
Therapeutic Approaches for ADHD by Developmental Stage and Clinical Presentation

 ,
, 
Abstract
:1. Introduction
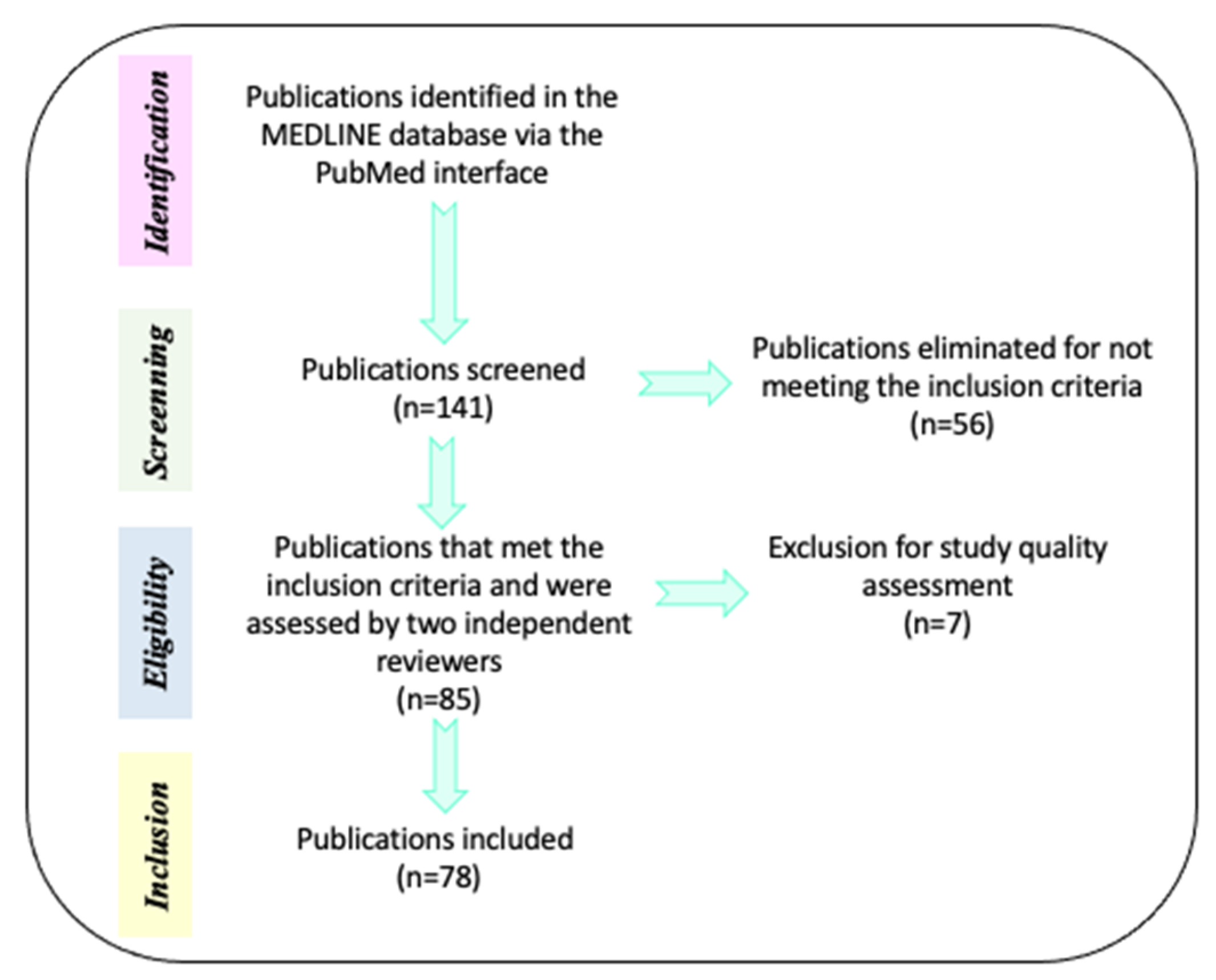
2. Materials and Methods
3. Results
3.1. Efficacy of Pharmacological Treatment According to Patients’ Development
3.2. Efficacy of the Neuropsychological Treatment According to Patients’ Development
3.3. Efficacy of Psychosocial Treatment According to Patients’ Development
- Behavioral techniques, based on rewards or punishments, that seek to generate more adaptive behaviors.
- Cognitive techniques that identify maladaptive beliefs and replace them with others that generate better adaptation, i.e., cognitive restructuring or rehabilitation.
- Combination of cognitive and behavioral techniques at a group or individual level.
- Training in organizational and/or social skills.
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, US, 2013; pp. 31–86. [Google Scholar]
- National Institutes of Health Consensus Development Conference Statement: Diagnosis and treatment of attention-deficit/hyperactivity disorder (ADHD). J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 182–193. [CrossRef]
- Andersen, S.L. Trajectories of brain development: Point of vulnerability or window of opportunity? Neurosci. Biobehav. Rev. 2003, 27, 3–18. [Google Scholar] [CrossRef] [Green Version]
- Mowlem, F.D.; Rosenqvist, M.A.; Martin, J.; Lichtenstein, P.; Asherson, P.; Larsson, H. Sex differences in predicting ADHD clinical diagnosis and pharmacological treatment. Eur. Child Adolesc. Psychiatry 2018, 28, 481–489. [Google Scholar] [CrossRef] [Green Version]
- Willcutt, E.G. The Prevalence of DSM-IV Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Greenhill, L.L.; Posner, K.; Vaughan, B.S.; Kratochvil, C.J. Attention Deficit Hyperactivity Disorder in Preschool Children. Child. Adolesc. Psychiatry Clin. N. Am. 2008, 17, 347–366. [Google Scholar] [CrossRef]
- Young, S.; Yoon, R.; Ravi, U.; Michael, C. Sleep and daytime function in adults with attention-deficit / hyperactivity disorder: Subtype differences. Sleep Med. Rev. 2013, 14, 648–655. [Google Scholar] [CrossRef]
- Lahey, B.B.; Pelham, W.E.; Loney, J.; Lee, S.S.; Willcutt, E. Instability of the DSM-IV Subtypes of ADHD From Preschool Through Elementary School. Arch. Gen. Psychiatry 2005, 62, 896. [Google Scholar] [CrossRef] [PubMed]
- Charach, A.; Dashti, B.; Carson, P.; Booker, L.; Lim, C.G.; Lillie, E.; Schachar, R. Attention Deficit Hyperactivity Disorder. Attention Deficit Hyperactivity Disorder: Effectiveness of Treatment in At-Risk Preschoolers; Long-Term Effectiveness in All Ages and Variability in Prevalence, Diagnosis, and Treatment; Agency for Healthcare Research and Quality: North Bethesda, MA, US, 2011. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22191110 (accessed on 4 October 2021).
- Chronis, A.M.; Jones, H.A.; Raggi, V.L. Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Clin. Psychol. Rev. 2006, 26, 486–502. [Google Scholar] [CrossRef]
- Hébert, J.; Cand, A.P.; Joober, R. Adherence to Psychostimulant Medication in Children with. J. Can. Acad. Child Adolesc. Psychiatry 2013, 22, 317–324. [Google Scholar]
- Barbaresi, W.J.; Katusic, S.K.; Colligan, R.C.; Weaver, A.L.; Jacobsen, S.J. Modifiers of Long-Term School Outcomes for Children with Attention-Deficit/Hyperactivity Disorder: Does Treatment with Stimulant Medication Make a Difference? Results from a Population-Based Study. J. Dev. Behav. Pediatr. 2007, 28, 274–287. [Google Scholar] [CrossRef]
- Caye, A.; Swanson, J.M.; Coghill, D.; Rohde, L.A. Treatment strategies for ADHD: An evidence-based guide to select optimal treatment. Mol. Psychiatry 2019, 24, 390–408. [Google Scholar] [CrossRef] [PubMed]
- Minzenberg, M.J. Pharmacotherapy for Attention-Deficit/Hyperactivity Disorder: From Cells to Circuits. Neurotherapeutics 2012, 9, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Cortese, S. Pharmacologic Treatment of Attention Deficit–Hyperactivity Disorder. N. Engl. J. Med. 2020, 383, 1050–1056. [Google Scholar] [CrossRef]
- Liu, Q.; Zhang, H.; Fang, Q.; Qin, L. Comparative efficacy and safety of methylphenidate and atomoxetine for attention-deficit hyperactivity disorder in children and adolescents: Meta-analysis based on head-to-head trials. J. Clin. Exp. Neuropsychol. 2017, 39, 854–865. [Google Scholar] [CrossRef]
- Stuhec, M.; Luki, P.; Locatelli, I. Efficacy, Acceptability, and Tolerability of Lisdexamfetamine, Mixed Amphetamine Salts, Methylphenidate, and Modafinil in the Treatment of Attention-Deficit Hyperactivity Disorder in Adults: A Systematic Review and Meta-analysis. Ann. Pharmacother. 2019, 53, 121–133. [Google Scholar] [CrossRef]
- Krogh, H.B.; Storebø, O.J.; Faltinsen, E.; Todorovac, A.; Ydedahl-Jensen, E.; Magnusson, F.L.; Simonsen, E. Methodological advantages and disadvantages of parallel and crossover randomised clinical trials on methylphenidate for attention deficit hyperactivity disorder: A systematic review and meta-analyses. BMJ Open 2019, 9, e026478. [Google Scholar] [CrossRef] [Green Version]
- Wilens, T.E. Effects of Methylphenidate on the Catecholaminergic System in Attention-Deficit/Hyperactivity Disorder. J. Clin. Psychopharmac. 2008, 28, S46–S53. [Google Scholar] [CrossRef]
- Huang, Y.S.; Tsai, M.H. Long-Term Outcomes with Medications for Attention-Deficit Hyperactivity Disorder. CNS Drugs 2011, 25, 539–554. [Google Scholar] [CrossRef]
- Mardomingo-Sanz, M.J. Clinical use of 30:70 controlled-release methylphenidate in the treatment of attention deficit hyperactivity disorder. Rev. Neurol. 2012, 55, 359–369. [Google Scholar] [PubMed]
- Zetterström, T.S.C. Chronic methylphenidate preferentially alters catecholamine protein targets in the parietal cortex and ventral striatum. Neurochem. Int. 2019, 124, 193–199. [Google Scholar] [CrossRef]
- Pietrzak, R.; Mollica, C.; Maruff, P.; Snyder, P. Cognitive effects of immediate-release methylphenidate in children with attention-deficit/hyperactivity disorder. Neurosci. Biobehav. Rev. 2006, 30, 1225–1245. [Google Scholar] [CrossRef] [PubMed]
- Zehle, S.; Bock, J.; Jezierski, G.; Gruss, M.; Braun, K. Methylphenidate treatment recovers stress-induced elevated dendritic spine densities in the rodent dorsal anterior cingulate cortex. Dev. Neurobiol. 2007, 67, 1891–1900. [Google Scholar] [CrossRef] [PubMed]
- Kodama, T.; Kojima, T.; Honda, Y.; Hosokawa, T.; Tsutsui, K.I.; Watanabe, M. Oral administration of methylphenidate (Ritalin) differentially affects dopamine release between the prefrontal cortex and striatum-a microdialysis study in the monkey. J. Neurosci. 2017, 37, 2116–2155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.P.; Bédard, A.C.V.; Fan, J.; Hildebrandt, T.B.; Stein, M.A.; Ivanov, I.; Halperin, J.M.; Newcorn, J.H. Striatal Activation Predicts Differential Therapeutic Responses to Methylphenidate and Atomoxetine. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 602–609. [Google Scholar] [CrossRef]
- Nakanishi, Y.; Ota, T.; Iida, J.; Yamamuro, K.; Kishimoto, N.; Okazaki, K.; Kishimoto, T. Differential therapeutic effects of atomoxetine and methylphenidate in childhood attention deficit/hyperactivity disorder as measured by near-infrared spectroscopy. Child Adolesc. Psychiatr. Ment. Health 2017, 11, 26. [Google Scholar] [CrossRef] [Green Version]
- Ozdemir, E.; Karaman, M.G.; Yurteri, N.; Erdogan, A. A case of suicide attempt with long-acting methylphenidate (Concerta). ADHD Atten. Def. Hyp. Disord. 2010, 2, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Krishna, A.S.; Lefevre, C.; Kaagaza, M.; Wittkamp, M. Methylphenidate Overdose Causing Secondary Polydipsia and Severe Hyponatremia in an 8-Year-Old Boy. Pediatr. Emerg. Care 2017, 33, e55–e57. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Xiong, Z.; Duffney, L.J.; Wei, J.; Liu, A.; Liu, S.; Chen, G.J.; Yan, Z. Methylphenidate Exerts Dose-Dependent Effects on Glutamate Receptors and Behaviors. Biol. Psychiatry 2014, 76, 953–962. [Google Scholar] [CrossRef] [Green Version]
- Huss, M.; Duhan, P.; Gandhi, P.; Chen, C.W.; Spannhuth, C.; Kumar, V. Methylphenidate dose optimization for ADHD treatment: Review of safety, efficacy, and clinical necessity. Neuropsychiatr. Dis. Treat. 2017, 13, 1741–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyer, C.; Staunton, C.; Moodley, K. The implications of Methylphenidate use by healthy medical students and doctors in South Africa. BMC Medic. Ethics 2014, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kortekaas-Rijlaarsdam, A.F.; Luman, M.; Sonuga-Barke, E.; Bet, P.M.; Oosterlaan, J. Short-term effects of methylphenidate on math productivity in children with attention-deficit/hyperactivity disorder are mediated by symptom improvements: Evidence from a placebo-controlled trial. J. Clin. Psychopharmacol. 2017, 37, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Masi, G.; Manfredi, A.; Nieri, G.; Muratori, P.; Pfanner, C.; Milone, A. A Naturalistic Comparison of Methylphenidate and Risperidone Monotherapy in Drug-Naive Youth with Attention-Deficit/Hyperactivity Disorder Comorbid with Oppositional Defiant Disorder and Aggression. J. Clin. Psychopharmacol. 2017, 37, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Golubchik, P.; Shalev, L.; Tsamir, D.; Manor, I.; Weizman, A. High pretreatment cognitive impulsivity predicts response of oppositional symptoms to methylphenidate in patients with attention-deficit hyperactivity disorder/oppositional defiant disorder. Int. Clin. Psychopharmacol. 2019, 34, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Reynaud, A.J.; Froesel, M.; Guedj, C.; Ben Hadj Hassen, S.; Cléry, J.; Meunier, M.; Hadj-Bouziane, F. Atomoxetine improves attentional orienting in a predictive context. Neuropharmacology 2019, 150, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Clemow, D.B.; Nyhuis, A.W.; Robinson, R.L. Clinical Impact of Not Achieving Recommended Dose on Duration of Atomoxetine Treatment in Adults with Attention-Deficit/Hyperactivity Disorder. CNS Neurosci. Ther. 2016, 22, 970–978. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, J. Best-worst multi-criteria decision-making method: Some properties and a linear model. Omega 2016, 16, 126–130. [Google Scholar] [CrossRef]
- Verplaetse, T.L.; Roberts, W.; Moore, K.E.; Peltier, M.R.; Oberleitner, L.M.; McKee, S.A. Pharmacokinetics and Pharmacodynamics of Immediate-Release Versus Extended-Release Guanfacine in Adult Daily Smokers. J. Clin. Psychopharmacol. 2019, 39, 124–128. [Google Scholar] [CrossRef]
- Iwanami, A.; Saito, K.; Fujiwara, M.; Okotsu, D.; Ichikawa, H. Efficacy and Safety of Guanfacine Extended-Release in the Treatment of Attention-Deficit/Hyperactivity Disorder in Adults: Results of a Randomized, Double-Blind, Placebo-Controlled Study. J. Clin. Psychiatr. 2020, 81, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Okazaki, K.; Yamamuro, K.; Iida, J.; Kishimoto, T. Guanfacine monotherapy for ADHD/ASD comorbid with Tourette syndrome: A case report. Ann. Gen. Psychiatr. 2019, 150, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Okada, M.; Fukuyama, K.; Kawano, Y.; Shiroyama, T.; Suzuki, D.; Ueda, Y. Effects of acute and sub-chronic administrations of guanfacine on catecholaminergic transmissions in the orbitofrontal cortex. Neuropharmacology 2019, 156, 107547. [Google Scholar] [CrossRef]
- Fitzpatrick, C.M.; Andreasen, J.T. Differential effects of ADHD medications on impulsive action in the mouse 5-choice serial reaction time task. Eur. J. Pharmacol. 2019, 847, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. Lancet Psychiatry 2018, 5, 727–738. [Google Scholar] [CrossRef] [Green Version]
- Bastiaens, L.; Scott, O.; Galus, J. Treatment of Adult ADHD without Stimulants: Effectiveness in A Dually Diagnosed Correctional Population. Psychiatr. Q. 2019, 90, 41–46. [Google Scholar] [CrossRef]
- Pievsky, M.A.; McGrath, R.E. The Neurocognitive Profile of Attention-Deficit/Hyperactivity Disorder: A Review of Meta-Analyses. Arch. Clin. Neuropsychol. 2018, 33, 143–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadi, M.R.; Araghi, S.M.; Zarafshan, H. Neurocognitive Profile of Children with Attention Deficit Hyperactivity Disorders (ADHD): A comparison between subtypes. Iran. J. Psychiatry 2014, 9, 197–202. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25792987 (accessed on 1 November 2021).
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellanos, F.X.; Tannock, R. Neuroscience of attention-deficit/hyperactivity disorder: The search for endophenotypes. Nat. Rev. Neurosc. 2002, 3, 617–628. [Google Scholar] [CrossRef]
- Diamond, A. Attention-deficit disorder (attention-deficit/ hyperactivity disorder without hyperactivity): A neurobiologically and behaviorally distinct disorder from attention-deficit/hyperactivity disorder (with hyperactivity). Dev. Psychopathol. 2005, 17, 807–825. [Google Scholar] [CrossRef] [Green Version]
- Biederman, J.; Newcorn, J.; Sprich, S. Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety, and other disorders. Am. J. Psychiatry 1991, 148, 564–577. [Google Scholar] [CrossRef] [Green Version]
- Daley, D.; Birchwood, J. ADHD and academic performance: Why does ADHD impact on academic performance and what can be done to support ADHD children in the classroom? Child Care Health. Dev. 2010, 36, 455–464. [Google Scholar] [CrossRef]
- Shuai, L.; Daley, D.; Wang, Y.F.; Zhang, J.S.; Kong, Y.T.; Tan, X.; Ji, N. Executive function training for children with attention deficit hyperactivity disorder. Chin. Med. J. 2017, 130, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Bahçivan Saydam, R.; Ayvaşik, H.B.; Alyanak, B. Executive Functioning in Subtypes of Attention Deficit Hyperactivity Disorder. Noro Psikiyatr. Ars. 2015, 52, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Ferrin, M.; Brandeis, D.; Buitelaar, J.; Daley, D.; Dittmann, R.W.; Holtmann, M.; Santosh, P.; Stevenson, J.; Stringaris, A.; et al. Cognitive training for attention-deficit/hyperactivity disorder: Meta-analysis of clinical and neuropsychological outcomes from randomized controlled trials. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 164–174. [Google Scholar] [CrossRef] [Green Version]
- Chan, E.; Fogler, J.M.; Hammerness, P.G. Treatment of Attention-Deficit/Hyperactivity Disorder in Adolescents. Jama 2016, 315, 1997. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, G.A.; Schatz, N.K.; Aloe, A.M.; Chacko, A.; Chronis-Tuscano, A. A Systematic Review of Meta-Analyses of Psychosocial Treatment for Attention-Deficit/Hyperactivity Disorder. Clin. Child. Fam. Psychol. Rev. 2015, 18, 77–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikic, A.; Reichow, B.; McCauley, S.A.; Ibrahim, K.; Sukhodolsky, D.G. Meta-analysis of organizational skills interventions for children and adolescents with Attention-Deficit/Hyperactivity Disorder. Clin. Psychol. Rev. 2017, 52, 108–123. [Google Scholar] [CrossRef]
- Serrano-Troncoso, E.; Guidi, M.; Alda-Díez, J.Á. ¿Es el tratamiento psicológico eficaz para el trastorno por déficit de atención con hiperactividad (TDAH)? Revisión sobre los tratamientos no farmacológicos en niños y adolescentes con TDAH. (Spanish). Actas Esp. Psiquiatry 2013, 41, 44–51. Available online: http://search.ebscohost.com/login.aspx?direct=true&db=fua&AN=87688096&lang=es&site=ehost-live (accessed on 1 November 2021).
- Sibley, M.H.; Kuriyan, A.B.; Evans, S.W.; Waxmonsky, J.G.; Smith, B.H. Pharmacological and psychosocial treatments for adolescents with ADHD: An updated systematic review of the literature. Clin. Psychol. Rev. 2014, 34, 218–232. [Google Scholar] [CrossRef]
- Burke, J.D.; Rolf, L.; Birmaher, B. Oppositional Defiant Disorder and Conduct Disorder: A Review of the Past 10 Years, Part II. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 1275–1293. [Google Scholar] [CrossRef] [Green Version]
- Connor, D.F.; Glatt, S.J.; Lopez, I.D.; Jackson, D.; Melloni, R.H. Psychopharmacology and Aggression. I: A Meta-Analysis of Stimulant Effects on Overt/Covert Aggression–Related Behaviors in ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 253–261. [Google Scholar] [CrossRef]
- Pelham, W.E.; Fabiano, G.A. Evidence-Based Psychosocial Treatments for Attention-Deficit/Hyperactivity Disorder. J. Clin. Child Adolesc. Psychol. 2008, 37, 184–214. [Google Scholar] [CrossRef]
- Evans, S.W.; Owens, J.S.; Bunford, N. Evidence-Based Psychosocial Treatments for Children and Adolescents Evidence-Based Psychosocial Treatments for Children and Adolescents with Disruptive Behavior. J. Clin. Child Adolesc. Psychol. 2014, 43, 527–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakashima, M.; Inada, N.; Tanigawa, Y.; Yamashita, M.; Maeda, E.; Kouguchi, M.; Sarad, Y.; Yano, H.; Ikari, K.; Kuga, H.; et al. Efficacy of Group Cognitive Behavior Therapy Targeting Time Management for Adults with Attention Deficit/Hyperactivity Disorder in Japan: A Randomized Control Pilot Trial. J. Atten. Disord. 2021, 26, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Estrada, R.; Bosch-Munso, R.; Nogueira-Morais, M.; Casas-Brugue, M.; Ramos-Quiroga, J.A. Psychological treatment of attention deficit hyperactivity disorder in adults: A systematic review. Actas Españolas De Psiquiatr. 2012, 40, 147–154. Available online: http://content.ebscohost.com.paloaltou.idm.oclc.org/ContentServer.asp?T=P&P=AN&K=22723133&S=R&D=mnh&EbscoContent=dGJyMNHX8kSep7E4zdnyOLCmr0qepq9Ssaq4SLaWxWXS&ContentCustomer=dGJyMPGut1CzrLZRuePfgeyx44Dt6fIA%5Cnhttps://paloaltou.idm.oclc.org/login?url=http (accessed on 5 November 2021).
- Faraone, S.V.; Biederman, J.; Weber, W.; Russell, R.L. Psychiatric, Neuropsychological, and Psychosocial Features of DSM-IV Subtypes of Attention-Deficit/Hyperactivity Disorder: Results from a Clinically Referred Sample. J. Am. Acad. Child Adolesc. Psychiatry 1998, 37, 185–193. [Google Scholar] [CrossRef]
- Mayes, S.D.; Calhoun, S.L.; Chase, G.A.; Mink, D.M.; Stagg, R.E. ADHD Subtypes and Co-Occurring Anxiety, Depression, and Oppositional-Defiant Disorder. Differences in Gordon Diagnostic System and Wechsler Working Memory and Processing Speed Index Scores. J. Atten. Disord. 2009, 12, 540–550. [Google Scholar] [CrossRef]
- Milich, R. ADHD Combined Type and ADHD Predominantly Inattentive Type Are Distinct and Unrelated Disorders. Clin. Psychl. Sci. Pract. 2001, 8, 463–488. [Google Scholar] [CrossRef]
- Power, T.J.; Costigan, T.E.; Eiraldi, R.B.; Leff, S.S. Variations in Anxiety and Depression as a Function of ADHD Subtypes Defined by DSM-IV: Do Subtype Differences Exist or Not? J. Abnorm. Child Psychol. 2004, 32, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Presentación, M.J.; Siegenthaler, R. Problemática asociada al TDAH subtipo combinado en una muestra escolar. Infanc. Aprendiz. 2005, 28, 261–275. [Google Scholar] [CrossRef]
- van den Hoofdakker, B.J.; van der Veen-Mulders, L.; Sytema, S.; Emmelkamp, P.M.G.; Minderaa, R.B.; Nauta, M.H. Effectiveness of behavioral parent training for children with ADHD in routine clinical practice: A randomized controlled study. J. Am. Acad. Child. Adolesc. Psychiatry 2007, 46, 1263–1271. [Google Scholar] [CrossRef]
- Jensen, C.M.; Amdisen, B.L.; Jørgensen, K.J.; Arnfred, S.M. Cognitive behavioural therapy for ADHD in adults: Systematic review and meta-analyses. ADHD Atten. Deficit Hyperact. Disord. 2016, 8, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Fullen, T.; Galab, N.; Abbott, K.A.; Adamou, M. Acceptance and Commitment Therapy for Adults with ADHD during COVID-19: An Open Trial. Open J. Psychiatry 2020, 10, 205. [Google Scholar] [CrossRef]
- Gadow, K.D.; Drabick, D.A.G.; Loney, J.; Sprafkin, J.; Salisbury, H.; Azizian, A.; Schwartz, J. Comparison of ADHD symptom subtypes as source-specific syndromes. J. Child Psychol. Psychiatry 2004, 45, 1135–1149. [Google Scholar] [CrossRef] [PubMed]
- Nolan, E.E.; Volpe, R.J.; Gadow, K.D.; Sprafkin, J. Developmental, Gender, and Comorbidity Differences in Clinically Referred Children with ADHD. J. Emot. Behav. Disord. 1999, 7, 11–20. [Google Scholar] [CrossRef]
- Díaz Atienza, J. Comorbilidad en el tdah. Rev. Psiquiatr. Psicol. Niño Adolesc. 2006, 6, 44–55. Available online: http://fundacioncadah.org/j289eghfd7511986_uploads/20120606_7mZG5IP3fsJy0YhrYekf_0.pdf (accessed on 5 November 2021).
- Deault, L.C. A Systematic Review of Parenting in Relation to the Development of Comorbidities and Functional Impairments in Children with Attention-Deficit/Hyperactivity Disorder (ADHD). Child Psychiatry Hum. Dev. 2010, 41, 168–192. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Presentations/Subtypes of ADHD | Behavioral Expression |
|---|---|
| Predominantly inattentive | Do not pay attention to the details of their tasks.
|
| Predominantlyhyperactive/impulsive | Hyperactivity |
| |
| Impulsive | |
| |
| Combined |
|
| Reference | Authors | Main Findings |
|---|---|---|
| 1 | APA | Report the diagnostic criteria for ADHD |
| 2 | National Institutes of Health Consensus Development Conference Statement | ADHD as a public health problem |
| 3 | Andersen, 2003 | 60% of the ADHD cases diagnosed in childhood can persist until adulthood |
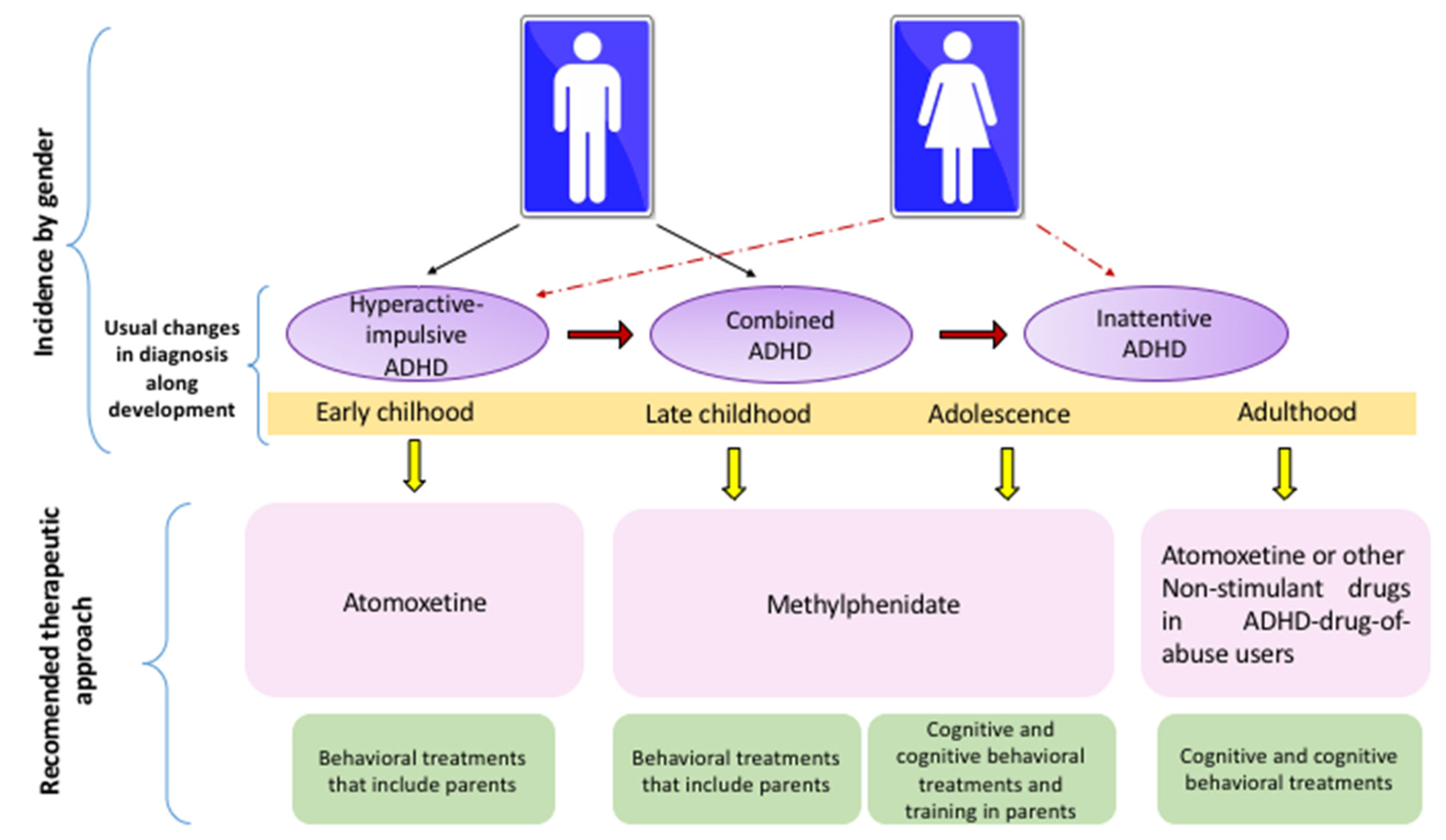
| 4 | Mowlem et al., 2018 | Percentage of diagnosis for each presentation in ADHD: inattention: 53.7%, combined type 26.8% and hyperactive/impulsive 19.5% |
| 5 | Willcutt et al., 2012 | The most diagnosed presentation |
| 6 | Greenhill et al., 2008 | The most diagnosed presentation |
| 7 | Young et al., 2013 | The inattention presentation of ADHD is the most common clinical feature for adults. |
| 8 | Lahey et al., 2005 | Dynamics in the diagnostic of each ADHD presentation throughout development. |
| 9 | Charach et al., 2011 | Diagnosis of ADHD by age |
| 10 | Chronis et al., 2006 | Importance of multimodal treatments for ADHD. |
| 11 | Hébert et al., 2013 | Clinical issues that affect the therapy adherence in ADHD patients. |
| 12 | Barbaresi et al., 2007 | Stimulant drugs improve reading, grade retention and school attendance |
| 13 | Caye et al., 2019 | The safety of ADHD treatments should be evaluated according to individualized patients’ features. |
| 14 | Minzenberg et al., 2012 | Subcellular mechanisms of pharmacological treatments in ADHD could be related to neural or cognition systems. |
| 15 | Cortese et al., 2020 | The efficacy of pharmacological treatments that have been approved by regulatory agencies. |
| 16 | Liu et al., 2017 | Methylphenidate shows higher response, decreases inattention and generates lower risk for adverse events as compared to Atomoxetine in children and adolescents |
| 17 | Stuhec et al., 2019 | Stimulant drugs with larger size effect for ADHD treatment in adults. |
| 18 | Storebø et al., 2019 | Parallel and crossover trials are suitable for analyzing the efficacy of methylphenidate in children and adolescents with ADHD. |
| 19 | Wilens et al., 2008 | Role of catecholaminergic systems in the improvement of core symptoms in ADHD. |
| 20 | Huang et al., 2011 | Long-term efficacy of pharmacological treatments in comparison to their adverse effects. |
| 21 | Mardomingo-Sanz et al., 2012 | Effectiveness of different formulations of methylphenidate. |
| 22 | Zetterström et al., 2019 | Methylphenidate efficacy depends on the duration of its administration and the brain region analyzed. |
| 23 | Pietrzak et al., 2006 | Intra- or inter-individual variability may affect the methylphenidate efficacy. |
| 24 | Zehle et al., 2007 | Indicates that methylphenidate could improve the core ADHD symptoms via increasing the synaptic organization. |
| 25 | Kodama et al., 2017 | Methylphenidate effects on the dopamine system are brain-region dependent. |
| 26 | Schulz et al., 2017 | Methylphenidate is better than atomoxetine for activating the caudate nucleus of young ADHD patients. |
| 27 | Nakanishi et al., 2017 | Effects of methylphenidate and atomoxetine in the prefrontal activity of children with ADHD. |
| 28 | Ozdemir, et al., 2010 | Risk of methylphenidate for developing suicide behavior. |
| 29 | Patel et al., 2017 | Effects of toxic doses of psychostimulants over psychotic symptoms. |
| 30 | Cheng et al., 2014 | Low doses of methylphenidate improve cognition by increasing excitatory postsynaptic currents (EPSCs), whereas high doses are related to psychosis because of EPSC blockage. |
| 31 | Huss et al., 2017 | Dose optimization of methylphenidate improves the efficacy of this treatment |
| 32 | Beyer, et al., 2014 | Methylphenidate as a cognitive enhancer in healthy people. |
| 33 | Kortekaas-Rijlaarsdam et al., 2017 | The efficacy of methylphenidate on academic performance could be limited to math abilities. |
| 34 | Masi et al., 2017 | Effectiveness of methylphenidate in aggressive behavior in ADHD plus ODD or Aggression. |
| 35 | Golubchik et al.,2019 | Effectiveness of methylphenidate againts impulsive behavior in ADHD and ADHD plus ODD patients |
| 36 | Reynaud et al., 2019 | Atomoxetine injections improves attentional orientation. |
| 37 | Clemow et al., 2016 | Optimal doses of atomoxetine by age. |
| 38 | Rezaei et al., 2016 | In children and adolescents, atomoxetine has similar size effect to methylphenidate with immediate-release vehicle, but not with the osmotic vehicles. |
| 39 | Verplaetse et al., 2019 | Guanfacine as adjuvant therapy for ADHD in children and adolescents. |
| 40 | Iwanami et al., 2020 | Guanfacine for the treatment of ADHD in adults. |
| 41 | Okazaki et al., 2019 | Guanfacine is effective and well tolerated when compared to atomoxetine and methylphenidate. |
| 42 | Okada et al., 2019 | Guanfacine reduces impulsivity. |
| 43 | Fitzpatrick et al., 2019 | Guanfacine improves cognitive performance in ADHD. |
| 44 | Cortese et al., 2018 | Atomoxetine is less effective for ADHD symptoms in late childhood |
| 45 | Bastiaens et al., 2019 | Methylphenidate is not recommended for ADHD patients with drug addictions. |
| 46 | Pievsky et al., 2018 | ADHD patients present worse neurocognitive performance as compared to neurotypical subjects. |
| 47 | Mohammadi et al., 2014 | Decision-making problems in ADHD patients. |
| 48 | Barkley et al., 1997 | A theoretical model which suggests that ADHD should be associated with deficits in inhibition, working memory, self-regulation and internalization of speech. |
| 49 | Castellanos et al., 2002 | Executive problems in ADHD patients. |
| 50 | Diamond et al., 2005 | Working memory is the main difficulty in the inattentive type of ADHD. |
| 51 | Biederman et al., 1991 | ADHD in children should be categorized by comorbidity. |
| 52 | Daley et al., 2010 | The core symptoms of ADHD and not the comorbid symptoms, underlaying poor academic performance. |
| 53 | Shuai et al., 2017 | Training in executive functions improve daily activities in children with ADHD. |
| 54 | Bahcivan et al., 2015 | Patients with inattentive-ADHD require executive skills training. |
| 55 | Cortese et al., 2015 | Cognitive training improves working memory performance on children/adolescents with ADHD. |
| 56 | Chan et al., 2016 | Pharmacological treatments improve the core symptoms whereas psychosocial treatments enhance academic and organizational skills in adolescents with ADHD. |
| 57 | Fabiano et al., 2015 | Methodological issues found in some reports that analyze the efficacy of psychosocial treatments |
| 58 | Bikic et al., 2017 | Organizational skill training improves the symptoms of ADHD In children, |
| 59 | Serrano-Troncoso et al., 2013 | Psychosocial strategies show efficacy for ADHD clinical management. |
| 60 | Sibley et al., 2014 | In adolescents with ADHD, behavioral therapy showed similar improvements to pharmacological approaches. |
| 61 | Burke et al., 2002 | Types of psychosocial treatments. |
| 62 | Connor et al., 2002 | Types of psychosocial treatments |
| 63 | Pelham, et al., 2008 | Types of psychosocial treatments |
| 64 | Evans et al., 2014 | Cognitive interventions show moderate size effect in children and adolescents. |
| 65 | Nakashima et al., 2021 | Cognitive interventions during adulthood improve the clinical presentation of ADHD. |
| 66 | Vidal et al., 2015 | Inattention symptoms improve with therapy in groups. |
| 67 | Faraone et al., 1998 | Anxiety and depression are the most common comorbid problems with ADHD. |
| 68 | Mayes et al., 2009 | Anxiety and depression are the most common comorbid problems with ADHD. |
| 69 | Milich et al., 2001 | Anxiety and depression are the most common comorbid problems with ADHD. |
| 70 | Power et al., 2004 | Anxiety and depression are the most common comorbid problems in children with ADHD. |
| 71 | Presentación & Siegenthaler, 2005 | Anxiety and depression are comorbid with ADHD throughout development. |
| 72 | Van Den Hoofdakker et al., 2007 | Behavioral training for parents improves the symptoms of anxiety and depression in ADHD. |
| 73 | Vidal Estrada et al., 2012 | Cognitive- behavioral training improves self-esteem in ADHD patients. |
| 74 | Fullen et al., 2020 | Acceptance and commitment therapy is an emerging treatment that reduces anxiety in adults with ADHD. |
| 75 | Gadow et al., 2004 | Oppositional-defiant disorder is comorbid with ADHD |
| 76 | Nolan et al., 1999 | Oppositional-defiant disorder are comorbid with ADHD |
| 77 | Díaz Atienza, 2006 | Oppositional-defiant disorder is characterized by the exteriorization of disruptive behaviors and behavioral alterations. |
| 78 | Deault, 2010 | Oppositional-defiant disorder generates social dysfunction. |
| Drug | Clinical Efficacy | Developmental Stage |
|---|---|---|
| MPH | Inattention, impulsivity and hyperactivity. | Children and adolescents |
| MPH | Math skills | Children and adolescents |
| MPH | Motivation | Children and adolescents |
| MPH (Osmotic release) | Verbal fluency, selective attention, inhibitory control, spatial intelligence and working memory | Children and adolescents |
| MPH (long-lasting release) | Academic performance | Children |
| MPH | Control incidence and severity of ODD assaults | Young |
| ATM | Hyperactive/impulsive | Preschool child |
| Guanfacine | Cognitive performance, attention deficit, hyperactivity and working memory | Children, adolescents and adults |
| Cognitive Training | Efficacy on Symptoms | Developmental Stage |
|---|---|---|
| Executive training | Executive skills and improve routines in real daily life | Children |
| Cognitive training | Improve deficits in visual and verbal working memory | Children |
| Psychosocial Managements | Externalizing Symptoms | Internalizing Symptoms | Inattention | Impulsivity | Hyperactivity | Development Stage |
|---|---|---|---|---|---|---|
| Behavioral therapy | − | + | − | − | − | Children |
| Behavioral parenting training | − | + | + | + | + | Children and adolescents |
| Cognitive interventions | − | − | + | − | − | Children, adolescents and adults |
| Cognitive/behavioral therapy | − | + | − | − | − | Adults |
| Cognitive therapy for groups | − | − | + | − | − | Adults |
| Organization training | − | − | + | − | − | Children and adolescents |
| Stage of Development | ADHD Innatentive | ADHD Combined |
|---|---|---|
| Childhood and adolescence | Behavioral training for parents. | Behavioral training for parents. |
| Training in organization of school supplies. | Training in organization of school supplies. | |
| Cognitive intervention. | Cognitive intervention. | |
| Behavioral management in classroom. | Behavioral management in classroom. | |
| Peer behavioral intervention. | Peer behavioral intervention. | |
| Organizational skills training. | Organizational skills training. | |
| Combination of behavioral treatments for parents and teachers. | Combination of behavioral treatments for parents and teachers. | |
| Strategies for contingency management and academic interventions. | ||
| Adulthood | Cognitive behavioral therapy. | Cognitive behavioral therapy. |
| Cognitive training. | Cognitive training. | |
| Metacognitive therapy. | Metacognitive therapy. | |
| Cognitive behavioral therapy. | Cognitive behavioral therapy. | |
| Cognitive rehabilitation. | Cognitive rehabilitation. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galvez-Contreras, A.Y.; Vargas-de la Cruz, I.; Beltran-Navarro, B.; Gonzalez-Castaneda, R.E.; Gonzalez-Perez, O. Therapeutic Approaches for ADHD by Developmental Stage and Clinical Presentation. Int. J. Environ. Res. Public Health 2022, 19, 12880. https://doi.org/10.3390/ijerph191912880
Galvez-Contreras AY, Vargas-de la Cruz I, Beltran-Navarro B, Gonzalez-Castaneda RE, Gonzalez-Perez O. Therapeutic Approaches for ADHD by Developmental Stage and Clinical Presentation. International Journal of Environmental Research and Public Health. 2022; 19(19):12880. https://doi.org/10.3390/ijerph191912880
Chicago/Turabian StyleGalvez-Contreras, Alma Y., Ivette Vargas-de la Cruz, Beatriz Beltran-Navarro, Rocio E. Gonzalez-Castaneda, and Oscar Gonzalez-Perez. 2022. "Therapeutic Approaches for ADHD by Developmental Stage and Clinical Presentation" International Journal of Environmental Research and Public Health 19, no. 19: 12880. https://doi.org/10.3390/ijerph191912880
APA StyleGalvez-Contreras, A. Y., Vargas-de la Cruz, I., Beltran-Navarro, B., Gonzalez-Castaneda, R. E., & Gonzalez-Perez, O. (2022). Therapeutic Approaches for ADHD by Developmental Stage and Clinical Presentation. International Journal of Environmental Research and Public Health, 19(19), 12880. https://doi.org/10.3390/ijerph191912880