
A Review of the Impact That Healthcare Risk Waste Treatment Technologies Have on the Environment


Abstract
1. Introduction
2. Discussion and Analysis Regarding Health Care
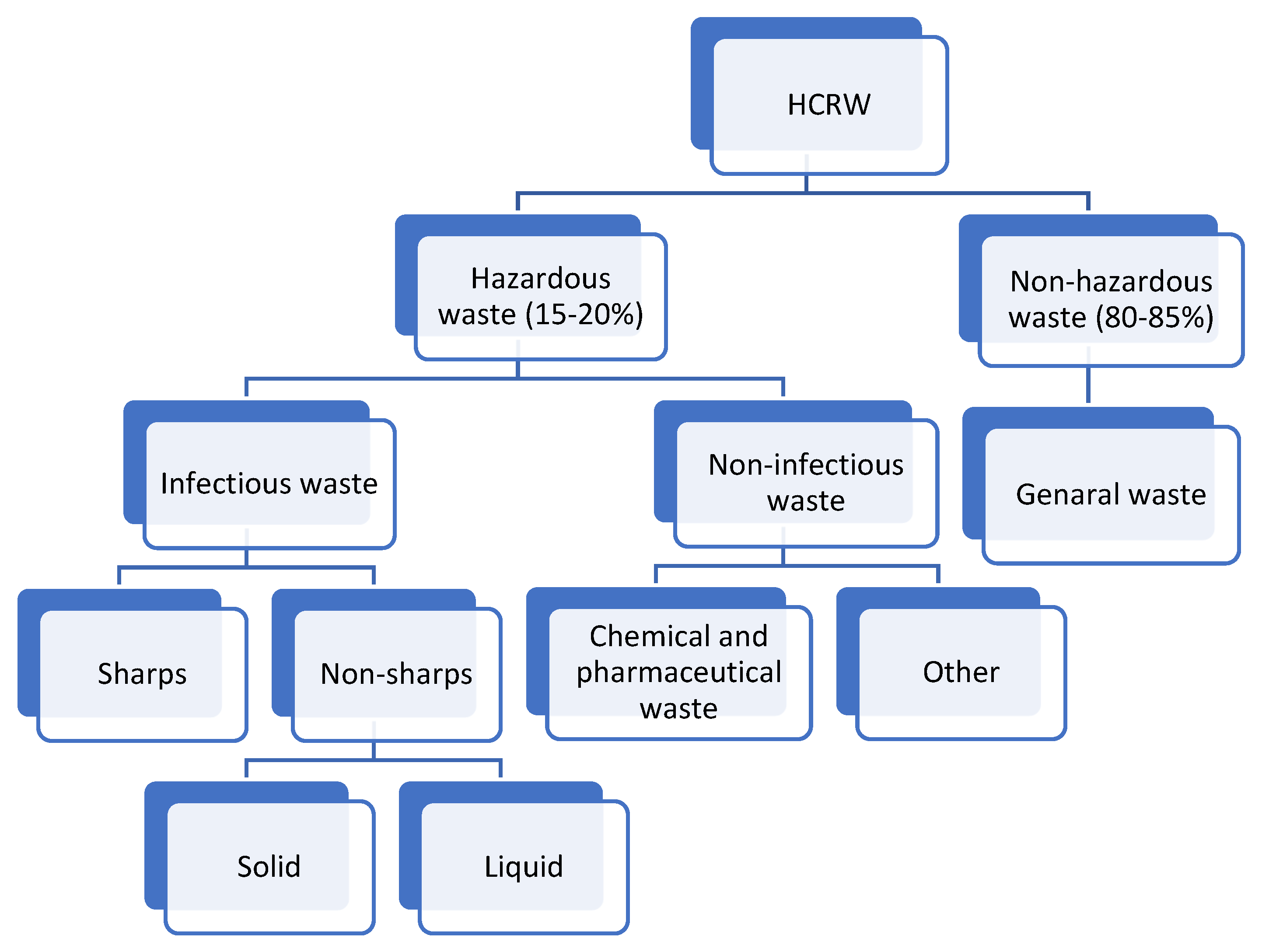
2.1. Health Care Risk Waste


{kind=link}
{kind=link}
| HCRW | Description | Sources | Management |
|---|---|---|---|
| Infectious waste | Waste contaminated with blood and other bodily fluids Cultures and stocks of infectious agents from laboratory work Waste from patients with infections | Hospitals Laboratories Research centers Mortuary Autopsy centers Blood banks Nursing homes Home health care Acupuncturist Paramedic and ambulance services Animal research Physicians’ offices Dental clinics Chiropractors Psychiatric hospitals Cosmetic piercing and tattooing Institutions for disabled people | Non-Burn Thermal Technologies
[40,45] |
| Pathological waste | Human tissues Organs or fluids Body parts Contaminated animal carcasses | Hospitals Laboratories Research centers Mortuary Autopsy centers Paramedic and ambulance services Animal research | Incineration [39,40] |
| Sharps waste | Syringes Needles Disposable scalpels Blades Razors Broken and/or contaminated glass Microscope slides Certain medical saws or amputation equipments Knives | Hospitals Laboratories Research centers Autopsy centers Blood banks Nursing homes Home health care Acupuncturist Paramedic and ambulance services Animal research Physicians’ offices Dental clinics Chiropractors Psychiatric hospitals Cosmetic piercing and tattooing Institutions for disabled people | Non-Burn Thermal Technologies
[39,45] |
| Chemical waste | Solvents Reagents used for laboratory preparations Disinfectants Sterilant Heavy metals contained in medical devices (e.g., mercury in broken thermometers) Batteries | Hospitals Laboratories Research centers Mortuary Autopsy centers Blood banks Nursing homes Home health care Acupuncturist Paramedic and ambulance services Animal research Physicians’ offices Dental clinics Chiropractors Psychiatric hospitals Cosmetic piercing and tattooing Institutions for disabled people | Ion exchange Precipitation Oxidation and Reduction Neutralization [40,46] |
| Pharmaceutical waste | Expired, unused and contaminated drugs Vaccines | Hospitals Laboratories Nursing homes Home health care Physicians’ offices Dental clinics Psychiatric hospitals Institutions for disabled people | Non-Burn Thermal Technologies
[46] |
| Cytotoxic waste | Waste containing substances with genotoxic properties (i.e., highly hazardous substances that are mutagenic, teratogenic, or carcinogenic), such as cytotoxic drugs used in cancer treatment and their metabolites | Hospitals Research centers Nursing homes Home health care Animal research | Incineration [39] |
| Radioactive waste | Such as products contaminated by radionuclides including radioactive diagnostic material or radiotherapeutic materials | Hospitals Research facilities | Most radioactive waste requires packaging in specially engineered containers for safe storage and disposal [40] |
2.2. Generation
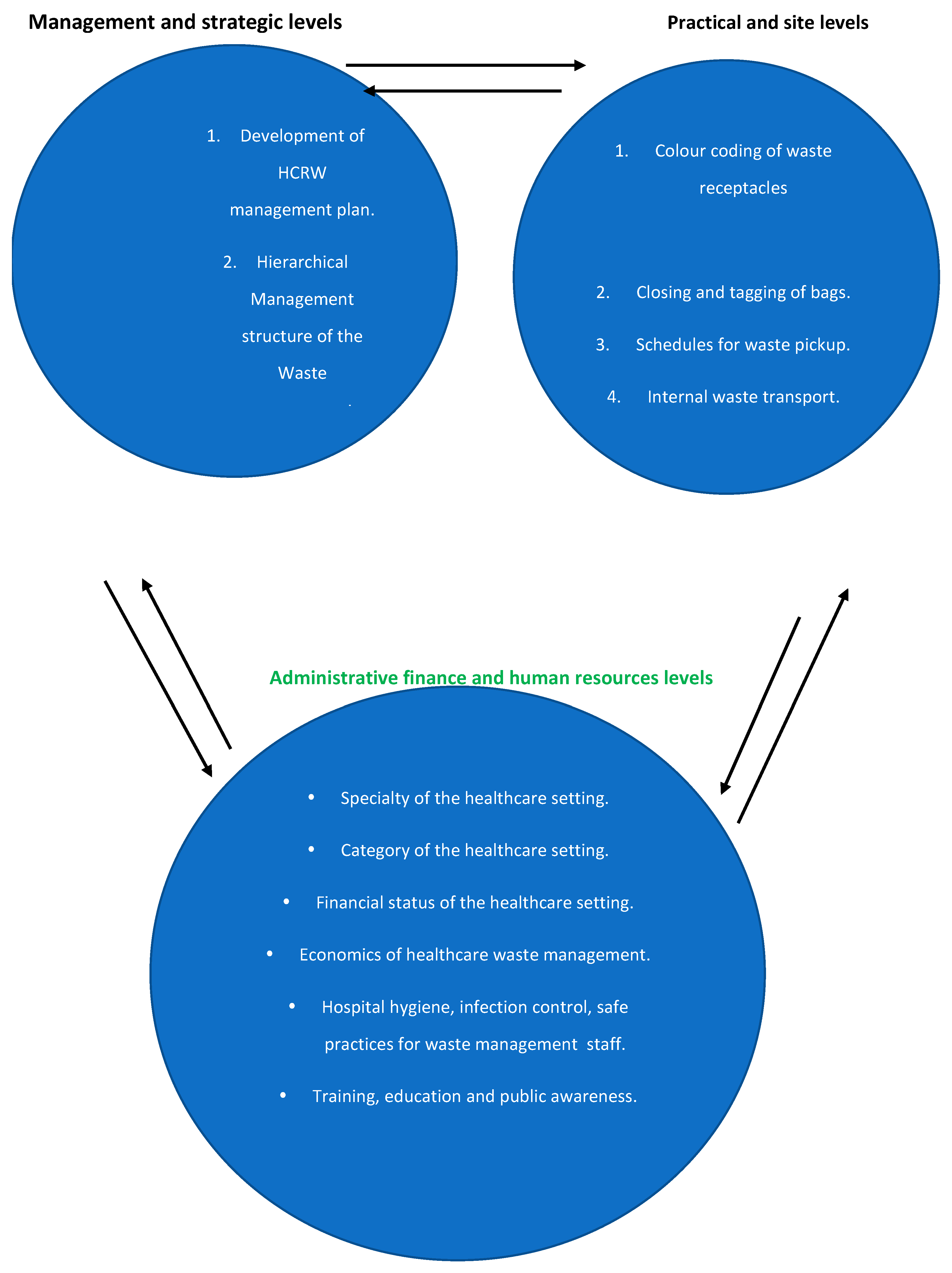
2.3. Management
2.3.1. Incineration
2.3.2. Autoclaving
2.3.3. Microwave Irradiation
2.3.4. Chemical Method
2.3.5. Plasma Pyrolysis
2.4. Environmental Impact of HCRW Treatment
3. Discussion on Challenges and Analysis on Prospective or Relevant Technology Options for the Treatment of HCRW
Suggested Steps, Operations or Actions to Be Taken for HCRW
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Babar, M.S.; Tazyeen, S.; Khan, H.; Tsagkaris, C.; Essar, M.Y.; Ahmad, S. Impact of climate change on health in Karachi, Pakistan. J. Clim. Chang. Health 2021, 2, 100013. [Google Scholar] [CrossRef]
- Malhi, Y.; Franklin, J.; Seddon, N.; Solan, M.; Turner, M.G.; Field, C.B.; Knowlton, N. Climate change and ecosystems: Threats, opportunities and solutions. Philos. Trans. R. Soc. B 2020, 375, 20190104. [Google Scholar] [CrossRef]
- Muluneh, M.G. Impact of climate change on biodiversity and food security: A global perspective—A review article. Agric. Food Secur. 2021, 10, 1–25. [Google Scholar] [CrossRef]
- World Health Organization. Healthy Hospitals—Healthy Planet—Healthy People: Addressing Climate Change in Health Care Settings Report. 2009. Available online: http://www.who.int/globalchange/publications/climatefootprint_ (accessed on 7 June 2020).
- Bergquist, M.; Nilsson, A.; Schultz, P.W. Experiencing a Severe Weather Event Increases Concern About Climate Change. Front. Psychol. 2019, 10, 220. [Google Scholar] [CrossRef] [PubMed]
- Moazami, A.; Nik, V.M.; Carlucci, S.; Geving, S. Impacts of future weather data typology on building energy performance—Investigating long-term patterns of climate change and extreme weather conditions. Appl. Energy 2019, 238, 696–720. [Google Scholar] [CrossRef]
- Linares, C.; Díaz, J.; Negev, M.; Martínez, G.S.; Debono, R.; Paz, S. Impacts of climate change on the public health of the Mediterranean Basin population-Current situation, projections, preparedness and adaptation. Environ. Res. 2020, 182, 109107. [Google Scholar] [CrossRef] [PubMed]
- Pottier, A.; Fleurbaey, M.; Méjean, A.; Zuber, S. Climate change and population: An assessment of mortality due to health impacts. Ecol. Econ. 2021, 183, 106967. [Google Scholar] [CrossRef]
- Santamouris, M. Recent progress on urban overheating and heat island research. Integrated assessment of the energy, environmental, vulnerability and health impact. Synergies with the global climate change. Energy Build. 2020, 207, 109482. [Google Scholar] [CrossRef]
- Stowell, J.D.; Kim, Y.-M.; Gao, Y.; Fu, J.S.; Chang, H.H.; Liu, Y. The impact of climate change and emissions control on future ozone levels: Implications for human health. Environ. Int. 2017, 108, 41–50. [Google Scholar] [CrossRef]
- Woodward, A.; Baumgartner, J.; Ebi, K.L.; Gao, J.; Kinney, P.L.; Liu, Q. Population health impacts of China’s climate change policies. Environ. Res. 2019, 175, 178–185. [Google Scholar] [CrossRef]
- World Health Organization. Global Environmental Change. 2020. Available online: http://www.who.int/globalchange/climate/en/ (accessed on 2 June 2022).
- Manzi, S.; Nichols, A.; Richardson, J. A non-participant observational study of health and social care waste disposal behaviour in the South West of England. J. Health Serv. Res. Policy 2014, 19, 231–235. [Google Scholar] [CrossRef]
- Minlargh, A. Assessment of Healthcare Waste Generation Rate and Infectious Waste Management Practices in St Paul’s Hospital in Addis Ababa, Ethiopia. Ph.D. Thesis, Bahir Dar University, Bahir Dar, Ethopia, 2020. [Google Scholar]
- Chowdhury, T.; Chowdhury, H.; Rahman, S.; Hossain, N.; Ahmed, A.; Sait, S.M. Estimation of the healthcare waste generation during COVID-19 pandemic in Bangladesh. Sci. Total Environ. 2021, 811, 152295. [Google Scholar] [CrossRef]
- Kenny, C.; Priyadarshini, A. Review of Current Healthcare Waste Management Methods and Their Effect on Global Health. Healthcare 2021, 9, 284. [Google Scholar] [CrossRef]
- Alharbi, N.; Alhaji, J.; Qattan, M. Toward sustainable environmental management of healthcare waste: A holistic perspective. Sustainability 2021, 13, 5280. [Google Scholar] [CrossRef]
- Wang, J.; Shen, J.; Ye, D.; Yan, X.; Zhang, Y.; Yang, W.; Li, X.; Wang, J.; Zhang, L.; Pan, L. Disinfection technology of hospital wastes and wastewater: Suggestions for disinfection strategy during coronavirus Disease 2019 (COVID-19) pandemic in China. Environ. Pollut. 2020, 262, 114665. [Google Scholar] [CrossRef]
- McGain, F.; Moore, G.; Black, J. Steam sterilisation’s energy and water footprint. Aust. Health Rev. 2017, 41, 26. [Google Scholar] [CrossRef]
- Hassan, M.F.; Shareefdeen, Z. Recent Developments in Sustainable Management of Healthcare Waste and Treatment Technologies. J. Sustain. Dev. Energy Water Environ. Syst. 2022, 10, 1–21. [Google Scholar] [CrossRef]
- Adeleke, O.; Akinlabi, S.A.; Jen, T.-C.; Dunmade, I. Environmental impact assessment of the current, emerging, and alternative waste management systems using life cycle assessment tools: A case study of Johannesburg, South Africa. Environ. Sci. Pollut. Res. 2021, 29, 7366–7381. [Google Scholar] [CrossRef]
- Kanhar, A.H.; Chen, S.; Wang, F. Incineration Fly Ash and Its Treatment to Possible Utilization: A Review. Energies 2020, 13, 6681. [Google Scholar] [CrossRef]
- National Research Council (US) Committee on Health Effects of Waste Incineration. 3. Incineration Processes and Environmental Releases. In Waste Incineration & Public Health; National Academies Press (US): Washington, DC, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK233627 (accessed on 2 June 2022).
- Maria, C.; Góis, J.; Leitão, A. Challenges and perspectives of greenhouse gases emissions from municipal solid waste management in Angola. Energy Rep. 2019, 6, 364–369. [Google Scholar] [CrossRef]
- Hassan, A.A.; Tudor, T.; Vaccari, M. Healthcare Waste Management: A Case Study from Sudan. Environments 2018, 5, 89. [Google Scholar] [CrossRef]
- Zikhathile, T.; Atagana, H. Challenges Facing Home-Based Caregivers in the Management of Health Care Risk Waste. Int. J. Environ. Res. Public Health 2018, 15, 2700. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, P.; He, X.; Wang, L. Groundwater Quality in and Around a Landfill in Northwest China: Characteristic Pollutant Identification, Health Risk Assessment, and Controlling Factor Analysis. Expo. Health 2022, 1–17. [Google Scholar] [CrossRef]
- Mukherjee, S.; Mukhopadhyay, S.; Hashim, M.A.; Gupta, B.S. Contemporary Environmental Issues of Landfill Leachate: Assessment and Remedies. Crit. Rev. Environ. Sci. Technol. 2014, 45, 472–590. [Google Scholar] [CrossRef]
- Wijekoon, P.; Koliyabandara, P.A.; Cooray, A.T.; Lam, S.S.; Athapattu, B.C.; Vithanage, M. Progress and prospects in mitigation of landfill leachate pollution: Risk, pollution potential, treatment and challenges. J. Hazard. Mater. 2021, 421, 126627. [Google Scholar] [CrossRef] [PubMed]
- Zierold, K.M.; Odoh, C. A review on fly ash from coal-fired power plants: Chemical composition, regulations, and health evidence. Rev. Environ. Health 2020, 35, 401–418. [Google Scholar] [CrossRef] [PubMed]
- Bian, R.; Zhang, T.; Zhao, F.; Chen, J.; Liang, C.; Li, W.; Sun, Y.; Chai, X.; Fang, X.; Yuan, L. Greenhouse gas emissions from waste sectors in China during 2006–2019: Implications for carbon mitigation. Process Saf. Environ. Prot. 2022, 161, 488–497. [Google Scholar] [CrossRef]
- Torkayesh, A.E.; Vandchali, H.R.; Tirkolaee, E.B. Multi-Objective Optimization for Healthcare Waste Management Network Design with Sustainability Perspective. Sustainability 2021, 13, 8279. [Google Scholar] [CrossRef]
- Storz, M.A. A Practical Guide for Physicians and Health Care Workers to Reduce Their Carbon Footprint in Daily Clinical Work. Perm. J. 2018, 22, 17–145. [Google Scholar] [CrossRef]
- Elimi, I.O. An Estimate of Carbon Footprint of Ekurhuleni Health District Office and Provincial Clinic Employees. Master’s Thesis, University of South Africa, Pretoria, South Africa, 2017. [Google Scholar]
- Tomson, C. Reducing the carbon footprint of hospital-based care. Futur. Hosp. J. 2015, 2, 57–62. [Google Scholar] [CrossRef]
- Cameron, L.; Rocque, R.; Penner, K.; Mauro, I. Public perceptions of Lyme disease and climate change in southern Manitoba, Canada: Making a case for strategic decoupling of climate and health messages. BMC Public Health 2021, 21, 617. [Google Scholar] [CrossRef]
- Paavola, J. Health impacts of climate change and health and social inequalities in the UK. Environ. Health 2017, 16, 61–68. [Google Scholar] [CrossRef]
- Zisis, E.; Hakimi, S.; Lee, E.-Y. Climate change, 24-hour movement behaviors, and health: A mini umbrella review. Glob. Health Res. Policy 2021, 6, 15. [Google Scholar] [CrossRef]
- Pruss, A.; Giroult, E.; Rushbrook, P. (Eds.) Safe Management of Wastes from Healthcare Activities; World Health Organization: Geneva, Switzerland, 1999; pp. 77–111. [Google Scholar]
- World Health Organization. Safe Management of Waste from Health-Care Activities, 2nd ed.; Department of Public Health, Environmental and Social Determinates of Health, World Health Organization: Geneva, Switzerland, 2013; Available online: www.who.int/phe (accessed on 17 May 2020).
- Singh, N.; Ogunseitan, O.A.; Tang, Y. Medical waste: Current challenges and future opportunities for sustainable management. Crit. Rev. Environ. Sci. Technol. 2021, 52, 2000–2022. [Google Scholar] [CrossRef]
- Anicetus, H.; Saria, J.; Mohamed, H. Estimation of Different Categories of Healthcare Waste Generated at Two Different Hospital Categories in Four Hospitals in Dar es Salaam City. J. Environ. Prot. 2020, 11, 872–888. [Google Scholar] [CrossRef]
- Zamparas, M.; Kapsalis, V.C.; Kyriakopoulos, G.L.; Aravossis, K.G.; Kanteraki, A.E.; Vantarakis, A.; Kalavrouziotis, I.K. Medical waste management and environmental assessment in the Rio University Hospital, Western Greece. Sustain. Chem. Pharm. 2019, 13, 10063. [Google Scholar] [CrossRef]
- Zikhathile, T.; Atagana, H. Health Care Risk Waste Generated in Domestic Settings through Home Health: A Review of the Health and Environmental Impact in South Africa. In Proceedings of the 10th Int’l Conference on Advances in Science, Engineering, Technology & Healthcare (ASETH-18), Cape Town, South Africa, 19–20 November 2018; pp. 57–65. [Google Scholar]
- Mol, M.P.; Ribeiro, P.A.M.; Neves, A.C. Quantitative estimation of healthcare wastes generated by brazilian hospitals: A literature review. Environ. Eng. Manag. J. 2020, 19, 1143–1156. [Google Scholar] [CrossRef]
- Silva, A.L.P.; Prata, J.C.; Walker, T.R.; Duarte, A.C.; Ouyang, W.; Barcelò, D.; Rocha-Santos, T. Increased plastic pollution due to COVID-19 pandemic: Challenges and recommendations. Chem. Eng. J. 2020, 405, 126683. [Google Scholar] [CrossRef]
- Minoglou, M.; Gerassimidou, S.; Komilis, D. Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors. Sustainability 2017, 9, 220. [Google Scholar] [CrossRef]
- Ye, J.; Song, Y.; Liu, Y.; Zhong, Y. Assessment of medical waste generation, associated environmental impact, and management issues after the outbreak of COVID-19: A case study of the Hubei Province in China. PLoS ONE 2022, 17, e0259207. [Google Scholar] [CrossRef]
- Peng, J.; Wu, X.; Wang, R.; Li, C.; Zhang, Q.; Wei, D. Medical waste management practice during the 2019–2020 novel coronavirus pandemic: Experience in a general hospital. Am. J. Infect. Control 2020, 48, 918–921. [Google Scholar] [CrossRef] [PubMed]
- Olaniyi, F.C.; Ogola, J.S.; Tshitangano, T.G. Challenges of effective management of medical waste in low-resource settings: Perception of healthcare workers in Vhembe district healthcare facilities, South Africa. Trans. R. Soc. S. Afr. 2021, 76, 81–88. [Google Scholar] [CrossRef]
- Ghannadpour, S.F.; Zandieh, F.; Esmaeili, F. Optimizing triple bottom-line objectives for sustainable health-care waste collection and routing by a self-adaptive evolutionary algorithm: A case study from tehran province in Iran. J. Clean. Prod. 2020, 287, 125010. [Google Scholar] [CrossRef]
- Tsai, W.-T. Analysis of medical waste management and impact analysis of COVID-19 on its generation in Taiwan. Waste Manag. Res. 2021, 39, 27–33. [Google Scholar] [CrossRef]
- Barua, U.; Hossain, D. A review of the medical waste management system at Covid-19 situation in Bangladesh. J. Mater. Cycles Waste Manag. 2021, 23, 2087–2100. [Google Scholar] [CrossRef]
- Wassie, B.; Gintamo, B.; Mekuria, Z.N.; Gizaw, Z. Healthcare Waste Management Practices and Associated Factors in Private Clinics in Addis Ababa, Ethiopia. Environ. Health Insights 2022, 16, 11786302211073383. [Google Scholar] [CrossRef]
- Thakur, V.; Mangla, S.K.; Tiwari, B. Managing healthcare waste for sustainable environmental development: A hybrid decision approach. Bus. Strat. Environ. 2020, 30, 357–373. [Google Scholar] [CrossRef]
- Pudussery, P.K. A Study on the Medical Waste Management at the Norfolk and Norwich University Hospital. Master’s Thesis, University of East Anglia, School of Environmental Sciences, Norwich, UK, 2011; pp. 11–13. [Google Scholar]
- Abah, S.A.; Ohimain, E.I. Healthcare waste management in Nigeria: A case study. J. Public Health Epidemiol. 2011, 3, 99–110. [Google Scholar]
- Gabela, S.D.; Knight, S.E. Healthcare waste management in clinics in a rural health district in KwaZulu-Natal. South. Afr. J. Epidemiol. Infect. 2010, 25, 19–21. [Google Scholar] [CrossRef]
- Padmanabhan, K.; Barik, D. Health Hazards of Medical Waste and its Disposal. In Energy from Toxic Organic Waste for Heat and Power Generation; Woodhead Publishing: Sawston, UK, 2019; pp. 99–118. [Google Scholar]
- Jansen, K.E.; Kocks, D.J.; Roberts, H. Healthcare risk waste and waste legislation in South Africa. Occup. Health S. Afr. 2017, 23, 15–17. [Google Scholar]
- Olaniyi, F.C.; Ogola, J.S.; Tshitangano, T.G. A Review of Medical Waste Management in South Africa. Open Environ. Sci. 2018, 10, 34–45. [Google Scholar]
- Syafei, A.N.; Utomo, S.W. Comparison of COVID-19 Medical Waste Management Strategies For Hospitals in Developed And Developing Country. KESANS Int. J. Health Sci. 2022, 1, 842–850. [Google Scholar] [CrossRef]
- Salimian, S.; Mousavi, S. The selection of healthcare waste treatment technologies by a multi-criteria group decision-making method with intuitionistic fuzzy sets. J. Ind. Syst. Eng. 2022, 14, 205–220. [Google Scholar]
- Shareefdeen, Z.; Ashoobi, N.; Ilyas, U. Medical Waste Management and Treatment Technologies. In Hazardous Waste Management; Shareefdeen, Z., Ed.; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Fu, Z.; Lin, S.; Tian, H.; Hao, Y.; Wu, B.; Liu, S.; Luo, L.; Bai, X.; Guo, Z.; Lv, Y. A comprehensive emission inventory of hazardous air pollutants from municipal solid waste incineration in China. Sci. Total Environ. 2022, 826. [Google Scholar] [CrossRef]
- Liu, F.; Liu, H.-Q.; Wei, G.-X.; Zhang, R.; Zeng, T.-T.; Liu, G.-S.; Zhou, J.-H. Characteristics and Treatment Methods of Medical Waste Incinerator Fly Ash: A Review. Processes 2018, 6, 173. [Google Scholar] [CrossRef]
- Pancholi, K.C.; Singh, P.J.; Bhattacharyya, K.; Tiwari, M.; Sahu, S.K.; Vincent, T.; Udupa, D.V.; Kaushik, C.P. Elemental analysis of residual ash generated during plasma incineration of cellulosic, rubber and plastic waste. Waste Manag. Res. 2021, 40, 665–675. [Google Scholar] [CrossRef]
- Jaber, S.K.; Aljawad, A.A.; Pop, E.; Prisecaru, T.; Pisa, I. The Use of Bottom Ash and Fly Ash from Medical Incinerators as Road Construction Material. Sci. Bull. -Univ. Politeh. Buchar. 2022, 84, 2. [Google Scholar]
- Elkhatib, A.; Barakat, N.A.; Youssef, N.A.; Samir, N.A. Bioaccumulation of heavy metals air pollutants by urban trees. Int. J. Phytoremediat. 2019, 22, 210–222. [Google Scholar] [CrossRef]
- Perry, A.G.; Potter, P.A.; Ostendorf, W.R. Clinical Skills and Nursing Techniques, 8th ed.; ElsevierMosby: St Louis, MO, USA, 2014. [Google Scholar]
- Satter, M.S. An Environmental Impact Perspective of the Management, Treatment, and Disposal of Hazardous Pharmaceutical Compounds Generated as Medical Waste at Selected Hospitals in Cape Town, South Africa. Master’s Thesis, Cape Peninsula University of Technology, Cape Town, South Africa, 2011. [Google Scholar]
- Ranjbari, M.; Esfandabadi, Z.S.; Shevchenko, T.; Chassagnon-Haned, N.; Peng, W.; Tabatabaei, M.; Aghbashlo, M. Mapping healthcare waste management research: Past evolution, current challenges, and future perspectives towards a circular economy transition. J. Hazard. Mater. 2021, 422, 126724. [Google Scholar] [CrossRef]
- Kollu, V.K.R.; Kumar, P.; Gautam, K. Comparison of microwave and autoclave treatment for biomedical waste disinfection. Syst. Microbiol. Biomanuf. 2022, 2, 1–11. [Google Scholar] [CrossRef]
- Hossain, S.; Santhanam, A.; Norulaini, N.N.; Omar, A.M. Clinical solid waste management practices and its impact on human health and environment—A review. Waste Manag. 2011, 31, 754–766. [Google Scholar] [CrossRef] [PubMed]
- Hooshmand, S.; Kargozar, S.; Ghorbani, A.; Darroudi, M.; Keshavarz, M.; Baino, F.; Kim, H.-W.; Hooshmand, S. Biomedical Waste Management by Using Nanophotocatalysts: The Need for New Options. Materials 2020, 13, 3511. [Google Scholar] [CrossRef] [PubMed]
- Prendeville, S.; Sanders, C.; Sherry, J.; Costa, F. Circular Economy: Is It Enough. EcoDesign Centre, Wales. 2014. Available online: https://www.researchgate.net/profile/Sharon-Prendeville-2/publication/301779162_Circular_Economy_Is_it_Enough/links/5727a2be08aef9c00b8b4ddd/Circular-Economy-Is-it-Enough.pdf?origin=publication_detail (accessed on 21 July 2014).
- Kumar, A.R.; Vaidya, A.N.; Singh, I.; Ambekar, K.; Gurjar, S.; Prajapati, A.; Kanade, G.S.; Hippargi, G.; Kale, G.; Bodkhe, S. Leaching characteristics and hazard evaluation of bottom ash generated from common biomedical waste incinerators. J. Environ. Sci. Health Part A 2021, 56, 1069–1079. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Dong, S.; Wang, P.; Hao, Y.; Wang, R.; Zhang, S.; Wang, Y.; Wang, P.; Zhang, Q.; Jiang, G. A pilot evaluation on the toxicokinetics and bioaccumulation of polychlorinated naphthalenes in laying hens. Sci. Total Environ. 2022, 835. [Google Scholar] [CrossRef]
- Petrlik, J.; Bell, L.; DiGangi, J.; Allo’O, S.M.A.; Kuepouo, G.; Ochola, G.O.; Grechko, V.; Jelinek, N.; Strakova, J.; Skalsky, M.; et al. Monitoring dioxins and PCBs in eggs as sensitive indicators for environmental pollution and global contaminated sites and recommendations for reducing and controlling releases and exposure. Emerg. Contam. 2022, 8, 254–279. [Google Scholar] [CrossRef]
- Mayilsamy, M.; Sangeetha, S.; Nakamura, M.; Ko, S.; Govarthanan, M.; Vimalkumar, K. Screening of PCDDs/Fs and DL-PCBs by AhR-CALUX bioassay in bovine milk and environment ash from India. Toxicol. Environ. Health Sci. 2022, 14, 223–234. [Google Scholar] [CrossRef]
- Choi, K.-H.; Lim, H.; Bae, S.; Ha, M.; Kwon, H.-J.; Yoon, M.; Hong, S.; Eom, S.-Y.; Kim, Y.-D.; Kim, H. Cancer risk in the residents of a town near three industrial waste incinerators in Korea: A retrospective cohort study. Int. Arch. Occup. Environ. Health 2022, 1–15. [Google Scholar] [CrossRef]
- Jury, M.R.; Buthelezi, M.S. Air Pollution Dispersion over Durban, South Africa. Atmosphere 2022, 13, 811. [Google Scholar] [CrossRef]
- Rizan, C.; Bhutta, M.F.; Reed, M.; Lillywhite, R. The carbon footprint of waste streams in a UK hospital. J. Clean. Prod. 2020, 286, 125446. [Google Scholar] [CrossRef]
- Manupati, V.K.; Ramkumar, M.; Baba, V.; Agarwal, A. Selection of the best healthcare waste disposal techniques during and post COVID-19 pandemic era. J. Clean. Prod. 2020, 281, 125175. [Google Scholar] [CrossRef]
- Talukder, B.; van Loon, G.W.; Hipel, K.W.; Chiotha, S.; Orbinski, J. Health impacts of climate change on smallholder farmers. One Health 2021, 13, 100258. [Google Scholar] [CrossRef]
- Ammann, P.; Dietler, D.; Winkler, M.S. Health impact assessment and climate change: A scoping review. J. Clim. Chang. Health 2021, 3, 100045. [Google Scholar] [CrossRef]
- Brown, M.J.; White, B.P.; Nicholas, P.K. Mental Health Impacts of Climate Change: Considerations for Nurse Practitioners. J. Nurse Pract. 2021, 18, 359–363. [Google Scholar] [CrossRef]
- Malik, A.; Lenzen, M.; McAlister, S.; McGain, F. The carbon footprint of Australian health care. Lancet Planet. Health 2018, 2, e27–e35. [Google Scholar] [CrossRef]
- Grobusch, L.C.; Grobusch, M.P. A hot topic at the environment-health nexus: Investigating the impact of climate change on infectious diseases. Int. J. Infect. Dis. 2021, 116, 7–9. [Google Scholar] [CrossRef]
- Kulkarni, M.A.; Duguay, C.; Ost, K. Charting the evidence for climate change impacts on the global spread of malaria and dengue and adaptive responses: A scoping review of reviews. Glob. Health 2022, 18, 1. [Google Scholar] [CrossRef]
- Rocque, R.J.; Beaudoin, C.; Ndjaboue, R.; Cameron, L.; Poirier-Bergeron, L.; Poulin-Rheault, R.-A.; Fallon, C.; Tricco, A.C.; Witteman, H.O. Health effects of climate change: An overview of systematic reviews. BMJ Open 2021, 11, e046333. [Google Scholar] [CrossRef]
- Xu, L.; Cherian, J.; Zaheer, M.; Sial, M.S.; Comite, U.; Cismas, L.M.; Cristia, J.F.E.; Oláh, J. The Role of Healthcare Employees’ Pro-Environmental Behavior for De-Carbonization: An Energy Conservation Approach from CSR Perspective. Energies 2022, 15, 3429. [Google Scholar] [CrossRef]
- Giakoumakis, G.; Politi, D.; Sidiras, D. Medical Waste Treatment Technologies for Energy, Fuels, and Materials Production: A Review. Energies 2021, 14, 8065. [Google Scholar] [CrossRef]

| Treatment Methods | Description | Types of Waste Treated | Temperature for Treatment | Treatment Time | Advantages | Disadvantages |
|---|---|---|---|---|---|---|
| Incineration | High-heat treatment converts waste into ash and exhaust gases. | Anatomical, infectious, and pharmaceutical wastes | Primary chamber 800–900 °C Secondary chamber 900–1200 °C | 4–6 h per batch | Suitable for treatment of all types of hazardous HCRW. Reduces the volume significantly. | Produces air pollutants, carcinogens (dioxins, polychlorinated biphenyls, polycyclic aromatic compounds) and harmful gases (HCl, HF, SO2). Very costly. |
| Autoclave | Use saturated steam to disinfect infectious waste. | Infectious, pharmaceutical, and sharps | 121–140 °C | 30–60 min per batch | Has better public acceptance than incinerators. | The disinfected waste is landfilled. The discharged moisture contaminates the environment. |
| Microwave | Steam-based technology. Uses microwave disinfection to treat waste. | Infectious, pharmaceutical, and sharps | 95–100 °C | ≥30 min per batch | Has better public acceptance than incinerators. | The disinfected waste is landfilled. |
| Reverse polymerization | Uses microwave energy to treat waste. Shredding is applied to the final sterilized carbon residue. | Infectious waste | 180–370 °C | 50–80 min per batch | Decreases the quantities of waste. | Use of Sodium Hydroxide (NaOH) and a scrubber to control gaseous emissions. Production of wastewater. Extremely costly. |
| Chemical disinfection | Uses a chemical technology with sodium hypochlorite as a disinfectant. | Liquid waste | 95–155 °C | 25 min exposure per batch | Low air emissions. Simple and convenient, good deodorization effect. | Production of liquid waste containing sodium hypochlorite (NaOCl). |
| Pyrolysis | Heats waste organic components under oxygen-free or -depleted conditions, breaks chemical bonds to transform combustible liquid and gas. | Infectious waste | 540–830 °C | 45 min | Pyrolysis technology has a high energy recovery rate, minimal secondary pollution, and sufficient economics. | Commonly used for organic materials. It occurs at high temperatures. |
| Gasification | Gas cloud formed by the ionization of an inert gas, usually referred to as the fourth state of matter. | Infectious waste | 3000 °C | 1/1000 s | Treats all HCRW. | Expensive. Energy demanding. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zikhathile, T.; Atagana, H.; Bwapwa, J.; Sawtell, D. A Review of the Impact That Healthcare Risk Waste Treatment Technologies Have on the Environment. Int. J. Environ. Res. Public Health 2022, 19, 11967. https://doi.org/10.3390/ijerph191911967
Zikhathile T, Atagana H, Bwapwa J, Sawtell D. A Review of the Impact That Healthcare Risk Waste Treatment Technologies Have on the Environment. International Journal of Environmental Research and Public Health. 2022; 19(19):11967. https://doi.org/10.3390/ijerph191911967
Chicago/Turabian StyleZikhathile, Thobile, Harrison Atagana, Joseph Bwapwa, and David Sawtell. 2022. "A Review of the Impact That Healthcare Risk Waste Treatment Technologies Have on the Environment" International Journal of Environmental Research and Public Health 19, no. 19: 11967. https://doi.org/10.3390/ijerph191911967
APA StyleZikhathile, T., Atagana, H., Bwapwa, J., & Sawtell, D. (2022). A Review of the Impact That Healthcare Risk Waste Treatment Technologies Have on the Environment. International Journal of Environmental Research and Public Health, 19(19), 11967. https://doi.org/10.3390/ijerph191911967