
Intergenerational Theater Workshops as Unique Recreational Activities among Older Adults in Japanese Care Facilities: A Qualitatively Driven Mixed-Methods Multiple-Case Study Design
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
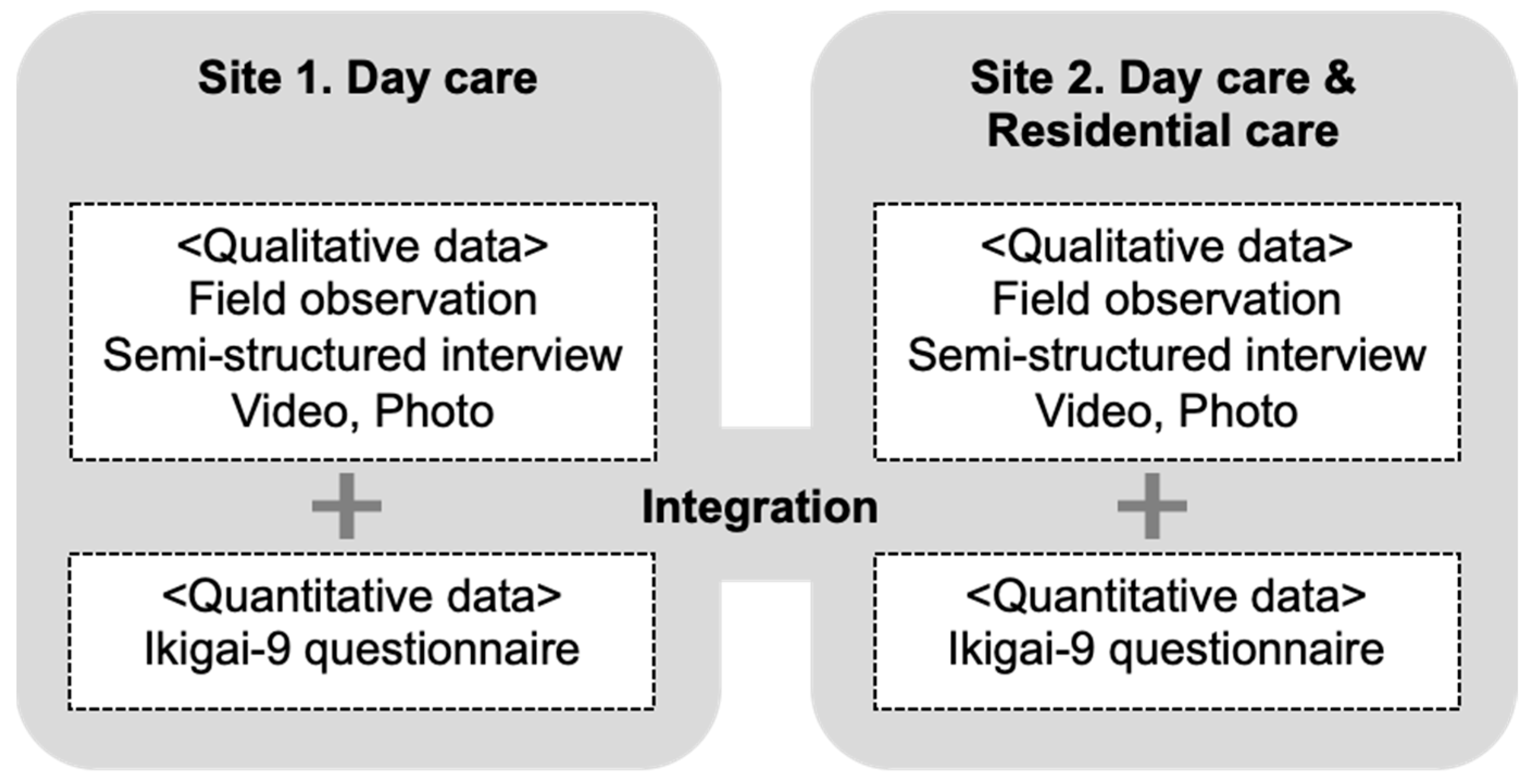
2.1. Study Design
2.2. Description of the Theater Workshop and the Provider
2.3. Selection of the Study Site and Participant Recruitment
2.4. Data Collection Instrument and the Procedure
2.4.1. Field Observation of the Workshop
2.4.2. Semi-Structured Interview of Care Provider
2.4.3. Pre–Post Changes on the Well-Being Survey Using Ikigai-9 Scales for Older Participants
2.4.4. Ethical Considerations
2.4.5. Data Analysis
3. Results
3.1. Description of the Site and Study Participants
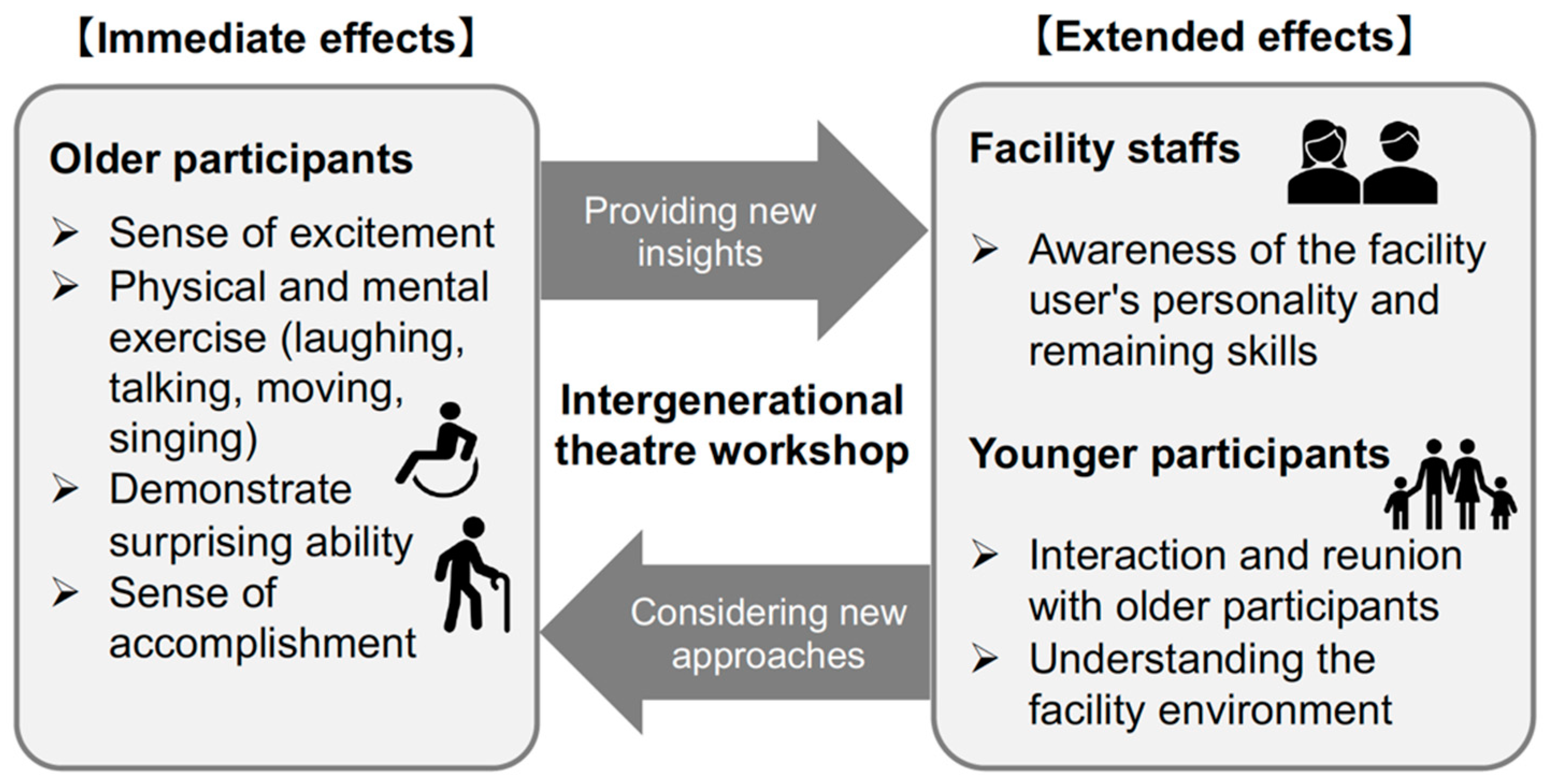
3.2. Research Question 1: How Will the Intergenerational Theater Workshop Affect the Participants?
3.2.1. Immediate Effects
3.2.2. Extended Effects
3.3. Research Question 2: Will the Workshop Improve Older Participants’ Well-Being?
3.4. Research Question 3: Under What Circumstances Would It Be More Effective for Older Participants’ Well-Being?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. The Growing Need for Long-Term Care Assumptions and Realities. Available online: https://www.un.org/development/desa/ageing/news/2016/09/briefing-paper-growing-need-for-long-term-care-assumptions-and-realities/ (accessed on 4 September 2022).
- World Health Organization. Decade of Healthy Aging 2020–2030. Available online: https://www.who.int/initiatives/decade-of-healthy-ageing (accessed on 4 September 2022).
- Gerritsen, D.L. Well-being in long-term care: An ode to vulnerability. Aging Ment. Health 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Well-Being Concept. Available online: https://www.cdc.gov/hrqol/wellbeing.htm (accessed on 4 September 2022).
- National Institute for Health and Care Excellence. Mental Wellbeing of Older People in Care Homes. Available online: www.nice.org.uk/guidance/qs50 (accessed on 4 September 2022).
- Maeda, N. A study on Quality of Life and Quality of Care for Older Adults with Care Needs—An Intervention Study of the Quality of Life care model; NLI Research Institute Report; NLI Research Institute: Tokyo, Japan, 2008; Volume 50, pp. 91–126. [Google Scholar]
- Irving, J.; Davis, S.; Collier, A. Aging with purpose: Systematic search and review of literature pertaining to older adults and purpose. Int. J. Aging Hum. Dev. 2017, 85, 403–437. [Google Scholar] [CrossRef] [PubMed]
- Fancourt, D.; Finn, S. What Is the Evidence on the Role of the Arts in Improving Health and Well-Being? A Scoping Review; WHO Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Jenkins, L.K.; Farrer, R.; Aujla, I.J. Understanding the impact of an intergenerational arts and health project: A study into the psychological well-being of participants, carers and artists. Public Health 2021, 194, 121–126. [Google Scholar] [CrossRef]
- Groot, B.; de Kock, L.; Liu, Y.; Dedding, C.; Schrijver, J.; Teunissen, T.; van Hartingsveldt, M.; Menderink, J.; Lengams, Y.; Lindenberg, J.; et al. The value of active arts engagement on health and well-being of older adults: A nation-wide participatory study. Int. J. Environ. Res. Public Health 2021, 18, 8222. [Google Scholar] [CrossRef] [PubMed]
- Martins, T.; Midão, L.; Martínez Veiga, S.; Dequech, L.; Busse, G.; Bertram, M.; McDonald, A.; Gilliland, G.; Orte, C.; Vives, M.; et al. Intergenerational programs review: Study design and characteristics of intervention, outcomes, and effectiveness. J. Intergener. Relatsh. 2019, 17, 93–109. [Google Scholar] [CrossRef]
- Gualano, M.R.; Voglino, G.; Bert, F.; Thomas, R.; Camussi, E.; Siliquini, R. The impact of intergenerational programs on children and older adults: A review. Int. Psychogeriatr. 2018, 30, 451–468. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, P.; Westberg, K.; Gustafson, D. Effect of participation in an intergenerational theater production. J. Intergener. Relatsh. 2022, 20, 183–198. [Google Scholar] [CrossRef]
- Anderson, S.; Fast, J.; Keating, N.; Eales, J.; Chivers, S.; Barnet, D. Translating knowledge. Health Promot. Pract. 2017, 18, 15–25. [Google Scholar] [CrossRef]
- Dassa, A.; Harel, D. People with dementia as ‘spect-actors’ in a musical theatre group with performing arts students from the community. Arts Psychother. 2019, 65, 101592. [Google Scholar] [CrossRef]
- Dassa, A.; Harel, D. Side-by-side on stage—Music and drama form a bridge between acting students and people with dementia in an intergenerational group work. J. Intergener. Relatsh. 2020, 18, 17–30. [Google Scholar] [CrossRef]
- Bernard, M.; Rickett, M. The cultural value of older people’s experiences of theater-making: A review. Gerontologist 2017, 57, e1–e26. [Google Scholar] [CrossRef] [PubMed]
- McCormick, S. Perspectives on Practice: Applied Theatre and Aging. In Applied Theatre: Creative Ageing, 1st ed.; Bloomsbury Publishing Plc: London, UK, 2017. [Google Scholar]
- Harries, B. The Storybox Project. In Examining the Role of a Theatre and Arts-Based Intervention for People with Dementia; Library Theatre Company: Manchester, UK, 2013. [Google Scholar]
- Nicholson, H. Summative Evaluation of Hearts and Minds. A Three Year Pilot Programme by Age Exchange Theatre Trust; Royal Holloway University of London: London, UK, 2013. [Google Scholar]
- Fritsch, T.; Kwak, J.; Grant, S.; Lang, J.; Montgomery, R.R.; Basting, A.D. Impact of TimeSlips, a creative expression intervention program, on nursing home residents with dementia and their caregivers. Gerontologist 2009, 49, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Zeilig, H.; Killick, J.; Fox, C. The participative arts for people living with a dementia: A critical review. Int. J. Ageing Later Life 2014, 9, 7–34. [Google Scholar] [CrossRef]
- Bellazzecca, E.; Teasdale, S.; Biosca, O.; Skelton, D.A. The health impacts of place-based creative programmes on older adults’ health: A critical realist review. Health Place 2022, 76, 102839. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Labor And Welfare, Summary of the Survey on Nursing Care Benefits and Other Costs. In 2017; p 4. (In Japanese). Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kaigo/kyufu/17/dl/11.pdf (accessed on 1 August 2022).
- Furuichi, T.; Kim, M. Recreation in nursing homes and its challenges (in Japanese). Int. J. Hum. Cult. Stud. 2020, 2020, 194–201. [Google Scholar] [CrossRef]
- Oshita, Y. Cultural policies for creative aging. Q. J. Public Policy Manag. 2016, 4, 85–128. (In Japanese) [Google Scholar]
- Sonobe, Y. Development of theatre activities involving older people: Analysis of newspaper articles in Japan. J. JSTR 2015, 60, 47–67. (In Japanese) [Google Scholar]
- Yoshimoto, M. The potential of art to draw out the capability of the elderly—The possibility of art for a super-aging society. Gerontol. J. 2011, 11, 1–15. (In Japanese) [Google Scholar]
- Watanabe, N.; Okazaki, K.; Gyo, R.; Watanabe, K.; Inoue, M. Potential of multi-generational theatrical workshops toward the creation of sustainable multi-generational communities. J. Jpn. Assoc. Health Commun. 2018, 9, 1–16. (In Japanese) [Google Scholar]
- Yin, R.K. Designing case studies. In Case study Research and Applications—Design and Methods, 6th ed.; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2018; pp. 47–78. [Google Scholar]
- Fàbregues, S.; Fetters, M.D. Fundamentals of case study research in family medicine and community health. Fam. Med. Community Health 2019, 7, e000074. [Google Scholar] [CrossRef]
- Kaushik, V.; Walsh, C.A. Pragmatism as a research paradigm and its implications for social work research. Soc. Sci. 2019, 8, 255. [Google Scholar] [CrossRef]
- Fido, D.; Kotera, Y.; Asano, K. English translation and validation of the Ikigai-9 in a UK sample. Int. J. Ment. Health Addict. 2020, 18, 1352–1359. [Google Scholar] [CrossRef]
- Imai, T.; Osada, H.; Nishimura, Y. The reliability and validity of a new scale for measuring the concept of Ikigai (Ikigai-9). Jpn. J. Public Health 2012, 59, 433–439. (In Japanese) [Google Scholar]
- Basting, A.D. Creative Care, 1st ed.; HarperOne: New York, NY, USA, 2020. [Google Scholar]
- Patton, M.Q. Qualitative Research and Evaluation Methods, 4th ed.; SAGE Publications, Inc.: London, UK, 2015. [Google Scholar]
- Fetters, M.D.; Rubinstein, E.B. The 3 Cs of content, context, and concepts: A practical approach to recording unstructured field observations. Ann. Fam. Med. 2019, 17, 554–560. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health Labor and Welfare, Report of the Study Group on New Rehabilitation Methods for the Elderly in the Community (In Japanese). In 2015. Available online: https://www.mhlw.go.jp/stf/shingi2/0000081906.html (accessed on 1 August 2022).
- Ministry of Health Labor and Welfare, Report of the Study Group on New Rehabilitation Methods for the Elderly in the Community (In Japanese). In 2020. Available online: https://www.mhlw.go.jp/stf/newpage_12394.html (accessed on 1 August 2022).
- Swinnen, A.; De Medeiros, K. “Play” and people living with dementia: A humanities-based inquiry of TimeSlips and the Alzheimer’s Poetry Project. Gerontologist 2018, 58, 261–269. [Google Scholar] [CrossRef]
- Sonobe, Y. Improvisational theatre learning forms and the transformation of older people: A case study of the Kururu Improvisational Theatre Company in Chiba. Jpn. J. Gerontol. 2017, 39, 21–30. (In Japanese) [Google Scholar]
- Gyo, R.; Suzuki, S.; Suenaga, E. A study of translating drama workshops into the policy. Policy Pract. Stud. 2016, 2, 203–209. (In Japanese) [Google Scholar]
- Takiguchi, M. The present conditions and problem of the therapeutic recreation in the elderly person welfare institution -Than a viewpoint of the life support in the social work. J. Health Soc. Welf. Sci. Nishikyushu Univ. 2019, 48, 27–38. (In Japanese) [Google Scholar]
- Evans, S.C.; Garabedian, C.; Bray, J.; Gray, K. Challenges and enablers for creative arts practice in care homes. J. Appl. Arts Health 2019, 10, 333–345. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Session | Activity Contents |
|---|---|
| 1 | Creating a nickname and a name tag for each participant Self-introduction and communication games Brief introduction of the play’s storyline |
| 2 | Greetings and communication games Casting proposal Play practices led by facilitators and creation of a story outline |
| 3 | Greetings and communication games Play practice (whole group) and with small, break-out groups |
| 4 | Greetings and communication games Play rehearsal (run through) Performance in front of the audience Sharing impressions |
| Site 1 | Site 2 | Reference | |
|---|---|---|---|
| Number of older participants signed up for the workshop | |||
| 11 | 16 | ||
| Average age | |||
| 86.4 ± 3.3 (82–91) | 87.0 ± 8.0 (70–98) | ||
| Gender | |||
| Male | 1 | 4 | |
| Female | 10 | 12 | |
| Day care use or resident | |||
| Day care | 11 | 8 | |
| Resident | 8 | ||
| Certification of needed support/long-term care need * | |||
| Independent | 2 | ||
| Support level 1 | Needs some support for task-based activities in daily life | ||
| Support level 2 | 1 | ||
| Care level 1 | 2 | 5 | Difficulty in performing essential daily life activities by himself/herself |
| Care level 2 | 6 | 4 | |
| Care level 3 | 1 | 2 | Requires almost constant care |
| Care level 4 | 1 | 3 | Faces difficulty living without constant care |
| Care level 5 | Requires almost constant care to live | ||
| Level of independent living based on the physical ability * | |||
| Independent | 6 | 4 | |
| A1 | 2 | 4 | Needs support to go outside |
| A2 | 2 | 6 | |
| B1 | 1 | Requires assistance for mobility in a house | |
| B2 | 2 | ||
| C2 | Mostly staying in bed | ||
| C3 | |||
| Level of independent living based on the cognitive ability * | |||
| Independent | 1 | 2 | |
| I | 1 | Mildly demented but can mostly live independently | |
| II a | 8 | Can live independently with someone’s support | |
| II b | 7 | 5 | |
| III a | 2 | 1 | Difficulty in behavior and communication, which necessitates care |
| III b | |||
| IV | Frequent issues in behavior and need for constant care | ||
| M | Needs specialized medical care | ||
| Site 1 | Site 2 | ||||||
|---|---|---|---|---|---|---|---|
| Number of Respondents Who Answered Both in Pre- and Post-Workshop | n = 10 | n = 8 | |||||
| Ikigai-9 scale of older participants: Wilcoxon signed-rank test of pre- and post-workshop | Average age | 86.7 ± 3.3 (82–91) | 87.6 ± 9.5 (70–98) | ||||
| Certified care level | Support level 2–Care level 4 | Independent–Care level 4 | |||||
| Items: Ikigai-9 Scale | Pre * | Post * | p ** | Pre * | Post * | p ** | |
| Total score (9–45 point) | 30.00 (7.45) | 33.22 (5.72) | 0.042 | 31.25 (9.62) | 34.38 (8.45) | 0.108 | |
| I. Emotions towards one’s life (3–15 point) | 9.30 (3.47) | 13.00 (1.56) | 0.020 | 11.25 (3.77) | 12.88 (2.48) | 0.168 | |
| (1) I often feel that I am happy. (1–5 point) | 3.30 (1.25) | 4.60 (0.52) | 0.017 | 3.75 (1.58) | 4.25 (1.04) | 0.461 | |
| (4) I have room in my mind. (1–5 point) | 2.80 (1.40) | 4.00 (1.05) | 0.066 | 4.00 (1.07) | 4.38 (0.92) | 0.083 | |
| (7) My life is mentally rich and fulfilled. (1–5 point) | 3.20 (1.32) | 4.40 (0.52) | 0.027 | 3.50 (1.51) | 4.25 (1.04) | 0.167 | |
| II. Attitudes towards one’s future (3–15 point) | 11.44 (2.46) | 11.44 (2.01) | 1.000 | 10.50 (3.46) | 10.88 (3.44) | 0.590 | |
| (2) I would like to learn something new or start something. (1–5 point) | 3.89 (1.27) | 3.56 (1.01) | 0.438 | 3.38 (1.51) | 3.38 (1.51) | 1.000 | |
| (5) I am interested in many things. (1–5 point) | 3.40 (1.43) | 4.60 (0.70) | 0.016 | 3.88 (1.13) | 4.25 (1.04) | 0.083 | |
| (8) I would like to develop myself. (1–5 point) | 4.30 (0.48) | 3.50 (1.65) | 0.102 | 3.25 (1.28) | 3.25 (1.49) | 0.861 | |
| III. The acknowledgement of one’s existence (3–15 point) | 9.78 (3.23) | 8.78 (3.15) | 0.202 | 9.50 (3.12) | 10.63 (3.85) | 0.320 | |
| (3) I feel that I am contributing to someone or the society. (1–5 point) | 3.60 (1.51) | 3.10 (1.37) | 0.096 | 2.75 (1.49) | 3.63 (1.30) | 0.168 | |
| (6) I think that my existence is needed by something or someone. (1–5 point) | 3.60 (1.51) | 3.30 (1.16) | 0.579 | 3.25 (1.28) | 3.75 (1.58) | 0.194 | |
| (9) I believe that I have some impact on someone. (1–5 point) | 2.89 (1.17) | 2.67 (1.32) | 0.516 | 3.50 (1.14) | 3.25 (1.28) | 0.683 | |
| Qualitative data of implementation environment | Younger participants | 3 to 4 Adults (30s and 40s) who responded through workshop providers’ social networks, and 3 to 4 children (3 to 11 years old). | 3 to 11 Neighborhood volunteers who belongs to a local amateur theater group and a public consumer center (40 s to 70 s). | ||||
| Facility staff | The facility manager remained in the room, other staff came in and out, most of them saw the final performance. | 2 to 4 staff attended the workshop site and enthusiastically supported the participation of the facility users. | |||||
| Relationship of the facility and the workshop provider | Second time to conduct theater workshops. The facility is in the same city as the workshop providers’ base. | First time to conduct theater workshops. The facility is in the different region to the workshop providers’ base. | |||||
| Meta-inference | Implications for improving the effectiveness of the activity, obtained from a comparison of the two sites. | -May be more challenging to satisfy everyone when the participants’ cognitive and physical conditions are more varied. - Continuity of the activity could create relax atmosphere among the participants, and for the facilitator’s ability of program arrangement. - Children’s participation may have more direct impact on present well-being for older participants. The benefit of adults’ participants may take a little longer to find an impact. - The facility staff may need to explore a balance between supporting and waiting to give older participants some space to display their ability. | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abe, M.; Gyo, R.; Shibata, J.; Okazaki, K.; Inoue, R.; Oishi, T.; Inoue, M. Intergenerational Theater Workshops as Unique Recreational Activities among Older Adults in Japanese Care Facilities: A Qualitatively Driven Mixed-Methods Multiple-Case Study Design. Int. J. Environ. Res. Public Health 2022, 19, 11474. https://doi.org/10.3390/ijerph191811474
Abe M, Gyo R, Shibata J, Okazaki K, Inoue R, Oishi T, Inoue M. Intergenerational Theater Workshops as Unique Recreational Activities among Older Adults in Japanese Care Facilities: A Qualitatively Driven Mixed-Methods Multiple-Case Study Design. International Journal of Environmental Research and Public Health. 2022; 19(18):11474. https://doi.org/10.3390/ijerph191811474
Chicago/Turabian StyleAbe, Michiko, Ren Gyo, Junro Shibata, Kentaro Okazaki, Rumiko Inoue, Tatsuki Oishi, and Machiko Inoue. 2022. "Intergenerational Theater Workshops as Unique Recreational Activities among Older Adults in Japanese Care Facilities: A Qualitatively Driven Mixed-Methods Multiple-Case Study Design" International Journal of Environmental Research and Public Health 19, no. 18: 11474. https://doi.org/10.3390/ijerph191811474