
The Level of COVID-19 Anxiety among Oncology Patients in Poland

 ,
,  ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
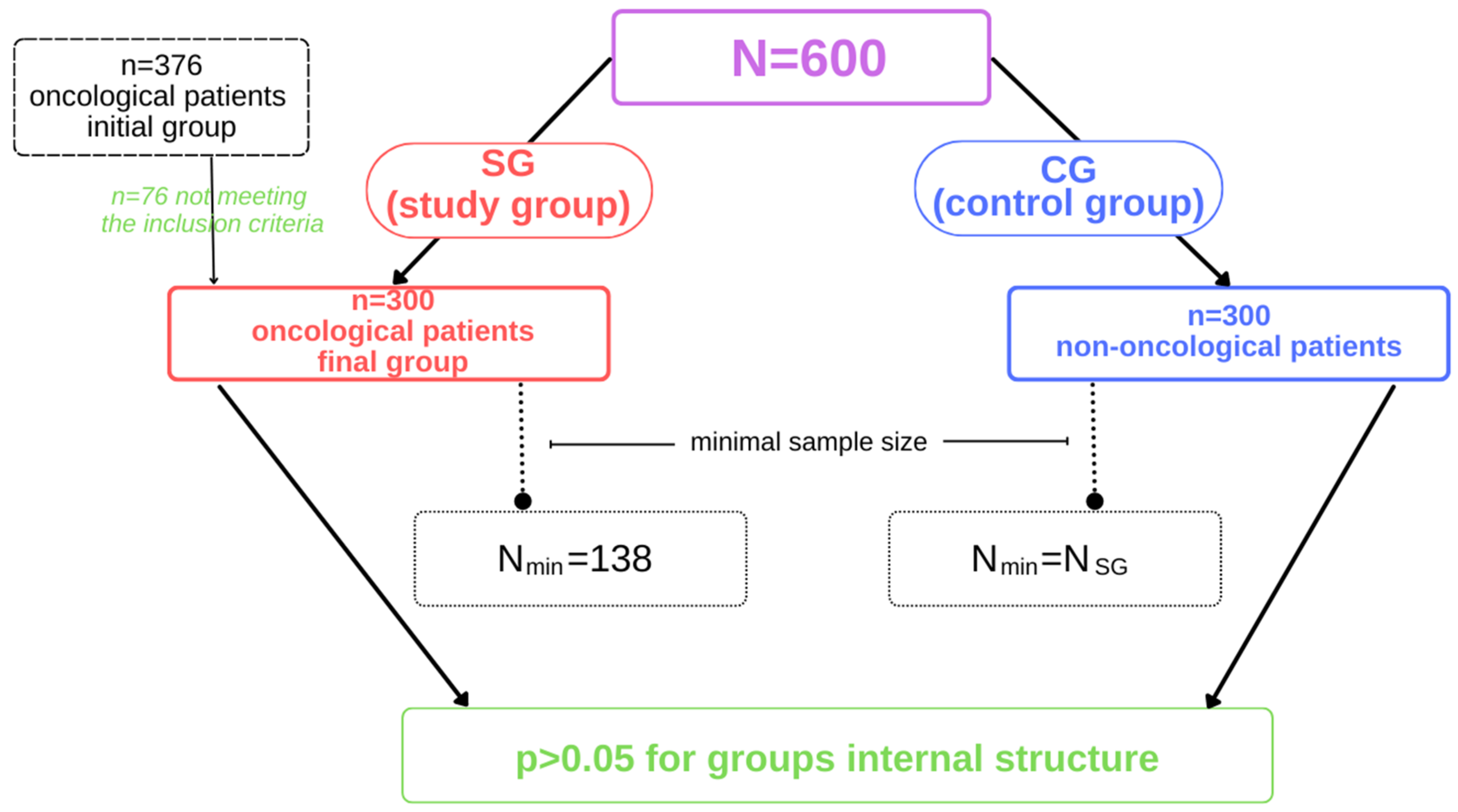
2.1. Participants
2.2. Sample Size Estimation
2.3. Eligibility Criteria
2.4. Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Botha, F.; Butterworth, P.; Wilkins, R. Evaluating How Mental Health Changed in Australia through the COVID-19 Pandemic: Findings from the ‘Taking the Pulse of the Nation’ (TTPN) Survey. Int. J. Environ. Res. Public Health 2022, 19, 558. [Google Scholar] [CrossRef]
- Petrie, K.; Smallwood, N.; Pascoe, A.; Willis, K. Mental Health Symptoms and Workplace Challenges among Australian Paramedics during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1004. [Google Scholar] [CrossRef]
- Kotera, Y.; Ozaki, A.; Miyatake, H.; Tsunetoshi, C.; Nishikawa, Y.; Kosaka, M.; Tanimoto, T. Qualitative Investigation into the Mental Health of Healthcare Workers in Japan during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 568. [Google Scholar] [CrossRef] [PubMed]
- Rozmiarek, M.; León-Guereño, P.; Tapia-Serrano, M.Á.; Thuany, M.; Gomes, T.N.; Płoszaj, K.; Firek, W.; Malchrowicz-Mośko, E. Motivation and Eco-Attitudes among Night Runners during the COVID-19 Pandemic. Sustainability 2022, 14, 1512. [Google Scholar] [CrossRef]
- Landi, G.; Pakenham, K.I.; Grandi, S.; Tossani, E. Young Adult Carers during the Pandemic: The Effects of Parental Illness and Other Ill Family Members on COVID-19-Related and General Mental Health Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 3391. [Google Scholar] [CrossRef] [PubMed]
- Krifa, I.; van Zyl, L.E.; Braham, A.; Ben Nasr, S.; Shankland, R. Mental Health during COVID-19 Pandemic: The Role of Optimism and Emotional Regulation. Int. J. Environ. Res. Public Health 2022, 19, 1413. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.A.; Ma, W.; Sikavi, D.R.; Drew, D.A.; Nguyen, L.H.; Bowyer, R.C.E.; Cardoso, M.J.; Fall, T.; Freidin, M.B.; Gomez, M.; et al. Cancer and Risk of COVID-19 Through a General Community Survey. Oncologist 2021, 26, 182–185. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Rolston, K. Infections in cancer patients with solid tumors: A review. Infect. Dis. Ther. 2017, 6, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Jammu, A.S.; Chasen, M.R.; Lofters, A.K.; Bhargava, R. Systematic rapid living review of the impact of the COVID-19 pandemic on cancer survivors: Update to August 27, 2020. Supportive Care Cancer 2021, 29, 2841–2850. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Kilgour, H.M.; Haase, K.R. The psychosocial impact of COVID-19 on older adults with cancer: A rapid review. Curr. Oncol. 2022, 29, 589–601. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Glaser, R.; Rice, J.; Sheridan, J.; Fertel, R.; Stout, J.; Speicher, C.; Pinsky, D.; Kotur, M.; Post, A.; Beck, M.; et al. Stress-related immune suppression: Health implications. Brain Behav. Immun. 1987, 1, 7–20. [Google Scholar] [CrossRef]
- Marroquín, B.; Vine, V.; Morgan, R. Mental health during the COVID-19 pandemic: Effects of stay-at-home policies, social distancing behavior, and social resources. Psychiatry Res. 2020, 293, 113419. [Google Scholar] [CrossRef]
- Zhao, S.Z.; Wong, J.Y.H.; Wu, Y.; Choi, E.P.H.; Wang, M.P.; Lam, T.H. Social Distancing Compliance under COVID-19 Pandemic and Mental Health Impacts: A Population-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 6692. [Google Scholar] [CrossRef]
- Kämpfen, F.; Kohler, I.V.; Ciancio, A.; Bruine de Bruin, W.; Maurer, J.; Kohler, H.-P. Predictors of mental health during the COVID-19 pandemic in the US: Role of economic concerns, health worries and social distancing. PLoS ONE 2020, 15, e0241895. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, P.; González-Santos, J.; Santamaría-Peláez, M.; Soto-Cámara, R.; Sánchez-González, E.; González-Bernal, J.J. Psychological Effects of Home Confinement and Social Distancing Derived from COVID-19 in the General Population—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6528. [Google Scholar] [CrossRef]
- Elran-Barak, R.; Mozeikov, M. One Month into the Reinforcement of Social Distancing due to the COVID-19 Outbreak: Subjective Health, Health Behaviors, and Loneliness among People with Chronic Medical Conditions. Int. J. Environ. Res. Public Health 2020, 17, 5403. [Google Scholar] [CrossRef]
- Reizer, A.; Geffen, L.; Koslowsky, M. Life under the COVID-19 lockdown: On the relationship between intolerance of uncertainty and psychological distress. Psychol. Trauma Theory Res. Pract. Policy 2021, 13, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, A.; Brähler, E.; Faller, H.; Härter, M.; Keller, M.; Schulz, H.; Wegscheider, K.; Weis, J.; Boehncke, A.; Hund, B.; et al. Four-week prevalence of mental disorders in patients with cancer across major tumor entities. J. Clin. Oncol. 2014, 32, 3540–3546. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Grajek, M.; Białek-Dratwa, A. The Impact of the Epidemiological Situation Resulting From COVID-19 Pandemic on Selected Aspects of Mental Health Among Patients With Cancer-Silesia Province (Poland). Front. Psychol. 2022, 13, 857326. [Google Scholar] [CrossRef]
- Górski, M.; Garbicz, J.; Buczkowska, M.; Marsik, G.; Grajek, M.; Całyniuk, B.; Polaniak, R. Depressive disorders among long-term care residents in the face of isolation due to COVID-19 pandemic. Psychiatr. Pol. 2022, 56, 101–114. [Google Scholar] [CrossRef]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of depression during the COVID-19 outbreak: A meta-analysis of community-based studies. Int. J. Clin. Health Psychol. 2020, 21, 100196. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef]
- Wu, X.; Nazari, N.; Griffiths, M.D. Using Fear and Anxiety Related to COVID-19 to Predict Cyberchondria: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e26285. [Google Scholar] [CrossRef]
- Quadros, S.; Garg, S.; Ranjan, R.; Vijayasarathi, G.; Mamun, M.A. Fear of COVID 19 Infection Across Different Cohorts: A Scoping Review. Front. Psychiatry 2021, 12, 708430. [Google Scholar] [CrossRef]
- Erdoğan, A.P.; Ekinci, F.; Acar, Ö.; Göksel, G. Level of COVID-19 fear in cancer patients. Middle East Curr. Psychiatry 2022, 29, 9. [Google Scholar] [CrossRef]
- Haddad, F.G.; Kourie, H.R.; Gebara, N.; Matta, C.; Eid, R.; El Karak, F.; Nasr, F.; Chahine, G.; Ghosn, M.; Kattan, J. Cancer Patients in the Era of Coronavirus: What to Fear Most? J. Patient Saf. 2021, 17, e35–e38. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.vogue.com/article/what-is-post-pandemic-stress-disorder (accessed on 10 February 2022).
- Szepietowska, E.M.; Zawadzka, E.; Filipiak, S. Symptoms of Post-Traumatic Stress Disorder and the Sense of Gains and Losses during the COVID-19 Pandemic: An International Study. Int. J. Environ. Res. Public Health 2022, 19, 3504. [Google Scholar] [CrossRef] [PubMed]
- Łaskawiec, D.; Grajek, M.; Szlacheta, P.; Korzonek-Szlacheta, I. Post-Pandemic Stress Disorder as an Effect of the Epidemiological Situation Related to the COVID-19 Pandemic. Healthcare 2022, 10, 975. [Google Scholar] [CrossRef] [PubMed]
- Alyami, M.; Henning, M.; Krägeloh, C.; Alyami, H. Psychometric evaluation of the Arabic version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 19, 2219–2232. [Google Scholar] [CrossRef]
- Sakib, N.; Bhuiyan, A.; Hossain, S.; Al Mamun, F.; Hosen, I.; Abdullah, A.H.; Sarker, A.; Mohiuddin, M.S.; Rayhan, I.; Hossain, M.; et al. Psychometric validation of the Bangla Fear of COVID-19 Scale: Confirmatory factor analysis and rasch analysis. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 20, 1913–1922. [Google Scholar] [CrossRef]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the Fear of COVID-19 Scale: Its association with psychological distress and life satisfaction in Turkey. Int. J. Ment. Health Addict. 2020, 19, 1980–1988. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Khamenka, N.; Isralowitz, R. COVID-19 fear in Eastern Europe: Validation of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 19, 1903–1908. [Google Scholar] [CrossRef]
- Tzur Bitan, D.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 Scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef]
- Huarcaya-Victoria, J.; Villarreal-Zegarra, D.; Podestà, A.; Luna-Cuadros, M. Psychometric properties of a Spanish version of the Fear of COVID-19 Scale in general population of Lima, Peru. Int. J. Ment. Health Addict. 2020, 20, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Barrios, I.; Ríos-González, C.; O’Higgins, M.; González, I.; García, O.; Díaz, N.R.; Castaldelli-Maia, J.M.; Ventriglio, A.; Torales, J. Psychometric properties of the Spanish version of the Fear of COVID-19 Scale (FCV-19S). Int. J. Ment. Health Addict. 2020, 20, 249–262. [Google Scholar] [CrossRef]
- Pisula, E.; Nowakowska, I. FCV-19S Coronavirus Anxiety Scale. Available online: https://www.researchgate.net/publication/344690639_Skala_Leku_przed_Koronawirusem_FCV-19S_Ahorsu_i_in_2020_-_polskie_tlumaczenie (accessed on 5 May 2022). [CrossRef]
- Krajowy Rejestr Nowotworów. Available online: http://onkologia.org.pl/ (accessed on 15 August 2022).
- Health at a Glance 2021 (OECD). Available online: https://www.oecd.org/health/health-at-a-glance/ (accessed on 15 August 2022).
- Yang, Y.-L.; Liu, L.; Wang, Y.; Wu, H.; Yang, X.-S.; Wang, J.-N.; Wang, L. The prevalence of depression and anxiety among Chinese adults with cancer: A systematic review and meta-analysis. BMC Cancer 2013, 13, 393. [Google Scholar] [CrossRef] [PubMed]
- Nikbakhsh, N.; Moudi, S.; Abbasian, S.; Khafri, S. Prevalence of depression and anxiety among cancer patients Caspian. J. Intern. Med. 2014, 5, 167–170. [Google Scholar]
- Lang, K. Krebs und Psyche. W: Psychoonkologie. Schulz-Kindermann, F. (red.). Beltz 2013, 6, 87–99. [Google Scholar]
- Kawase, E.; Karasawa, K.; Shimotsu, S.; Izawa, H.; Hirowatari, H.; Saito, A.I.; Ito, K.; Horikawa, N. Estimation of anxiety and depression in patients with early stage breast cancer before and after radiation therapy. Breast Cancer 2012, 19, 147–152. [Google Scholar] [CrossRef]
- Atkin, N.; Vickerstaff, V.; Candy, B. Worried to death’: The assessment and management of anxiety in patients with advanced life-limiting disease, a national survey of palliative medicine physicians. BMC Palliat. Care 2017, 16, 69. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.C.; Syrjala, K.L. Anxiety and depression in cancer survivors. Med. Clin. N. Am. 2017, 101, 1099–1113. [Google Scholar] [CrossRef]
- Dinkel, A.; Herschbach, P. Fear of progression in cancer patients and survivors. Recent Results Cancer Res. 2018, 210, 13–33. [Google Scholar]
- Oncology 2025. Available online: http://www.onkologia2025.pl/ (accessed on 5 May 2022).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder. The GAD-7. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef]
- Babicki, M.; Mastalerz-Migas, A. Prevalence of anxiety disorders among Poles in the era of the COVID-19 pandemic. Psychiatr. Pol. 2021, 55, 497–509. [Google Scholar] [CrossRef]
- Karacin, C.; Bilgetekin, I.; Basal, F.B.; Oksuzoglu, O.B. How does COVID-19 fear and anxiety affect chemotherapy adherence in patients with cancer. Future Oncol. 2020, 16, 2283–2293. [Google Scholar] [CrossRef] [PubMed]
- Özdin, S.; Bayrak-Özdin, S. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Fujita, K.; Ito, T.; Saito, Z.; Kanai, O.; Nakatani, K.; Mio, T. Impact of COVID-19 pandemic on lung cancer treatment scheduling. Thorac. Cancer 2020, 11, 2983–2986. [Google Scholar] [CrossRef] [PubMed]
- Vanni, G.; Materazzo, M.; Pellicciaro, M.; Ingallinella, S.; Rho, M.; Santori, F.; Cotesta, M.; Caspi, J.; Makarova, A.; Pistolese, C.A.; et al. Breast cancer and COVID-19: The effect of fear on patients’ decision-making process. In Vivo 2020, 34 (Suppl. 3), 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Zhou, S.; Tan, S.H.; Ishak, N.D.B.; Goh, Z.Z.S.; Chua, Z.Y.; Chia, J.M.X.; Chew, E.L.; Shwe, T.; Mok, J.K.Y.; et al. Understanding the Psychological Impact of COVID-19 Pandemic on Patients With Cancer, Their Caregivers, and Health Care Workers in Singapore. JCO Glob. Oncol. 2020, 6, 1494–1509. [Google Scholar] [CrossRef] [PubMed]
- Oncology Portal. Available online: https://www.zwrotnikraka.pl/ (accessed on 5 May 2022).
- Sigorski, D.; Sobczuk, P.; Osmola, M.; Kuć, K.; Walerzak, A.; Wilk, M.; Ciszewski, T.; Kopeć, S.; Hryń, K.; Rutkowski, P.; et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open 2020, 5, e000970. [Google Scholar] [CrossRef] [PubMed]
- Parlapani, E.; Holeva, V.; Nikopoulou, V.A.; Sereslis, K.; Athanasiadou, M.; Godosidis, A.; Stephanou, T.; Diakogiannis, I. Intolerance of Uncertainty and Loneliness in Older Adults During the COVID-19 Pandemic. Frontline Psychiatry 2020, 19, 842. [Google Scholar] [CrossRef] [PubMed]
- Korukcu, O.; Ozkaya, M.; Faruk Boran, O.; Boran, M. The effect of the COVID-19 pandemic on community mental health: A psychometric and prevalence study in Turkey. Health Soc. Care Community 2021, 29, e204–e213. [Google Scholar] [CrossRef]
- Tokgoz, V.Y.; Kaya, Y.; Tekin, A.B. The level of anxiety in infertile women whose ART cycles are postponed due to the COVID-19 outbreak. J. Psychosom. Obstet. Gynaecol. 2022, 43, 114–121. [Google Scholar] [CrossRef]
- Rahman, M.A.; Hoque, N.; Alif, S.M.; Salehin, M.; Islam, S.M.S.; Banik, B.; Sharif, A.; Nazim, N.B.; Sultana, F.; Cross, W. Factors associated with psychological distress, fear and coping strategies during the COVID-19 pandemic in Australia. Glob. Health 2020, 16, 95. [Google Scholar] [CrossRef] [PubMed]
- Giordani, R.; Zanoni da Silva, M.; Muhl, C.; Giolo, S.R. Fear of COVID-19 scale: Assessing fear of the coronavirus pandemic in Brazil. J. Health Psychol. 2020, 16, 1359105320982035. [Google Scholar] [CrossRef] [PubMed]
- Doshi, D.; Karunakar, P.; Sukhabogi, J.R.; Prasanna, J.S.; Mahajan, S.V. Assessing Coronavirus Fear in Indian Population Using the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 28, 2383–2391. [Google Scholar] [CrossRef] [PubMed]
- Lang-Rollin, I.; Berberich, G. Psycho-oncology. Dialog.-Clin. Neurosci. 2018, 20, 13–22. [Google Scholar] [CrossRef]
- Senf, B.; Fettel, J.; Demmerle, C.; Maiwurm, P. Physicians’ attitudes towards psycho-oncology, perceived barriers, and psychosocial competencies: Indicators of successful implementation of adjunctive psycho-oncological care? Psycho-Oncology 2018, 28, 415–422. [Google Scholar] [CrossRef]
- Dinkel, A.; Goerling, U.; Hönig, K.; Karger, A.; Maatouk, I.; Petermann-Meyer, A.; Senf, B.; Woellert, K.; Wünsch, A.; Zimmermann, T.; et al. Psychooncological care for patients with cancer during 12 months of the COVID-19 pandemic: Views and experiences of senior psychooncologists at German Comprehensive Cancer Centers. Psycho-Oncology 2021, 30, 1982–1985. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Mitchell, H.R.; Ting, A. Application of psychological theories on the role of gender in caregiving to psycho-oncology research. Psycho-Oncology 2018, 28, 228–254. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Anxiety Level by GAD-7 | SG | CG |
|---|---|---|
| Lack of anxiety | 19% | 45% |
| Mild anxiety | 12% | 30% |
| Moderate anxiety | 10% | 10% |
| Severe anxiety | 15% | 4% |
| Generalized anxiety (greater than 10 points) | 44% | 11% |
| FCV-19S * Scale Discriminator | Group | Strongly Disagree | Rather Disagree | No Opinion | Rather Agree | Strongly Agree |
|---|---|---|---|---|---|---|
| I am very afraid of SARS-CoV-2 (coronavirus) | SG | 7% | 11% | 23% | 35% | 24% |
| CG | 20% | 23% | 43% | 11% | 3% | |
| Total | 14% | 17% | 33% | 23% | 14% | |
| I feel anxious when I think about coronavirus | SG | 9% | 9% | 19% | 31% | 32% |
| CG | 26% | 17% | 29% | 17% | 11% | |
| Total | 18% | 13% | 24% | 24% | 22% | |
| My hands sweat when I think about coronavirus | SG | 23% | 19% | 29% | 15% | 14% |
| CG | 48% | 31% | 9% | 13% | 9% | |
| Total | 36% | 25% | 19% | 14% | 12% | |
| I’m afraid of losing my life due to coronavirus | SG | 8% | 10% | 33% | 29% | 20% |
| CG | 34% | 27% | 17% | 9% | 13% | |
| Total | 21% | 19% | 25% | 19% | 17% | |
| When I watch the news and learn about coronavirus-related stories on social media, I get nervous or anxious | SG | 9% | 11% | 23% | 33% | 24% |
| CG | 22% | 23% | 43% | 9% | 3% | |
| Total | 16% | 17% | 33% | 21% | 14% | |
| I can’t sleep because I’m worried about getting infected with coronavirus | SG | 31% | 27% | 9% | 14% | 19% |
| CG | 42% | 31% | 19% | 7% | 1% | |
| Total | 37% | 29% | 14% | 11% | 10% | |
| My heart beats rapidly when I think of coronavirus infection | SG | 23% | 19% | 19% | 17% | 22% |
| CG | 34% | 31% | 21% | 13% | 1% | |
| Total | 29% | 25% | 20% | 15% | 12% |
| FCV-19S * Scale Discriminator | Group | X | SD | MIN | MAX | Me | Mo | t | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| I am very afraid of SARS-CoV-2 (coronavirus) | SG | 4.1 | 0.9 | 1 | 5 | 3 | 4 | 11.298 | 0.001 |
| CG | 2.8 | 0.7 | 1 | 5 | 3 | 3 | |||
| Total | 3.4 | 0.8 | 1 | 5 | 3 | 3 | |||
| I feel anxious when I think about coronavirus | SG | 3.5 | 0.5 | 1 | 5 | 3 | 4 | 10.986 | 0.001 |
| CG | 2.2 | 0.7 | 1 | 5 | 3 | 2 | |||
| Total | 2.8 | 0.7 | 1 | 5 | 3 | 3 | |||
| My hands sweat when I think about coronavirus | SG | 1.9 | 0.9 | 1 | 5 | 3 | 2 | 12.862 | 0.001 |
| CG | 1.2 | 0.9 | 1 | 5 | 3 | 2 | |||
| Total | 1.5 | 0.9 | 1 | 5 | 3 | 2 | |||
| I’m afraid of losing my life due to coronavirus | SG | 2.5 | 0.7 | 1 | 5 | 3 | 2 | 10.632 | 0.001 |
| CG | 1.2 | 0.5 | 1 | 5 | 3 | 2 | |||
| Total | 1.7 | 0.7 | 1 | 5 | 3 | 2 | |||
| When I watch the news and learn about coronavirus-related stories on social media, I get nervous or anxious | SG | 3.3 | 0.5 | 1 | 5 | 3 | 3 | 10.256 | 0.001 |
| CG | 1.5 | 0.5 | 1 | 5 | 3 | 2 | |||
| Total | 2.5 | 0.5 | 1 | 5 | 3 | 2 | |||
| I can’t sleep because I’m worried about getting infected with coronavirus | SG | 2.5 | 0.3 | 1 | 5 | 3 | 3 | 11.753 | 0.001 |
| CG | 1.1 | 0.5 | 1 | 5 | 3 | 1 | |||
| Total | 1.4 | 0.4 | 1 | 5 | 3 | 1 | |||
| My heart beats rapidly when I think of coronavirus infection | SG | 2.3 | 0.9 | 1 | 5 | 3 | 2 | 12.765 | 0.001 |
| CG | 1.1 | 0.5 | 1 | 5 | 3 | 1 | |||
| Total | 1.6 | 0.7 | 1 | 5 | 3 | 1 | |||
| Raw score (points) | SG | 20.1 ± 4.7 | 11.824 | 0.001 | |||||
| CG | 10.6 ± 4.3 | ||||||||
| Total | 14.9 ± 4.5 | ||||||||
| Recalculated result (%) | SG | 57.4 | |||||||
| CG | 30.3 | ||||||||
| Total | 42.6 | ||||||||
| Interpretation | SG | Moderate level of anxiety | |||||||
| CG | Low anxiety | ||||||||
| Total | Low anxiety | ||||||||
| Reason for Anxiety | SG | CG | Total | t | p-Value |
|---|---|---|---|---|---|
| Death alone | 82% | 54% | 68% | 12.866 | 0.023 |
| Complications | 46% | 56% | 51% | 13.001 | 0.013 |
| Treatment delay | 62% | 38% | 50% | 10.581 | 0.001 |
| Income loss | 38% | 32% | 35% | 10.549 | 0.002 |
| Separation | 36% | 26% | 31% | 12.987 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grajek, M.; Krupa-Kotara, K.; Rozmiarek, M.; Sobczyk, K.; Działach, E.; Górski, M.; Kobza, J. The Level of COVID-19 Anxiety among Oncology Patients in Poland. Int. J. Environ. Res. Public Health 2022, 19, 11418. https://doi.org/10.3390/ijerph191811418
Grajek M, Krupa-Kotara K, Rozmiarek M, Sobczyk K, Działach E, Górski M, Kobza J. The Level of COVID-19 Anxiety among Oncology Patients in Poland. International Journal of Environmental Research and Public Health. 2022; 19(18):11418. https://doi.org/10.3390/ijerph191811418
Chicago/Turabian StyleGrajek, Mateusz, Karolina Krupa-Kotara, Mateusz Rozmiarek, Karolina Sobczyk, Eliza Działach, Michał Górski, and Joanna Kobza. 2022. "The Level of COVID-19 Anxiety among Oncology Patients in Poland" International Journal of Environmental Research and Public Health 19, no. 18: 11418. https://doi.org/10.3390/ijerph191811418
APA StyleGrajek, M., Krupa-Kotara, K., Rozmiarek, M., Sobczyk, K., Działach, E., Górski, M., & Kobza, J. (2022). The Level of COVID-19 Anxiety among Oncology Patients in Poland. International Journal of Environmental Research and Public Health, 19(18), 11418. https://doi.org/10.3390/ijerph191811418