

Mindfulness-Based Intervention for the Reduction of Compassion Fatigue and Burnout in Nurse Caregivers of Institutionalized Older Persons with Dementia: A Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
1.1. Theoretical Framework
1.1.1. Compassion Fatigue
1.1.2. Mindfulness-Based Interventions (MBIs)
2. Materials and Methods
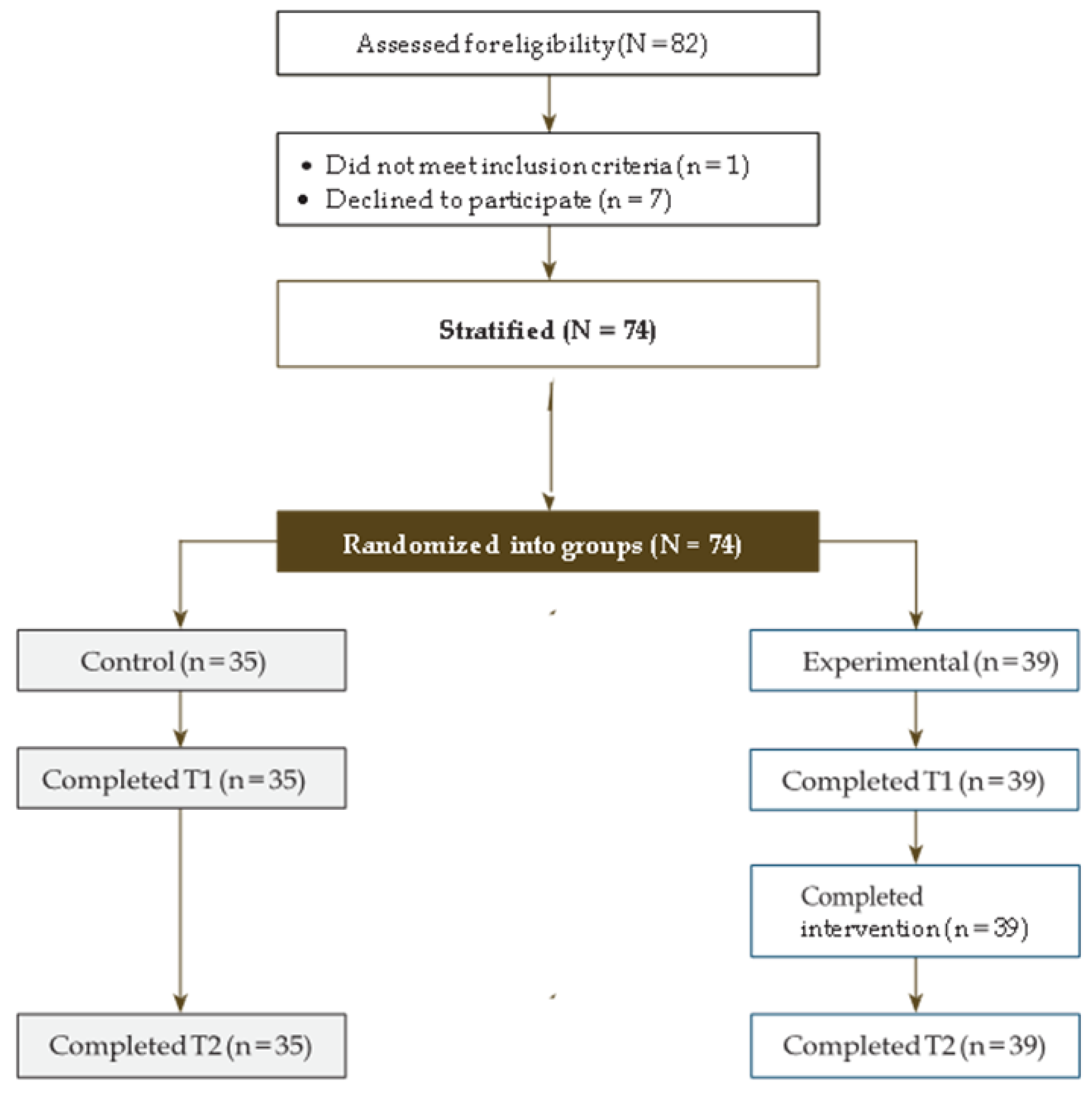
2.1. Participants
2.2. Variables
2.2.1. Dependent Variable
2.2.2. Independent Variables: Training Program
2.3. Outcome Measures
2.4. Intervention
2.5. Procedure
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kushal, A.; Gupta, S.; Mehta, M.; Singh, M.M. Study of stress among health care professionals: A systemic review. Int. J. Res. Found. Hosp. Healthc. Adm. 2018, 6, 6–11. [Google Scholar]
- Patel, R.S.; Bachu, R.; Adikey, A.; Malik, M.; Shah, M. Factors related to physician burnout and its consequences: A review. Behav. Sci. 2018, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Nepa, G.; Prout, T.A.; Albertini, F.; Marcelli, S.; Orrù, G.; Conversano, C. Stress, burnout, and resilience among healthcare workers during the COVID-19 emergency: The role of defense mechanisms. Int. J. Environ. Res. Public Health 2021, 18, 5258. [Google Scholar] [CrossRef]
- Bamonti, P.M.; Smith, A.; Smith, H.M. Cognitive emotion regulation strategies predict burnout in geriatric nursing staff. Clin. Gerontol. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Costello, H.; Walsh, S.; Cooper, C.; Livingston, G. A systematic review and meta-analysis of the prevalence and associations of stress and burnout among staff in long-term care facilities for people with dementia. Int. Psychogeriatr. 2019, 31, 1203–1216. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.R.; Han, E.K. Factors Affecting the Care Burden of Nurses Caring Elderly Patients with Dementia. J. Korean Acad. Community Health Nurs. 2019, 30, 368–376. [Google Scholar] [CrossRef]
- Potard, C.; Landais, C. Relationships between frustration intolerance beliefs, cognitive emotion regulation strategies and burnout among geriatric nurses and care assistants. Geriatr. Nurs. 2021, 42, 700–707. [Google Scholar] [CrossRef]
- Ursin, H.; Eriksen, H.R. The cognitive activation theory of stress. Psychoneuroendocrinology 2004, 29, 567–592. [Google Scholar] [CrossRef]
- Meurs, J.A.; Perrewé, P.L. Cognitive activation theory of stress: An integrative theoretical approach to work stress. J. Manag. 2011, 37, 1043–1068. [Google Scholar] [CrossRef]
- Steinheiser, M.M.; Crist, J.D.; Shea, K.D. Compassion fatigue among RNs working in skilled nursing facilities. Res. Gerontol. Nurs. 2020, 13, 320–328. [Google Scholar] [CrossRef]
- Joinson, C. Coping with compassion fatigue. Nursing 1992, 22, 116–122. [Google Scholar]
- Figley, C.R. Compassion fatigue: Psychotherapists’ chronic lack of self-care. J. Clin. Psychol. 2002, 58, 1433–1441. [Google Scholar] [CrossRef]
- Thorson-Olesen, S.J.; Meinertz, N.; Eckert, S. Caring for aging populations: Examining compassion fatigue and satisfaction. J. Adult Dev. 2019, 26, 232–240. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Zhang, C.; Han, X.R.; Li, W.; Wang, Y.L. Determinants of compassion satisfaction, compassion fatigue and burn out in nursing: A correlative meta-analysis. Medicine 2018, 97, e11086. [Google Scholar] [CrossRef]
- Ortega-Campos, E.; Vargas-Román, K.; Velando-Soriano, A.; Suleiman-Martos, N.; Cañadas-de la Fuente, G.A.; Albendín-García, L.; Gómez-Urquiza, J.L. Compassion fatigue, compassion satisfaction, and burnout in oncology nurses: A systematic review and meta-analysis. Sustainability 2019, 12, 72. [Google Scholar] [CrossRef]
- Lee, H.F.; Kuo, C.C.; Chien, T.W.; Wang, Y.R. A meta-analysis of the effects of coping strategies on reducing nurse burnout. Appl. Nurs. Res. 2016, 31, 100–110. [Google Scholar] [CrossRef]
- Bakker, A.B.; de Vries, J.D. Job Demands–Resources theory and self-regulation: New explanations and remedies for job burnout. Anxiety Stress Coping 2021, 34, 1–21. [Google Scholar] [CrossRef]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A systematic review and meta-analysis of the impact of mindfulness-based interventions on the well-being of healthcare professionals. Mindfulness 2019, 10, 1193–1216. [Google Scholar] [CrossRef]
- Britt, T.W.; Shuffler, M.L.; Pegram, R.L.; Xoxakos, P.; Rosopa, P.J.; Hirsh, E.; Jackson, W. Job demands and resources among healthcare professionals during virus pandemics: A review and examination of fluctuations in mental health strain during COVID-19. Appl. Psychol. 2021, 70, 120–149. [Google Scholar] [CrossRef]
- Kriakous, S.A.; Elliott, K.A.; Lamers, C.; Owen, R. The effectiveness of mindfulness-based stress reduction on the psychological functioning of healthcare professionals: A systematic review. Mindfulness 2021, 12, 1–28. [Google Scholar] [CrossRef]
- Donald, J.N.; Sahdra, B.K.; Van Zanden, B.; Duineveld, J.J.; Atkins, P.W.; Marshall, S.L.; Ciarrochi, J. Does your mindfulness benefit others? A systematic review and meta-analysis of the link between mindfulness and prosocial behaviour. Br. J. Psychol. 2019, 110, 101–125. [Google Scholar] [CrossRef] [PubMed]
- Malinowski, P. Mindfulness as psychological dimension: Concepts and applications. Ir. J. Psychol. 2008, 29, 155–166. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Lipworth, L.; Burney, R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J. Behav. Med. 1985, 8, 163–190. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Some reflections on the origins of MBSR, skillful means, and the trouble with maps. In Mindfulness; Routledge: London, UK, 2013; pp. 281–306. [Google Scholar]
- Moore, M.T.; Lau, M.A.; Haigh, E.A.; Willett, B.R.; Bosma, C.M.; Fresco, D.M. Association between decentering and reductions in relapse/recurrence in mindfulness-based cognitive therapy for depression in adults: A randomized controlled trial. J. Consult. Clin. Psychol. 2022, 90, 137. [Google Scholar] [CrossRef]
- Khoury, B.; Sharma, M.; Rush, S.E.; Fournier, C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J. Psychosom. Res. 2015, 78, 519–528. [Google Scholar] [CrossRef]
- Williams, M.; Penman, D. Mindfulness: A Practical Guide to Finding Peace in a Frantic World; Hachette UK: Paris, France, 2011. [Google Scholar]
- Duarte, R.; Lloyd, A.; Kotas, E.; Andronis, L.; White, R. Are acceptance and mindfulness-based interventions ‘value for money’? Evidence from a systematic literature review. Br. J. Clin. Psychol. 2019, 58, 187–210. [Google Scholar] [CrossRef]
- Fjorback, L.O.; Arendt, M.; Ørnbøl, E.; Fink, P.; Walach, H. Mindfulness-Based Stress Reduction and Mindfulness-Based Cognitive Therapy—A systematic review of randomized controlled trials. Acta Psychiatr. Scand. 2011, 124, 102–119. [Google Scholar] [CrossRef]
- Gu, J.; Strauss, C.; Bond, R.; Cavanagh, K. How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clin. Psychol. Rev. 2015, 37, 1–12. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef]
- Scheepers, R.A.; Emke, H.; Epstein, R.M.; Lombarts, K.M. The impact of mindfulness-based interventions on doctors’ well-being and performance: A systematic review. Med. Educ. 2020, 54, 138–149. [Google Scholar] [CrossRef]
- Howarth, A.; Smith, J.G.; Perkins-Porras, L.; Ussher, M. Effects of brief mindfulness-based interventions on health-related outcomes: A systematic review. Mindfulness 2019, 10, 1957–1968. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Riordan, K.M.; Sun, S.; Davidson, R.J. The empirical status of mindfulness-based interventions: A systematic review of 44 meta-analyses of randomized controlled trials. Perspect. Psychol. Sci. 2022, 17, 108–130. [Google Scholar] [CrossRef]
- Sulosaari, V.; Unal, E.; Cinar, F.I. The effectiveness of mindfulness-based interventions on the psychological well-being of nurses: A systematic review. Appl. Nurs. Res. 2022, 64, 151565. [Google Scholar] [CrossRef]
- Armstrong, J.W.; Turne, L.N. Mindfulness-based interventions to reduce stress and burnout in nurses: An integrative review. Br. J. Ment. Health Nurs. 2022, 11, 1–11. [Google Scholar] [CrossRef]
- Bartlett, L.; Martin, A.; Neil, A.L.; Memish, K.; Otahal, P.; Kilpatrick, M.; Sanderson, K. A systematic review and meta-analysis of workplace mindfulness training randomized controlled trials. J. Occup. Health Psychol. 2019, 24, 108. [Google Scholar] [CrossRef]
- Stamm, H.B. Professional Quality of Life Measure: Compassion, Satisfaction, and Fatigue Version 5 (ProQOL). 2009. Available online: https://proqol.org/proqol-manual (accessed on 15 June 2022).
- Morante Benadero, M.; Moreno Jiménez, B.; Rodríguez Muñoz, A. Professional Satisfaction and Fatigue Subscales-version IV (ProQOL). Traducción del Instrumento de Evaluación al Español; Universidad Autónoma de Madrid: Madrid, Spain, 2006. [Google Scholar]
- Hemsworth, D.; Baregheh, A.; Aoun, S.; Kazanjian, A. A critical enquiry into the psychometric properties of the professional quality of life scale (ProQol-5) instrument. Appl. Nurs. Res. 2018, 39, 81–88. [Google Scholar] [CrossRef]
- Hotchkiss, J.T.; Wong, M.Y.C. Factorial Structure of the ProQOL—Systematic Meta-analysis and Integration of 27 International Factor Analysis Studies. Trends Psychol. 2022, 1–32. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Meditation is not what you think. Mindfulness 2021, 12, 784–787. [Google Scholar] [CrossRef]
- Wagh-Gumaste, S. Influence of Hindu Spiritual Teachers on Mindfulness-Based Stress Reduction (MBSR) of Jon Kabat-Zinn: Focusing on the Teachings of Sri Nisargadatta Maharaj and Sri Ramana Maharshi. Int. J. South Asian Stud. 2022, 12, 1–18. [Google Scholar]
- Zou, H.; Cao, X.; Chair, S.Y. A systematic review and meta-analysis of mindfulness-based interventions for patients with coronary heart disease. J. Adv. Nurs. 2021, 77, 2197–2213. [Google Scholar] [CrossRef]
- Querstret, D.; Morison, L.; Dickinson, S.; Cropley, M.; John, M. Mindfulness-based stress reduction and mindfulness-based cognitive therapy for psychological health and well-being in nonclinical samples: A systematic review and meta-analysis. Int. J. Stress Manag. 2020, 27, 394. [Google Scholar] [CrossRef]
- Wong, S.; Chan, J.Y.; Zhang, D.; Lee, E.K.; Tsoi, K.K. The safety of mindfulness-based interventions: A systematic review of randomized controlled trials. Mindfulness 2018, 9, 1344–1357. [Google Scholar] [CrossRef]
- Alagamy, Z.; Metwaly, S.M.; Zaki, S.M.; Mohammed, R.F. Fear of COVID-19, Nurse’s Stress, and Health Care Behaviors toward Elderly People. NILES J. Geriatr. Gerontol. 2022, 5, 64–81. [Google Scholar] [CrossRef]
- Dincer, B.; Inangil, D. The effect of Emotional Freedom Techniques on nurses’ stress, anxiety, and burnout levels during the COVID-19 pandemic: A randomized controlled trial. Explore 2021, 17, 109–114. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the COVID-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Belton, S. Caring for the caregivers: Making the case for mindfulness-based wellness programming to support nurses and prevent staff turnover. Nurs. Econ. 2018, 36, 191–195. [Google Scholar]
- Singh, N.N.; Lancioni, G.E.; Medvedev, O.N.; Myers, R.E.; Chan, J.; McPherson, C.L.; Kim, E. Comparative effectiveness of caregiver training in mindfulness-based positive behavior support (MBPBS) and positive behavior support (PBS) in a randomized controlled trial. Mindfulness 2018, 1–13. [Google Scholar] [CrossRef]
- Baker, C.; Huxley, P.; Dennis, M.; Islam, S.; Russell, I. Alleviating staff stress in care homes for people with dementia: Protocol for stepped-wedge cluster randomised trial to evaluate a web-based Mindfulness-Stress Reduction course. BMC Psychiatry 2015, 15, 317. [Google Scholar] [CrossRef]
- Klein, A.; Taieb, O.; Xavier, S.; Baubet, T.; Reyre, A. The benefits of mindfulness-based interventions on burnout among health professionals: A systematic review. Explore 2020, 16, 35–43. [Google Scholar] [CrossRef]
- Mantzorou, M.; Koukia, E. Professional burnout of geriatric nurses caring for elderly people with dementia. Perioper. Nurs. -Q. Sci. Online Off. J. GORNA 2018, 6–26. [Google Scholar] [CrossRef]
- Gilbert, J.; Ward, L.; Walter, R. A labour of love: Reward and satisfaction for nurses: Findings from a grounded theory study in dementia care. Dementia 2021, 20, 1697–1710. [Google Scholar] [CrossRef] [PubMed]
- Teitominaga, M.; Nakanishi, M. Factors of feelings of happiness at work among staff in geriatric care facilities. Geriatr. Gerontol. Int. 2021, 21, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Marotta, M.; Gorini, F.; Parlanti, A.; Berti, S.; Vassalle, C. Effect of Mindfulness-Based Stress Reduction on the Well-Being, Burnout and Stress of Italian Healthcare Professionals during the COVID-19 Pandemic. J. Clin. Med. 2022, 11, 3136. [Google Scholar] [CrossRef]
- Watts, K.J.; O’Connor, M.; Johnson, C.E.; Breen, L.J.; Kane, R.T.; Choules, K.; Doyle, C.; Buchanan, G.; Yuen, K. Mindfulness-based compassion training for health professionals providing end-of-life care: Impact, feasibility, and acceptability. J. Palliat. Med. 2021, 24, 1364–1374. [Google Scholar] [CrossRef] [PubMed]
- Wasson, R.S.; Barratt, C.; O’Brien, W.H. Effects of mindfulness-based interventions on self-compassion in health care professionals: A meta-analysis. Mindfulness 2020, 11, 1914–1934. [Google Scholar] [CrossRef] [PubMed]
- Bluth, K.; Lathren, C.; Silbersack Hickey, J.V.; Zimmerman, S.; Wretman, C.J.; Sloane, P.D. Self-compassion training for certified nurse assistants in nursing homes. J. Am. Geriatr. Soc. 2021, 69, 1896–1905. [Google Scholar] [CrossRef] [PubMed]
- Masiero, M.; Cutica, I.; Russo, S.; Mazzocco, K.; Pravettoni, G. Psycho-cognitive predictors of burnout in healthcare professionals working in emergency departments. J. Clin. Nurs. 2018, 27, 2691–2698. [Google Scholar] [CrossRef] [PubMed]
- Lubbadeh, T. Job burnout: A general literature review. Int. Rev. Manag. Mark. 2020, 10, 7. [Google Scholar] [CrossRef]
- Brodaty, H.; Draper, B.; Low, L.F. Nursing home staff attitudes towards residents with dementia: Strain and satisfaction with work. J. Adv. Nurs. 2003, 44, 583–590. [Google Scholar] [CrossRef]
- McPherson, S.; Hiskey, S.; Alderson, Z. Distress in working on dementia wards-A threat to compassionate care: A grounded theory study. Int. J. Nurs. Stud. 2016, 53, 95–104. [Google Scholar] [CrossRef]
- Spinelli, C.; Wisener, M.; Khoury, B. Mindfulness training for healthcare professionals and trainees: A meta-analysis of randomized controlled trials. J. Psychosom. Res. 2019, 120, 29–38. [Google Scholar] [CrossRef]
- Stratton, E.; Lampit, A.; Choi, I.; Calvo, R.A.; Harvey, S.B.; Glozier, N. Effectiveness of eHealth interventions for reducing mental health conditions in employees: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189904. [Google Scholar] [CrossRef]
- Young, C.C.; Kesler, S.; Walker, V.G.; Johnson, A.; Harrison, T.C. An Online Mindfulness-based Intervention for Certified Nursing Assistants in Long-term Care. J. Holist. Nurs. 2022. [Google Scholar] [CrossRef]
- Suleiman-Martos, N.; Gomez-Urquiza, J.L.; Aguayo-Estremera, R.; Cañadas-De La Fuente, G.A.; De La Fuente-Solana, E.I.; Albendín-García, L. The effect of mindfulness training on burnout syndrome in nursing: A systematic review and meta-analysis. J. Adv. Nurs. 2020, 76, 1124–1140. [Google Scholar] [CrossRef]
- Kor, P.P.K.; Liu, J.Y.W.; Chien, W.T. Effects of a modified mindfulness-based cognitive therapy for family caregivers of people with dementia: A pilot randomized controlled trial. Int. J. Nurs. Stud. 2019, 98, 107–117. [Google Scholar] [CrossRef]
- Zhang, D.; Lee, E.K.; Mak, E.C.; Ho, C.Y.; Wong, S.Y. Mindfulness-based interventions: An overall review. Br. Med. Bull. 2021, 138, 41–57. [Google Scholar] [CrossRef]
- De Witt, L.; Ploeg, J. Caring for older people living alone with dementia: Healthcare professionals’ experiences. Dementia 2016, 15, 221–238. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Experimental (n = 39) | Control (n = 35) | p * | ||
|---|---|---|---|---|---|
| M (SD) | Range | M (SD) | Range | ||
| Professional Quality of Life ProQoL (0–50) | |||||
| Satisfaction | 40.49 (7.22) | 29–50 | 41.25 (5.02) | 11–50 | 0.087 |
| Compassion fatigue | 16.44 (4.45) | 2–30 | 17.45 (7.12) | 2–47 | 0.065 |
| Burnout | 17.88 (7.33) | 8–28 | 18.38 (4.05) | 4–34 | 0.074 |
| Model | R2 | R2 Change | Variable | Standardized β | p |
|---|---|---|---|---|---|
| ProQOL: Compassion satisfaction | |||||
| 1 | 0.45 | 0.45 | <0.001 | ||
| Time | 0.62 | <0.001 | |||
| 2 | 0.50 | 0.11 | <0.001 | ||
| Exp. vs. control | 0.31 | <0.001 | |||
| ProQOL: Compassion fatigue | |||||
| 1 | 0.40 | 0.40 | <0.001 | ||
| Time | −0.61 | <0.001 | |||
| 2 | 0.61 | 0.16 | <0.001 | ||
| Exp. vs. control | −0.69 | <0.001 | |||
| ProQOL: Burnout | |||||
| 1 | 0.38 | 0.37 | <0.001 | ||
| Time | −0.60 | <0.001 | |||
| 2 | 0.44 | 0.11 | <0.001 | ||
| Exp. vs. control | −0.32 | <0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez, V.; Menéndez-Crispín, E.J.; Sarabia-Cobo, C.; de Lorena, P.; Fernández-Rodríguez, A.; González-Vaca, J. Mindfulness-Based Intervention for the Reduction of Compassion Fatigue and Burnout in Nurse Caregivers of Institutionalized Older Persons with Dementia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 11441. https://doi.org/10.3390/ijerph191811441
Pérez V, Menéndez-Crispín EJ, Sarabia-Cobo C, de Lorena P, Fernández-Rodríguez A, González-Vaca J. Mindfulness-Based Intervention for the Reduction of Compassion Fatigue and Burnout in Nurse Caregivers of Institutionalized Older Persons with Dementia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(18):11441. https://doi.org/10.3390/ijerph191811441
Chicago/Turabian StylePérez, Victoria, Ernesto J. Menéndez-Crispín, Carmen Sarabia-Cobo, Pablo de Lorena, Angela Fernández-Rodríguez, and Julia González-Vaca. 2022. "Mindfulness-Based Intervention for the Reduction of Compassion Fatigue and Burnout in Nurse Caregivers of Institutionalized Older Persons with Dementia: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 18: 11441. https://doi.org/10.3390/ijerph191811441