
Assessment of the Long-Term Mental Health Effects on Austrian Students after COVID-19 Restrictions
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
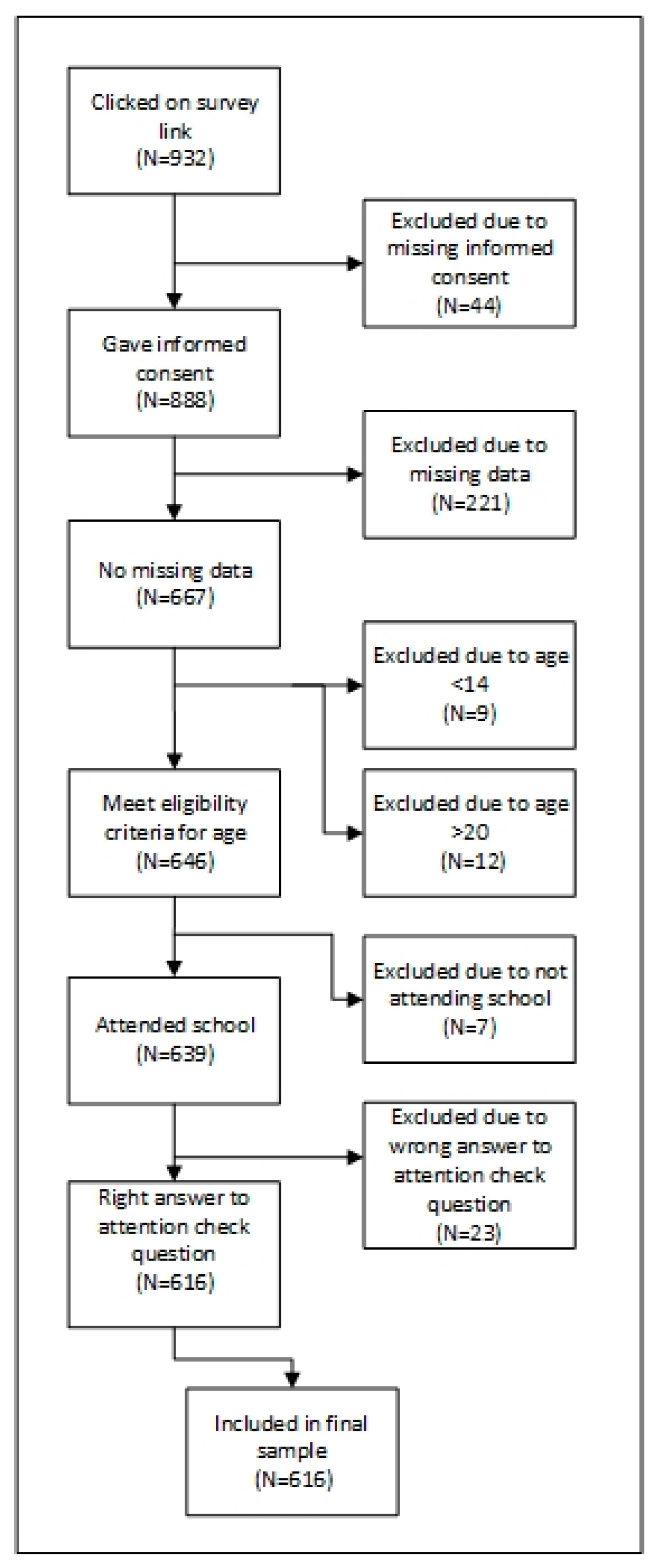
2.2. Participants
2.3. Variables
2.3.1. Well-Being
2.3.2. Stress
2.3.3. Depression
2.3.4. Suicidal Ideation
2.3.5. Anxiety
2.3.6. Insomnia
2.3.7. Smartphone Usage
2.3.8. Physical Activity
2.3.9. Gender
2.4. Study Sample Size
2.5. Statistical Analyses
3. Results
3.1. Sample
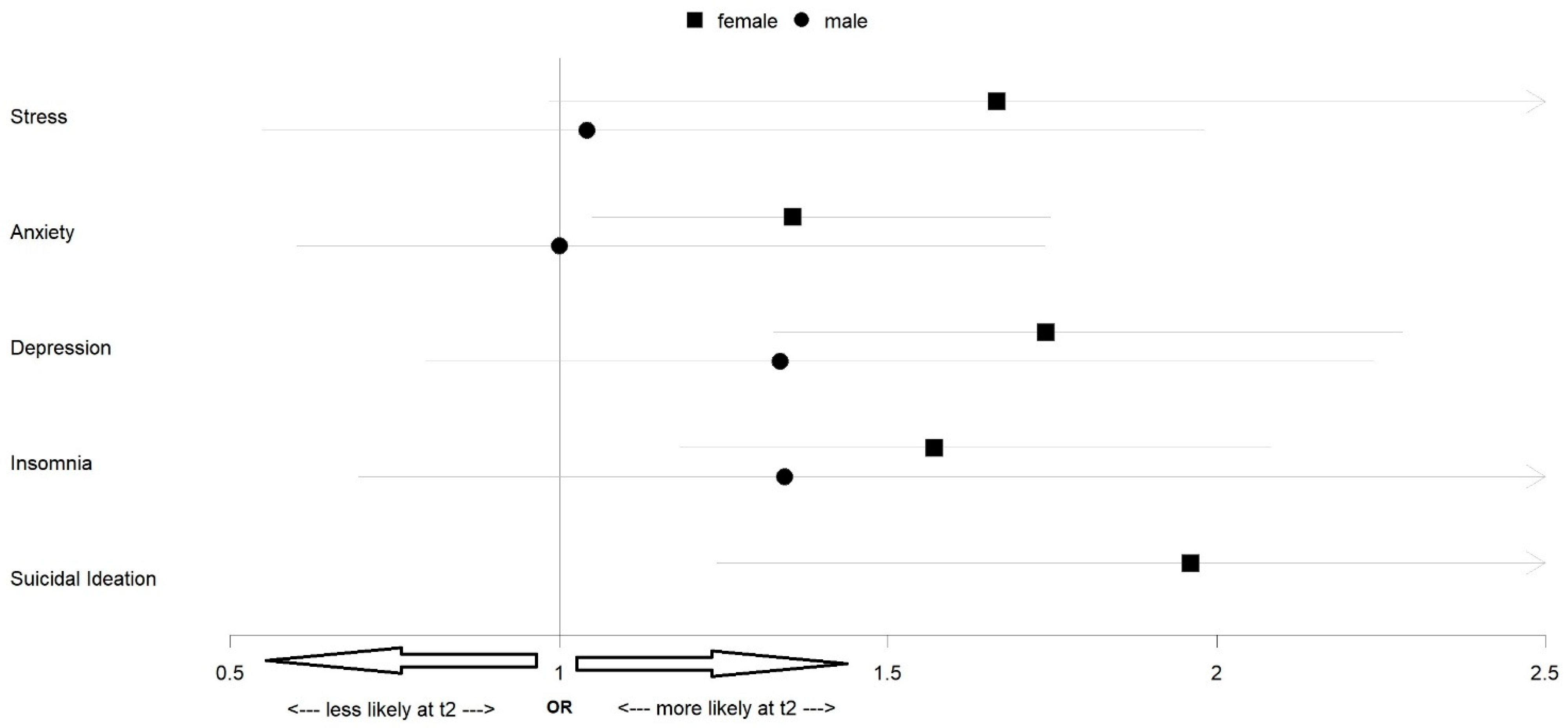
3.2. Mental Health Measures
3.3. Smartphone Usage
3.4. Physical Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Octavius, G.S.; Silviani, F.R.; Lesmandjaja, A.; Angelina; Juliansen, A. Impact of COVID-19 on adolescents’ mental health: A systematic review. Middle East Curr. Psychiatry 2020, 27, 72. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2022, 31, 879–889. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Humer, E.; Probst, T. Comparing Mental Health During the COVID-19 Lockdown and 6 Months after the Lockdown in Austria: A Longitudinal Study. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef]
- Pieh, C.; Probst, T.; Budimir, S.; Humer, E. Diminished well-being persists beyond the end of the COVID-19 lockdown. Gen. Hosp. Psychiatry 2021, 70, 137–138. [Google Scholar] [CrossRef]
- Dale, R.; Budimir, S.; Probst, T.; Stippl, P.; Pieh, C. Mental Health during the COVID-19 Lockdown over the Christmas Period in Austria and the Effects of Sociodemographic and Lifestyle Factors. Int. J. Environ. Res. Public. Health 2021, 18, 3679. [Google Scholar] [CrossRef]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.-L.; Bonell, C.; Hudson, L.; et al. School Closures During Social Lockdown and Mental Health, Health Behaviors, and Well-being Among Children and Adolescents During the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef]
- Albrecht, J.N.; Werner, H.; Rieger, N.; Widmer, N.; Janisch, D.; Huber, R.; Jenni, O.G. Association Between Homeschooling and Adolescent Sleep Duration and Health During COVID-19 Pandemic High School Closures. JAMA Netw. Open 2022, 5, e2142100. [Google Scholar] [CrossRef] [PubMed]
- Poulain, T.; Meigen, C.; Sobek, C.; Ober, P.; Igel, U.; Körner, A.; Kiess, W.; Vogel, M. Loss of childcare and classroom teaching during the COVID-19-related lockdown in spring 2020: A longitudinal study on consequences on leisure behavior and schoolwork at home. PLoS ONE 2021, 16, e0247949. [Google Scholar] [CrossRef] [PubMed]
- Calvano, C.; Engelke, L.; Di Bella, J.; Kindermann, J.; Renneberg, B.; Winter, S.M. Families in the COVID-19 pandemic: Parental stress, parent mental health and the occurrence of adverse childhood experiences—Results of a representative survey in Germany. Eur. Child Adolesc. Psychiatry 2022, 31, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) Pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Houghton, S.; Kyron, M.; Hunter, S.C.; Lawrence, D.; Hattie, J.; Carroll, A.; Zadow, C. Adolescents’ longitudinal trajectories of mental health and loneliness: The impact of COVID-19 school closures. J. Adolesc. 2022, 94, 191–205. [Google Scholar] [CrossRef] [PubMed]
- Hammerstein, S.; König, C.; Dreisörner, T.; Frey, A. Effects of COVID-19-Related School Closures on Student Achievement—A Systematic Review. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Jesser, A.; Schaffler, Y.; Gächter, A.; Dale, R.; Humer, E.; Pieh, C. School Students’ Concerns and Support after One Year of COVID-19 in Austria: A Qualitative Study Using Content Analysis. Healthcare 2022, 10, 1334. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.M.D.D.; Butini, L.; Pauletto, P.; Lehmkuhl, K.M.; Stefani, C.M.; Bolan, M.; Guerra, E.; Dick, B.; De Luca Canto, G.; Massignan, C. Mental health effects prevalence in children and adolescents during the COVID-19 pandemic: A systematic review. Worldviews Evid. Based Nurs. 2022, 19, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Plener, P.L.; Probst, T.; Dale, R.; Humer, E. Assessment of Mental Health of High School Students During Social Distancing and Remote Schooling During the COVID-19 Pandemic in Austria. JAMA Netw. Open 2021, 4, e2114866. [Google Scholar] [CrossRef] [PubMed]
- Humer, E.; Dale, R.; Plener, P.L.; Probst, T.; Pieh, C. Assessment of Mental Health of High School Students 1 Semester After COVID-19–Associated Remote Schooling Measures Were Lifted in Austria in 2021. JAMA Netw. Open 2021, 4, e2135571. [Google Scholar] [CrossRef]
- Dale, R.; Jesser, A.; Pieh, C.; O’Rourke, T.; Probst, T.; Humer, E. Mental health burden of high school students, and suggestions for psychosocial support, 1.5 years into the COVID-19 pandemic in Austria. Eur. Child Adolesc. Psychiatry 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Halldorsdottir, T.; Thorisdottir, I.E.; Meyers, C.C.A.; Asgeirsdottir, B.B.; Kristjansson, A.L.; Valdimarsdottir, H.B.; Allegrante, J.P.; Sigfusdottir, I.D. Adolescent well-being amid the COVID-19 pandemic: Are girls struggling more than boys? JCPP Adv. 2021, 1, e12027. [Google Scholar] [CrossRef] [PubMed]
- Bian, S. The Impact of COVID-19 Pandemic on Problematic Smartphone Using Among Adolescents. In Proceedings of the 2021 4th International Conference on Humanities Education and Social Sciences, Xishuangbanna, China, 29–31 October 2021. [Google Scholar]
- Wacks, Y.; Weinstein, A.M. Excessive Smartphone Use Is Associated With Health Problems in Adolescents and Young Adults. Front. Psychiatry 2021, 12, 669042. [Google Scholar] [CrossRef] [PubMed]
- Marconcin, P.; Werneck, A.O.; Peralta, M.; Ihle, A.; Gouveia, É.R.; Ferrari, G.; Sarmento, H.; Marques, A. The association between physical activity and mental health during the first year of the COVID-19 pandemic: A systematic review. BMC Public Health 2022, 22, 209. [Google Scholar] [CrossRef]
- Li, M.; Wang, Q.; Shen, J. The Impact of Physical Activity on Mental Health during COVID-19 Pandemic in China: A Systematic Review. Int. J. Environ. Res. Public. Health 2022, 19, 6584. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, 31. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Brähler, E.; Mühlan, H.; Albani, C.; Schmidt, S. Teststatistische Prüfung und Normierung der deutschen Versionen des EUROHIS-QOL Lebensqualität-Index und des WHO-5 Wohlbefindens-Index. Diagnostica 2007, 53, 83–96. [Google Scholar] [CrossRef]
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale–psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Richardson, L.P.; McCauley, E.; Grossman, D.C.; McCarty, C.A.; Richards, J.; Russo, J.E.; Rockhill, C.; Katon, W. Evaluation of the Patient Health Questionnaire-9 Item for Detecting Major Depression Among Adolescents. Pediatrics 2010, 126, 1117–1123. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.; Lang, C.; Lemola, S.; Colledge, F.; Kalak, N.; Holsboer-Trachsler, E.; Pühse, U.; Brand, S. Validation of the German version of the insomnia severity index in adolescents, young adults and adult workers: Results from three cross-sectional studies. BMC Psychiatry 2016, 16, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Teutsch, F.; Ramelow, D.; Maier, G.; Felder-Puig, R. Lineartabellen zu den Ergebnissen der HBSC-Studie 2018: Gesundheit und Gesundheitsverhalten von Schülerinnen und Schülern in Österreich; Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentenschutz: Vienna, Austria, 2018. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/publications-detail-redirect/9789241599979 (accessed on 21 September 2022).
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Koletsi, D.; Pandis, N. Matched analysis for paired binary data (McNemar test). Am. J. Orthod. Dentofacial Orthop. 2017, 151, 222–223. [Google Scholar] [CrossRef] [Green Version]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Lenhard, W.; Lenhard, A. Testing the Significance of Correlations. Psychometrica 2014. [Google Scholar] [CrossRef]
- American Association for Public Opinion Research. Standard Definitions.Final Dispositions of Case Codes and Outcome Rates for Surveys; American Association for Public Opinion Research: Alexandria, VA, USA, 2016; p. 81. [Google Scholar]
- Mendolia, S.; Suziedelyte, A.; Zhu, A. Have girls been left behind during the COVID-19 pandemic? Gender differences in pandemic effects on children’s mental wellbeing. Econ. Lett. 2022, 214, 110458. [Google Scholar] [CrossRef]
- Magson, N.R.; Freeman, J.Y.A.; Rapee, R.M.; Richardson, C.E.; Oar, E.L.; Fardouly, J. Risk and Protective Factors for Prospective Changes in Adolescent Mental Health during the COVID-19 Pandemic. J. Youth Adolesc. 2021, 50, 44–57. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Ciaccioni, S.; Thomas, G.; Vergeer, I. Physical activity and mental health in children and adolescents: An updated review of reviews and an analysis of causality. Psychol. Sport Exerc. 2019, 42, 146–155. [Google Scholar] [CrossRef]
- McMahon, E.M.; Corcoran, P.; O’Regan, G.; Keeley, H.; Cannon, M.; Carli, V.; Wasserman, C.; Hadlaczky, G.; Sarchiapone, M.; Apter, A.; et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur. Child Adolesc. Psychiatry 2017, 26, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Vilhjalmsson, R.; Kristjansdottir, G. Gender differences in physical activity in older children and adolescents: The central role of organized sport. Soc. Sci. Med. 2003, 56, 363–374. [Google Scholar] [CrossRef]
- David, M.E.; Roberts, J.A. Smartphone Use during the COVID-19 Pandemic: Social Versus Physical Distancing. Int. J. Environ. Res. Public. Health 2021, 18, 1034. [Google Scholar] [CrossRef] [PubMed]
- Prowse, R.; Sherratt, F.; Abizaid, A.; Gabrys, R.L.; Hellemans, K.G.C.; Patterson, Z.R.; McQuaid, R.J. Coping with the COVID-19 Pandemic: Examining Gender Differences in Stress and Mental Health among University Students. Front. Psychiatry 2021, 12, 650759. [Google Scholar] [CrossRef] [PubMed]
- Soutar, C.; Wand, A.P.F. Understanding the Spectrum of Anxiety Responses to Climate Change: A Systematic Review of the Qualitative Literature. Int. J. Environ. Res. Public. Health 2022, 19, 990. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| t1 a | t2 b | Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Gender | ||||||
| Girl | 481 | 80.3 | 477 | 79.6 | 958 | 80 |
| Boy | 118 | 19.7 | 122 | 20.4 | 240 | 20 |
| Migration background | ||||||
| No | 491 | 82.0 | 488 | 81.5 | 979 | 81.7 |
| Yes | 108 | 18.0 | 111 | 18.5 | 219 | 18.3 |
| Region | ||||||
| Northeast | 380 | 63.4 | 379 | 63.3 | 759 | 63.4 |
| Southeast | 171 | 28.5 | 172 | 28.7 | 343 | 28.6 |
| West | 48 | 8 | 48 | 8 | 96 | 8 |
| Age M (SD) | 16.64 (1.46) | 16.66 (1.48) | 16.65 (1.47) | |||
| Total | Girls | Boys | |||
|---|---|---|---|---|---|
| t1 | t2 | t1 | t2 | Statistics | |
| N | 481 | 477 | 118 | 122 | |
| WHO-5 M (SD) | 36.62 (18.95) | 32.69 (18.71) | 44.61 (23.07) | 44.03 (20.60) | F(2;1195) = 27.78; p < 0.001 |
| PHQ-9 M (SD) | 11.99 (6.02) | 14.16 (6.18) | 9.19 (6.55) | 10.70 (6.53) | F(2;1195) = 27.78; p < 0.001 |
| ≥11, % (n) | 60 (290) | 73 (346) | 37 (44) | 44 (54) | |
| GAD-7 M (SD) | 10.80 (4.96) | 11.48 (5.04) | 8.05 (5.22) | 8.56 (5.52) | F(2;1195) = 32.32; p < 0.001 |
| ≥11, % (n) | 50 (238) | 57 (272) | 35 (41) | 35 (43) | |
| ISI M (SD) | 10.85 (5.31) | 11.89 (6.20) | 8.26 (5.67) | 9.55 (6.16) | F(2;1195) = 22.39; p < 0.001 |
| ≥15, %(n) | 24 (117) | 34 (160) | 16 (19) | 21 (25) | |
| PSS-10 M (SD) | 24.35 (6.83) | 24.90 (6.61) | 20.20 (7.90) | 20.02 (7.70) | F(2;1195) = 40.90; p < 0.001 |
| ≥14, % (n) | 92 (442) | 95 (453) | 81 (95) | 81 (99) | |
| Suicidal ideations | |||||
| ≥“more than half the days” % (n) | 12 (59) | 24 (114) | 10 (12) | 12 (15) | |
| Smartphone Use | |||||||
|---|---|---|---|---|---|---|---|
| <1 h/Day | 1–2 h/Day | 3–4 h/Day | 5–6 h/Day | 7–8 h/Day | >8 h/Day | ||
| Boys | t1 | 0.8% (1) | 11.9% (14) | 31.4% (37) | 30.5% (36) | 15.3% (18) | 10.2% (12) |
| t2 | 0.8% (1) | 19.7% (24) | 47.5% (58) | 16.4% (20) | 7.4% (9) | 8.2% (10) | |
| Girls | t1 | 1% (5) | 10.2% (49) | 32.8% (158) | 25.2% (121) | 16.6% (80) | 14.1% (68) |
| t2 | 1.5% (7) | 13.4% (64) | 38.8% (185) | 26.4% (126) | 11.5 (55) | 8.4% (40) | |
| Physical Activity | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Days/Week | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| Boys | t1 | 11.9% (14) | 12.7% (15) | 16.1% (19) | 10.2% (12) | 11.9% (14) | 11.9% (14) | 5.9% (7) | 19.5% (23) |
| t2 | 11.5% (14) | 13.9% (17) | 19.7% (24) | 18.9% (23) | 9% (11) | 8.2% (10) | 9.8% (12) | 9% (11) | |
| Girls | t1 | 7.1% (34) | 14.3% (69) | 19.1% (92) | 20.2% (97) | 16% (77) | 9.8% (47) | 6% (29) | 7.5% (36) |
| t2 | 15.3% (73) | 17.4% (83) | 17.6% (84) | 18.9% (90) | 10.3% (49) | 8.4% (40) | 5.9% (28) | 6.3% (30) | |
| Girls | Boys | |||
|---|---|---|---|---|
| Variable | 1. Smartphone Use | 2. Physical Activity | 1. Smartphone Use | 2. Physical Activity |
| 1. Smartphone use | ||||
| 2. Physical activity | −0.221 ** | −0.144 | ||
| 3. General anxiety | 0.135 ** | −0.192 ** | 0.160 | −0.213 * |
| 4. Depression | 0.214 ** | −0.164 ** | 0.335 ** | −0.077 |
| 5. Insomnia | 0.185 ** | −0.171 ** | 0.353 ** | −0.136 |
| 6. Well-being | −0.213 ** | 0.264 ** | −0.235 * | 0.235 ** |
| 7. Stress | 0.144 ** | −0.170 ** | 0.311 ** | −0.292 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaltschik, S.; Pieh, C.; Dale, R.; Probst, T.; Pammer, B.; Humer, E. Assessment of the Long-Term Mental Health Effects on Austrian Students after COVID-19 Restrictions. Int. J. Environ. Res. Public Health 2022, 19, 13110. https://doi.org/10.3390/ijerph192013110
Kaltschik S, Pieh C, Dale R, Probst T, Pammer B, Humer E. Assessment of the Long-Term Mental Health Effects on Austrian Students after COVID-19 Restrictions. International Journal of Environmental Research and Public Health. 2022; 19(20):13110. https://doi.org/10.3390/ijerph192013110
Chicago/Turabian StyleKaltschik, Stefan, Christoph Pieh, Rachel Dale, Thomas Probst, Barbara Pammer, and Elke Humer. 2022. "Assessment of the Long-Term Mental Health Effects on Austrian Students after COVID-19 Restrictions" International Journal of Environmental Research and Public Health 19, no. 20: 13110. https://doi.org/10.3390/ijerph192013110
APA StyleKaltschik, S., Pieh, C., Dale, R., Probst, T., Pammer, B., & Humer, E. (2022). Assessment of the Long-Term Mental Health Effects on Austrian Students after COVID-19 Restrictions. International Journal of Environmental Research and Public Health, 19(20), 13110. https://doi.org/10.3390/ijerph192013110