

‘Next Stop: Mum’: Evaluation of a Postpartum Depression Prevention Strategy in Poland


Abstract
1. Introduction
1.1. Pilot National Program
The Aim of the Study
2. Materials and Methods
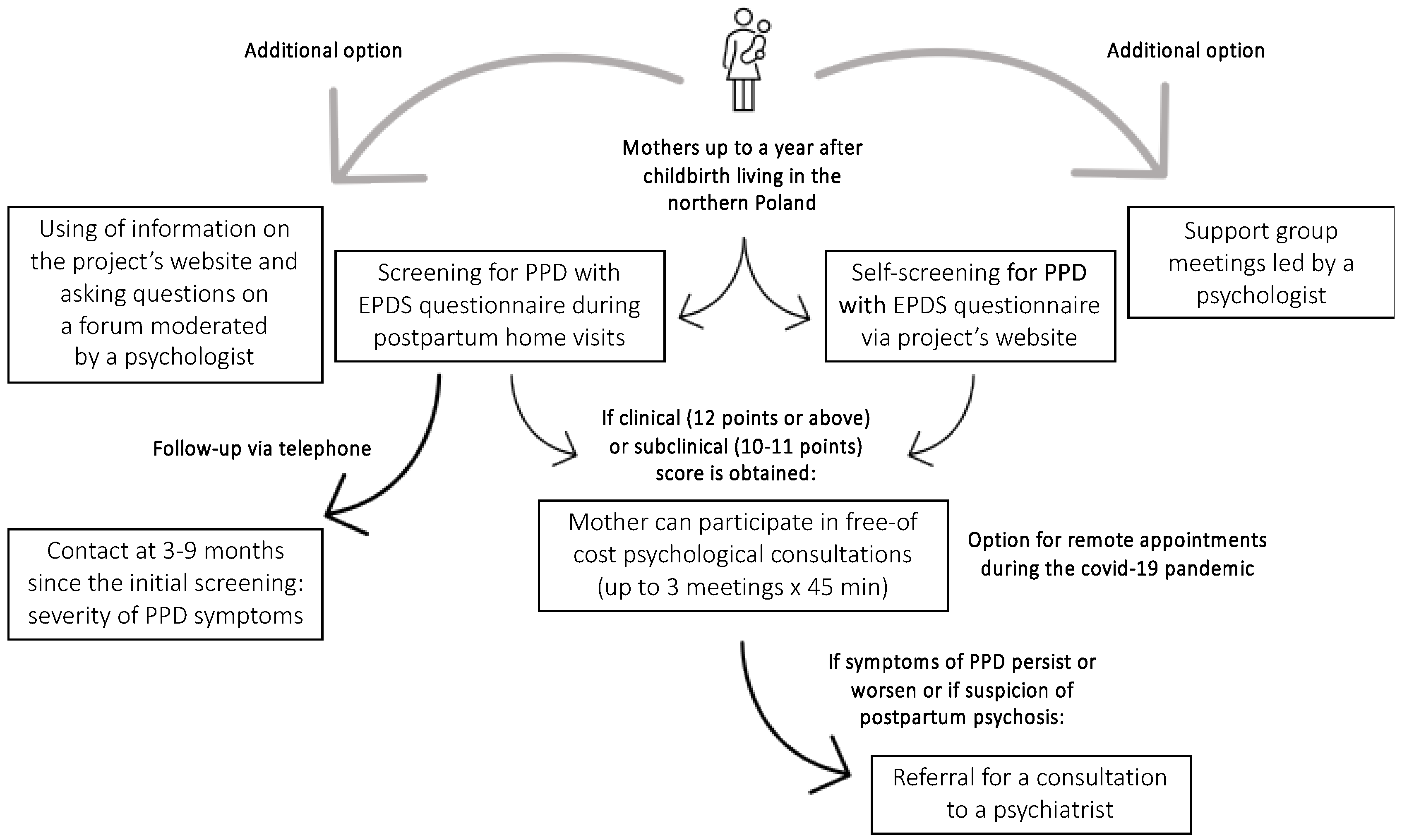
2.1. Study Design
2.1.1. Education of Health Care Professionals (Mainly Midwives, Nurses, and Physicians in Primary Healthcare Settings)
2.1.2. Educational and Information Campaigns
2.1.3. Screening and Follow Up
2.1.4. Consultations with Psychologists
2.2. Setting
2.3. Measurement Tools
2.3.1. Edinburgh Postnatal Depression Scale
2.3.2. Sociodemographic Survey
2.3.3. The Modified Version of the Test of Antenatal and Postpartum Depression Knowledge
2.3.4. Psychological Consultation Cards
2.4. Compliance with Ethical Standards
Ethics Approval and Consent to Participate
3. Results
3.1. Screening for PPD
3.2. Follow-Up
3.3. Education of Health Care Professionals
3.4. Psychological Consultations
4. Discussion
4.1. PPD Screening Procedures
4.2. Education of Health Care Professionals
4.3. Psychological Consultations
5. Conclusions
- (1)
- The discrepancy in EPDS results in face-to-face contact and on the online platform: 7.3% versus 77%.
- (2)
- A lower number of women achieved higher scores in face-to-face contact (7.3% versus 15% expected).
- (3)
- The online screening raises much more interest than expected: the number of women participating in the online survey turned out to be almost twice as high as we assumed when planning the project (in the halfway: 10,454; we expected 6000 in total). Therefore, as disclosing complete information about mental state in contact with the nurse/midwife may be influenced by self-stigma, the possibility of performing an anonymous self-examination with clear guidance on further treatment steps is recommended.
- (4)
- As the initial screening score provided in direct contact increased by 55% of women, it is justified and highly recommended to extend the PPD screening period (Polish recommendations apply only to the first six weeks postpartum).
- (5)
- The number of psychological consultations was lower than expected. However, with a lower rate of EPDS score > 12, the referral rate of 26% of women was almost twice as large as we assumed at the beginning of the project.
- (6)
- Although the training concerning perinatal mental health contributes to increased knowledge about PPD, the awareness of the seriousness of this disorder is still low.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Melvaer, L.B.; Videbech, P.; Lamont, R.F.; Joergensen, J.S. Risk factors for developing post-traumatic stress disorder following childbirth: A systematic review. Actabstetriciana Et Gynecol. Scand. 2012, 91, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.R.; Fawcett, J.M. The Prevalence of Anxiety Disorders During Pregnancy and the Postpartum Period: A Multivariate Bayesian Meta-Analysis. J. Clin. Psychiatry 2019, 80, 18r12527. [Google Scholar] [CrossRef] [PubMed]
- Hahn-Holbrook, J.; Cornwell-Hinrichs, T.; Anaya, I. Economic and Health Predictors of National Postpartum Depression Prevalence: A Systematic Review, Meta-analysis, and Meta-Regression of 291 Studies from 56 Countries. Front. Psychiatry 2018, 8, 248. [Google Scholar] [CrossRef] [PubMed]
- Shorey, S.; Chee, C.; Ng, E.D.; Chan, Y.H.; Tam, W.; Chong, Y.S. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef]
- Rymaszewska, J.; Dolna, M.; Gryboś, M.; Kiejna, A. Mental disorders during pregnancy and postpartum period—Epidemiology, etiology, classification and treatment. Ginekol. Pol. 2005, 76, 322–330. [Google Scholar]
- Jaeschke, R.R.; Dudek, D.; Topór-Mądry, R.; Drozdowicz, K.; Datka, W.; Siwek, M.; Rybakowski, J. Postpartum depression: Bipolar or unipolar? Analysis of 434 Polish postpartum women. Braz. J. Psychiatry 2016, 39, 154–159. [Google Scholar] [CrossRef]
- Cox, E.Q.; Sowa, N.A.; Meltzer-Brody, S.E.; Gaynes, B.N. The perinatal depression treatment cascade: Baby steps toward improving outcomes. J. Clin. Psychiatry 2016, 77, 1189–1200. [Google Scholar] [CrossRef]
- The Lifeline and 988. National Suicide Prevention Lifeline. Available online: https://suicidepreventionlifeline.org/current-events/the-lifeline-and-988/ (accessed on 28 August 2022).
- Netsi, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of Persistent and Severe Postnatal Depression with Child Outcomes. JAMA Psychiatry 2018, 75, 247–253. [Google Scholar] [CrossRef]
- Beebe, B.; Jaffe, J.; Markese, S.; Buck, K.; Chen, H.; Cohen, P.; Bahrick, L.; Andrews, H.; Feldstein, S. The origins of 12-month attachment: A microanalysis of 4-month mother-infant interaction. Attach. Hum. Dev. 2010, 12, 3–141. [Google Scholar] [CrossRef]
- Dayan, J.; Creveuil, C.; Marks, M.N.; Conroy, S.; Herlicoviez, M.; Dreyfus, M.; Tordjman, S. Prenatal depression, prenatal anxiety, and spontaneous preterm birth: A prospective cohort study among women with early and regular care. Psychosom. Med. 2006, 68, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Grote, N.K.; Bridge, J.A.; Gavin, A.R.; Melville, J.L.; Iyengar, S.; Katon, W.J. A Meta-analysis of Depression During Pregnancy and the Risk of Preterm Birth, Low Birth Weight, and Intrauterine Growth Restriction. Arch. Gen. Psychiatry 2010, 67, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Reilly, N.; Kingston, D.; Loxton, D.; Talcevska, K.; Austin, M.P. A narrative review of studies addressing the clinical effectiveness of perinatal depression screening programs. Women Birth 2020, 33, 51–59. [Google Scholar] [CrossRef]
- Jones, C.J.; Creedy, D.K.; Gamble, J.A. Australian midwives’ knowledge of antenatal and postpartum depression: A national survey. J. Midwifery Women’s Health 2011, 56, 353–361. [Google Scholar] [CrossRef]
- Jones, C.J.; Creedy, D.K.; Gamble, J.A. Australian midwives’ awareness and management of antenatal and postpartum depression. Women Birth J. Aust. Coll. Midwives 2012, 25, 23–28. [Google Scholar] [CrossRef]
- Polish Statistical Council. [Dataset] April 2018. GUS Poland: Basic Statistical Data on Delivery and Pregnancy. Available online: https://stat.gov.pl/podstawowe-dane/ (accessed on 22 August 2019).
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry: J. Ment. Sci. 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Steiner, M.; Yonkers, K. Depresja u Kobiet; Wydawnictwo Via Medica: Gdańsk, Poland, 1999; pp. 31–47. [Google Scholar]
- Siu, A.L.; US Preventive Services Task Force (USPSTF); Bibbins-Domingo, K.; Grossman, D.C.; Baumann, L.C.; Davidson, K.W.; Ebell, M.; García, F.A.; Gillman, M.; Herzstein, J.; et al. Screening for Depression in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 315, 380–387. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance; British Psychological Society: Leicester, UK, 2014. [Google Scholar]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef]
- Chrzan-Dętkoś, M.; Walczak-Kozłowska, T. Antenatal and postnatal depression—Are Polish midwives really ready for them? Midwifery 2020, 83, 102646. [Google Scholar] [CrossRef] [PubMed]
- Mule, V.; Reilly, N.M.; Schmied, V.; Kingston, D.; Austin, M.V. Why do some pregnant women not fully disclose at the comprehensive psychosocial assessment with their midwife? Women Birth 2022, 35, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Forder, P.M.; Rich, J.; Harris, S.; Chojenta, C.; Reilly, N.; Austin, M.P.; Loxton, D. Honesty and comfort levels in mothers when screened for perinatal depression and anxiety. Women Birth 2020, 33, e142–e150. [Google Scholar] [CrossRef] [PubMed]
- Bucci, S.; Schwannauer, M.; Berry, N. The digital revolution and its impact on mental health care. Psychol. Psychother. 2019, 92, 277–297. [Google Scholar] [CrossRef] [PubMed]
- Naslund, J.A.; Aschbrenner, K.A.; Marsch, L.A.; Bartels, S.J. The future of mental health care: Peer-to-peer support and social media. Epidemiol. Psychiatr. Sci. 2016, 25, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Chrzan-Dętkoś, M.; Walczak-Kozłowska, T.Z. How do new mothers perceive screening for perinatal depression? Health Psychol. Rep. 2021, 9, 207–216. [Google Scholar] [CrossRef]
- Reilly, N.; Harris, S.; Loxton, D.; Chojenta, C.; Forder, P.; Milgrom, J.; Austin, M.P. Referral for management of emotional health issues during the perinatal period: Does mental health assessment make a difference? Birth 2013, 40, 297–306. [Google Scholar] [CrossRef]


{kind=link}
| Cut-Off Points | ||||
|---|---|---|---|---|
| The Moment of Assessment | Mean Score (SD) | Normal Range (0–9 Points) | Slightly Increased (10–11 Points) | Increased (12 Points and More) |
| Overall, n = 7345 | 4.73 (4.15) | 86.5% | 4.7% | 7.3% |
| month postpartum, n = 5556 | 4.80 (4.11) | 87.6% | 5.0% | 7.3% |
| 1–2 months postpartum, n = 649 | 4.33 (3.92) | 89.7% | 4.3% | 6.0% |
| 2–3 months postpartum, n = 268 | 4.13 (4.19) | 90.3% | 3.7% | 6.0% |
| 3–4 months postpartum, n = 128 | 4.25 (4.34) | 93.8% | 1.6% | 4.7% |
| 4–5 months postpartum, n = 106 | 4.48 (4.15) | 90.6% | 3.8% | 5.7% |
| 5–6 months postpartum, n = 86 | 5.43 (5.56) | 82.8% | 3.4% | 12.6% |
| 6–12 months postpartum, n = 284 | 4.42 (4.20) | 88.8% | 3.2% | 7.7% |
| No data provided, n = 268 | ||||
| Cut-Off Points | ||||
|---|---|---|---|---|
| The Moment of Assessment | Mean Score (SD) | Normal Range (0–9 Points) | Slightly Increased (10–11 Points) | Increased (12 Points and More) |
| Overall, n = 10,454 | 16.05 (5.975) | 14.7% | 8.3% | 77.0% |
| month postpartum, n = 694 | 16.79 (5.77) | 12.0% | 6.6% | 81.4% |
| 1–2 months postpartum, n = 472 | 16.57 (5.48) | 11.4% | 7.4% | 81.1% |
| 2–3 months postpartum, n = 350 | 16.48 (5.84) | 10.6% | 10.6% | 78.9% |
| 3–4 months postpartum, n = 309 | 15.88 (5.88) | 16.2% | 9.7% | 74.1% |
| 4–5 months postpartum, n = 280 | 16.70 (5.91) | 13.9% | 3.6% | 82.5% |
| 5–6 months postpartum, n = 192 | 15.71 (5.79) | 14.9% | 10.1% | 75.0% |
| 6–12 months postpartum, n = 867 | 15.16 (5.89) | 17.9% | 9.1% | 73.0% |
| 13–24 months postpartum, n = 718 | 15.48 (5.93) | 16.4% | 9.2% | 74.4% |
| 25–36 months postpartum, n = 328 | 16.27 (6.22) | 14.9% | 8.8% | 76.2% |
| 37–48 months postpartum, n = 385 | 17.14 (5.98) | 11.4% | 5.7% | 82.9% |
| EPDS’s Cut-Off Points | Change in the Severity of PPD Symptoms | ||||||
|---|---|---|---|---|---|---|---|
| Time Since the First Examination | Mean Score (SD) | Normal Range (0–9 Points) | Slightly Increased (10–11 Points) | Increased (12 Points and More) | Increase in EPDS Scores | Decrease in EPDS Scores | No Difference in EPDS Scores |
| Overall, n = 1297 | 5.99 (5.02) | 76.8% | 6.7% | 16.5% | 55.5% | 32.1% | 14.1% |
| 3 months after first screening, n = 85 | 5.55 (4.98) | 76.4% | 10.6% | 12.9% | 56.5% | 29.4% | 14.1% |
| 4 months after first screening, n = 162 | 5.49 (5.10) | 79.0% | 4.9% | 16.0% | 54.3% | 27.7% | 17.9% |
| 5 months after first screening, n = 143 | 6.76 (5.56) | 70.6% | 5.6% | 23.7% | 61.5% | 28.7% | 9.7% |
| 6 months after first screening, n = 165 | 6.47 (5.36) | 71.5% | 7.2% | 21.2% | 60.0% | 30.9% | 9.1% |
| 6 months after first screening, n = 120 | 6.51 (4.69) | 78.3% | 4.1% | 17.5% | 55.5% | 28.3% | 16.7% |
| 8 months after first screening, n = 81 | 5.81 (4.58) | 81.5% | 8.6% | 9.9% | 58.0% | 30.9% | 11.1% |
| 9 months after first screening, n = 112 | 6.84 (5.05) | 69.6% | 12.5% | 17.9% | 67.9% | 21.4% | 10.7% |
| 10 months after first screening, n = 23 | 6.39 (4.83) | 73.9% | 0.0% | 26.1% | 65.2% | 21.7% | 13.0% |
| Follow-Up Assessment with EPDS 1 | |||
|---|---|---|---|
| Initial Assessment with EPDS Provided by a Midwife | Normal Range (0–9 Points), | Slightly Increased (10–11 Points), | Increased (12 Points and More), |
| Normal range (0–9 points) | 72.3% | 5.6% | 13.5% |
| Slightly increased (10–11 points) | 1.8% | 1.3% | 1.5% |
| Increased (12 points and more) | 26.3% | 3.4% | 3.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrzan-Dętkoś, M.; Murawska, N.; Walczak-Kozłowska, T. ‘Next Stop: Mum’: Evaluation of a Postpartum Depression Prevention Strategy in Poland. Int. J. Environ. Res. Public Health 2022, 19, 11731. https://doi.org/10.3390/ijerph191811731
Chrzan-Dętkoś M, Murawska N, Walczak-Kozłowska T. ‘Next Stop: Mum’: Evaluation of a Postpartum Depression Prevention Strategy in Poland. International Journal of Environmental Research and Public Health. 2022; 19(18):11731. https://doi.org/10.3390/ijerph191811731
Chicago/Turabian StyleChrzan-Dętkoś, Magdalena, Natalia Murawska, and Tamara Walczak-Kozłowska. 2022. "‘Next Stop: Mum’: Evaluation of a Postpartum Depression Prevention Strategy in Poland" International Journal of Environmental Research and Public Health 19, no. 18: 11731. https://doi.org/10.3390/ijerph191811731
APA StyleChrzan-Dętkoś, M., Murawska, N., & Walczak-Kozłowska, T. (2022). ‘Next Stop: Mum’: Evaluation of a Postpartum Depression Prevention Strategy in Poland. International Journal of Environmental Research and Public Health, 19(18), 11731. https://doi.org/10.3390/ijerph191811731