
Refugees' Agency: On Resistance, Resilience, and Resources


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Data Collection
2.3.1. Topic List
2.3.2. Procedures
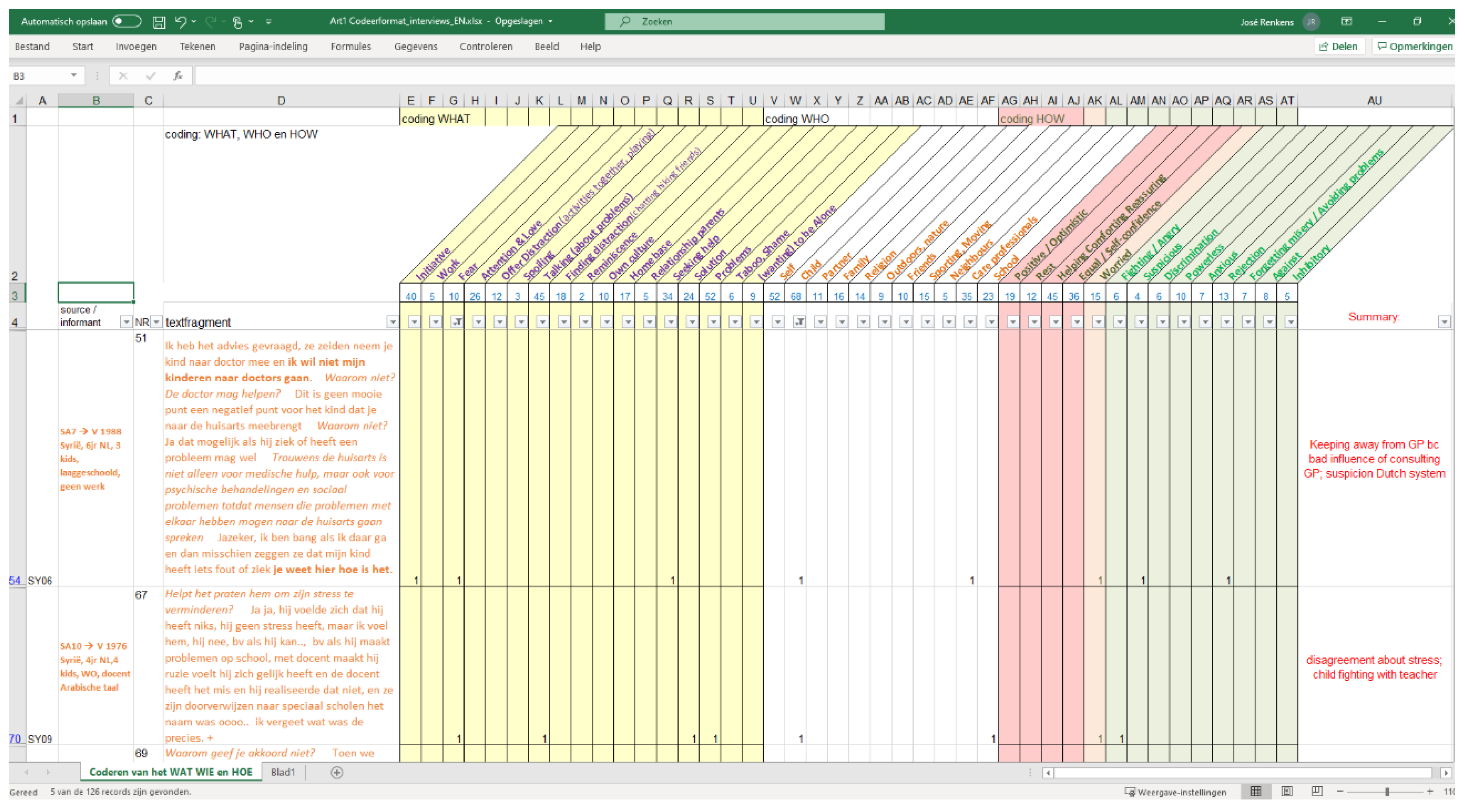
2.4. Data Analyses
2.5. Ethical Considerations
3. Findings
3.1. Characteristics of the Study Population
3.2. Decision-Making
3.2.1. Decision-Making: Finding and Offering Distraction
‘I like to walk between the trees.The most important thing indeed is to leave the house,the first 10 steps change my psyche completely.’[F58_SY07]
‘Yes, walking in the woods and breathing fresh air,that helps me to release stress and feel comfortable.’[F26_SY04]
‘.. when I am too busy at work, or there are many things about my homelandor something, then I go gaming, or sports, yes I do sports. Sports really help. (..).Then, I do not think about it, then I concentrate on other things, sport helps, (…)it makes me feel calm, and yes, happy, and with gaming too.’[F87+88_SY11]
‘We talk to them about interesting subjects,let them remember the most beautiful days in Syria,not the bad things that resulted from the war,like their visits to their grandparents. So, we let them focus on the positive sides.’[F28_SY02]
3.2.2. Decision-Making: Focus
‘My daughter’s best friend was in a different group. So, I talked to her,are you sad, or how do you feel when he goes to another group?’F91_IR01
‘When I pray, it is a mix of movement and recitation,I read some syllables from Quran while I make moves, it is somehow like Yoga. I believe in what I read. In Quran are so many sermons, wisdom and lessons which relieve your heart and soul.Then, you know deep in your heart that all the difficulties will also go away, God will be with you, help you, and the future will be better.’[F27_SA5]
Some people actively seek solitude:‘I will sit in my room alone for a while, when I feel discomfort I like to sit alone. I am sitting alone, with my discomfort.I log out from whatsapp, I turn off the phone…everything becomes irritating to my nerves.I then need to be alone with myself in my room.Then, I will read the Quran or pray, or do Tasspeeh [praise God]Then, yes, I feel better.’F70_SY09
‘They never asked our opinion; they find it normaland were surprised when I refused—‘on the contrary, it would be better for my child, would be good for his morals’ [they said].We are people who think this is shameful, my child cannot go to such a centre. It is shameful, not suitable for us.They may have different insights, they may be right, but we do not accept it.We have a different culture; the Arab culture exists inside us. We cannot integrate.’[F74_SY09]
‘Because the mentality is not very similar, unless the caregiveris a foreigner too—or they think that the person, despite being Dutch,sympathizes with the situation,only then they will allow it.’F104_AR01
‘but I do not want my children to see doctors.I am afraid that if I go there, maybe they saythere’s something wrong with my child, or he’s sick.You know how it is here.’F51_SY06
3.3. Leadership and Collective Action
‘Actually, I have founded an organisation,that can take care of mental health problems in refugee childrenabout which the parents need more education.I need professionals to give courses about these issues to refugees.Through my organization I can provide the public with more educationand support for refugees parents.’F31_SY04
‘We are an organisation that can give this informationbut it needs to reach the public of refugees, there is a missing link in the circle between [refugees and professionals]. So we can offer the connectionbetween the group of refugees and the professionals.We know more about the problems of refugees, andDutch organizations know more about solutions,so, the refugee organizations must be activated.We as newcomers can do primarily a lot for refugees and this society regarding refugee issues.’F32a_SY04
3.4. Agency under Pressure/Suffering & Surviving
‘We tried several things in this country but found no solution.In this country, when a teacher writes something downin his report about a child, there’s nothing you can doThere is no solution,I felt injustice against my child (..)Finally, I gave up.’F69_SY09
4. Discussion
4.1. Main Findings
4.2. Reflection on Agency and Comparison with Other Studies
4.3. Strengths and Limitations
4.4. Implications/Lessons Learned
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Schie, R. Psychische Problematiek bij Vluchtelingkinderen en—Jongeren; Handreiking-Maart 2017; Radboud Universiteit Nijmegen: Utrecht, The Netherlands; Nijmegen, The Netherlands, 2017. [Google Scholar]
- Kien, C.; Sommer, I.; Faustmann, A.; Gibson, L.; Schneider, M.; Krczal, E.; Jank, R.; Klerings, I.; Szelag, M.; Kerschner, B.; et al. Prevalence of Mental Disorders in Young Refugees and Asylum Seekers in European Countries: A Systematic Review. Eur. Child Adolesc. Psychiatry 2019, 28, 1295–1310. [Google Scholar] [CrossRef] [Green Version]
- Van Der Boor, C.F.; White, R. Barriers to Accessing and Negotiating Mental Health Services in Asylum Seeking and Refugee Populations: The Application of the Candidacy Framework. J. Immigr. Minority Health 2019, 22, 156–174. [Google Scholar] [CrossRef] [Green Version]
- Wiegersma, P.A.; Stellinga-Boelen, A.A.M.; Reijneveld, S.A. Psychosocial Problems in Asylum Seekers’ Children: The Parent, Child, and Teacher Perspective Using the Strengths and Difficulties Questionnaire. J. Nerv. Ment. Dis. 2011, 199, 85–90. [Google Scholar] [CrossRef]
- Goosen, E.S.M. A Safe and Healthy Future? Epidemiological Studies on the Health of Asylum Seekers and Refugees in the Netherlands. Ph.D. Thesis, University of Amsterdam, Utrecht, The Netherlands, 2014. Available online: https://hdl.handle.net/11245/1.417931 (accessed on 12 January 2021).
- Dagevos, J.; Huijnk, W.; Maliepaard, M.; Miltenburg, E. Syriërs in Nederland: Een Studie over de Eerste Jaren van hun Leven in Nederland; Sociaal En Cultureel Planbureau: Den Haag, The Netherlands, 2018. [Google Scholar]
- Hodes, M.; Vostanis, P. Practitioner Review: Mental Health Problems of Refugee Children and Adolescents and Their Management. J. Child Psychol. Psychiatry 2019, 60, 716–731. [Google Scholar] [CrossRef]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and Health in an Increasingly Diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Spiritus-Beerden, E.; Verelst, A.; Devlieger, I.; Langer Primdahl, N.; Botelho Guedes, F.; Chiarenza, A.; De Maesschalck, S.; Durbeej, N.; Garrido, R.; Gaspar De Matos, M.; et al. Mental Health of Refugees and Migrants during the COVID-19 Pandemic: The Role of Experienced Discrimination and Daily Stressors. Int. J. Environ. Res. Public Health 2021, 18, 6354. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.J.; House, J.S.; Israel, B.A.; Mentz, G.; Dvonch, J.T.; Miranda, P.Y.; Kannan, S.; Koch, M. Relational Pathways between Socioeconomic Position and Cardiovascular Risk in a Multiethnic Urban Sample: Complexities and Their Implications for Improving Health in Economically Disadvantaged Populations. J. Epidemiol. Community Health 2008, 62, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Hjern, A.; Jeppsson, O. Mental Health Care for Refugee Children in Exile. In Forced Migration and Mental Health: Rethinking the Care of Refugees and Displaced Persons; Ingleby, D., Ed.; International and Cultural Psychology Series; Springer: Boston, MA, USA, 2005; pp. 115–128. ISBN 978-0-387-22693-4. [Google Scholar]
- Teunissen, E.; Bavel, E.V.; Mareeuw, F.V.D.D.; Macfarlane, A.; Weel-Baumgarten, E.V.; Muijsenbergh, M.V.D.; Weel, C.V. Mental Health Problems of Undocumented Migrants in the Netherlands: A Qualitative Exploration of Recognition, Recording, and Treatment by General Practitioners. Scand. J. Prim. Health Care 2015, 33, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, P.; Damhuis, E.; Verhue, D. Samen beslissen—Rapport—Rijksoverheid.nl; Ministerie Van Algemene Zaken: The Hague, The Netherlands, 2020.
- Satinsky, E.; Fuhr, D.C.; Woodward, A.; Sondorp, E.; Roberts, B. Mental Health Care Utilisation and Access among Refugees and Asylum Seekers in Europe: A Systematic Review. Health Policy 2019, 123, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Groark, C.; Sclare, I.; Raval, H. Understanding the Experiences and Emotional Needs of Unaccompanied Asylum-Seeking Adolescents in the UK. Clin. Child Psychol. Psychiatry 2011, 16, 421–442. [Google Scholar] [CrossRef]
- Fazel, M.; Reed, R.V.; Panter-Brick, C.; Stein, A. Mental Health of Displaced and Refugee Children Resettled in High-Income Countries: Risk and Protective Factors. Lancet 2012, 379, 266–282. [Google Scholar] [CrossRef]
- Slotman, A.; Tuk, B.; De Jager, M. Werkverslag Welkom op School; Pharos: Utrecht, The Netherlands, 2014. [Google Scholar]
- Heptinstall, E.; Sethna, V.; Taylor, E. PTSD and Depression in Refugee Children. Eur. Child Adolesc. Psychiatry 2004, 13, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Pacione, L.; Measham, T.; Rousseau, C. Refugee Children: Mental Health and Effective Interventions. Curr. Psychiatry Rep. 2013, 15, 341. [Google Scholar] [CrossRef] [PubMed]
- Bronstein, I.; Montgomery, P. Psychological Distress in Refugee Children: A Systematic Review. Clin. Child Fam. Psychol. Rev. 2011, 14, 44–56. [Google Scholar] [CrossRef]
- De Haene, L.; Rober, P.; Adriaenssens, P.; Verschueren, K. Voices of Dialogue and Directivity in Family Therapy with Refugees: Evolving Ideas About Dialogical Refugee Care. Fam. Process 2012, 51, 391–404. [Google Scholar] [CrossRef]
- Van Loenen, T.; Van Den Muijsenbergh, M.; Hofmeester, M.; Dowrick, C.; Van Ginneken, N.; Mechili, E.A.; Angelaki, A.; Ajdukovic, D.; Bakic, H.; Pavlic, D.R.; et al. Primary Care for Refugees and Newly Arrived Migrants in Europe: A Qualitative Study on Health Needs, Barriers and Wishes. Eur. J. Public Health 2018, 28, 82–87. [Google Scholar] [CrossRef]
- Iliadou, M.; Papadakaki, M.; Sioti, E.; Giaxi, P.; Leontitsi, E.; Petelos, E.; Van den Muijsenbergh, M.; Tziaferi, S.; Mastroyiannakis, A.; Vivilaki, V.G. Addressing Mental Health Issues among Migrant and Refugee Pregnant Women: A Call for Action. Eur. J. Midwifery 2019, 3, 1–8. [Google Scholar] [CrossRef]
- Robertshaw, L.; Dhesi, S.; Jones, L.L. Challenges and Facilitators for Health Professionals Providing Primary Healthcare for Refugees and Asylum Seekers in High-Income Countries: A Systematic Review and Thematic Synthesis of Qualitative Research. BMJ Open 2017, 7, e015981. [Google Scholar] [CrossRef] [Green Version]
- Van Berkum, M.; Smulders, E.; Haker, F.; Bloemen, E.; Van Wieringen, J.; Looman, B.; Geraci, D.; Jansen, J. Zorg, Ondersteuning En Preventie Voor Nieuwkomende Vluchtelingen: Wat Is Er Nodig? Pharos: Utrecht, The Netherlands, 2016. [Google Scholar]
- Van Eerdewijk, A.; Wong, F.; Vaast, C.; Newton, J.; Tyszler, M.; Pennington, A. White Paper: A Conceptual Model on Women and Girls’ Empowerment; Royal Tropical Institute (KIT): Amsterdam, The Netherlands, 2017. [Google Scholar]
- Mohanty, C. Under Western Eyes: Feminist Scholarship and Colonial Discourses. Fem. Rev. 1988, 30, 61–88. [Google Scholar] [CrossRef] [Green Version]
- Mahmood, S. Feminist Theory, Embodiment, and the Docile Agent: Some Reflections on the Egyptian Islamic Revival. Cult. Anthropol. 2001, 16, 202–236. [Google Scholar] [CrossRef]
- Mahmood, S. Politics of Piety: The Islamic Revival and the Feminist Subject; Princeton University Press: Princeton, NJ, USA, 2012; ISBN 978-0-691-14980-6. [Google Scholar]
- Gammage, S.; Kabeer, N.; Van Der Meulen Rodgers, Y. Voice and Agency: Where Are We Now? Fem. Econ. 2016, 22, 1–29. [Google Scholar] [CrossRef]
- Kabeer, N. Paid Work, Women’s Empowerment and Gender Justice: Critical Pathways of Social Change. Available online: http://www.pathwaysofempowerment.org/ (accessed on 29 June 2021).
- Butler, J.; Gambetti, Z.; Sabsay, L. Vulnerability in Resistance; Duke University Press: Durham, NC, USA, 2016; ISBN 978-0-8223-7349-0. [Google Scholar]
- Madhok, S.; Phillips, A.; Wilson, K.; Hemmings, C. Gender, Agency, and Coercion; Palgrave Macmillan: London, UK, 2013; ISBN 978-1-137-29561-3. [Google Scholar]
- Willan, S.; Gibbs, A.; Petersen, I.; Jewkes, R. Exploring Young Women’s Reproductive Decision-Making, Agency and Social Norms in South African Informal Settlements. PLoS ONE 2020, 15, e0231181. [Google Scholar] [CrossRef]
- Clare, S. Agency, Signification, and Temporality. Hypatia 2009, 24, 50–62. [Google Scholar] [CrossRef]
- Butler, J. The Psychic Life of Power: Theories in Subjection; Stanford University Press: Palo Alto, CA, USA, 1997; ISBN 978-0-8047-2812-6. [Google Scholar]
- Bracke, S. Bouncing Back: Vulnerability and Resistance in Times of Resilience. In Vulnerability in Resistance; Duke University Press: Durham, NC, USA, 2016; pp. 52–75. ISBN 978-0-8223-7349-0. [Google Scholar]
- EmpowerMENT: EMPOWERende, Integrale Persoonsgerichte Ondersteuning en Samenwerking Vanuit de Eerste lijn Voor Screening, Begeleiding en Verwijzing bij Vluchtelingkinderen Met MENTale Problemen—ZonMw. Available online: https://www.zonmw.nl/nl/onderzoek-resultaten/geestelijke-gezondheid-ggz/programmas/project-detail/zorg-voor-vluchtelingen/empowerment-empowerende-integrale-persoonsgerichte-ondersteuning-en-samenwerking-vanuit-de-eerste/ (accessed on 24 November 2021).
- “Shabab Akwa”—“Stronger Youth”. Empowerment “PLUS”—Empowerment of Self-Management and Care Seeking Behaviour for Refugee Childrens’ Stress-Related Health Problems.|NOW. Available online: https://www.nwo.nl/en/projects/vidw115419004 (accessed on 24 November 2021).
- Strauss, A.; Corbin, J. Discovery of Grounded Theory; Weidenfield & Nicolson: London, UK, 1967; pp. 1–19. [Google Scholar]
- Kooiker, S.; Hoeymans, N. Burgers en Gezondheid: Themarapport Volksgezondheid Toekomst Verkenning 2014; RIVM: Bilthoven, The Netherlands, 2014; ISBN 978-90-6960-269-1.
- Tengland, P.-A. Behavior Change or Empowerment: On the Ethics of Health-Promotion Goals. Health Care Anal. 2016, 24, 24–46. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, K.; Dihle, A.; Hansen, C.; Nordhaug, M.; Jerpseth, H.; Tveiten, S.; Joranger, P.; Ruud Knutsen, I. Empowerment in Healthcare: A Thematic Synthesis and Critical Discussion of Concept Analyses of Empowerment. Patient Educ. Couns. 2020, 103, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Davids, T. Trying to Be a Vulnerable Observer: Matters of Agency, Solidarity and Hospitality in Feminist Ethnography. Women’s Stud. Int. Forum 2014, 43, 50–58. [Google Scholar] [CrossRef]
- Paudyal, P.; Tattan, M.; Cooper, M.J.F. Qualitative Study on Mental Health and Well-Being of Syrian Refugees and Their Coping Mechanisms towards Integration in the UK. BMJ Open 2021, 11, e046065. [Google Scholar] [CrossRef]
- Lewis, H.; Dwyer, P.; Hodkinson, S.; Waite, L. Hyper-Precarious Lives: Migrants, Work and Forced Labour in the Global North. Prog. Hum. Geogr. 2015, 39, 580–600. [Google Scholar] [CrossRef] [Green Version]
- Butler, J. Performativity, Precarity and Sexual Politics 1. Rev. Antropol. Iberoam. 2009, 4, i–xiii. [Google Scholar]
- Bracke, S. Is the Subaltern Resilient? Notes on Agency and Neoliberal Subjects. Cult. Stud. 2016, 30, 839–855. [Google Scholar] [CrossRef]
- Barber, B.K.; McNeely, C.A.; Sarraj, E.E.; Daher, M.; Giacaman, R.; Arafat, C.; Barnes, W.; Mallouh, M.A. Mental Suffering in Protracted Political Conflict: Feeling Broken or Destroyed. PLoS ONE 2016, 11, e0156216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S. Living a Feminist Life; Duke University Press: Durham, NC, USA, 2017; ISBN 978-0-8223-7337-7. [Google Scholar]
- Bohlmeijer, E. 1 Herinneringen, levensverhalen en gezondheid. In De Betekenis van Levensverhalen: Theoretische Beschouwingen en Toepassingen in Onderzoek en Praktijk; Bohlmeijer, E., Mies, L., Westerhof, G., Eds.; Bohn Stafleu Van Loghum: Houten, The Netherlands, 2007; pp. 29–39. ISBN 978-90-313-6400-8. [Google Scholar]
- Dierx, J.; Kasper, H. Refining Insights on the Impact of SES on Perceived Health: A Positive Health Perspective (preprint). Res. Sq. 2021. [Google Scholar] [CrossRef]


{kind=link}
| ID Code | Home Country | Male (M)/Female (F) + Age | Educational Level | Duration of Stay in NL * [in Years] | Number of Children * |
|---|---|---|---|---|---|
| SY01 | Syria | F57 | Lower vocational education | 5 | 3 |
| SY02 | Syria | F36 | University education | 5 | 2 |
| YE01 | Yemen | F29 | Lower vocational education | 10 | 5 |
| SY03 | Syria | M33 | University education | 6 | 0 |
| SY04 | Syria | F41 | University education | 6 | 2 |
| SY05 | Syria | F39 | University education | 5 | 2 |
| SY06 | Syria | F32 | Lower vocational education | 6 | 3 |
| SY07 | Syria | F48 | No education | 5 | 4 |
| SY08 | Syria | M44 | University education | 6 | 2 |
| SY09 | Syria | F44 | University education | 4 | 4 |
| SY10 | Syria | F54 | Higher vocational education | 5 | 3 |
| YE02 | Yemen | F37 | Higher vocational education | 2 | 3 |
| SY11 | Syria | M40 | Higher vocational education | 6 | 3 |
| IR01 | Iran | F29 | No education | 5 | 1 |
| AF01 | Afghanistan | F42 | Secondary school | 12 | 4 |
| AF02 | Afghanistan | M31 | University education | 12 | 0 |
| AF03 | Afghanistan | F56 | Higher vocational education | 16 | 4 |
| AR01 | Armenia | F20 | Vocational education | <1 | 0 ** |
| AR02 | Armenia (mother + daughter) | F66 F33 | Vocational education University education | 6 4 | 2 0 |
| ER01 | Eritrea (couple) | F33 M36 | Higher vocational education University education | 4 6 | 3 |
| ER02 | Eritrea (couple) | F34 M51 | Secondary school Higher vocational education | 3 4 | 4 |
| ER03 | Eritrea (couple) | F25 M29 | Secondary school Secondary school | 5 both | 2 |
| IR02 | Iran | M49 | Higher vocational education | 9 | 1 |
| KT01 | Turkish Kurdistan (couple) | F31 M33 | University education University education | 13 both | 1 (new-born) |
| VIE01 | Vietnam | F55 | Higher vocational education | 16 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renkens, J.; Rommes, E.; van den Muijsenbergh, M. Refugees' Agency: On Resistance, Resilience, and Resources. Int. J. Environ. Res. Public Health 2022, 19, 806. https://doi.org/10.3390/ijerph19020806
Renkens J, Rommes E, van den Muijsenbergh M. Refugees' Agency: On Resistance, Resilience, and Resources. International Journal of Environmental Research and Public Health. 2022; 19(2):806. https://doi.org/10.3390/ijerph19020806
Chicago/Turabian StyleRenkens, José, Els Rommes, and Maria van den Muijsenbergh. 2022. "Refugees' Agency: On Resistance, Resilience, and Resources" International Journal of Environmental Research and Public Health 19, no. 2: 806. https://doi.org/10.3390/ijerph19020806
APA StyleRenkens, J., Rommes, E., & van den Muijsenbergh, M. (2022). Refugees' Agency: On Resistance, Resilience, and Resources. International Journal of Environmental Research and Public Health, 19(2), 806. https://doi.org/10.3390/ijerph19020806