving the frontline health workforce amidst the COVID-19 crisis: Challenges and recommendations. J. Glob. Health 2020, 10, 010345. [Google Scholar] [CrossRef]
- Rose, C. Am I Part of the Cure or Am I Part of the Disease? Keeping Coronavirus Out When a Doctor Comes Home. New Engl. J. Med. 2020, 382, 1684–1685. [Google Scholar] [CrossRef]
- Tefera, Y.G.; Ayele, A.A. Newborns and Under-5 Mortality in Ethiopia: The Necessity to Revitalize Partnership in Post-COVID-19 Era to Meet the SDG Targets. J. Prim. Care Community Health 2021, 12, 2150132721996889. [Google Scholar] [CrossRef]
- Kibret, S.; Teshome, D.; Fenta, E.; Hunie, M.; Tamire, T. Prevalence of anxiety towards COVID-19 and its associated factors among healthcare workers in a Hospital of Ethiopia. PLoS ONE 2020, 15, e0243022. [Google Scholar] [CrossRef]
- Pant, S.; Koirala, S.; Subedi, M. Access to Maternal Health Services during COVID-19. Eur. J. Med. Sci. 2020, 20, 46. Available online: https://www.europasianjournals.org/ejms/index.php/ejms/article/view/110 (accessed on 10 February 2022). [CrossRef]
- Tsehay, M.; Belete, A.; Necho, M. Factors Associated with Psychological Distress and Brief Resilient Coping Level During the COVID-19 Pandemic Among Health-Care Professionals in Dessie, Ethiopia. Psychol. Res. Behav. Manag. 2020, 13, 1213–1221. [Google Scholar] [CrossRef]
- World Health Organization. Toolkit on Monitoring Health Systems Strengthening. 2008. Available online: https://www.who.int/healthinfo/statistics/toolkit_hss/EN_PDF_Toolkit_HSS_InformationSystems.pdf (accessed on 23 April 2022).
- World Health Organization. Home Care for Patients with Suspected Novel Coronavirus (nCoV) Infection Presenting with Mild Symptoms and Management of Contacts. Interim Guidance. 2020. Available online: https://www.who.int/publications-detail/home-care-for-patients-with-suspected-novel-coronavirus-(ncov)-infection-presenting-with-mild-symptoms-and-management-of-contacts (accessed on 13 May 2022).
- Runkle, J.D.; Brock-Martin, A.; Karmaus, W.; Svendsen, E.R. Secondary Surge Capacity: A Framework for Understanding Long-Term Access to Primary Care for Medically Vulnerable Populations in Disaster Recovery. Am. J. Public Health 2012, 102, e24–e32. [Google Scholar] [CrossRef]
- Barasa, E.W.; Ouma, P.O.; Okiro, E.A. Assessing the hospital surge capacity of the Kenyan health system in the face of the COVID-19 pandemic. PLoS ONE 2020, 15, e0236308. [Google Scholar] [CrossRef]
- Centre for International Private Enterprise (CIPE). Responding to the COVID-19 Pandemic in Ethiopia: The Private Sector Experience; CIPE: Washington, DC, USA, 2020. [Google Scholar]
- Mukwege, D.; Cadière, G.-B.; Vandenberg, O. COVID-19 Response in Sub-Saharan Low-Resource Setting: Healthcare Soldiers Need Bullets. Am. J. Trop. Med. Hyg. 2020, 103, 549–550. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Expenditure Database; WHO: Geneva, Switzerland, 2020; Available online: https://apps.who.int/nha/database/ViewData/Indicators/en (accessed on 13 May 2022).
- Gebremeskel, A.T.; Out, A.; Abimbola, S.; Yaya, S. Building resilient health systems in Africa beyond the COVID-19 pandemic response. BMJ Glob. Health 2021, 6, e006108. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| (1) The study deals with the health response and management of the COVID-19 pandemic. | (1) The study is conducted in other countries than Ethiopia. |
| (2) The study setting is Ethiopia. | (2) The article is written in other languages than English. |
| (3) The article is written in English. | (3) The article’s full text is not available. |
| Authors/Ref | Publication Date | Methodology Used | Study Aim | Population and Sample Size | Identified Challenges to Pandemic Response |
|---|---|---|---|---|---|
| Tulu et al. 2020 [18] | 9 July 2020 | Description of events | To describe the general epidemic preparedness of Ethiopia. | NA |
|
| Mulu, et al. 2020 [19] | 16 September 2021 | Facility-based cross-sectional | To assess the preparedness and responses of healthcare providers to combat the spread of COVID-19 among North Shewa Zone Hospitals, Amhara, Ethiopia. | 422 healthcare providers |
|
| Shimeles et al. 2021 [20] | 8 July 2021 | multi-facility-based cross-sectional | To assess the trend of health service utilization and challenges faced during the COVID-19 pandemic at primary units in Addis Ababa, Ethiopia. | NA |
|
| Mersha et al., 2021 [21] | 22 January 2021 | semi-structured interview | To explore barriers affecting the practice of preventive measures for the COVID-19 among health professionals. | 16 key informants |
|
| Abdela et al., 2020 [22] | 5 August 2020 | Description of events | To understand the reasons behind the decrease in patient flow by referral Hospitals in Ethiopia. | NA |
|
| Shimeles et al., 2021 [23] | 6 April 2021 | Multi-site cross-sectional | To assess the magnitude and associated factors of poor medication adherence among diabetic and hypertensive patients visiting public health facilities in Addis Ababa, Ethiopia during the COVID-19 pandemic. | 422 participants |
|
| Shigute et al., 2021 [24] | 19 May 2020 | Description of events | To describe the balance in access during the pandemic. | NA |
|
| Abraha et al., 2021 [25] | 10 March 2021 | Secondary data | To describe the clinical features and assess the determinants of severity and in-hospital mortality of patients with coronavirus disease 2019 (COVID-19) in a unique setting in Ethiopia. | 2617 patients admitted to COVID-19 center |
|
| Miretu et al., 2021 [26] | 20 March 2021 | Community-based cross-sectional study | To assess the impact of COVID-19 on vaccination coverage among children aged 15–23. | 633 children with their mother/caregiver were interviewed |
|
| Birihane et al., 2020 [27] | 20 November 2020 | Primary data | To assess perceived barriers and preventive measures of corona virus disease among healthcare providers in Debretabor Town, north central Ethiopia. | healthcare professional n = 203. |
|
| Mekonen et al., 2020 [28] | 5 January 2021 | Primary data | To assess the prevalence and associated factors of anxiety, depression, and stress among nurses working in northwest Amhara referral hospitals. | 302 nurses |
|
| Mohammed et al., 2020 [29] | 16 September 2020 | Description of events | To describe the COVID-19 containment measures and its implication on tuberculosis care and research in Ethiopia. | NA |
|
| Wodajo et al., 2020 [30] | 8 March 2020 | Record review | To assesses the impact of the COVID-19 response on the TB control activities of Addis Ababa health centers. | 56 selected public health clinics |
|
| Seid et al., 2020 [31] | 27 August 2020 | Description of events | Describing COVID-19 impact on NTD prevention and care. | NA |
|
| Tiruneh et al., 2021 [32] | 10 February 2021 | Institutionally based survey | To assess the level of hospital preparedness for COVID-19 in South Gondar Zone Governmental Hospitals, 2020. | NA |
|
| Boti et al., 2021 [33] | 19 March 2021 | Phenomenological | To explore the barriers to effective implementation of public health measures for prevention and control of the COVID-19 pandemic in the Gamo Zone of southern Ethiopia. | NA |
|
| Gudina et al., 2020 [34] | 29 March 2021 | Surveillance data base | To describe the epidemiology of COVID-19 in Oromia Region, the largest and most populous region in Ethiopia, during the early months of the outbreak. | NA |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abagero, A.; Ragazzoni, L.; Hubloue, I.; Barone-Adesi, F.; Lamine, H.; Addissie, A.; Della Corte, F.; Valente, M. A Review of COVID-19 Response Challenges in Ethiopia. Int. J. Environ. Res. Public Health 2022, 19, 11070. https://doi.org/10.3390/ijerph191711070
Abagero A, Ragazzoni L, Hubloue I, Barone-Adesi F, Lamine H, Addissie A, Della Corte F, Valente M. A Review of COVID-19 Response Challenges in Ethiopia. International Journal of Environmental Research and Public Health. 2022; 19(17):11070. https://doi.org/10.3390/ijerph191711070
Chicago/Turabian StyleAbagero, Abdulnasir, Luca Ragazzoni, Ives Hubloue, Francesco Barone-Adesi, Hamdi Lamine, Adamu Addissie, Francesco Della Corte, and Martina Valente. 2022. "A Review of COVID-19 Response Challenges in Ethiopia" International Journal of Environmental Research and Public Health 19, no. 17: 11070. https://doi.org/10.3390/ijerph191711070