
Predicting the Clean Movement Technique in Crossfit® Athletes Using an Optimal Upper-Limb Range of Motion: A Prospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Procedure Study
2.3.1. Age, Anthropometric and CrossFit® Training Data
2.3.2. Upper-Limb ROM Profile Assessment
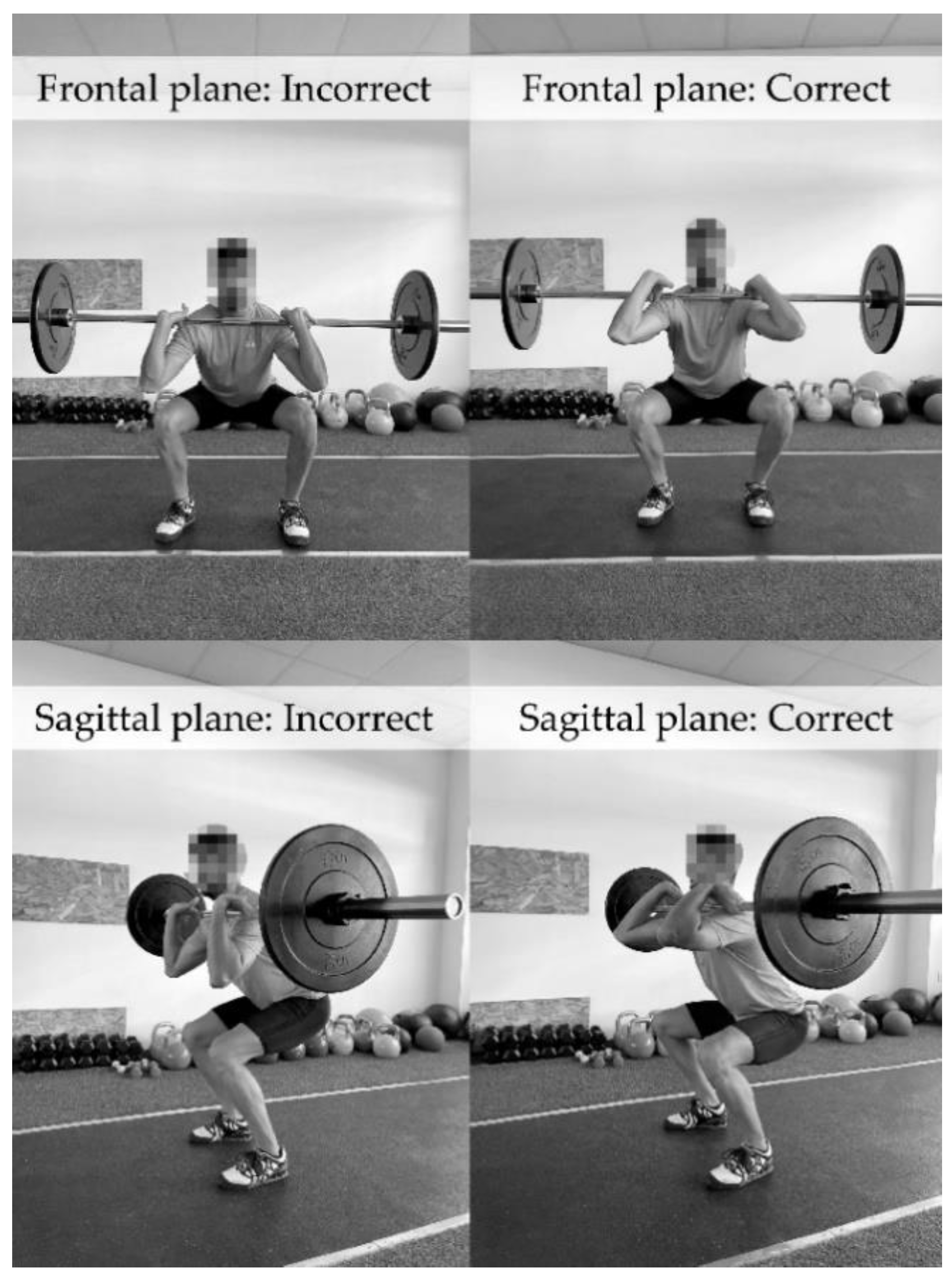
2.3.3. Clean Movement Technique Assessment
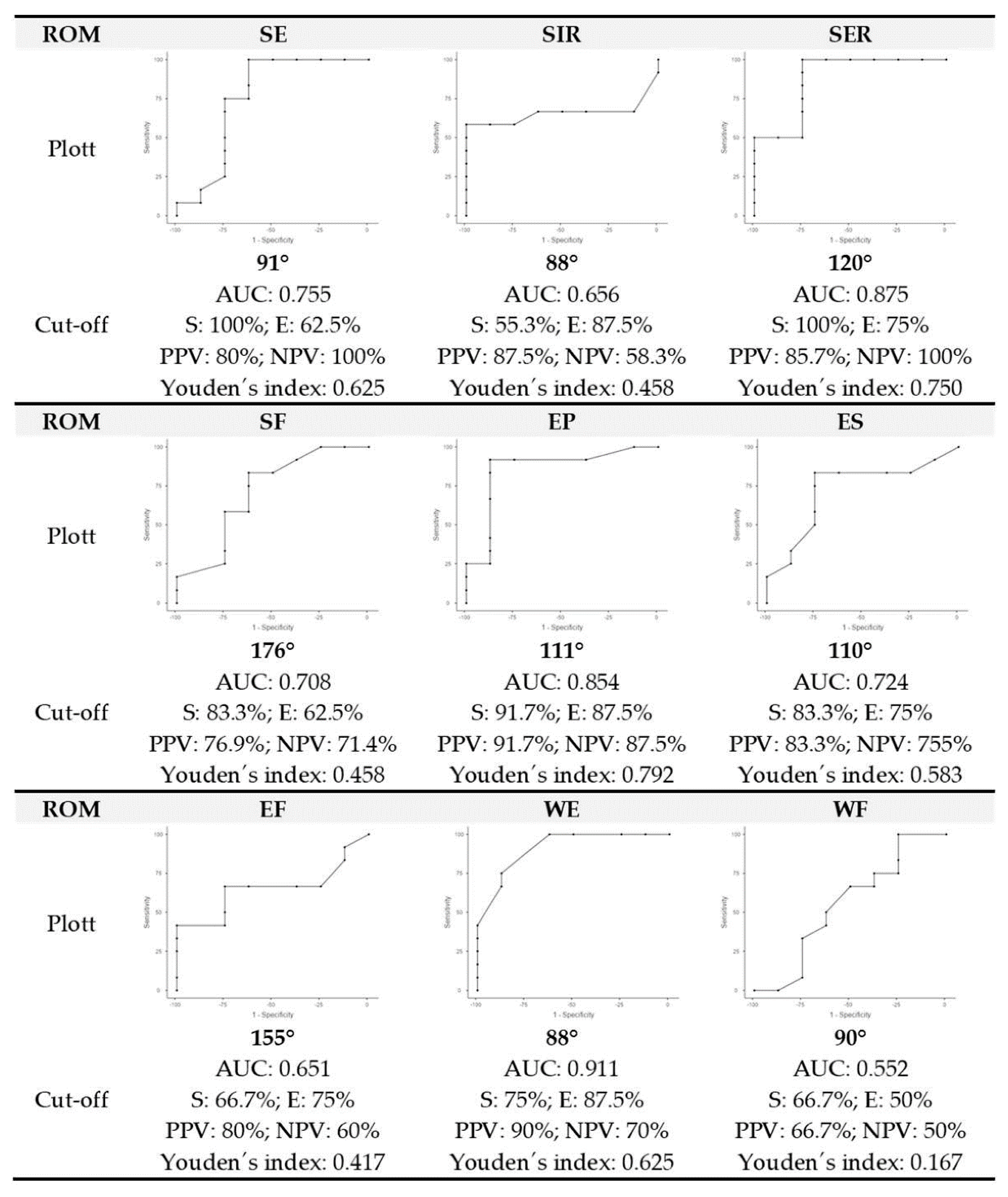
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CrossFit, L. About Affiliation. Available online: https://www.crossfit.com/gyms (accessed on 9 August 2022).
- CrossFit, L. What Is CrossFit? Available online: https://www.crossfit.com/what-is-crossfit (accessed on 26 September 2022).
- Hech Dominski, F.; Cristina Siqueira, T.; Teixeira Serafim, T.; Andrade, A. Injury profile in CrossFit practitioners: Systematic review. Fisioter. Pesqui. 2018, 25, 229–239. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, M.; García-Calleja, P.; Terrados, N.; Crespo, I.; Del Valle, M.; Olmedillas, H. Injury in CrossFit®: A Systematic Review of Epidemiology and Risk Factors. Physician Sportsmed. 2022, 50, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Burrows, E.; Tabb, L. A 4-year analysis of the incidence of injuries among CrossFit-trained participants. Orthop. J. Sports Med. 2018, 6, 2325967118803100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montalvo, A.; Shaefer, H.; Rodriguez, B.; Li, T.; Epnere, K.; Myer, G. Retrospective injury epidemiology and risk factors for injury in CrossFit. J. Sports Sci. Med. 2017, 16, 53–59. [Google Scholar]
- Summitt, R.; Cotton, R.; Kays, A.; Slaven, E. Shoulder injuries in individuals who participate in CrossFit training. Sports Health 2016, 8, 541–546. [Google Scholar] [CrossRef] [Green Version]
- Weisenthal, B.; Beck, C.; Maloney, M.; DeHaven, K.; Giordano, B. Injury rate and patterns among CrossFit athletes. Orthop. J. Sports Med. 2014, 2, 2325967114531177. [Google Scholar] [CrossRef]
- Hak, P.; Hodzovic, E.; Hickey, B. The nature and prevalence of injury during CrossFit training. J. Strength Cond. Res. 2013, 22, 1–13. [Google Scholar] [CrossRef]
- Tafuri, S.; Salatino, G.; Napoletano, P.; Monno, A.; Notarnicola, A. The risk of injuries among CrossFit athletes: An Italian observational retrospective survey. J. Sports Med. Phys. Fit. 2018, 59, 1544–1550. [Google Scholar] [CrossRef]
- Suchomel, T.; Comfort, P.; Stone, M. Weightlifting Pulling Derivatives: Rationale for Implementation and Application. Sports Med. 2015, 45, 823–839. [Google Scholar] [CrossRef]
- Suchomel, T.; Comfort, P.; Lake, J. Enhancing the force-velocity profile of athletes using weightlifting derivatives. Strength Cond. J. 2017, 39, 10–20. [Google Scholar] [CrossRef]
- Comfort, P.; Williams, R.; Suchomel, T. A comparison of catch phase force-time characteristics during clean derivatives from the knee. J. Strength Cond. Res. 2017, 31, 1911–1918. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.; Pierce, K.; Sands, W.; Stone, M. Weightlifting: A brief overview. Strength Cond. J. 2006, 28, 50–66. [Google Scholar] [CrossRef]
- Fry, A.; Ciroslan, D.; Fry, M.; LeRoux, C.; Schilling, B.; Chiu, L. Anthropometric and performance variables discriminating elite American junior men weightlifters. J. Strength Cond. Res. 2006, 20, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Aasa, U.; Svartholm, I.; Andersson, F.; Berglund, L. Injuries among weightlifters and powerlifters: A systematic review. Br. J. Sports Med. 2017, 51, 211–219. [Google Scholar] [CrossRef] [Green Version]
- Strömbäck, E.; Aasa, U.; Gilenstam, K.; Berglund, L. Prevalence and consequences of injuries in powerlifting: A cross-sectional study. Orthop. J. Sports Med. 2018, 6, 2325967118771016. [Google Scholar] [CrossRef] [Green Version]
- Keogh, J.; Winwood, P. The Epidemiology of Injuries Across the Weight-Training Sports. Sports Med. 2017, 47, 479–501. [Google Scholar] [CrossRef] [Green Version]
- Sprey, J.; Ferreira, T.; De Lima, M.; Duarte, A.; Jorge, P.; Santili, C. An epidemiological profile of CrossFit athletes in Brazil. Orthop. J. Sports Med. 2016, 4, 2325967116663706. [Google Scholar] [CrossRef] [Green Version]
- Bousquet, B.; Olson, T. Starting at the Ground Up: Range of Motion Requirements and Assessment Procedures for Weightlifting Movements. Strength Cond. J. 2018, 40, 56–67. [Google Scholar] [CrossRef]
- Claudino, J.; Gabbett, T.; Bourgeois, F.; Souza, H.; Miranda, R.; Mezêncio, B.; Soncin, R.; Cardoso Filho, C.; Bottaro, M.; Hernandez, A.; et al. CrossFit Overview: Systematic Review and Meta-analysis. Sports Med.-Open-Open 2018, 4, 1–14. [Google Scholar] [CrossRef]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.; Chamari, K. International Olympic Committee consensus statement: Methods for Recording and Reporting of Epidemiological Data on Injury and Illness in Sports 2020 (Including the STROBE Extension for Sports Injury and Illness Surveillance (STROBE-SIIS)). Orthop. J. Sports Med. 2020, 8, 372–389. [Google Scholar] [CrossRef] [Green Version]
- Cejudo, A.; Sánchez-Castillo, S.; Sainz de Baranda, P.; Gámez, J.; Santonja-Medina, F. Low Range of Shoulders Horizontal Abduction Predisposes for Shoulder Pain in Competitive Young Swimmers. Front. Psychol. 2019, 10, 478. [Google Scholar] [CrossRef] [PubMed]
- Cejudo, A. Description of ROM-SPORT I Battery: Keys to Assess Lower Limb Flexibility. Int. J. Environ. Res. Public Health 2022, 19, 10747. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, J.; Cocchiarella, L.; Lea, R. The Practical Guide to Range of Motion Assessment; American Medical Association: Chicago, IL, USA, 2002. [Google Scholar]
- Cejudo, A.; Abril-Guiote, J.E.; Igualada-Fernández, A.; Sainz de Baranda, P. Valoración del riesgo de dolor de hombro en trabajadores de limpieza viaria y recogida de residuos. Proyecto PRE-REFILAB. JUMP 2021, 3, 17–27. [Google Scholar] [CrossRef]
- Kilduff, L.; Bevan, H.; Owen, N.; Kingsley, M.; Bunce, P.; Bennett, M.; Cunningham, D. Optimal Loading for Peak Power Output During the Hang Power Clean in Professional Rugby Players. Int. J. Sports Physiol. Perform. 2007, 2, 260–269. [Google Scholar] [CrossRef] [Green Version]
- Cormie, P.; McCaulley, G.; Triplett, N.; McBride, J. Optimal loading for maximal power output during lower-body resistance exercises. Med. Sci. Sports Exerc. 2007, 39, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.; Comfort, P. Advanced Strength and Conditioning: An Evidence-Based Approach, 2nd ed.; Routledge: London, UK, 2022. [Google Scholar]
- Storey, A.; Smith, H. Unique Aspects of Competitive Weightlifting. Sports Med. 2012, 42, 769–790. [Google Scholar] [CrossRef] [PubMed]
- Doncaster, G.; Page, R.; White, P.; Svenson, R.; Twist, C. Analysis of Physical Demands During Youth Soccer Match-Play: Considerations of Sampling Method and Epoch Length. Res. Q. Exerc. Sport 2020, 91, 326–334. [Google Scholar] [CrossRef]
- Linke, D.; Link, D.; Weber, H.; Lames, M. Decline in match running performance in football is affected by an increase in game interruptions. J. Sports Sci. Med. 2018, 17, 662–667. [Google Scholar]
- Lee, M.; Wagenmakers, E. Bayesian Data Analysis for Cognitive Science: A Practical Course; Cambridge University Press: New York, NY, USA, 2013. [Google Scholar]
- Batterham, A.; Hopkins, W. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Thiele, C. Cutpointr: Determine and Evaluate Optimal Cutpoints in Binary Classification Tasks [R Package]. Available online: https://cran.r-project.org/package=cutpointr (accessed on 5 January 2022).
- Hosmer, D.; Lemeshow, S.; Sturdivant, R. Applied Logistic Regression; John Wiley & Sons: New York, NY, USA, 2013. [Google Scholar]
- Youden, W. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Takano, B. Coaching optimal technique in the snatch and the clean and jerk. NSCA J. 1987, 9, 52–56. [Google Scholar]
- CrossFit, L. CrossFit Certificate Courses. Available online: https://www.crossfit.com/certificate-courses (accessed on 18 August 2022).
- Spence, A.; Helms, E.; McGuigan, M. Range of Motion Is Not Reduced in National-Level New Zealand Female Powerlifters. J. Strength Cond. Res. 2021, 35, 2737–2741. [Google Scholar] [CrossRef] [PubMed]
- Garhammer, J. Biomechanical Profiles of Olympic Weightlifters. Int. J. Sport Biomech. 1985, 1, 122–130. [Google Scholar] [CrossRef]
- Winwood, P.; Cronin, J.; Brown, S. A biomechanical analysis of the heavy sprint-style sled pull and comparison with the back squat. J. Sports Sci. Coach. 2015, 10, 869–886. [Google Scholar] [CrossRef] [Green Version]
- Hindle, B.; Lorimer, A.; Winwood, P.; Keogh, J. The Biomechanics and Applications of Strongman Exercises: A Systematic Review. Sports Med.-Open 2019, 5, 49. [Google Scholar] [CrossRef]
- Bloomquist, K.; Langberg, H.; Karlsen, S.; Madsgaard, S.; Boesen, M.; Raastad, T. Effect of range of motion in heavy load squatting on muscle and tendon adaptations. Eur. J. Appl. Physiol. 2013, 113, 2133–2142. [Google Scholar] [CrossRef]
- Silva, J.; Gomes, W.; Pecoraro, S.; Soares, E.; Magalhães, R.; Fioravanti, G.; Baladán, R.; Lopes, C.; Marchetti, P. The range of motion of the back squat exercise affects absolute volume load without changing the rating of perceived exertion. Rev. Bras. Cineantropometria Desempenho Hum. 2020, 22, e58196. [Google Scholar] [CrossRef]
- da Costa, T.; Louzada, C.; Miyashita, G.; da Silva, P.; Sungaila, H.; Lara, P.; de Castro, A.; Ejnisman, B.; Cohen, M.; Arliani, G. CrossFit s: Injury prevalence and main risk factors. Clinics 2019, 74, e1402. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Wu, M.; Huang, C.; Wu, J.; Guo, L.; Wu, W. The analysis of upper limb movement and EMG activation during the snatch under various loading conditions. J. Mech. Med. Biol. 2013, 13, 1350010. [Google Scholar] [CrossRef]
- Ammar, A.; Riemann, B.; Masmoudi, L.; Blaumann, M.; Abdelkarim, O.; Hökelmann, A. Kinetic and kinematic patterns during high intensity clean movement: Searching for optimal load. J. Sports Sci. 2018, 36, 1319–1330. [Google Scholar] [CrossRef]
- Khaled, E.; Ibrahim, A. The effect of development of muscular balance on some dynamic parameters and level of achievement for clean and jerk skill for weightlifters. Ovidius Univ. Ann. Ser. Phys. Educ. Sport/Sci. Mov. HealthScience Mov. Health 2013, 13, 172–182. [Google Scholar]
- Wilk, K.; Macrina, L.; Fleisig, G.; Aune, K.; Porterfield, R.; Harker, P.; Evans, T.; Andrews, J. Deficits in glenohumeral passive range of motion increase risk of shoulder injury in professional baseball pitchers: A prospective study. Am. J. Sports Med. 2015, 43, 2379–2385. [Google Scholar] [CrossRef] [PubMed]
- Shanley, E.; Rauh, M.; Michener, L.; Ellenbecker, T.; Garrison, J.; Thigpen, C. Shoulder range of motion measures as risk factors for shoulder and elbow injuries in high school softball and baseball players. Am. J. Sports Med. 2011, 39, 1997–2006. [Google Scholar] [CrossRef]
- Kendall, F.; McCreary, E.; Provance, P.; Rodgers, M.; Romani, W. Muscles: Testing and Function with Posture and Pain; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2005; ISBN 0781747805. [Google Scholar]
- Lewis, J.; Green, A.; Wright, C. Subacromial impingement syndrome: The role of posture and muscle imbalance. J. Shoulder Elb. Surg. 2005, 14, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Codine, P.; Bernard, P.; Benaim, C.; Brun, V. Influence of sports discipline on shoulder rotator cuff balance. Med. Sci. Sports Excercices 1997, 29, 1400–1405. [Google Scholar] [CrossRef]
- Kolber, M.; Beekhuizen, K.; Cheng, M.; Hellman, M. Shoulder joint and muscle characteristics in the recreational weight training population. J. Strength Cond. Res. 2009, 23, 148–157. [Google Scholar] [CrossRef]
- Lavallee, M.; Balam, T. An overview of strength training injuries: Acute and chronic. Curr. Sports Med. Rep. 2010, 9, 307–313. [Google Scholar] [CrossRef]
- Morton, S.; Whitehead, J.; Brinkert, R. Resistance training vs. static stretching: Effects on flexibility and strength. J. Strength Cond. Res. 2011, 25, 3391–3398. [Google Scholar] [CrossRef] [Green Version]
- Fees, M.; Decker, T.; Snyder-Mackler, L.; Axe, M. Upper extremity weight-training modifications for the injured athlete: A clinical perspective. Am. J. Sports Med. 1998, 26, 732–742. [Google Scholar] [CrossRef]
- Kolber, M.; Corrao, M.; Hanney, W. Characteristics of anterior shoulder instability and hyperlaxity in the weight-training population. J. Strength Cond. Res. 2013, 27, 1333–1339. [Google Scholar] [CrossRef]
- Ayala, F.; Sainz De Baranda, P. Calidad metodológica de los programas de estiramiento: Revisión sistemática. Int. J. Med. Sci. Phys. Act. Sport 2013, 13, 163–181. [Google Scholar]
- Mohr, A.; Long, B.; Goad, C. Effect of foam rolling and static stretching on passive hip-flexion range of motion. J. Sport Rehabil. 2014, 23, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Decicco, P.; Fisher, M. The effects of proprioceptive neuromuscular facilitation stretching on shoulder range of motion in overhand athletes. J. Sports Med. Phys. Fit. 2005, 45, 183–187. [Google Scholar]
- Wiewelhove, T.; Döweling, A.; Schneider, C.; Hottenrott, L.; Meyer, T.; Kellmann, M.; Pfeiffer, M.; Ferrauti, A. A meta-analysis of the effects of foam rolling on performance and recovery. Front. Physiol. 2019, 10, 376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, D.; Buschbacher, L.; Edlich, R. Limited joint mobility in power lifters. Am. J. Sports Med. 1988, 16, 280–284. [Google Scholar] [CrossRef]
- Gadomski, S.; Ratamess, N. Range of Motion Adaptations in Powerlifters. J. Strength Cond. Res. 2018, 32, 3020–3028. [Google Scholar] [CrossRef]
- Barlow, J.; Benjamin, B.; Birt, P.; Hughes, C.; Barlow, J.; Benjamin, B.; Birt, P.; Hughes, C. Shoulder strength and range-of-motion characteristics in bodybuilders. J. Strength Cond. Res. 2002, 16, 367–372. [Google Scholar] [CrossRef]
- Beedle, B.; Jessee, C.; Stone, M. Flexibility characteristics among athletes who weight train. J. Appl. Sport Sci. Res. 1991, 5, 150–154. [Google Scholar]
- Cejudo, A.; Moreno-Alcaraz, V.; Izzo, R.; Robles-Palazón, F.J.; Sainz de Baranda, P.; Santonja-Medina, F. Flexibility in Spanish Elite Inline Hockey Players: Profile, Sex, Tightness and Asymmetry. Int. J. Environ. Res. Public Health 2020, 17, 3295. [Google Scholar] [CrossRef]
- International Powerlifting Federation Technical Rules. Available online: https://www.powerlifting.sport/fileadmin/ipf/data/rules/technical-rules/english/IPF_Technical_Rules_Book_2022_1.pdf (accessed on 19 August 2022).
- Kouyoumdjian, P.; Coulomb, R.; Sanchez, T.; Asencio, G. Clinical evaluation of hip joint rotation range of motion in adults. Orthop. Traumatol. Surg. Res. 2012, 98, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Battista, R.; Pivarnik, J.; Dummer, G.; Sauer, N.; Malina, R. Comparisons of physical characteristics and performances among female collegiate rowers. J. Sports Sci. 2007, 25, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Kapandji, A. The Physiology of the Joints: The Upper Limb, 7th ed.; Handspring Publishing: London, UK, 2019; ISBN 1912085593. [Google Scholar]
- O’Sullivan, K.; McAuliffe, S.; DeBurca, N. The effects of eccentric training on lower limb flexibility: A systematic review. Br. J. Sports Med. 2012, 46, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Choi, S. Cellular mechanism of eccentric-induced muscle injury and its relationship with sarcomere heterogeneity. J. Exerc. Rehabil. 2014, 10, 200–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fridén, J.; Lieber, R. Eccentric exercise-induced injuries to contractile and cytoskeletal muscle fibre components. In Proceedings of the Acta Physiologica Scandinavica; John Wiley & Sons Ltd.: Copenhagen, Denmark, 2001; Volume 171, pp. 321–326. [Google Scholar]
- Ying, J.; Cen, X.; Yu, P. Effects of Eccentric Exercise on Skeletal Muscle Injury: From An Ultrastructure Aspect: A Review. Phys. Act. Health 2021, 5, 15–20. [Google Scholar] [CrossRef]
- Mangine, G.; Tankersley, J.; Mcdougle, J.; Velazquez, N.; Roberts, M.; Esmat, T.; Vandusseldorp, T.; Feito, Y. Predictors of CrossFit open performance. Sports 2020, 8, 102. [Google Scholar] [CrossRef]
- Martínez-Gómez, R.; Valenzuela, P.; Alejo, L.; Gil-Cabrera, J.; Montalvo-Pérez, A.; Talavera, E.; Lucia, A.; Moral-González, S.; Barranco-Gil, D. Physiological Predictors of Competition Performance in CrossFit Athletes. Int. J. Environ. Res. Public Health 2020, 17, 3699. [Google Scholar] [CrossRef]
- Toledo, R.; Dias, M.; Toledo, R.; Erotides, R.; Pinto, D.; Reis, V.; Novaes, J.; Vianna, J.; Heinrich, K.; Schmidt, A.; et al. Comparison of Physiological Responses and Training Load between Different CrossFit® Workouts with Equalized Volume in Men and Women. Life 2021, 11, 586. [Google Scholar] [CrossRef]
- Keogh, J.; Hume, P.; Pearson, S. Retrospective injury epidemiology of one hundred one competitive Oceania power lifters: The effects of age, body mass, competitive standard, and gender. J. Strength Cond. Res. 2006, 20, 672–681. [Google Scholar] [CrossRef]
- Sugimoto, D.; Zwicker, R.; Quinn, B. Part II: Comparison of CrossFit-related injury presenting to sports medicine clinic by sex and age. Clin. J. Sport Med. 2020, 30, 251–256. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Male (n = 12) | Female (n = 8) | Bayesian Factor | δ (95% Credible Interval) | Evidence | Total (n = 20) |
|---|---|---|---|---|---|---|
| Age (y) | 32.67 ± 3.31 | 27.25 ± 2.71 | 25.59 | 1.45 (0.39, 2.57) | Strong B10 | 30.50 ± 4.06 |
| Body mass (kg) | 80.42 ± 12.07 | 60.00 ± 4.93 | 84.65 | 1.77 (0.62, 2.95) | Very strong B10 | 72.25 ± 14.09 |
| Body height (cm) | 175.50 ± 9.45 | 165.38 ± 3.85 | 4.98 | 1.01 (0.09, 2.04) | Moderate B10 | 171.45 ± 9.12 |
| Body mass index (kg/m2) | 26.06 ± 2.98 | 21.91 ± 1.22 | 20.55 | 1.39 (0.35, 2.51) | Strong B10 | 24.40 ± 3.17 |
| Training experience (y) | 2.92 ± 1.83 | 3.13 ± 1.89 | 2.44 | −0.06 (−0.82, 0.67) | Anecdotal B01 | 3.00 ± 1.81 |
| Months training per year (mth) * | 11.67 ± 0.49 | 11.50 ± 0.53 | 2.07 | 0.21 (−0.51, 1.01) | Anecdotal B01 | 11.60 ± 0.50 |
| Training frequency per week (day) * | 3.33 ± 1.30 | 3.50 ± 1.20 | 2.37 | −0.11 (−0.87, 0.62) | Anecdotal B01 | 3.40 ± 1.23 |
| Training session duration (min) * | 70.00 ± 14.77 | 71.88 ± 15.10 | 2.40 | −0.09 (−0.85, 0.64) | Anecdotal B01 | 72.35 ± 14.53 |
| Shoulder extension (degree) | 84.08 ± 8.67 | 88.88 ± 12.51 | 1.73 | −0.31 (−1.14, 0.42) | Anecdotal B01 | 86.00 ± 10.34 |
| Shoulder internal rotation (degree) | 91.92 ± 9.02 | 87.38 ± 9.12 | 1.63 | 0.33 (−0.39, 1.18) | Anecdotal B01 | 90.10 ± 9.11 |
| Shoulder external rotation (degree) | 111.67 ± 9.77 | 124.63 ± 11.92 | 3.73 | 0.92 (−1.94, −0.04) | Moderate B10 | 116.85 ± 12.25 |
| Shoulder flexion (degree) | 173.08 ± 3.63 | 176.88 ± 4.36 | 1.73 | −0.698 (−1.66, 0.11) | Anecdotal B10 | 174.60 ± 4.27 |
| Elbow pronation (degree) * | 104.25 ± 7.39 | 113.25 ± 2.43 | 8.64 | −1.16 (−2.23, −0.19) | Moderate B10 | 107.85 ± 7.36 |
| Elbow supination (degree) | 107.58 ± 5.05 | 109.00 ± 5.40 | 2.19 | −0.18 (−0.97, 0.54) | Anecdotal B01 | 108.15 ± 5.10 |
| Elbow flexion (degree) | 155.25 ± 8.29 | 155.75 ± 6.92 | 2.46 | −0.041 (−0.79, 0.69) | Anecdotal B01 | 155.45 ± 7.58 |
| Wrist extension, elbow at 0° (degree) * | 84.33 ± 7.56 | 91.38 ± 5.73 | 2.03 | −0.75 (−1.71, 0.08) | Anecdotal B10 | 87.15 ± 7.60 |
| Wrist flexion, elbow at 0° (degree) | 90.92 ± 4.85 | 93.00 ± 6.63 | 2.00 | −0.23 (−1.04, 0.49) | Anecdotal B01 | 91.75 ± 5.56 |
| Variables | Incorrect CPCM (n = 12) | Correct CPCM (n = 8) | Bayesian Factor | δ (95% Credible Interval) | Evidence |
|---|---|---|---|---|---|
| Age (y) | 31.83 ± 3.93 | 28.50 ± 3.59 | 1.37 | 0.62 (−1.16, 1.56) | Anecdotal B10 |
| Body mass (kg) | 78.17 ± 13.50 | 63.38 ± 10.14 | 3.56 | 0.91 (0.03, 1.92) | Moderate B10 |
| Height (cm) | 173.75 ± 9.39 | 168.00 ± 8.02 | 1.25 | 0.44 (−0.30, 1.32) | Anecdotal B01 |
| Body mass index (kg/m2) | 25.79 ± 3.21 | 22.31 ± 1.65 | 4.67 | 0.99 (0.08, 2.02) | Moderate B10 |
| Training experience (y) | 2.08 ± 1.44 | 4.38 ± 1.41 | 19.08 | −1.38 (−2.48, −0.34) | Strong B10 |
| Months training per year (mth) | 11.58 ± 0.51 | 11.63 ± 0.52 | 2.45 | −0.05 (−0.81, 0.68) | Anecdotal B01 |
| Training frequency (per week) | 2.75 ± 0.87 | 4.38 ± 1.06 | 12.74 | −1.27 (−2.35, −0.26) | Strong B10 |
| Training duration (min) * | 62.5 ± 8.66 | 83.13 ± 12.08 | 67.03 | −1.70 (−2.87, −0.57) | Very strong B10 |
| Shoulder extension (degree) | 81.83 ± 6.60 | 92.25 ± 12.14 | 2.89 | −0.85 (−1.85, 0.01) | Anecdotal B10 |
| Shoulder internal rotation (degree) | 88.50 ± 11.24 | 92.50 ± 3.96 | 1.80 | −0.29 (−1.12, 0.43) | Anecdotal B01 |
| Shoulder external rotation (degree) | 109.83 ± 7.03 | 127.38 ± 10.85 | 69.70 | −1.71 (−2.89, −0.58) | Very strong B10 |
| Shoulder flexion (degree) | 173.33 ± 3.45 | 176.50 ± 4.90 | 1.07 | −0.54 (−1.45, 0.22) | Anecdotal B10 |
| Elbow pronation (degree) * | 104.83 ± 7.46 | 112.38 ± 4.57 | 3.13 | −0.85 (−1.84, 0.01) | Moderate B10 |
| Elbow supination (degree) | 106.58 ± 5.00 | 110.50 ± 4.57 | 1.15 | −0.57 (−1.49, 0.21) | Anecdotal B10 |
| Elbow flexion (degree) | 153.67 ± 8.39 | 158.13 ± 5.64 | 1.37 | −0.40 (−1.27, 0.33) | Anecdotal B01 |
| Wrist extension, elbow at 0° (degree) * | 83.33 ± 6.77 | 92.88 ± 4.70 | 13.20 | −1.28 (−2.36, −0.27) | Strong B10 |
| Wrist flexion, elbow at 0° (degree) | 91.25 ± 5.05 | 92.50 ± 6.55 | 2.30 | −0.14 (−0.91, 0.59) | Anecdotal B01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cejudo, A. Predicting the Clean Movement Technique in Crossfit® Athletes Using an Optimal Upper-Limb Range of Motion: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 12985. https://doi.org/10.3390/ijerph191912985
Cejudo A. Predicting the Clean Movement Technique in Crossfit® Athletes Using an Optimal Upper-Limb Range of Motion: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12985. https://doi.org/10.3390/ijerph191912985
Chicago/Turabian StyleCejudo, Antonio. 2022. "Predicting the Clean Movement Technique in Crossfit® Athletes Using an Optimal Upper-Limb Range of Motion: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 19: 12985. https://doi.org/10.3390/ijerph191912985