
The Association between Early Opioids Prescribing and the Length of Disability in Acute Lower Back Pain: A Systematic Review and Narrative Synthesis
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Criteria for Considering Studies for the Review
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Study Selection Process
2.4. Quality Assessment
2.5. Data Extraction
2.6. Data Analysis
3. Results
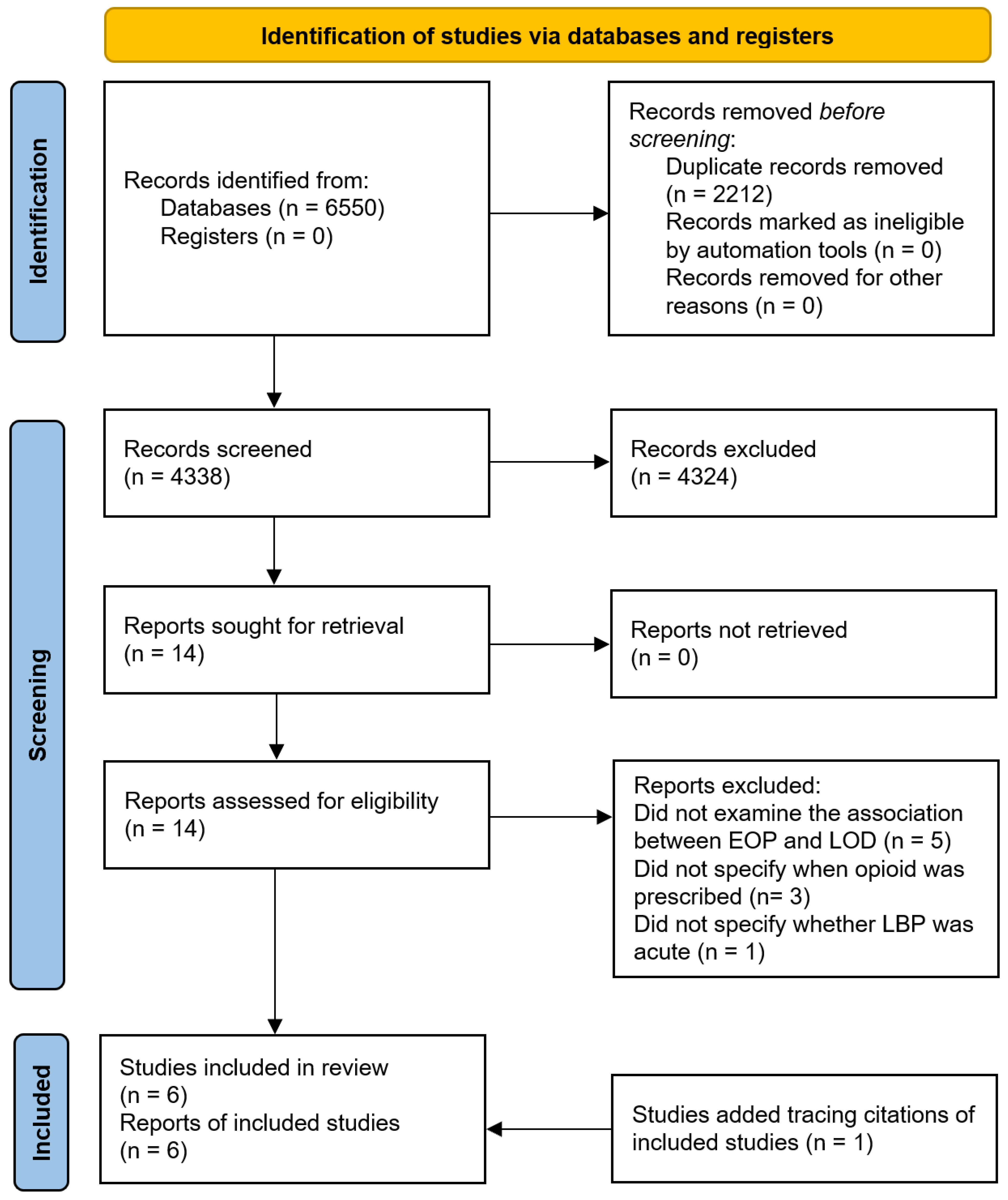
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
3.4. The Association between EOP and LOD
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Becker, A.; Held, H.; Redaelli, M.; Strauch, K.; Chenot, J.F.; Leonhardt, C.; Keller, S.; Baum, E.; Pfingsten, M.; Hildebrandt, J.; et al. Low back pain in primary care: Costs of care and prediction of future health care utilization. Spine 2010, 35, 1714–1720. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Chen, M.; Wu, X.; Lin, S.; Tao, C.; Cao, H.; Shao, Z.; Xiao, G. Global, regional and national burden of low back pain 1990–2019: A systematic analysis of the Global Burden of Disease study 2019. J. Orthop. Transl. 2022, 32, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef]
- Costa, L.d.M.; Maher, C.G.; Hancock, M.J.; McAuley, J.H.; Herbert, R.D.; Costa, L.O. The prognosis of acute and persistent low-back pain: A meta-analysis. CMAJ 2012, 184, E613–E624. [Google Scholar] [CrossRef]
- da Silva, T.; Mills, K.; Brown, B.T.; Herbert, R.D.; Maher, C.G.; Hancock, M.J. Risk of Recurrence of Low Back Pain: A Systematic Review. J. Orthop. Sports Phys. 2017, 47, 305–313. [Google Scholar] [CrossRef]
- Andersson, G.B. Epidemiological features of chronic low-back pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Gore, M.; Sadosky, A.; Stacey, B.R.; Tai, K.S.; Leslie, D. The burden of chronic low back pain: Clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine 2012, 37, E668–E677. [Google Scholar] [CrossRef]
- Lambeek, L.C.; van Tulder, M.W.; Swinkels, I.C.; Koppes, L.L.; Anema, J.R.; van Mechelen, W. The trend in total cost of back pain in The Netherlands in the period 2002 to 2007. Spine 2011, 36, 1050–1058. [Google Scholar] [CrossRef]
- Deyo, R.A.; Mirza, S.K.; Turner, J.A.; Martin, B.I. Overtreating chronic back pain: Time to back off? J. Am. Board Fam. Med. 2009, 22, 62–68. [Google Scholar] [CrossRef]
- Dagenais, S.; Caro, J.; Haldeman, S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008, 8, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Steenstra, I.A.; Verbeek, J.H.; Heymans, M.W.; Bongers, P.M. Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: A systematic review of the literature. Occup. Env. Med. 2005, 62, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Maher, C.G.; Wiech, K.; Van Zundert, J.; Meloto, C.B.; Diatchenko, L.; Battié, M.C.; Goossens, M.; Koes, B.; Linton, S.J. Low back pain. Nat. Rev. Dis Primers 2018, 4, 52. [Google Scholar] [CrossRef] [PubMed]
- Shraim, M.; Cifuentes, M.; Willetts, J.L.; Marucci-Wellman, H.R.; Pransky, G. Regional socioeconomic disparities in outcomes for workers with low back pain in the United States. Am. J. Ind. Med. 2017, 60, 472–483. [Google Scholar] [CrossRef]
- Shraim, M.; Cifuentes, M.; Willetts, J.L.; Marucci-Wellman, H.R.; Pransky, G. Length of Disability and Medical Costs in Low Back Pain: Do State Workers' Compensation Policies Make a Difference? J. Occup. Env. Med. 2015, 57, 1275–1283. [Google Scholar] [CrossRef]
- Shraim, B.A.; Shraim, M.A.; Ibrahim, A.R.; Elgamal, M.E.; Al-Omari, B.; Shraim, M. The association between early MRI and length of disability in acute lower back pain: A systematic review and narrative synthesis. BMC Musculoskelet Disord 2021, 22, 983. [Google Scholar] [CrossRef]
- Webster, B.S.; Verma, S.K.; Gatchel, R.J. Relationship between early opioid prescribing for acute occupational low back pain and disability duration, medical costs, subsequent surgery and late opioid use. Spine 2007, 32, 2127–2132. [Google Scholar] [CrossRef]
- Oliva-Pascual-Vaca, Á.; González-González, C.; Oliva-Pascual-Vaca, J.; Piña-Pozo, F.; Ferragut-Garcías, A.; Fernández-Domínguez, J.C.; Heredia-Rizo, A.M. Visceral Origin: An Underestimated Source of Neck Pain. A Systematic Scoping Review. Diagnostics 2019, 9, 186. [Google Scholar] [CrossRef]
- Giamberardino, M.; Affaitati, G.C. Costantini. Visceral Referred Pain. J. Musculoskelet. Pain 2010, 18, 403–410. [Google Scholar] [CrossRef]
- Cervero, F. Central sensitization and visceral hypersensitivity: Facts and fictions. Scand. J. Pain 2014, 5, 49–50. [Google Scholar] [CrossRef]
- Bikbov, M.M.; Kazakbaeva, G.M.; Zainullin, R.M.; Salavatova, V.F.; Gilmanshin, T.R.; Arslangareeva, I.I.; Nikitin, N.A.; Mukhamadieva, S.R.; Yakupova, D.F.; Panda-Jonas, S.; et al. Prevalence of and factors associated with low Back pain, thoracic spine pain and neck pain in Bashkortostan, Russia: The Ural Eye and Medical Study. BMC Musculoskelet Disord 2020, 21, 64. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.D.; Russell, A.; Hodges, P.W. How common is back pain in women with gastrointestinal problems? Clin. J. Pain 2008, 24, 199–203. [Google Scholar] [CrossRef]
- Benyamin, R.; Trescot, A.M.; Datta, S.; Buenaventura, R.; Adlaka, R.; Sehgal, N.; Glaser, S.E.; Vallejo, R. Opioid complications and side effects. Pain Physician 2008, 11, S105–S120. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Singh, A. Therapeutic opioids: A ten-year perspective on the complexities and complications of the escalating use, abuse, and nonmedical use of opioids. Pain Physician 2008, 11, S63–S88. [Google Scholar] [CrossRef]
- Ballantyne, J.C.; LaForge, S.K. Opioid dependence and addiction during opioid treatment of chronic pain. Pain 2007, 129, 235–255. [Google Scholar] [CrossRef] [PubMed]
- van Tulder, M.; Becker, A.; Bekkering, T.; Breen, A.; del Real, M.T.; Hutchinson, A.; Koes, B.; Laerum, E.; Malmivaara, A. Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur. Spine J. 2006, 15 (Suppl. S2), S169–S191. [Google Scholar] [CrossRef]
- National Guideline, C. National Guideline, C. National Institute for Health and Care Excellence: Guidelines. In Low Back Pain and Sciatica in Over 16s: Assessment and Management; National Institute for Health and Care Excellence (NICE): London, UK, 2016. [Google Scholar]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A.; Denberg, T.D.; Barry, M.J.; Boyd, C.; Chow, R.D.; Fitterman, N.; Harris, R.P.; et al. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2017, 166, 514–530. [Google Scholar] [CrossRef]
- Jeffrey Kao, M.C.; Minh, L.C.; Huang, G.Y.; Mitra, R.; Smuck, M. Trends in ambulatory physician opioid prescription in the United States, 1997-2009. PM R 2014, 6, 575–582.e574. [Google Scholar] [CrossRef]
- Lee, S.S.; Choi, Y.; Pransky, G.S. Extent and Impact of Opioid Prescribing for Acute Occupational Low Back Pain in the Emergency Department. J. Emerg. Med. 2016, 50, 376–384. [Google Scholar] [CrossRef]
- Vogt, M.T.; Kwoh, C.K.; Cope, D.K.; Osial, T.A.; Culyba, M.; Starz, T.W. Analgesic usage for low back pain: Impact on health care costs and service use. Spine 2005, 30, 1075–1081. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, M.A.; Webster, B.S.; Courtney, T.K.; Matz, S.; Tacci, J.A.; Christiani, D.C. Clinical management and the duration of disability for work-related low back pain. J. Occup. Env. Med. 2000, 42, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Wells, G.; Shea, B.; Shea, B.; O’Connell, D.; Peterson, J.; Welch; Losos, M.; Tugwell, P.; Ga, S.W.; et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; University of Ottawa: Ottawa, ON, Canada, 2014. [Google Scholar]
- Viswanathan, M.; Ansari, M.; Berkman, N.; Chang, S.; Hartling, L.; McPheeters, L.; Santaguida, P.; Shamliyan, T.; Singh, K.; Tsertsvadze, A.; et al. Assessing the Risk of Bias of Individual Studies in Systematic Reviews of Health Care Interventions. Agency for healthcare research and quality methods guide for comparative effectiveness reviews. In AHRQ Methods for Effective Health Care; U.S. Department of Health & Human Services, Agency for Healthcare Research and Quality: Rockville, MD, USA, 2012. [Google Scholar]
- Gaspar, F.W.; Thiese, M.S.; Wizner, K.; Hegmann, K. Guideline adherence and lost workdays for acute low back pain in the California workers' compensation system. PLoS ONE 2021, 16, e0253268. [Google Scholar] [CrossRef] [PubMed]
- Shraim, M.; Cifuentes, M.; Willetts, J.L.; Marucci-Wellman, H.R.; Pransky, G. Why does the adverse effect of inappropriate MRI for LBP vary by geographic location? An exploratory analysis. BMC Musculoskelet Disord 2019, 20, 574. [Google Scholar] [CrossRef] [PubMed]
- Gross, D.P.; Stephens, B.; Bhambhani, Y.; Haykowsky, M.; Bostick, G.P.; Rashiq, S. Opioid prescriptions in canadian workers' compensation claimants: Prescription trends and associations between early prescription and future recovery. Spine (Phila Pa 1976) 2009, 34, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Cifuentes, M.; Webster, B.; Genevay, S.; Pransky, G. The course of opioid prescribing for a new episode of disabling low back pain: Opioid features and dose escalation. Pain 2010, 151, 22–29. [Google Scholar] [CrossRef]
- Verster, J.C.; Veldhuijzen, D.S.; Volkerts, E.R. Effects of an opioid (oxycodone/paracetamol) and an NSAID (bromfenac) on driving ability, memory functioning, psychomotor performance, pupil size, and mood. Clin. J. Pain 2006, 22, 499–504. [Google Scholar] [CrossRef]
- Deyo, R.A.; Von Korff, M.; Duhrkoop, D. Opioids for low back pain. BMJ 2015, 350, g6380. [Google Scholar] [CrossRef]
- Ashworth, J.; Green, D.J.; Dunn, K.M.; Jordan, K.P. Opioid use among low back pain patients in primary care: Is opioid prescription associated with disability at 6-month follow-up? Pain 2013, 154, 1038–1044. [Google Scholar] [CrossRef]
- Krause, N.; Dasinger, L.K.; Deegan, L.J.; Brand, R.J.; Rudolph, L. Alternative approaches for measuring duration of work disability after low back injury based on administrative workers' compensation data. Am. J. Ind. Med. 1999, 35, 604–618. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Setting and Data Source | Sample Size | Population |
|---|---|---|---|
| Gasper 2021 [36] | WC administrative database: California’s Department of Industrial Relations WC Information System | 59,656 cases with acute LBP from 2009 to 2018 | Mean age = 41 years, (SD = 12); 66.1% men |
| Shraim 2019 [37], 2015 [15] | WC administrative database: a single private insurer representing approximately 10% of the U.S. private WC market | 59,360 cases with acute LBP from 2002 to 2008 | Mean age = 39.4 years, SD = 10.8, 69.1% men |
| Lee 2016 [30] | WC administrative database: a single private insurer representing approximately 10% of the U.S. private WC market | 2887 cases with acute LBP from 2009 to 2011 | Mean age = 41 years, 61.7% men |
| Gross 2009 [38] | WC administrative database: WC board of Alberta | 47,784 cases from 2000 to 2005 with acute LBP | Mean age = 37 years, SD = 12, about 67.7% men |
| Webster 2007 [17] | WC administrative database: a single private insurer representing approximately 10% of the U.S. private WC market | 8443 cases with acute LBP from 2002 to 2003 | Mean age = 40.3 years, SD = 10.4, 71.8% men |
| Study | Selection | Comparability | Outcome | Total Quality Score |
|---|---|---|---|---|
| Gasper 2021 [36] | **** | *** | 7 | |
| Shraim 2019 [37] | **** | ** | *** | 9 |
| Lee 2016 [30] | **** | ** | *** | 9 |
| Shraim 2015 [15] | **** | ** | *** | 9 |
| Gross 2009 [38] | **** | * | *** | 8 |
| Webster 2007 [17] | **** | ** | *** | 9 |
| Study | Exposure | Variables Adjusted for in Multivariable Analysis | Association between EOP and LOD |
|---|---|---|---|
| Gasper 2021 [36] | Not reported | No report of adjusted variables. Descriptive statistics were used to assess the relationship between EOP and LOD. | The opioid group had a longer median LOD by 4 days when compared to the no opioid group (medians = 30 vs. 26 days). |
| Shraim 2019 [37] | MEA | Age, gender, tenure, industry, injury severity, early MRI, lumbar surgery, litigation status, live–work in the same state, wage replacement rate, waiting period, retroactive period, state medical fee schedule, treating provider choice, treating provider change, MRI facility rate, Wage replacement rate, State medical fee schedule, and unemployment rate. | Increase in EOP by 100 mg MEA was associated increase in mean LOD by 0.4 day (95% CI 0.3, 0.5). |
| Lee 2016 [30] | MEA | Adjusted for age, gender, job tenure, early MRI, and injury severity. | The EOP group had a higher mean LOD than the no EOP group (100.8 vs. 104 days). EOP was associated with an increased hazard of longer disability duration, but this was not statistically significant (hazard ratio 1.02, 95% CI 0.91, 1.13). |
| Shraim 2015 [15] | MEA | Age, gender, tenure, industry, injury severity, early MRI, lumbar surgery, litigation status, live-work in the same state, wage replacement rate, waiting period, retroactive period, state medical fee schedule, treating provider choice, and treating provider change. | Increase in EOP by 100 mg MEA was associated increase in LOD by 0.4 day (95% CI 0.3, 0.4). |
| Gross 2009 [38] | Not reported | Adjusted for age, gender, annual salary, year, number of previous claims, and injury type. | The EOP group had a higher hazard of continuation of time loss benefits by 1.94 (95% CI 1.86, 2.02). |
| Webster 2007 [17] | MEA | Adjusted for age, gender, job tenure, and lower back injury severity group. | As compared to subjects who did not receive EOP, subjects who received EOP had increased mean LOD days with increasing MEA dosage: 5.2 days (95% CI −14.6, 25.0) for 1–140 mg, 21.9 days (95% CI 3.2, 40.6) for 141–225 mg, 43.8 days (95% CI 23.7, 63.9) for 226–450 mg, and 69.1 (95% CI 49.3, 89.0) for 450+ mg. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, A.R.; Elgamal, M.E.; Moursi, M.O.; Shraim, B.A.; Shraim, M.A.; Shraim, M.; Al-Omari, B. The Association between Early Opioids Prescribing and the Length of Disability in Acute Lower Back Pain: A Systematic Review and Narrative Synthesis. Int. J. Environ. Res. Public Health 2022, 19, 12114. https://doi.org/10.3390/ijerph191912114
Ibrahim AR, Elgamal ME, Moursi MO, Shraim BA, Shraim MA, Shraim M, Al-Omari B. The Association between Early Opioids Prescribing and the Length of Disability in Acute Lower Back Pain: A Systematic Review and Narrative Synthesis. International Journal of Environmental Research and Public Health. 2022; 19(19):12114. https://doi.org/10.3390/ijerph191912114
Chicago/Turabian StyleIbrahim, Ayman R., Mohamed E. Elgamal, Moaz O. Moursi, Bara A. Shraim, Muath A. Shraim, Mujahed Shraim, and Basem Al-Omari. 2022. "The Association between Early Opioids Prescribing and the Length of Disability in Acute Lower Back Pain: A Systematic Review and Narrative Synthesis" International Journal of Environmental Research and Public Health 19, no. 19: 12114. https://doi.org/10.3390/ijerph191912114
APA StyleIbrahim, A. R., Elgamal, M. E., Moursi, M. O., Shraim, B. A., Shraim, M. A., Shraim, M., & Al-Omari, B. (2022). The Association between Early Opioids Prescribing and the Length of Disability in Acute Lower Back Pain: A Systematic Review and Narrative Synthesis. International Journal of Environmental Research and Public Health, 19(19), 12114. https://doi.org/10.3390/ijerph191912114