
Barriers and Facilitators to Participating in an Exercise Referral Scheme among Women Living in a Low Socioeconomic Area in Australia: A Qualitative Investigation Using the COM-B and Theoretical Domains Framework


{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
- Female;
- Aged 18 years or older;
- Registered with LLGA’s St Mary’s camp (Lang Park, St Mary’s, NSW, Australia) and either attended or not attended sessions;
- Living in St Mary’s.
2.3. Procedures
2.4. Analysis
2.5. Reflexivity
3. Results
3.1. Participant Characteristics
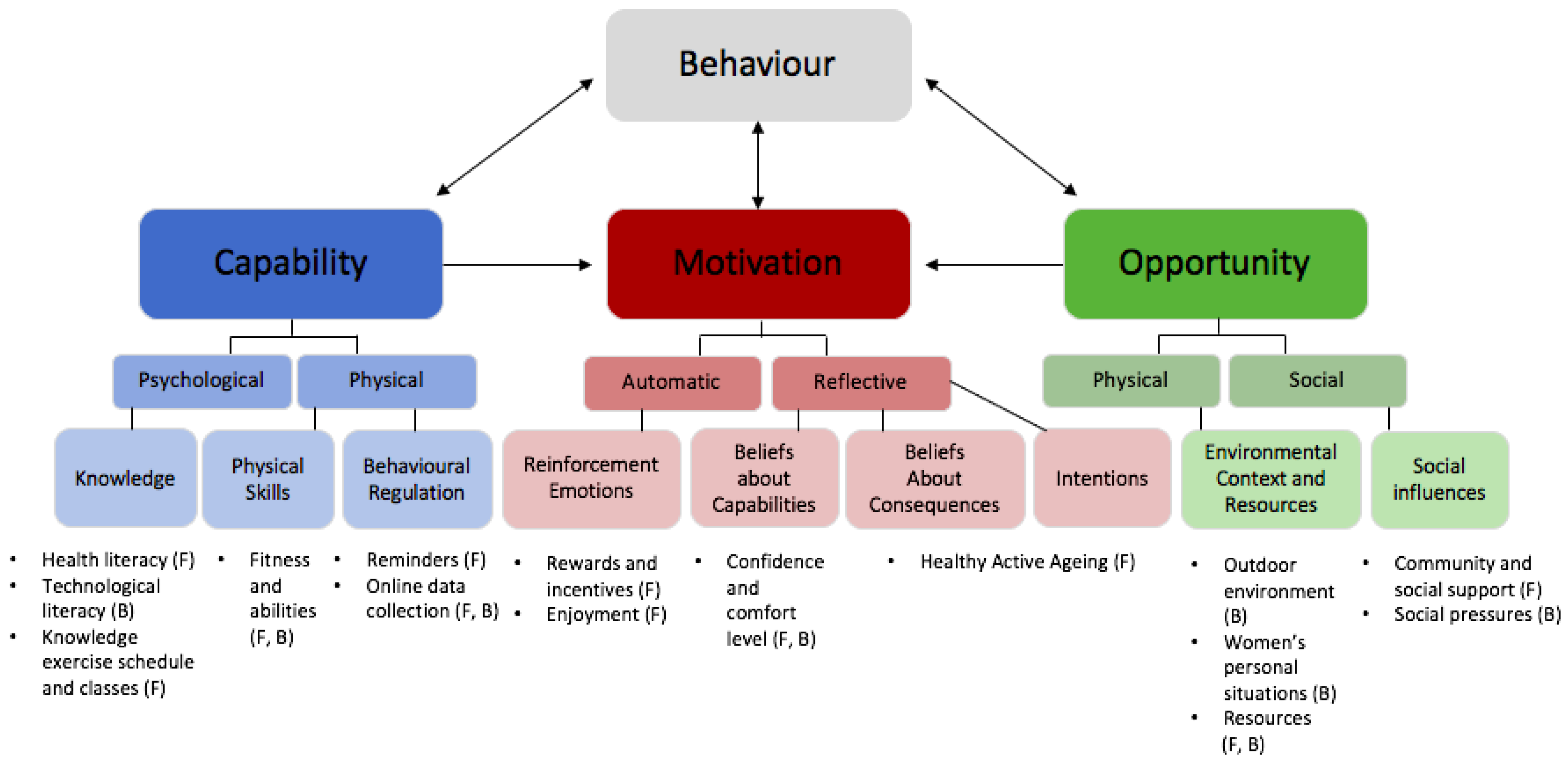
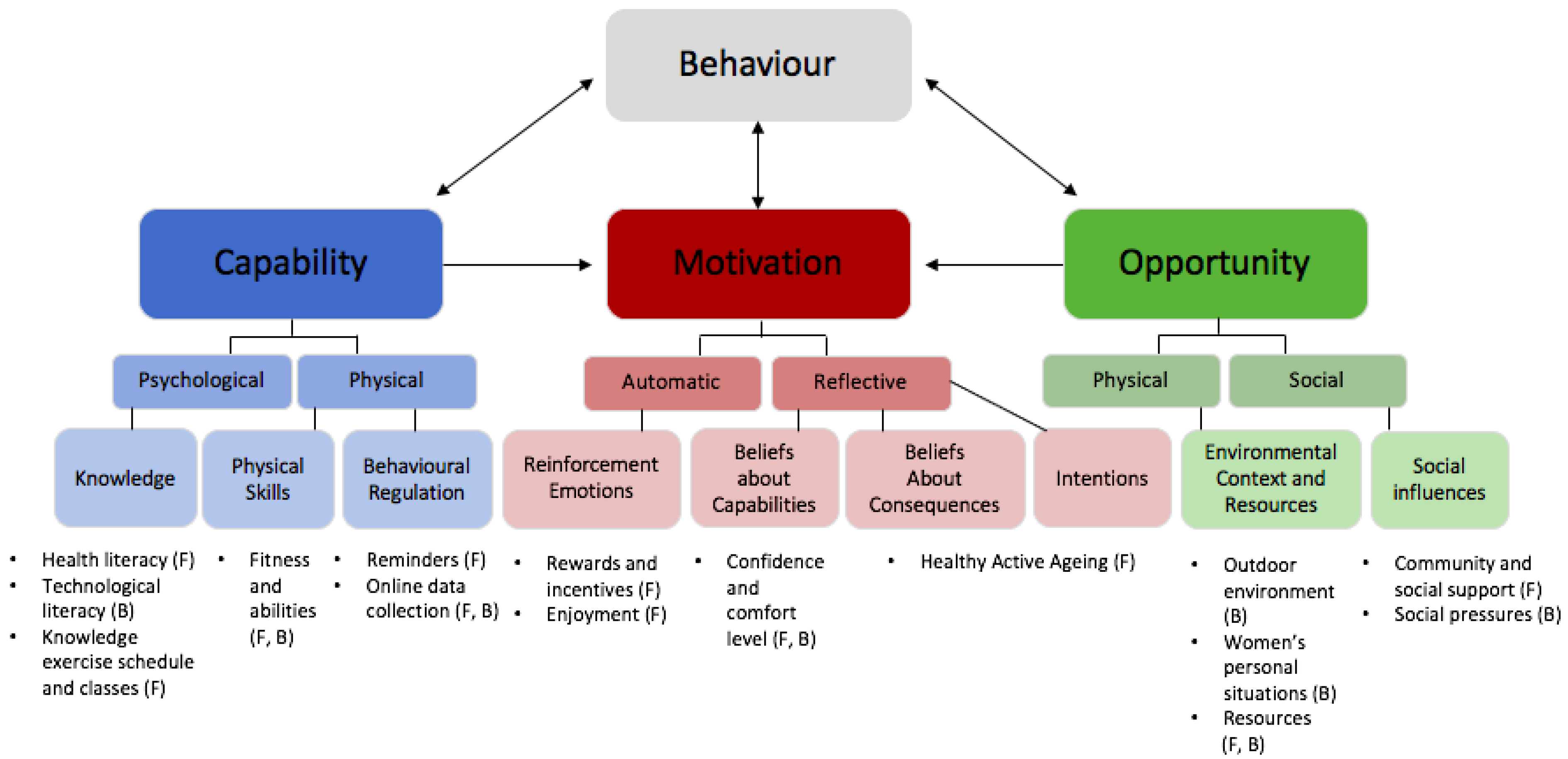
3.2. TDF and COM-B Analysis: Barriers and Facilitators to Using a Free Exercise Referral Scheme
3.3. Capability
3.3.1. Psychological Capability—Knowledge
- Health Literacy
- 2.
- Technological Literacy
“I have a friend who doesn’t even have a mobile phone. So that would definitely be a barrier for them.”—Elsie, 60
- 3.
- Knowledge Exercise Schedule and Classes
“I don’t even understand what some classes would entail like boxing, I think it was Box Fit. I’ve got no idea if that’s full on.”—Jada, 50
3.3.2. Physical Capability—Physical Skills
- Fitness and Abilities
“There are people of all different fitness levels, all different ages, and we all support each other to go further, within our journey.”—Jenny, 30
To increase attendance, it was suggested to include “an easier class for people who do have trouble getting up and getting down again.”—Mary, 69
3.3.3. Physical Capability—Behavioural Regulation
- Reminders
“I think a text message is a very good idea because sometimes you forget.”—Camila, 61
- 2.
- Online Data Collection
“I don’t like that either personally, always asking about your weight and if you’ve lost weight or if you’ve gained weight… I don’t want to be weighing myself all the time just to put that in, I mean because I don’t want to become obsessed with that.”—Camila, 61
“I think [the online data collection] is helpful and the trainers will acknowledge when people have been there for significant sessions.”—Elsie, 60
3.4. Opportunity
3.4.1. Physical Opportunity—Environmental Context and Resources
- Outdoor Environment
“In the morning most times are okay, but you know if you get those really hot days it’s a little bit hot. So you know that’s the downside of being outdoors. When it rains obviously it’s a bit of an issue as well.”—Mahlia, 67
“There used to be like people sort of drug users walking past. There was sort of undesirable people which would sort of walk past, and you have your belongings on the ground. I used to think I hope no one picks up my bag and runs off with it.”—Susan, 42
“I have to say that it does because I used to quite enjoy but now they all got bulldozed for houses and we’re going to have a massive housing development. And I like greenery. So you go on a walk, I want to walk where there’s trees and greenery and birds, and all that sort of stuff.”—Jada, 50
- 2.
- Women’s Personal Situations
“Truthfully, the fact that it was free. That was a big plus for me because, like I had stopped working and one of the reasons why I had, is you know I needed to help my daughter a little bit more with her child. So, I’ve found there’s people like me in those classes and so, you know, now I have to really watch money. I don’t know if it’s a good thing or not but certainly that was a big factor for me.”—Camila, 61
“I used to be involved in a gym but I’m on limited income so you know some gym memberships can get a little bit expensive”—Mahlia, 67
“…you know you’re tired, you’re raising a family. You’re working.”—Camila, 61
“… last year, we had a fantastic opportunity where a lady‘s son who was probably about eight, he exercised with us, and the trainer was so beautiful…. He said to the child hey, you can be my supervisor, you can make sure all the ladies are doing the exercise, and that it boosted the kids confidence so not just people without children, but people with children can feel comfortable there….”—Jenny, 30
- 3.
- Resources
“If the places have trainers from my community too. Someone knows them and then families and that go and support each other.”—Layla, 53
“If they have another program for the kids while the mums are doing the exercising the kids can too.”—Tess, 43
3.4.2. Social Opportunity—Social Support and Social Influences
- Community and Social Support
“I’d sort of told a couple of my other friends about it so like the three of us sort of like, you know, went together that first week, so you know like I knew somebody.”—Mahlia, 67
“You become friends with people and you tend to after training, you get to sit for five minutes and just chat and it might turn into, hey, what do you doing? Want to meet up at Woolworths and continue shopping together and get groceries?”—Tess, 43
- 2.
- Social Pressures
“Society has really created this persona that you have to look, act and afford to be able to be active…..Every time I wanted to go there [to a gym], I felt like I had to wear expensive clothing.”—Jenny, 30
“I have looked at going to gyms in the past, but I look at the machines and I don’t even know how to use them.”—Jada, 50
“My mental health didn’t feel comfortable being in a gym because of my social status, not having much money, and so, when I walked past Live Life Get Active I was like, they told me it was free they told me what they run, and I was just intrigued, because I since childhood has been a community person.”—Jenny, 30
3.5. Motivation
3.5.1. Automatic Motivation—Reinforcement Emotions
- Rewards and Incentives
“Every now and then maybe having some sort of competition. Sign up a friend or something.”—Elsie, 60
- 2.
- Enjoyment
“I do like going to a class, yeah I personally it’s not so much the social thing really, but yeah I do I do just love the structure of the class I like the instructor up there, the facilitator what do you call it and yeah, it is a bit social, that’s kind of a bonus but I just like the whole thing of a class.”—Camila, 61
3.5.2. Reflective Motivation—Beliefs about Capabilities
- Confidence and Comfort Level
“You’re able to get this confidence boost about you, you’re able to validate and feel proud of yourself.”—Jenny, 30
“I was attending some other classes, they were for over 50 s, or over 55 s and because I wasn’t all that confident about joining a regular open aged class.”—Mary, 69
3.5.3. Reflective Motivation—Beliefs about Consequences and Intentions
- Healthy Active Ageing
“If you don’t use it, you lose it, so it’s about health, staying flexible, getting less aches and pains, sort of wards off illness.”—Elsie, 60
“Weight loss is a bonus but it’s also getting to meet people, but also it’s something that I can do for me with, and, you know, like, and it does help mentally for me. It is a mental thing because I do have those mental challenges so it’s that 45 min of not thinking of all the other stuff and just focusing on me.”—Tess, 43
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Firth, J.; Solmi, M.; Wootton, R.E.; Vancampfort, D.; Schuch, F.; Hoare, E.; Gilbody, S.; Torous, J.; Teasdale, S.B.; Jackson, S.E.; et al. A meta-review of “lifestyle psychiatry”: The role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry 2020, 19, 360–380. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Physical Activity. Available online: https://www.who.int/westernpacific/health-topics/physical-activity (accessed on 25 May 2022).
- World Health Organization. Noncommunicable Diseases Country Profiles 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Katzmarzyk, P.T.; Friedenreich, C.; Shiroma, E.J.; Lee, I.M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sport. Med. 2022, 56, 101–106. [Google Scholar] [CrossRef]
- Rutter, H.; Cavill, N.; Bauman, A.; Bull, F. Systems approaches to global and national physical activity plans. Bull. World Health Organ. 2019, 97, 162–165. [Google Scholar] [CrossRef]
- Foley, B.C.; McLaughlin, M.; Edney, S.; Islam, S.M.S.; Seymour, J.; Peralta, L.R.; Douglas, A.; Rosenbaum, S.; Thorpe, H.; Atkin, J.; et al. “A 15% Reduction in Physical Inactivity Will Be Achieved in Australasia by 2030”—Audience Votes Negative in Online Debate. J. Phys. Act. Health 2021, 18, 1321–1324. [Google Scholar] [CrossRef]
- Gidlow, C.; Johnston, L.H.; Crone, D.; Ellis, N.; James, D. A systematic review of the relationship between socio-economic position and physical activity. Health Educ. J. 2006, 65, 338–367. [Google Scholar] [CrossRef]
- Fryers, T.; Melzer, D.; Jenkins, R. Social inequalities and the common mental disorders. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Montoye, H.J. Measuring Physical Activity and Energy Expenditure; Human Kinetics: Champaign, IL, USA, 1996; pp. 3–118. [Google Scholar]
- Alliott, O.; Ryan, M.; Fairbrother, H.; van Sluijs, E. Do adolescents’ experiences of the barriers to and facilitators of physical activity differ by socioeconomic position? A systematic review of qualitative evidence. Obes. Rev. 2022, 23, e13374. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Carver, A.; Downing, K.; Jackson, M.; O’Rourke, K. Addressing the social determinants of inequities in physical activity and sedentary behaviours. Health Promot. Int. 2015, 30 (Suppl. S2), ii8–ii19. [Google Scholar] [CrossRef]
- Teychenne, M.; White, R.L.; Richards, J.; Schuch, F.B.; Rosenbaum, S.; Bennie, J.A. Do we need physical activity guidelines for mental health: What does the evidence tell us? Ment. Health Phys. Act. 2020, 18, 100315. [Google Scholar] [CrossRef]
- Ball, K.; Carver, A.; Jackson, M.; Downing, K. Evidence Review: Addressing the Social Determinants of Inequities in Physical Activity and Related Health Outcomes; Victorian Health Promotion Foundation: Carlton South, Australia, 2015. [Google Scholar]
- Stalsberg, R.; Pedersen, A.V. Are differences in physical activity across socioeconomic groups associated with choice of physical activity variables to report? Int. J. Environ. Res. Public Health 2018, 15, 922. [Google Scholar] [CrossRef] [PubMed]
- Cleland, C.L.; Tully, M.A.; Kee, F.; Cupples, M.E. The effectiveness of physical activity interventions in socio-economically disadvantaged communities: A systematic review. Prev. Med. 2012, 54, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Salmon, J.; Giles-Corti, B.; Crawford, D. How can socio-economic differences in physical activity among women be explained? A qualitative study. Women Health 2006, 43, 93–113. [Google Scholar] [CrossRef] [PubMed]
- King, T.; Kavanagh, A.M.; Jolley, D.; Turrell, G.; Crawford, D. Weight and place: A multilevel cross-sectional survey of area-level social disadvantage and overweight/obesity in Australia. Int. J. Obes. 2006, 30, 281–287. [Google Scholar] [CrossRef]
- Wilson, D.K.; Kirtland, K.A.; Ainsworth, B.E.; Addy, C.L. Socioeconomic status and perceptions of access and safety for physical activity. Ann. Behav. Med. 2004, 28, 20–28. [Google Scholar] [CrossRef]
- Derose, K.P.; Han, B.; Williamson, S.; Cohen, D.A. Gender Disparities in Park Use and Physical Activity among Residents of High-Poverty Neighborhoods in Los Angeles. Women’s Health Issues 2018, 28, 6–13. [Google Scholar] [CrossRef]
- Morris, K.A.; Arundell, L.; Cleland, V.; Teychenne, M. Social ecological factors associated with physical activity and screen time amongst mothers from disadvantaged neighbourhoods over three years. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 110. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sport Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Sfm, C.; Van Cauwenberg, J.; Maenhout, L.; Cardon, G.; Lambert, E.V.; Van Dyck, D. Inequality in physical activity, global trends by income inequality and gender in adults. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 142. [Google Scholar] [CrossRef]
- Doan, T.; Yu, P.; LaBond, C.; Gong, C.; Strazdins, L. Time for Physical Activity: Different, Unequal, Gendered. J. Health Soc. Behav. 2022, 63, 37–54. [Google Scholar] [CrossRef]
- Nayak, M.; Wills, K.; Teychenne, M.; Salmon, J.; Cleland, V. Patterns and Predictors of Sitting among Women from Disad-Vantaged Neighbourhoods over Time: A 5-Year Prospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 4625. [Google Scholar] [CrossRef] [PubMed]
- Droomers, M.; Schrijvers, C.T.; Mackenbach, J.P. Educational level and decreases in leisure time physical activity: Predictors from the longitudinal GLOBE study. J. Epidemiol. Community Health 2001, 55, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Cockerham, W.C.; Hamby, B.W.; Oates, G.R. The social determinants of chronic disease. Am. J. Prev. Med. 2017, 52, S5–S12. [Google Scholar] [CrossRef]
- Hankivsky, O. Women’s health, men’s health, and gender and health: Implications of intersectionality. Soc. Sci. Med. 2012, 74, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Mielke, G.I.; Malta, D.C.; Nunes, B.P.; Cairney, J. All are equal, but some are more equal than others: Social determinants of leisure time physical activity through the lens of intersectionality. BMC Public Health 2022, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Morgan, F.; Battersby, A.; Weightman, A.L.; Searchfield, L.; Turley, R.; Morgan, H.; Jagroo, J.; Ellis, S. Adherence to exercise referral schemes by participants–what do providers and commissioners need to know? A systematic review of barriers and facilitators. BMC Public Health 2016, 16, 36. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.L.; Oliver, E.J.; Dodd-Reynolds, C.J.; Allin, L.J. How do participant experiences and characteristics influence engagement in exercise referral? A qualitative longitudinal study of a scheme in Northumberland, UK. BMJ Open 2019, 9, e024370. [Google Scholar] [CrossRef]
- Eynon, M.; Foad, J.; Downey, J.; Bowmer, Y.; Mills, H. Assessing the psychosocial factors associated with adherence to exercise referral schemes: A systematic review. Scand. J. Med. Sci. Sport. 2019, 29, 638–650. [Google Scholar] [CrossRef]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Flannery, C.; McHugh, S.; Anaba, A.E.; Clifford, E.; O’Riordan, M.; Kenny, L.C.; McAuliffe, F.M.; Kearney, P.M.; Byrne, M. Enablers and barriers to physical activity in overweight and obese pregnant women: An analysis informed by the theoretical domains framework and COM-B model. BMC Pregnancy Childbirth 2018, 18, 178. [Google Scholar] [CrossRef] [PubMed]
- Bentley, M.R.N.; Mitchell, N.; Sutton, L.; Backhouse, S.H. Sports nutritionists’ perspectives on enablers and barriers to nutritional adherence in high performance sport: A qualitative analysis informed by the COM-B model and theoretical domains framework. J. Sport. Sci. 2019, 37, 2075–2085. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M.; et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, C.; Atkinson, S.; Doody, O. Employing a qualitative description approach in health care research. Glob. Qual. Nurs. Res. 2017, 4, 2333393617742282. [Google Scholar] [CrossRef]
- Mackenzie, N.; Knipe, S. Research dilemmas: Paradigms, methods and methodology. Issues Educ. Res. 2006, 16, 193–205. [Google Scholar]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- ABS. Socio-Economic Indexes for Areas (SEIFA) 2016. Available online: http://www.abs.gov.au/ausstats/[email protected]/mf/2033.0.55.001 (accessed on 15 April 2022).
- Australian Bureau of Statistics. Census of Population and Housing 2006; Australian Bureau of Statistics: Camberra, Australia, 2016. [Google Scholar]
- McDonagh, L.K.; Saunders, J.M.; Cassell, J.; Curtis, T.; Bastaki, H.; Hartney, T.; Rait, G. Application of the COM-B model to barriers and facilitators to chlamydia testing in general practice for young people and primary care practitioners: A systematic review. Implement. Sci. 2018, 13, 1–19. [Google Scholar] [CrossRef]
- Pozzan, E.; Cattaneo, U. Women Health Workers: Working Relentlessly in Hospitals and at Home; International Labour Organisation: Geneva, Switzerland, 2020. Available online: https://www.ilo.org/tokyo/information/pr/WCMS_741060/lang--en/index.htm (accessed on 15 April 2022).
- Moreira da Silva, J. Why You Should Care about Unpaid Care Work; OECD: Paris, France, 2019. [Google Scholar]
- Pridgeon, L.; Grogan, S. Understanding exercise adherence and dropout: An interpretative phenomenological analysis of men and women’s accounts of gym attendance and non-attendance. Qual. Res. Sport Exerc. Health 2012, 4, 382–399. [Google Scholar] [CrossRef]
- Foster, S.; Giles-Corti, B. The built environment, neighborhood crime and constrained physical activity: An exploration of inconsistent findings. Prev. Med. 2008, 47, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Pearce, J.; Mitchell, R.; Kingham, S. Role of physical activity in the relationship between urban green space and health. Public Health 2013, 127, 318–324. [Google Scholar] [CrossRef]
- Schmidt, M.; Absalah, S.; Nierkens, V.; Stronks, K. Which factors engage women in deprived neighbourhoods to participate in exercise referral schemes? BMC Public Health 2008, 8, 371. [Google Scholar] [CrossRef] [PubMed]
- Milkman, K.L.; Gromet, D.; Ho, H.; Kay, J.S.; Lee, T.W.; Pandiloski, P.; Park, Y.; Rai, A.; Bazerman, M.; Beshears, J. Megastudies improve the impact of applied behavioural science. Nature 2021, 600, 478–483. [Google Scholar] [CrossRef]
- Burgoyne, L.N.; Woods, C.; Coleman, R.; Perry, I.J. Neighbourhood perceptions of physical activity: A qualitative study. BMC Public Health 2008, 8, 101. [Google Scholar] [CrossRef]
- Kivimäki, M.; Batty, G.D.; Pentti, J.; Shipley, M.J.; Sipilä, P.N.; Nyberg, S.T.; Suominen, S.B.; Oksanen, T.; Stenholm, S.; Virtanen, M. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: A multi-cohort study. Lancet Public Health 2020, 5, e140–e149. [Google Scholar]
- Rowlands, J. Interviewee Transcript Review as a Tool to Improve Data Quality and Participant Confidence in Sensitive Research. Int. J. Qual. Methods 2021, 20, 16094069211066170. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McKeon, G.; Mastrogiovanni, C.; Teychenne, M.; Rosenbaum, S. Barriers and Facilitators to Participating in an Exercise Referral Scheme among Women Living in a Low Socioeconomic Area in Australia: A Qualitative Investigation Using the COM-B and Theoretical Domains Framework. Int. J. Environ. Res. Public Health 2022, 19, 12312. https://doi.org/10.3390/ijerph191912312
McKeon G, Mastrogiovanni C, Teychenne M, Rosenbaum S. Barriers and Facilitators to Participating in an Exercise Referral Scheme among Women Living in a Low Socioeconomic Area in Australia: A Qualitative Investigation Using the COM-B and Theoretical Domains Framework. International Journal of Environmental Research and Public Health. 2022; 19(19):12312. https://doi.org/10.3390/ijerph191912312
Chicago/Turabian StyleMcKeon, Grace, Chiara Mastrogiovanni, Megan Teychenne, and Simon Rosenbaum. 2022. "Barriers and Facilitators to Participating in an Exercise Referral Scheme among Women Living in a Low Socioeconomic Area in Australia: A Qualitative Investigation Using the COM-B and Theoretical Domains Framework" International Journal of Environmental Research and Public Health 19, no. 19: 12312. https://doi.org/10.3390/ijerph191912312
APA StyleMcKeon, G., Mastrogiovanni, C., Teychenne, M., & Rosenbaum, S. (2022). Barriers and Facilitators to Participating in an Exercise Referral Scheme among Women Living in a Low Socioeconomic Area in Australia: A Qualitative Investigation Using the COM-B and Theoretical Domains Framework. International Journal of Environmental Research and Public Health, 19(19), 12312. https://doi.org/10.3390/ijerph191912312