

A Single Dose of Beer after Moderate Aerobic Exercise Did Not Affect the Cardiorespiratory and Autonomic Recovery in Young Men and Women: A Crossover, Randomized and Controlled Trial
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Ethical Approval and Informed Consent
2.4. Initial Assessment
2.5. Outcomes
2.5.1. Cardiovascular Variables
2.5.2. HR and HRV Analysis
2.6. Interventions
2.6.1. Initial Assessment
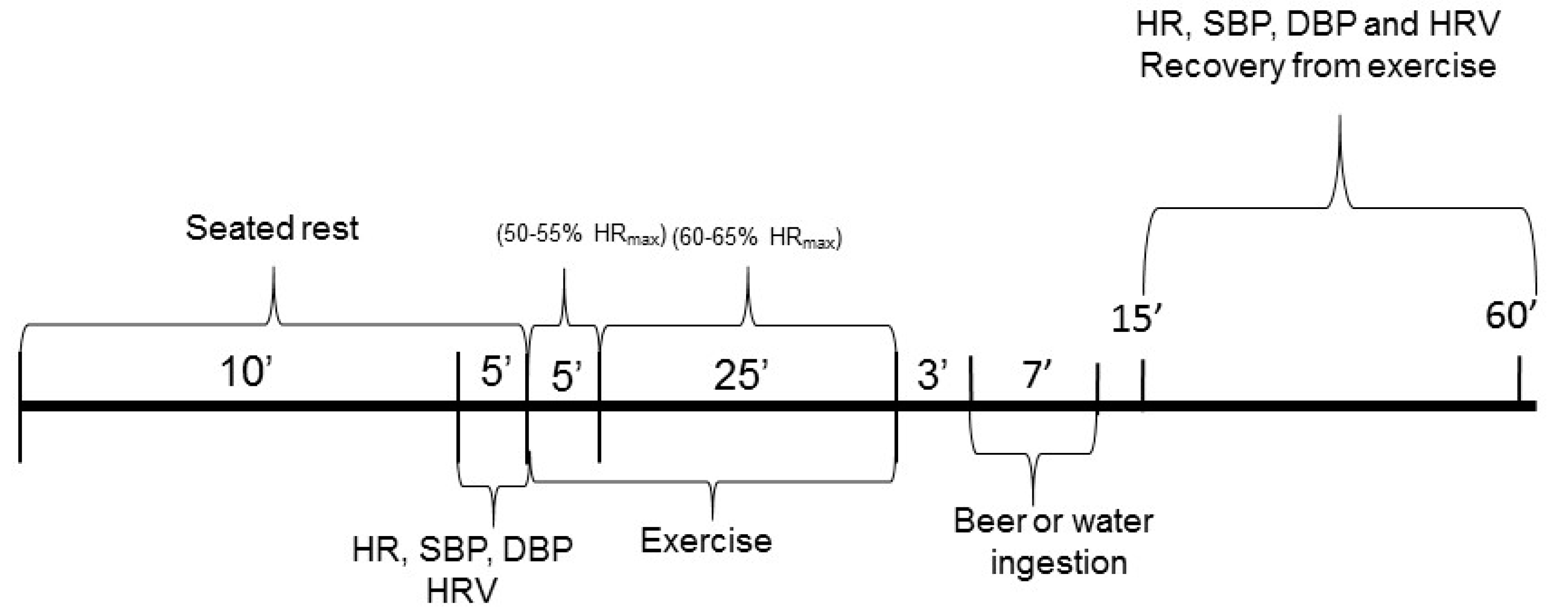
2.6.2. Experimental Protocols
2.7. Beer Composition
2.8. Sample Size
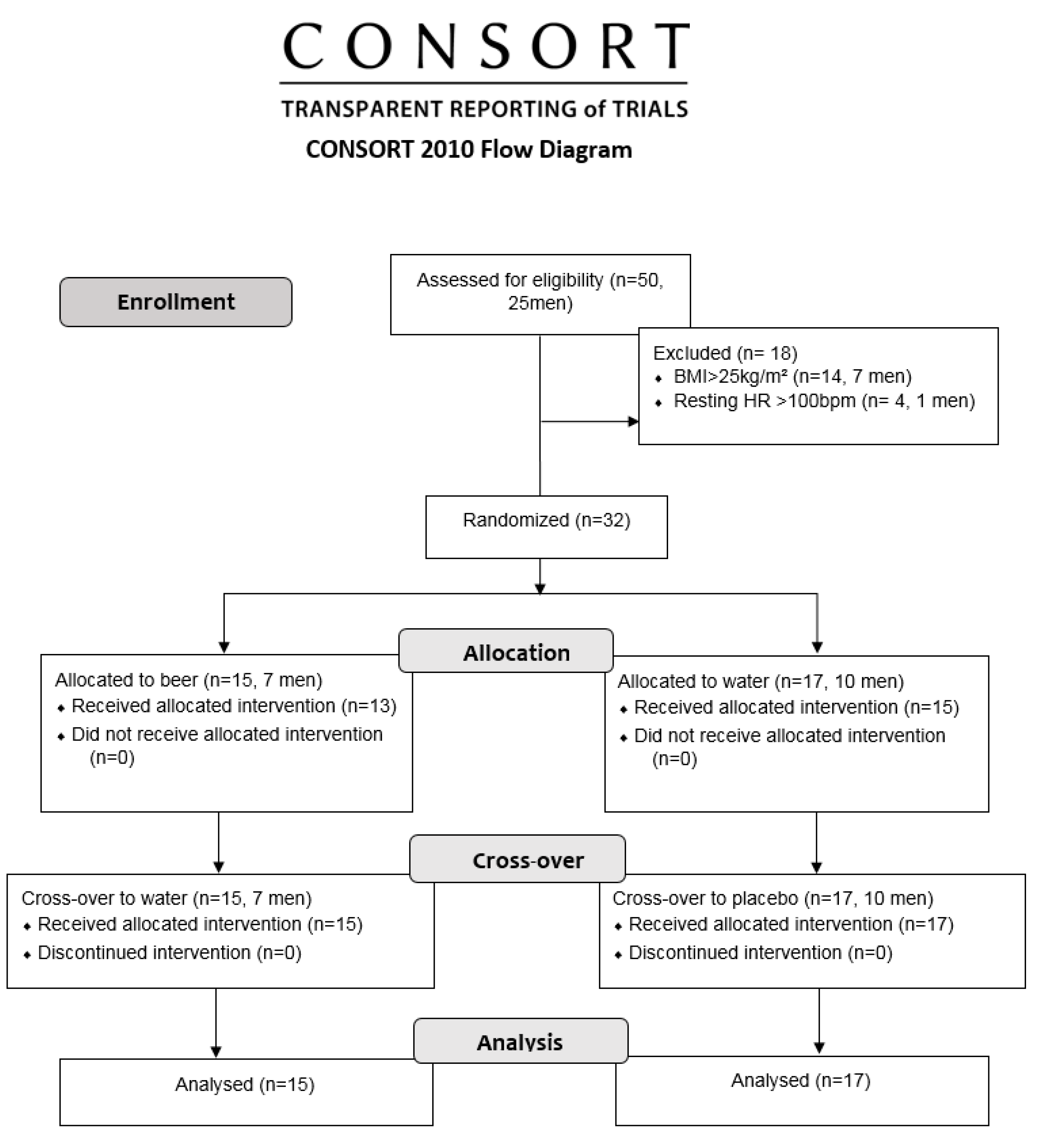
2.9. Randomization
2.10. Statistical Methods
3. Results
3.1. Sample Profile
3.2. HR, SBP and DBP during Recovery from Exercise
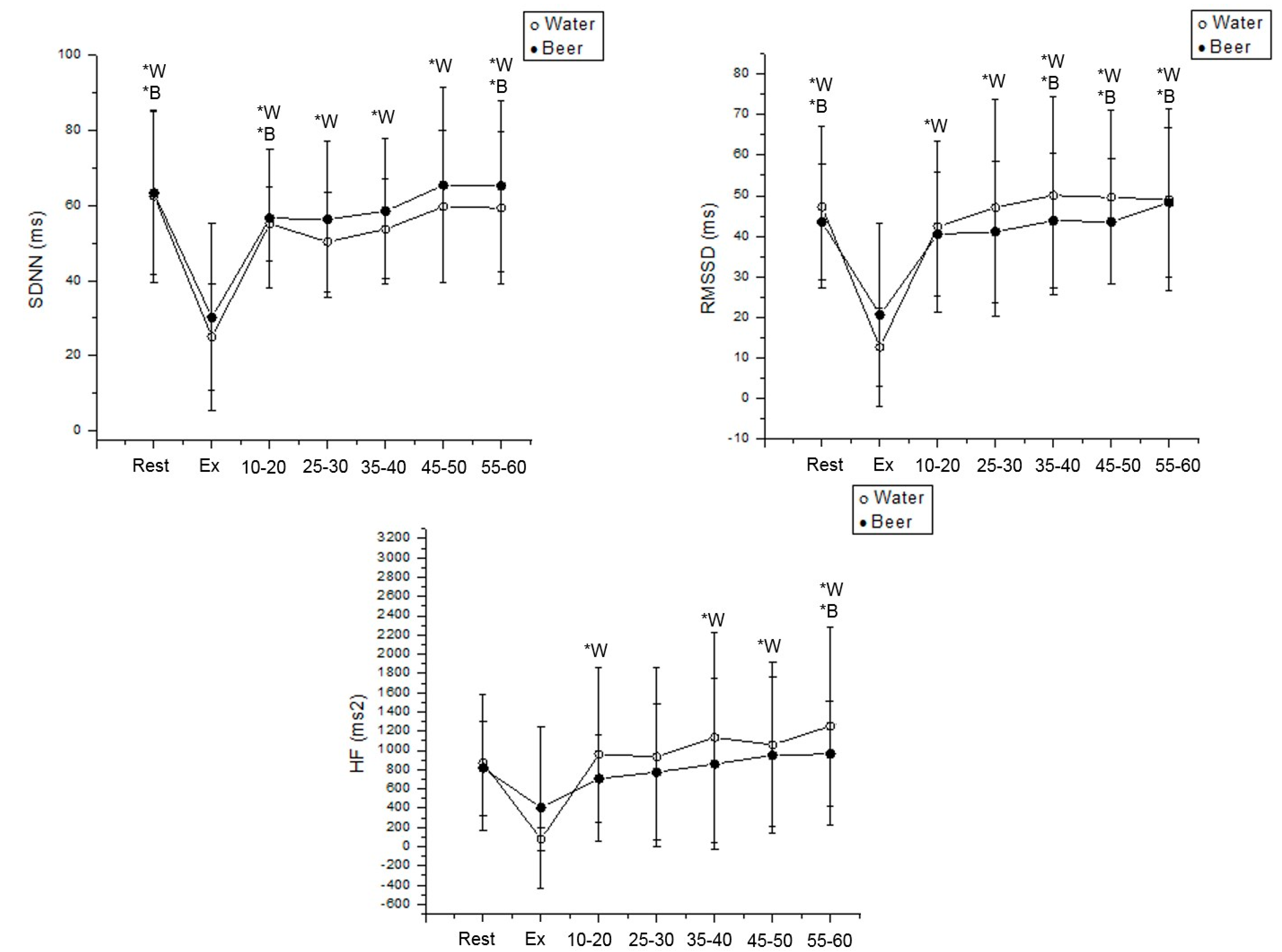
3.3. HRV during Exercise and following Effort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Alcohol in the European Union: Consumption, Harm and Policy Approaches; World Health Organization: Geneva, Switzerland, 2012; pp. 10–28. [Google Scholar]
- Adjemian, M.K.; Street, E. Alcohol Consumption and Food-at-Home Dietary Quality in the United States. In Proceedings of the 2012 Annual Meeting, Seattle, DC, USA, 12–14 August 2012; pp. 1–25. [Google Scholar]
- Varela, J.; Varela, C. Microbiological strategies to produce beer and wine with reduced ethanol concentration. Curr. Opin. Biotechnol. 2019, 56, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Martens, M.P.; Dams-O’Connor, K.; Beck, N.C. A systematic review of college student-athlete drinking: Prevalence rates, sport-related factors, and interventions. J. Subst. Abuse Treat. 2006, 31, 305–316. [Google Scholar] [CrossRef]
- Desbrow, B.; Barnes, K.; Cox, G.R.; Iudakhina, E.; McCartney, D.; Skepper, S.; Young, C.; Irwin, C. Calorie-containing recovery drinks increase recreational runners’ voluntary energy and carbohydrate intake, with minimal impact on fluid recovery. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 359–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, L.M.; Collier, G.R.; Broad, E.M.; Davis, P.G.; Martin, D.T.; Sanigorski, A.J.; Hargreaves, M. Effect of alcohol intake on muscle glycogen storage after prolonged exercise. J. Appl. Physiol. 2003, 95, 983–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, H.A.; Hengist, A.; Bonson, D.J.; Walhin, J.-P.; Jones, R.; Tsintzas, K.; Afman, G.H.; Gonzalez, J.T.; Betts, J.A. Muscle Glycogen Utilization during Exercise after Ingestion of Alcohol. Med. Sci. Sports Exerc. 2021, 53, 211–217. [Google Scholar] [CrossRef]
- Dawson, D.; Reid, K.J. Fatigue, alcohol and performance impairment. Nature 1997, 388, 235. [Google Scholar] [CrossRef] [PubMed]
- Parr, E.; Camera, D.; Areta, J.; Burke, L.M.; Phillips, S.; Hawley, J.A.; Coffey, V.G. Alcohol Ingestion Impairs Maximal Post-Exercise Rates of Myofibrillar Protein Synthesis following a Single Bout of Concurrent Training. PLoS ONE 2014, 9, e88384. [Google Scholar] [CrossRef] [Green Version]
- McManus, D.D.; Yin, X.; Gladstone, R.; Vittinghoff, E.; Vasan, R.S.; Larson, M.G.; Benjamin, E.J.; Marcus, G.M. Alcohol Consumption, Left Atrial Diameter, and Atrial Fibrillation. J. Am. Hear. Assoc. 2016, 5, e004060. [Google Scholar] [CrossRef] [Green Version]
- Brunner, S.; Herbel, R.; Drobesch, C.; Peters, A.; Massberg, S.; Kääb, S.; Sinner, M.F. Alcohol consumption, sinus tachycardia, and cardiac arrhythmias at the Munich Octoberfest: Results from the Munich Beer Related Electrocardiogram Workup Study (MunichBREW). Eur. Heart J. 2017, 38, 2100–2106. [Google Scholar] [CrossRef] [Green Version]
- Koskinen, P.; Virolainen, J.; Kupari, M. Acute Alcohol Intake Decreases Short-Term Heart Rate Variability in Healthy Subjects. Clin. Sci. 1994, 87, 225–230. [Google Scholar] [CrossRef]
- Kumar, D.M.; Kumar, P.; Sudarshan, B.G.; Yadhuraj, S.R. A study on impact of alcohol among young Indian population using HRV analysis. Int. J. Comput. Sci. Eng. Inf. Technol. 2014, 4, 55–65. [Google Scholar] [CrossRef]
- Julian, T.H.; Syeed, R.; Glascow, N.; Zis, P. Alcohol-induced autonomic dysfunction: A systematic review. Clin. Auton. Res. 2019, 30, 29–41. [Google Scholar] [CrossRef] [Green Version]
- Siscovick, D.S.; Weiss, N.S.; Fletcher, R.H.; Lasky, T. The incidence of primary cardiac arrest during vigorous exercise. N. Engl. J. Med. 1984, 311, 874–877. [Google Scholar] [CrossRef]
- Albert, C.M.; Mittleman, M.A.; Chae, C.U.; Lee, I.M.; Hennekens, C.H.; Manson, J.E. Triggering of sudden death from cardiac causes by vigorous exertion. N. Engl. J. Med. 2001, 344, 854–855. [Google Scholar] [CrossRef]
- Peçanha, T.; Bartels, R.; Brito, L.C.; Paula-Ribeiro, M.; Oliveira, R.S.; Goldberger, J.J. Methods of assessment of the post-exercise cardiac autonomic recovery: A methodological review. Int. J. Cardiol. 2017, 227, 795–802. [Google Scholar] [CrossRef]
- Porto, A.A.; Benjamim, C.J.R.; Gonzaga, L.A.; Luciano de Almeida, M.; Bueno Júnior, C.R.; Garner, D.M.; Valenti, V.E. Caffeine intake and its influences on heart rate variability recovery in healthy active adults after exercise: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1071–1082. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Moreno, I.L.; Pastre, C.M.; Ferreira, C.; de Abreu, L.C.; Valenti, V.E.; Vanderlei, L.C.M. Effects of an isotonic beverage on autonomic regulation during and after exercise. J. Int. Soc. Sports Nutr. 2013, 10, 2. [Google Scholar] [CrossRef] [Green Version]
- Abellán-Aynés, O.; López-Plaza, D.; Alacid, F.; Naranjo-Orellana, J.; Manonelles, P. Recovery of Heart Rate Variability after Exercise under Hot Conditions: The Effect of Relative Humidity. Wilderness Environ. Med. 2019, 30, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Kaikkonen, P.; Nummela, A.; Rusko, H. Heart rate variability dynamics during early recovery after different endurance exercises. Eur. J. Appl. Physiol. 2007, 102, 79–86. [Google Scholar] [CrossRef]
- ESHRE Capri Workshop Group Hormones and cardiovascular health in women. Hum. Reprod. Updat. 2006, 12, 483–497. [CrossRef] [PubMed]
- Lerma, C.; Vallejo, M.; Urias, K.; Hermosillo, A.G.; Cárdenas, M. Differences in cardiac autonomic modulation between women and men. Arch. Cardiol. Mex. 2006, 76, 277–282. [Google Scholar] [PubMed]
- Huikuri, H.V.; Pikkujamsa, S.M.; Airaksinen, J.; Ikaheimo, M.J.; Rantala, A.O.; Kauma, H.; Lilja, M.; Kesaniemi, Y.A. Sex-Related Differences in Autonomic Modulation of Heart Rate in Middle-aged Subjects. Circulation 1996, 94, 122–125. [Google Scholar] [CrossRef]
- The International Clinical Trial Registry Platform (ICTRP) of the World Health Organization Has Accredited Two New Primary Registries. Available online: https://www.paho.org/hq/index.php?option=com_content&view=article&id=5488,2011-international-clinical-trial-registry-platform-ictrp&Itemid=820&lang=en (accessed on 14 October 2019).
- Bai, X.; Li, J.; Zhou, L.; Li, X. Influence of the menstrual cycle on nonlinear properties of heart rate variability in young women. Am. J. Physiol.-Heart Circ Physiol. 2009, 297, H765–H774. [Google Scholar] [CrossRef] [PubMed]
- Rzewnicki, R.; Vanden Auweele, Y.; De Bourdeaudhuij, I. Addressing overreporting on the International Physical Activity Questionnaire (IPAQ) telephone survey with a population sample. Public Health Nutr. 2003, 6, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Hnatkova, K.; Šišáková, M.; Smetana, P.; Toman, O.; Huster, K.M.; Novotný, T.; Schmidt, G.; Malik, M. Sex differences in heart rate responses to postural provocations. Int. J. Cardiol. 2019, 297, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Lohman, T.G.; Roche, A.F.; Martorelli, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1988. [Google Scholar]
- Brazilian Society of Cardiology; Brazilian Society of Hypertension; Brazilian Society of Nephrology. Brazilian guidelines on hypertension VI. J. Bras Nefrol. 2010, 95, 1–55. [Google Scholar]
- Benjamim, C.J.R.; Júnior, F.W.S.; de Figueirêdo, M.Í.L.S.; Benjamim, C.J.R.; Cavalcante, T.C.F.; da Silva, A.A.M.; Monteiro, L.R.L.; Santana, M.D.R.; Garner, D.M.; Valenti, V.E. Beetroot (Beta vulgaris L.) Extract Acutely Improves Heart Rate Variability Recovery Following Strength Exercise: A Randomized, Double-Blind, Placebo-Controlled Crossover Trial-Pilot Study. J. Am. Coll. Nutr. 2021, 40, 307–316. [Google Scholar] [CrossRef]
- Benjamim, C.J.R.; Monteiro, L.R.L.; Pontes, Y.M.M.; Silva, A.A.M.D.; Souza, T.K.M.; Valenti, V.E.; Garner, D.M.; Cavalcante, T.C.F. Caffeine slows heart rate autonomic recovery following strength exercise in healthy subjects. Rev. Port. Cardiol. 2021, 40, 399–406. [Google Scholar] [CrossRef]
- Tavares, B.S.; Vidigal, G.A.; Garner, D.M.; Raimundo, R.D.; de Abreu, L.C.; Valenti, V.E. Effects of guided breath exercise on complex behaviour of heart rate dynamics. Clin. Physiol. Funct. Imaging 2017, 37, 622–629. [Google Scholar] [CrossRef]
- Benjamim, C.J.R.; de Sousa Júnior, F.W.; Porto, A.A.; Rocha, É.M.B.; Santana, M.D.; Garner, D.M.; Valenti, V.E.; Júnior, C.R.B. Bitter Orange (Citrus aurantium L.) Intake Before Submaximal Aerobic Exercise Is Safe for Cardiovascular and Autonomic Systems in Healthy Males: A Randomized Trial. Front. Nutr. 2022, 9, 890388. [Google Scholar] [CrossRef] [PubMed]
- Niskanen, J.P.; Tarvainen, M.P.; Ranta-Aho, P.O.; Karjalainen, P.A. Software for advanced HRV analysis. Comput. Methods Programs. Biomed. 2004, 76, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.B.; Cornélissen, G.; Weydahl, A.; Schwartzkopff, O.; Katinas, G.; Otsuka, K.; Watanabe, Y.; Yano, S.; Mori, H.; Ichimaru, Y.; et al. Circadian heart rate and blood pressure variability considered for research and patient care. Int. J. Cardiol. 2003, 87, 9–28. [Google Scholar] [CrossRef]
- Fox, S.M., 3rd; Naughton, J.P.; Haskell, W.L. Physical activity and the prevention of coronary heart disease. Ann. Clin. Res. 1971, 3, 404–432. [Google Scholar] [CrossRef] [Green Version]
- Santana, M.D.R.; Kliszczewicz, B.; Vanderlei, F.M.; Monteiro, L.R.L.; Martiniano, E.C.; de Moraes, Y.M.; Mangueira, L.B.; Alcantara, G.C.; da Silva, J.R.A.; Benjamim, C.J.R.; et al. Autonomic responses induced by aerobic submaximal exercise in obese and overweight adolescents. Cardiol. Young 2019, 29, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Gonzaga, L.A.; Vanderlei, L.C.M.; Gomes, R.L.; Valenti, V.E. Caffeine affects autonomic control of heart rate and blood pressure recovery after aerobic exercise in young adults: A crossover study. Sci. Rep. 2017, 7, 14091. [Google Scholar] [CrossRef] [Green Version]
- Porto, A.A.; Valenti, V.E.; Amaral, J.A.T.D.; Benjamim, C.J.R.; Garner, D.M.; Ferreira, C. Energy Drink before Exercise Did Not Affect Autonomic Recovery Following Moderate Aerobic Exercise: A Crossover, Randomized and Controlled Trial. J. Am. Coll. Nutr. 2021, 40, 280–286. [Google Scholar] [CrossRef]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research-Recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [Green Version]
- Quintana, D.S.; Heathers, J.A. Considerations in the assessment of heart rate variability in biobehavioral research. Front. Psychol. 2014, 5, 805. [Google Scholar] [CrossRef] [Green Version]
- Johnson, V.E. Revised standards for statistical evidence. Proc. Natl. Acad. Sci. USA 2013, 110, 19313–19317. [Google Scholar] [CrossRef] [Green Version]
- Quintana, D.S. Statistical considerations for reporting and planning heart rate variability case-control studies. Psychophysiology 2017, 54, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Castro-Sepulveda, M.; Johannsen, N.; Astudillo, S.; Jorquera, C.; Álvarez, C.; Zbinden-Foncea, H.; Ramírez-Campillo, R. Effects of beer, non-alcoholic beer and water consumption before exercise on fluid and electrolyte homeostasis in athletes. Nutrients 2016, 8, 345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janszky, I.; Ericson, M.; Blom, M.; Georgiades, A.; Magnusson, J.O.; Alinagizadeh, H.; Ahnve, S. Wine drinking is associated with increased heart rate variability in women with coronary heart disease. Heart 2005, 91, 314–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svedahl, K.; MacIntosh, B.R. Anaerobic threshold: The concept and methods of measurement. Can. J. Appl. Physiol. 2003, 28, 299–323. [Google Scholar] [CrossRef] [Green Version]
- Koob, G.F. Alcoholism: Allostasis and beyond. Alcohol. Clin. Exp. Res. 2003, 27, 232–243. [Google Scholar] [CrossRef]
- Li, H.B.; Qin, D.N.; Cheng, K.; Su, Q.; Miao, Y.W.; Guo, J.; Zhang, M.; Zhu, G.Q.; Kang, Y.M. Central blockade of salusin β attenuates hypertension and hypothalamic inflammation in spontaneously hypertensive rats. Sci. Rep. 2015, 5, 11162. [Google Scholar] [CrossRef] [Green Version]
- Tjen-A-Looi, S.C.; Guo, Z.L.; Fu, L.W.; Longhurst, J.C. Paraventricular Nucleus Modulates Excitatory Cardiovascular Reflexes during Electroacupuncture. Sci. Rep. 2016, 6, 25910. [Google Scholar] [CrossRef] [Green Version]
- Wiklund, U.; Karlsson, M.; Oström, M.; Messner, T. Influence of energy drinks and alcohol on post-exercise heart rate recovery and heart rate variability. Clin. Physiol. Funct. Imaging 2009, 29, 74–80. [Google Scholar] [CrossRef]
- Sivasinprasasn, S.; Tanajak, P.; Pongkan, W.; Pratchayasakul, W.; Chattipakorn, S.C.; Chattipakorn, N. DPP-4 inhibitor and estrogen share similar efficacy against cardiac ischemic-reperfusion injury in obese-insulin resistant and estrogen-deprived female rats. Sci. Rep. 2017, 7, 44306. [Google Scholar] [CrossRef] [Green Version]
- Maayah, Z.H.; Levasseur, J.; Siva Piragasam, R.; Abdelhamid, G.; Dyck, J.R.; Fahlman, R.P.; Siraki, A.G.; El-Kadi, A.O. 2-Methoxyestradiol protects against pressure overload-induced left ventricular hypertrophy. Sci. Rep. 2018, 8, 2780. [Google Scholar] [CrossRef] [Green Version]
- Camps, G.; De Graaf, K.; Smeets, P.A.M. Men and women differ in gastric fluid retention and neural activation after consumption of carbonated beverages. J. Nutr. 2018, 148, 1976–1983. [Google Scholar] [CrossRef] [PubMed]
- Sekime, A.; Horikoshi, M.; Funakoshi, A.; Miyasaka, K. Sex difference in the effects of alcohol on gastric emptying in healthy volunteers: A study using the 13C breath test. Biomed. Res. 2013, 34, 275–280. [Google Scholar]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savin, W.M.; Davidson, D.M.; Haskell, W. Autonomic contribution to heart rate recovery from exercise in humans. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1982, 53, 1572–1575. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Men | Women | p-Value | Cohen’s d |
|---|---|---|---|---|
| Mass (kg) | 65.22 ± 7.65 [46.1–78.6] | 60.99 ± 8 [48.9–79] | 0.13 | - |
| Height (m) | 1.72 ± 0.06 [1.63–1.82] | 1.62 ± 0.06 [1.56–1.79] | <0.0001 | 1.67 |
| Age (years) | 20.94 ± 2.33 [18–26] | 22.67 ± 3.56 [19–32] | 0.13 | - |
| BMI (kg/m2) | 21.92 ± 2.68 [17.35–24.8] | 23.12 ± 1.95 [18.86–24.9] | 0.16 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santana, M.R.D.; Pontes, Y.M.d.M.; Benjamim, C.J.R.; Rodrigues, G.d.S.; Liberalino, G.A.; Mangueira, L.B.; Feitosa, M.E.; Leal, J.; Akimoto, A.; Garner, D.M.; et al. A Single Dose of Beer after Moderate Aerobic Exercise Did Not Affect the Cardiorespiratory and Autonomic Recovery in Young Men and Women: A Crossover, Randomized and Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 13330. https://doi.org/10.3390/ijerph192013330
Santana MRD, Pontes YMdM, Benjamim CJR, Rodrigues GdS, Liberalino GA, Mangueira LB, Feitosa ME, Leal J, Akimoto A, Garner DM, et al. A Single Dose of Beer after Moderate Aerobic Exercise Did Not Affect the Cardiorespiratory and Autonomic Recovery in Young Men and Women: A Crossover, Randomized and Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(20):13330. https://doi.org/10.3390/ijerph192013330
Chicago/Turabian StyleSantana, Milana R. Drumond, Yasmim M. de Moares Pontes, Cicero Jonas R. Benjamim, Guilherme da Silva Rodrigues, Gabriela A. Liberalino, Luana B. Mangueira, Maria E. Feitosa, Jessica Leal, Amanda Akimoto, David M. Garner, and et al. 2022. "A Single Dose of Beer after Moderate Aerobic Exercise Did Not Affect the Cardiorespiratory and Autonomic Recovery in Young Men and Women: A Crossover, Randomized and Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 20: 13330. https://doi.org/10.3390/ijerph192013330