
Contemplative Practices Behavior Is Positively Associated with Well-Being in Three Global Multi-Regional Stanford WELL for Life Cohorts
 ,
,  , , ,
, , ,  ,
, 
Abstract
:1. Introduction
1.1. Introducing Contemplative Practices
1.2. Contemplative Practices and Well-Being
1.3. Understanding Multiple Practices: Contemplative Practice Behavior
2. Materials and Methods
2.1. Study Setting and Design
2.2. Independent Variable
2.3. Outcome Measure (Well-Being and Its Nine Domains)
2.4. Test–Retest Reliability and Convergent Validity
2.5. Covariates
2.5.1. Physical Activity
2.5.2. Demographic Characteristics
2.6. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Descriptive Statistics for CPB, PA, and Well-Being
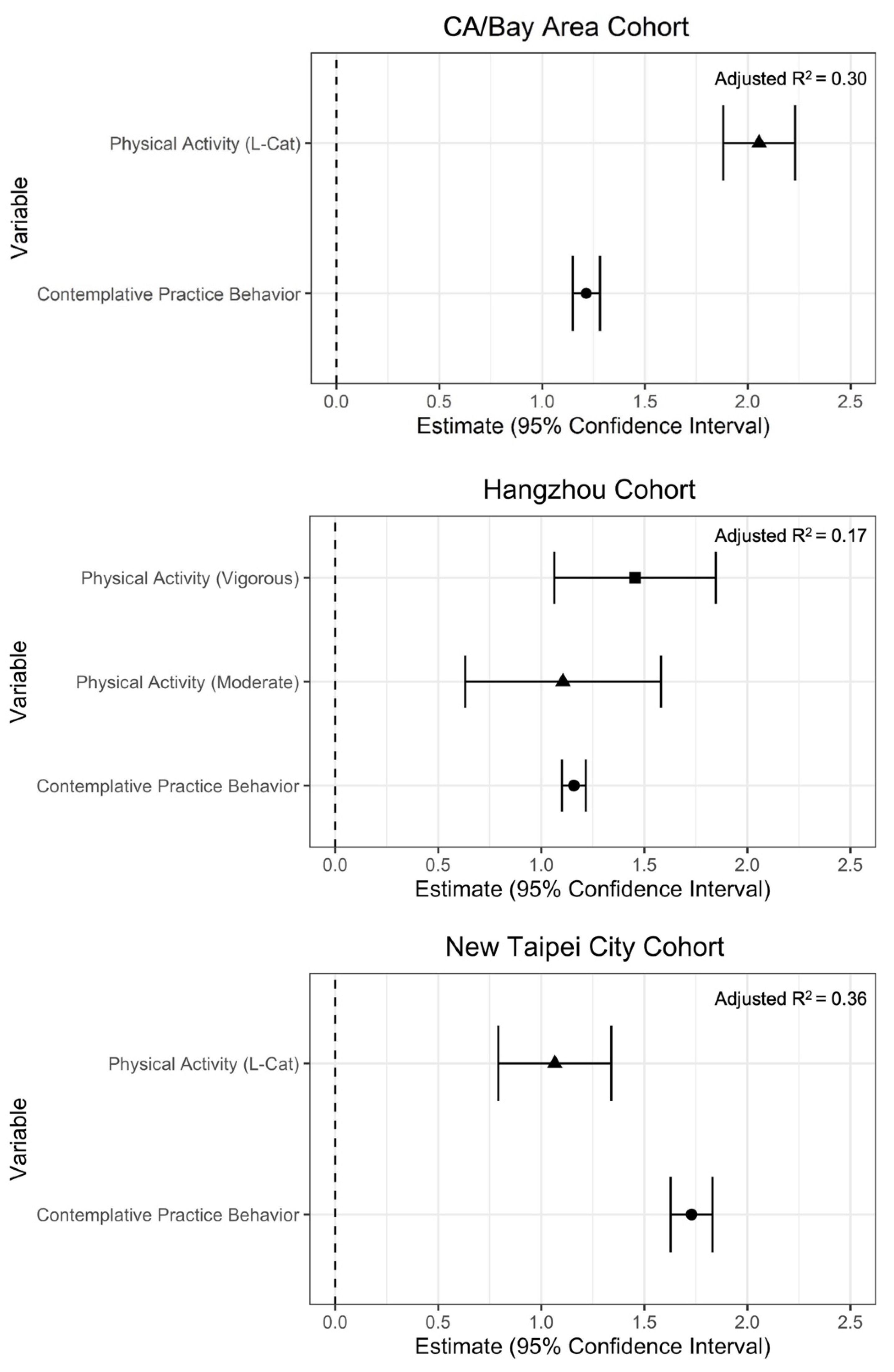
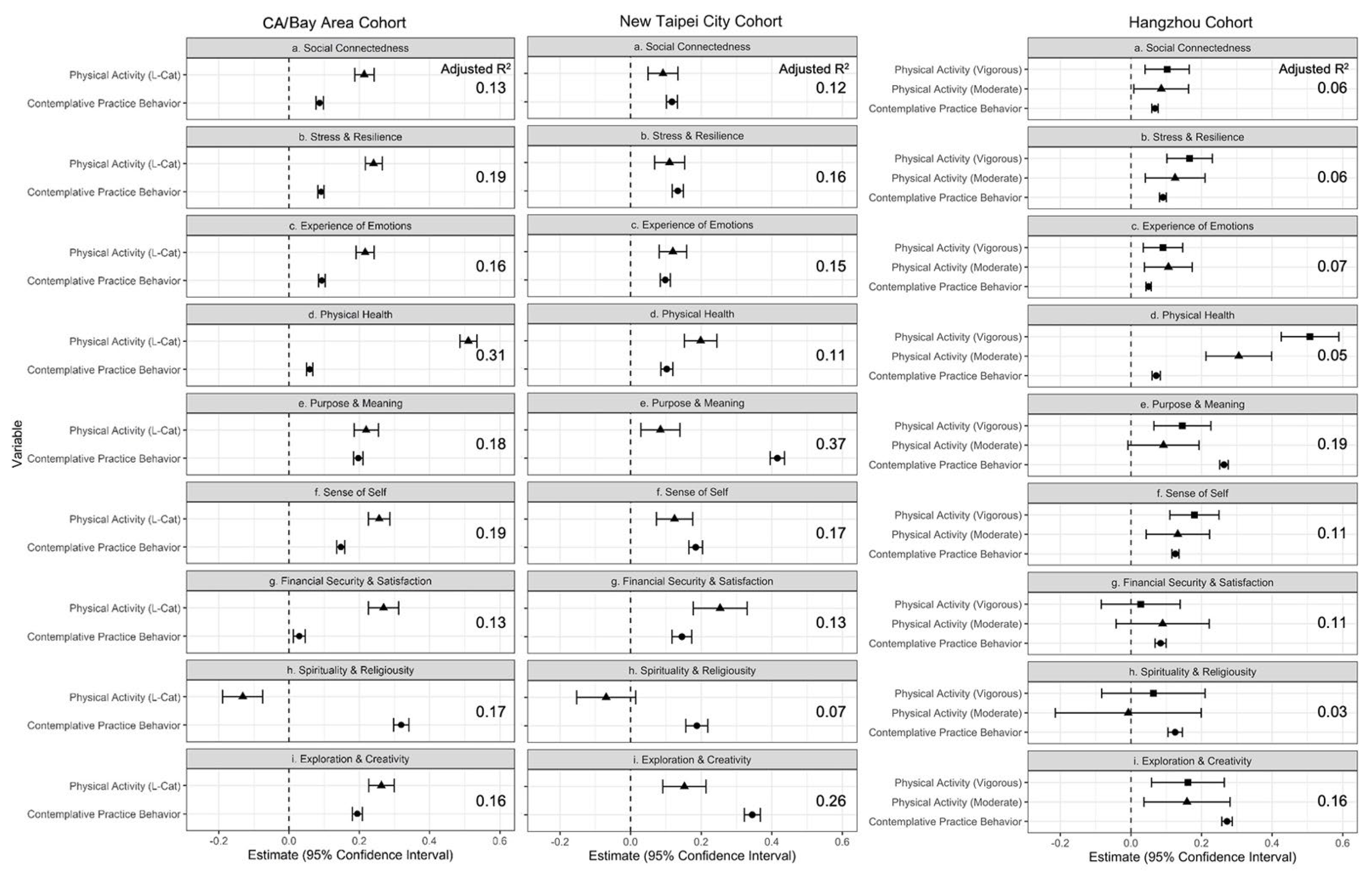
3.3. Contemplative Practice Behavior and Well-Being
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suvarna, B.; Suvarna, A.; Phillips, R.; Juster, R.-P.; McDermott, B.; Sarnyai, Z. Health risk behaviours and allostatic load: A systematic review. Neurosci. Biobehav. Rev. 2020, 108, 694–711. [Google Scholar] [CrossRef]
- Siegel, D.J. Mindsight: The New Science of Personal Transformation; Bantam Books: New York, NY, USA, 2010. [Google Scholar]
- Hoge, E.A.; Acabchuk, R.L.; Kimmel, H.; Moitra, E.; Britton, W.B.; Dumais, T.; Fulwiler, C. Emotion-related constructs engaged by mindfulness-based interventions: A systematic review and meta-analysis. Mindfulness 2021, 12, 1041–1062. [Google Scholar] [CrossRef] [PubMed]
- Sala, M.; Rochefort, C.; Lui, P.P.; Baldwin, A.S. Trait mindfulness and health behaviours: A meta-analysis. Health Psychol. Rev. 2020, 14, 345–393. [Google Scholar] [CrossRef] [PubMed]
- Goleman, D.; Davidson, R.J. Altered Traits: Science Reveals How Meditation Changes Your Mind, Brain, and Body; Avery: New York, NY, USA, 2021. [Google Scholar]
- Davidson, R.J. Mindfulness and more: Toward a science of human flourishing. Psychosom. Med. 2021, 83, 665. [Google Scholar] [CrossRef]
- Davidson, R.J.; Dahl, C.J. Varieties of Contemplative Practice. JAMA Psychiatry 2017, 74, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Fiske, E. Self-transcendence theory and contemplative practices. Holist. Nurs. Pract. 2019, 33, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Reed, P.G. Theory of self-transcendence. In Middle Range Theory for Nursing; Smith, M.J., Liehr, P.R., Eds.; Springer: New York, NY, USA, 2018; Volume 3, pp. 119–146. [Google Scholar]
- Reed, P.G. Unitary Human Beings: Theory and Research. In Patterns of Rogerian Knowing; Madrid, M., Ed.; National League for Nursing Press: New York, NY, USA, 1997; 15, pp. 187–196. ISBN 0-88737-688-6. [Google Scholar]
- Vago, D.R.; Silbersweig, D.A. Self-awareness, self-regulation, and self-transcendence (S-ART): A framework for understanding the neurobiological mechanisms of mindfulness. Front. Hum. Neurosci. 2012, 6, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coward, D.D.; Reed, P.G. Self-transcendence theory. In Nursing Theorists and Their Work; Alligood, M.R., Tomey, A.M., Eds.; Elsevier/Mosby: St. Louis, MO, USA, 2014; pp. 574–592. [Google Scholar]
- Seppälä, E.M.; Simon-Thomas, E.; Brown, S.L.; Worline, M.C.; Cameron, C.D.; Doty, J.R. (Eds.) The Oxford Handbook of Compassion Science; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- McEntee, R.; Bucko, A. New Monasticism: An Interspiritual Manifesto for Contemplative Living; Orbis Books: Maryknoll, NY, USA, 2015. [Google Scholar]
- Chrisinger, B.W.; Rich, T. Contemplation by Design: Leveraging the “Power of the Pause” on a Large University Campus Through Built and Social Environments. Front. Public Health 2020, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- DiPerna, D. Streams of Wisdom: An Advanced Guide to Integral Spirtual Development; Bright Alliance: San Francisco, CA, USA, 2017; Volume 1. [Google Scholar]
- Wilber, K. A Brief History of Everything; Shambhala Publications: Boston, MA, USA, 1996. [Google Scholar]
- Wilber, K.; Patten, T.; Leonard, A.; Morelli, M. Integral Life Practice: A 21st-Century Blueprint for Physical Health, Emotional Balance, Mental Clarity, and Spiritual Awakening; Shambhala Publications: Boston, MA, USA, 2008. [Google Scholar]
- Underhill, E. (Ed.) A Book of Contemplation: The Which Is Called the Cloud of Unknowing, in Which the Soul Is Oned with God; John M. Watkins: London, UK, 1912. [Google Scholar]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Don, B.P.; Van Cappellen, P.; Fredrickson, B.L. Understanding Engagement in and Affective Experiences During Physical Activity: The Role of Meditation Interventions. Psychosom. Med. 2021, 83, 592–601. [Google Scholar] [CrossRef] [PubMed]
- Sala, M.; Geary, B.; Baldwin, A.S. A mindfulness-based physical activity intervention: A randomized pilot study. Psychosom. Med. 2021, 83, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Strowger, M.; Kiken, L.G.; Ramcharran, K. Mindfulness meditation and physical activity: Evidence from 2012 National Health Interview Survey. Health Psychol. 2018, 37, 924. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.; Heerkens, Y.; Kuijer, W.; van der Heijden, B.; Engels, J. Effects of Mindfulness-Based Stress Reduction on employees’ mental health: A systematic review. PLoS ONE 2018, 13, e0191332. [Google Scholar] [CrossRef]
- Kirby, J.N.; Tellegen, C.L.; Steindl, S.R. A Meta-Analysis of Compassion-Based Interventions: Current State of Knowledge and Future Directions. Behav. Ther. 2017, 48, 778–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, B.A.; Shapiro, S.L. Mental balance and well-being: Building bridges between Buddhism and Western psychology. Am. Psychol. 2006, 61, 690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, S.B.; Riordan, K.M.; Sun, S.; Davidson, R.J. The empirical status of mindfulness-based interventions: A systematic review of 44 meta-analyses of randomized controlled trials. Perspect. Psychol. Sci. 2022, 17, 108–130. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822. [Google Scholar] [CrossRef] [Green Version]
- Chiesa, A.; Serretti, A. Mindfulness-Based Stress Reduction for Stress Management in Healthy People: A Review and Meta-Analysis. J. Altern. Complement. Med. 2009, 15, 593–600. [Google Scholar] [CrossRef] [Green Version]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Bishop, S.R.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.D.; Carmody, J.; Segal, Z.; Abbey, S.; Speca, M.; Devins, G. Mindfulness: A Proposed Operational Definition. Clin. Psychol. Sci. Pract. 2004, 11, 230–241. [Google Scholar] [CrossRef]
- Leyland, A.; Rowse, G.; Emerson, L.-M. Experimental Effects of Mindfulness Inductions on Self-Regulation: Systematic Review and Meta-Analysis. Emotion 2019, 19, 108–122. [Google Scholar] [CrossRef] [PubMed]
- MacCoon, D.G.; Imel, Z.E.; Rosenkranz, M.A.; Sheftel, J.G.; Weng, H.Y.; Sullivan, J.C.; Bonus, K.A.; Stoney, C.M.; Salomons, T.V.; Davidson, R.J. The validation of an active control intervention for Mindfulness Based Stress Reduction (MBSR). Behav. Res. Ther. 2012, 50, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kral, T.R.A.; Schuyler, B.S.; Mumford, J.A.; Rosenkranz, M.A.; Lutz, A.; Davidson, R.J. Impact of short- and long-term mindfulness meditation training on amygdala reactivity to emotional stimuli. NeuroImage 2018, 181, 301–313. [Google Scholar] [CrossRef]
- Jacobs, T.L.; Epel, E.S.; Lin, J.; Blackburn, E.H.; Wolkowitz, O.M.; Bridwell, D.A.; Zanesco, A.P.; Aichele, S.R.; Sahdra, B.K.; MacLean, K.A.; et al. Intensive meditation training, immune cell telomerase activity, and psychological mediators. Psychoneuroendocrinology 2011, 36, 664–681. [Google Scholar] [CrossRef] [PubMed]
- Younge, J.O.; Gotink, R.A.; Baena, C.P.; Roos-Hesselink, J.W.; Hunink, M.M. Mind–body practices for patients with cardiac disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 1385–1398. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Speca, M.; Faris, P.; Patel, K.D. One-year pre–post intervention follow-up of psychological, immune, endocrine and blood pressure outcomes of mindfulness-based stress reduction (MBSR) in breast and prostate cancer outpatients. Brain Behav. Immun. 2007, 21, 1038–1049. [Google Scholar] [CrossRef]
- Carlson, L.E.; Speca, M.; Patel, K.D.; Goodey, E. Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress and levels of cortisol dehydroepiandrosterone sulfate (DHEAS) and melatonin in breast and prostate cancer outpatients. Psychoneuroendocrinology 2004, 29, 448–474. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The Effect of Mindfulness-Based Therapy on Anxiety and Depression: A Meta-Analytic Review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef]
- Heaney, C.; Avery, E.; Rich, T.; Ahuja, N.; Winter, S.; Stanford WELL for Life Measures Work Group. Stanford WELL for Life: Learning What It Means to Be Well. Am. J. Health Promot. 2017, 31, 449–450. [Google Scholar]
- Min, Y.; Zhao, X.; Stafford, R.S.; Ma, X.; Chen, S.-H.; Gan, D.; Wei, C.; Huang, C.; Chen, L.; Gao, P.; et al. Cohort Profile: WELL Living Laboratory in China (WELL-China). Int. J. Epidemiol. 2021, 50, 1432–1443. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Strauss, C.; Crane, C.; Barnhofer, T.; Karl, A.; Cavanagh, K.; Kuyken, W. Examining the factor structure of the 39-item and 15-item versions of the Five Facet Mindfulness Questionnaire before and after mindfulness-based cognitive therapy for people with recurrent depression. Psychol. Assess. 2016, 28, 791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neff, K.D. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude Toward Oneself. Self Identity 2003, 2, 85–101. [Google Scholar] [CrossRef] [Green Version]
- Ooi, S.L.; Pak, S. The Landscape of Current Meditation Research: An Overview to the Special Issue on ’Health Benefits of Meditation’. OBM Integr. Complement. Med. 2019, 4, 033. [Google Scholar] [CrossRef] [Green Version]
- Seppälä, E.M.; Nitschke, J.B.; Tudorascu, D.L.; Hayes, A.; Goldstein, M.R.; Nguyen, D.T.; Perlman, D.; Davidsaon, R.J. Breathing-based meditation decreases posttraumatic stress disorder symptoms in US Military veterans: A randomized controlled longitudinal study. J. Trauma. Stress 2014, 27, 397–405. [Google Scholar] [CrossRef]
- Vieten, C.; Wahbeh, H.; Cahn, B.R.; MacLean, K.; Estrada, M.; Mills, P.; Murphy, M.; Wahbeh, H.; Cahn, B.R.; MacLean, K.; et al. Future directions in meditation research: Recommendations for expanding the field of contemplative science. PLoS ONE 2018, 13, e0205740. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [Green Version]
- Baer, R.A.; Smith, G.T.; Lykins, E.; Button, D.; Krietemeyer, J.; Sauer, S.; Walsh, E.; Duggam, D.; Williams, J.M.G. Construct validity of the five-facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment 2008, 15, 329–342. [Google Scholar] [CrossRef]
- Berkovich-Ohana, A.; Jennings, P.A.; Lavy, S. Contemplative Neuroscience, Self-Awareness, and Education. Prog. Brain Res. 2019, 244, 355–385. [Google Scholar]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The Neuroscience of Mindfulness Meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef]
- Lutz, J.; Herwig, U.; Opialla, S.; Hittmeyer, A.; Jäncke, L.; Rufer, M.; Grosse Holtforth, M.; Brühl, A.B. Mindfulness and Emotion Regulation—An FMRI Study. Soc. Cogn. Affect. Neurosci. 2014, 9, 776–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robins, C.J.; Keng, S.-L.; Ekblad, A.G.; Brantley, J.G. Effects of Mindfulness-Based Stress Reduction on Emotional Experience and Expression: A Randomized Controlled Trial. J. Clin. Psychol. 2012, 68, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Goldin, P.R.; Gross, J.J. Effects of Mindfulness-Based Stress Reduction (MBSR) on Emotion Regulation in Social Anxiety Disorder. Emotion 2010, 10, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, R.; Gullone, E.; Allen, N.B. Mindful Emotion Regulation: An Integrative Review. Clin. Psychol. Rev. 2009, 29, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Phillips, W.J.; Hine, D.W. Self-compassion, physical health, and health behaviour: A meta-analysis. Health Psychol. Rev. 2021, 15, 113–139. [Google Scholar] [CrossRef]
- Ferrari, M.; Hunt, C.; Harrysunker, A.; Abbott, M.J.; Beath, A.P.; Einstein, D.A. Self-compassion interventions and psychosocial outcomes: A meta-analysis of RCTs. Mindfulness 2019, 10, 1455–1473. [Google Scholar] [CrossRef]
- Luberto, C.M.; Shinday, N.; Song, R.; Philpotts, L.L.; Park, E.R.; Fricchione, G.L.; Yeh, G.Y. A systematic review and meta-analysis of the effects of meditation on empathy, compassion, and prosocial behaviors. Mindfulness 2018, 9, 708–724. [Google Scholar] [CrossRef]
- Strauss, C.; Taylor, B.L.; Gu, J.; Kuyken, W.; Baer, R.; Jones, F.; Cavanagh, K. What is compassion and how can we measure it? A review of definitions and measures. Clin. Psychol. Rev. 2016, 47, 15–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chrisinger, B.W.; Gustafson, J.A.; King, A.C.; Winter, S.J. Understanding Where We Are Well: Neighborhood-Level Social and Environmental Correlates of Well-Being in the Stanford Well for Life Study. Int. J. Environ. Res. Public Health 2019, 16, 1786. [Google Scholar] [CrossRef] [Green Version]
- Willis, G.; Schechter, S.; Whitaker, K. A Comparison of Cognitive Interviewing, Expert Review, and Behavior Coding: What Do They Tell Us? American Statistical Association: Alexandria, VA, USA, 1999. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; US Department of Health and Human Services: Washington, DC, USA, 2018; p. 779.
- Gillison, F.B.; Skevington, S.M.; Sato, A.; Standage, M.; Evangelidou, S. The effects of exercise interventions on quality of life in clinical and healthy populations; a meta-analysis. Soc. Sci. Med. 2009, 68, 1700–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paluska, S.A.; Schwenk, T.L. Physical Activity and Mental Health. Sport. Med. 2000, 29, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Kiernan, M.; Schoffman, D.E.; Lee, K.; Brown, S.D.; Fair, J.M.; Perri, M.G.; Haskell, W.L. The Stanford Leisure-Time Activity Categorical Item (L-Cat): A single categorical item sensitive to physical activity changes in overweight/obese women. Int. J. Obes. 2013, 37, 1597–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sport. Exerc. 2000, 32 (Suppl. S9), S498–S504. [Google Scholar] [CrossRef] [Green Version]
- Van Buuren, S. Flexible Imputation of Missing Data, 2nd ed.; Chapman and Hall: London, UK, 2018; Available online: https://stefvanbuuren.name/fimd/ (accessed on 16 April 2021).
- Kontopantelis, E.; White, I.R.; Sperrin, M.; Buchan, I. Outcome-sensitive multiple imputation: A simulation study. BMC Med. Res. Methodol. 2017, 17, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wulff, J.N.; Jeppesen, L.E. Multiple imputation by chained equations in praxis: Guidelines and review. Electron. J. Bus. Res. Methods 2017, 15, 41–56. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016; Available online: https://www.R-project.org/ (accessed on 6 September 2022).
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. Available online: https://econpapers.repec.org/article/jssjstsof/v_3a045_3ai03.htm (accessed on 10 November 2018). [CrossRef] [Green Version]
- Achepohl, G.; Heaney, C.; Rosas, L.G.; Moore, J.; Rich, T.; Winter, S.J. The Value of Contemplative Practices: A Mixed Methods Approach Exploring Associations between Resilience and Experiences of the COVID-19 Pandemic among Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 10224. [Google Scholar] [CrossRef]
- Chrisinger, B.W.; Rich, T.; Lounsbury, D.; Peng, K.; Zhang, J.; Heaney, C.A.; Lu, Y.; Hsing, A.W. Coping with the COVID-19 pandemic: Contemplative practice behaviors are associated with better mental health outcomes and compliance with Shelter-In-Place orders in a prospective cohort study. Prev. Med. Rep. 2021, 23, 101451. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.R. The influence of physical activity on mental well-being. Public Health Nutr. 1999, 2, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Ivandic, I.; Freeman, A.; Birner, U.; Nowak, D. A systematic review of brief mental health and well-being interventions in organizational settings. Scand. J. Work. Environ. Health 2017, 43, 99–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tudor-Locke, C.; Bassett, D.R. How Many Steps/Day Are Enough? Sport. Med. 2004, 34, 1–8. [Google Scholar] [CrossRef]
- Office of Disease Prevention and Health Promotion. Healthy People 2030 Framework; U.S. Department of Health and Human Services: Washington, DC, USA, 2020.
- Office of Disease Prevention and Health Promotion. Healthy People 2020 Framework; U.S. Department of Health and Human Services: Washington, DC, USA, 2010.
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System—Questionnaires. Available online: https://www.cdc.gov/brfss/questionnaires/index.htm (accessed on 17 August 2020).
- Centers for Disease Control and Prevention. (March 2019). Detailed Outline of Topics in the Redesigned National Health Interview Survey (NHIS): Sample Adult Questionnaire. Available online: https://www.cdc.gov/nchs/data/nhis/AdultNHISRedesignTopics201903.pdf (accessed on 17 August 2020).
- Navarro, A.M.; Voetsch, K.P.; Liburd, L.C.; Giles, H.W.; Collins, J.L. Charting the Future of Community Health Promotion: Recommendations. Natl. Expert Panel Community Health Promot. 2007, 4, 7. [Google Scholar]
- World Health Organization. Constitution of the World Health Organization.2005. Available online: http://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf?ua=1 (accessed on 12 November 2018).
- Schmidt, A.F.; Finan, C. Linear regression and the normality assumption. J. Clin. Epidemiol. 2018, 98, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Thibodeaux, N.; Rossano, M.J. Meditation and immune function: The impact of stress management on the immune system. OBM Integr. Complement. Med. 2018, 3, 032. [Google Scholar] [CrossRef]
- Gamaiunova, L.; Brandt, P.-Y.; Bondolfi, G.; Kliegel, M. Exploration of psychological mechanisms of the reduced stress response in long-term meditation practitioners. Psychoneuroendocrinology 2019, 104, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Bostanov, V.; Ohlrogge, L.; Britz, R.; Hautzinger, M.; Kotchoubey, B. Measuring Mindfulness: A Psychophysiological Approach. Front. Hum. Neurosci. 2018, 12, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, F.; Nash, J.; Parim, N.; Cohen, B.H. Does the MRI/fMRI Procedure Itself Confound the Results of Meditation Research? An Evaluation of Subjective and Neurophysiological Measures of TM Practitioners in a Simulated MRI Environment. Front. Psychol. 2020, 11, 728. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Domain | Definition | Example Items | Number of Items |
|---|---|---|---|
| Social Connectedness | Positive or negative relationships with others and how they influence your well-being. | During the last two weeks, how often did you feel …
| 13 |
| Stress and Resilience | Stress: Feelings of overload and an inability to balance or manage tasks Resilience: Ability to adapt to change and bounce back after hardship. |
| 14 |
| Experience of Emotions | How often you experience both pleasant and unpleasant emotions. | During the last two weeks, how often did you feel
| 11 |
| Physical Health | Perception of your own health status, i.e., energy levels, ability to resist illness, physical fitness, and experience of pain. |
| 4 |
| Purpose and Meaning | Having a sense that aspects of your life provide purpose and meaning, i.e., goals, dreams, and being part of something larger than yourself. | How often does your daily life include experiences that give your life
| 2 |
| Sense of Self | The extent to which you feel you know yourself, can express your true self, have self-confidence, and feel good about who you are. | During the last two weeks, how often did you feel
| 5 |
| Financial Security and Satisfaction | Your perception of having enough money to meet your needs. |
| 11 |
| Spirituality and Religiosity | The extent to which spiritual and religious beliefs, practices, communities, and traditions are important in your life. |
| 1 |
| Exploration and Creativity | Having opportunities to grow as a person and to explore new experiences and ways of thinking. |
| 1 |
| CA/Bay Area 2 (n = 6442) | Hangzhou (n = 10,268) | New Taipei City (n = 3033) | |
|---|---|---|---|
| Age, mean (SD) | 41.4 (17.2) | 53.2 (14.1) | 54.4 (11.5) |
| Gender 3 | |||
| Female | 4586 (71.2) | 6187 (60.3) | 2064 (68.1) |
| Male | 1754 (27.2) | 4081 (39.7) | 969 (31.9) |
| Missing | 28 (0.4) | 0 (0.0) | 0 (0.0) |
| Educational attainment | |||
| High school or less | 819 (12.7) | 7499 (73.0) | 1593 (52.5) |
| Some college | 1221 (19.0) | 1255 (12.2) | |
| Bachelor’s degree 4 | 2084 (32.4) | 1208 (11.8) | 1173 (38.7) |
| Post-graduate/professional degree | 2273 (35.3) | NA | 264 (8.7) |
| Missing | 45 (0.7) | 306 (3.0) | 3 (0.1) |
| Employment status | |||
| Working | 4356 (67.6) | 3036 (29.6) | 1627 (53.6) |
| Not Working | 539 (8.4) | 2171 (21.1) | 507 (16.7) |
| Retired | 472 (7.3) | 4723 (46.0) | 835 (27.5) |
| Student | 1047 (16.3) | 32 (0.3) | 13 (0.4) |
| Missing | 28 (0.4) | 306 (3.0) | 51 (1.7) |
| Marital status | |||
| Married or cohabiting | 2758 (42.8) | 8748 (85.2) | 2293 (75.6) |
| Single | 2606 (40.5) | 555 (5.4) | 407 (13.4) |
| Other | 1047 (16.3) | 659 (6.4) | 329 (10.8) |
| Missing | 31 (0.5) | 306 (3.0) | 4 (0.1) |
| CA/Bay Area (n = 6442) | Hangzhou (n = 10,268) | New Taipei City (n = 3033) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Mean | sd | n Missing | % missing | Mean | sd | n Missing | % Missing | Mean | sd | n Missing | % Missing |
| Contemplative Practice Behavior (CPB) | 8.20 | 3.72 | 100 | 1.55 | 8.90 | 2.95 | 361 | 3.50 | 9.20 | 3.21 | 3 | 0.10 |
| 2.20 | 1.17 | 68 | 1.06 | 2.30 | 1.02 | 360 | 3.50 | 2.60 | 0.94 | 1 | 0.03 |
| 1.80 | 1.21 | 70 | 1.09 | 1.90 | 0.99 | 361 | 3.50 | 2.10 | 1.05 | 0 | 0.00 |
| 1.90 | 1.08 | 66 | 1.02 | 2.30 | 0.90 | 360 | 3.50 | 2.20 | 0.98 | 1 | 0.03 |
| 2.40 | 1.06 | 69 | 1.07 | 2.30 | 0.91 | 360 | 3.50 | 2.30 | 0.93 | 1 | 0.03 |
| Physical activity (L-Cat) | 3.50 | 1.45 | 92 | 1.43 | 2.60 | 1.23 | 60 | 1.98 | ||||
| Physical activity (IPAQ) 2 | 6.10 | 4.26 | 1201 | 11.70 | ||||||||
| WELL overall score | 59.10 | 11.96 | 147 | 2.28 | 55.90 | 9.16 | 360 | 3.50 | 55.30 | 11.03 | 10 | 0.33 |
Domain-specific scores
| 5.90 | 1.58 | 36 | 0.56 | 6.70 | 1.11 | 354 | 3.40 | 6.50 | 1.35 | 5 | 0.17 |
| 6.90 | 2.23 | 71 | 1.10 | 5.00 | 2.29 | 360 | 3.50 | 5.30 | 2.32 | 1 | 0.03 |
| 7.70 | 2.62 | 75 | 1.16 | 7.00 | 2.39 | 360 | 3.50 | 6.40 | 2.61 | 0 | 0.00 |
| 6.80 | 1.61 | 27 | 0.42 | 6.20 | 1.55 | 332 | 3.20 | 6.10 | 1.58 | 0 | 0.00 |
| 6.80 | 2.15 | 88 | 1.37 | 6.30 | 1.81 | 360 | 3.50 | 5.90 | 2.23 | 1 | 0.03 |
| 4.70 | 3.58 | 57 | 0.88 | 3.70 | 3.04 | 358 | 3.50 | 4.70 | 2.82 | 0 | 0.00 |
| 6.70 | 1.67 | 41 | 0.64 | 7.30 | 1.21 | 354 | 3.40 | 7.00 | 1.44 | 1 | 0.03 |
| 6.30 | 1.50 | 35 | 0.54 | 6.60 | 1.34 | 350 | 3.40 | 6.30 | 1.49 | 5 | 0.17 |
| 7.30 | 1.89 | 51 | 0.79 | 7.20 | 1.51 | 358 | 3.50 | 7.20 | 1.84 | 1 | 0.03 |
| Cohort | Estimate | Std. Error | Lower CI | Upper CI | |
|---|---|---|---|---|---|
| Contemplative Practice Behavior | CA/Bay Area | 1.22 | 0.03 | 1.15 | 1.28 |
| New Taipei City | 1.73 | 0.05 | 1.63 | 1.83 | |
| Hangzhou | 1.16 | 0.03 | 1.10 | 1.22 | |
| Physical Activity 1 | CA/Bay Area | 2.06 | 0.09 | 1.88 | 2.23 |
| New Taipei City | 1.07 | 0.14 | 0.79 | 1.34 | |
| Hangzhou Vigorous | 1.45 | 0.20 | 1.06 | 1.85 | |
| Hangzhou Moderate | 1.11 | 0.24 | 0.63 | 1.58 |
| Model 1 | Model 2 | Model 3 | |
|---|---|---|---|
| Domain | Demographic Covariates | Demographic Covariates + PA 1 | Demographic Covariates + PA 1 + CPB |
| CA/Bay Area | Adj R2(95% CI) | Adj R2(95% CI), p-value | Adj R2(95% CI), p-value |
| WELL overall score | 0.09 (0.08–0.1) | 0.16 (0.15–0.18), <0.001 | 0.30 (0.29–0.32), <0.001 |
| Experience of Emotions | 0.07 (0.06–0.08) | 0.11 (0.1–0.13), <0.001 | 0.16 (0.14–0.18), <0.001 |
| Exploration and Creativity | 0.03 (0.02–0.03) | 0.06 (0.05–0.08), <0.001 | 0.16 (0.15–0.18), <0.001 |
| Financial Sec. and Satisfaction | 0.11 (0.09–0.12) | 0.13 (0.11–0.14), <0.001 | 0.13 (0.11–0.15), <0.001 |
| Physical Health | 0.08 (0.07–0.09) | 0.29 (0.27–0.31), <0.001 | 0.31 (0.29–0.33), <0.001 |
| Purpose and Meaning | 0.04 (0.03–0.05) | 0.07 (0.06–0.08), <0.001 | 0.18 (0.16–0.2), <0.001 |
| Sense of Self | 0.06 (0.05–0.07) | 0.11 (0.09–0.12), <0.001 | 0.19 (0.17–0.21), <0.001 |
| Social Connectedness | 0.06 (0.05–0.07) | 0.1 (0.08–0.11), <0.001 | 0.13 (0.12–0.15), <0.001 |
| Spirituality and Religiosity | 0.06 (0.05–0.08) | 0.06 (0.05–0.08), 0.05 | 0.17 (0.16–0.19), <0.001 |
| Stress and Resilience | 0.08 (0.07–0.09) | 0.14 (0.13–0.16), <0.001 | 0.19 (0.17–0.21), <0.001 |
| Hangzhou | Adj R2 (95% CI) | Adj R2 (95% CI), p-val. | Adj R2 (95% CI), p-val. |
| WELL overall score | 0.03 (0.02–0.03) | 0.04 (0.03–0.04), <0.001 | 0.17 (0.16–0.19), <0.001 |
| Experience of Emotions | 0.05 (0.04–0.06) | 0.05 (0.04–0.06), <0.001 | 0.07 (0.06–0.08), <0.001 |
| Exploration and Creativity | 0.04 (0.03–0.05) | 0.04 (0.03–0.05), <0.001 | 0.16 (0.15–0.17), <0.001 |
| Financial Sec. and Satisfaction | 0.1 (0.09–0.12) | 0.1 (0.09–0.12), 0.212 | 0.11 (0.1–0.13), <0.001 |
| Physical Health | 0.01 (0.01–0.02) | 0.03 (0.02–0.04), <0.001 | 0.05 (0.04–0.06), <0.001 |
| Purpose and Meaning | 0.01 (0.01–0.01) | 0.01 (0.01–0.02), <0.001 | 0.19 (0.18–0.21), <0.001 |
| Sense of Self | 0.05 (0.04–0.06) | 0.06 (0.05–0.07), <0.001 | 0.11 (0.1–0.12), <0.001 |
| Social Connectedness | 0.04 (0.03–0.04) | 0.04 (0.03–0.05), <0.001 | 0.06 (0.05–0.07), <0.001 |
| Spirituality and Religiosity | 0.02 (0.01–0.02) | 0.02 (0.01–0.02), 0.312 | 0.03 (0.03–0.04), <0.001 |
| Stress and Resilience | 0.02 (0.01–0.02) | 0.02 (0.02–0.03), <0.001 | 0.06 (0.05–0.07), <0.001 |
| New Taipei City | Adj R2(95% CI) | Adj R2(95% CI), p-val. | Adj R2(95% CI), p-val. |
| WELL overall score | 0.08 (0.06–0.1) | 0.12 (0.1–0.14), <0.001 | 0.36 (0.33–0.38), <0.001 |
| Experience of Emotions | 0.08 (0.06–0.1) | 0.1 (0.08–0.12), <0.001 | 0.15 (0.13–0.18), <0.001 |
| Exploration and Creativity | 0.03 (0.02–0.04) | 0.05 (0.04–0.07), <0.001 | 0.26 (0.24–0.29), <0.001 |
| Financial Sec. and Satisfaction | 0.08 (0.06–0.1) | 0.1 (0.08–0.12), <0.001 | 0.13 (0.11–0.16), <0.001 |
| Physical Health | 0.04 (0.02–0.05) | 0.07 (0.05–0.09), <0.001 | 0.11 (0.09–0.13), <0.001 |
| Purpose and Meaning | 0.02 (0.01–0.03) | 0.04 (0.02–0.05), <0.001 | 0.37 (0.35–0.4), <0.001 |
| Sense of Self | 0.06 (0.04–0.08) | 0.07 (0.06–0.09), <0.001 | 0.17 (0.15–0.2), <0.001 |
| Social Connectedness | 0.05 (0.03–0.06) | 0.06 (0.05–0.08), <0.001 | 0.12 (0.1–0.15), <0.001 |
| Spirituality and Religiosity | 0.03 (0.02–0.04) | 0.03 (0.02–0.04), 0.826 | 0.07 (0.05–0.09), <0.001 |
| Stress and Resilience | 0.07 (0.05–0.09) | 0.09 (0.07–0.11), <0.001 | 0.16 (0.14–0.19), <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rich, T.; Chrisinger, B.W.; Kaimal, R.; Winter, S.J.; Hedlin, H.; Min, Y.; Zhao, X.; Zhu, S.; You, S.-L.; Sun, C.-A.; et al. Contemplative Practices Behavior Is Positively Associated with Well-Being in Three Global Multi-Regional Stanford WELL for Life Cohorts. Int. J. Environ. Res. Public Health 2022, 19, 13485. https://doi.org/10.3390/ijerph192013485
Rich T, Chrisinger BW, Kaimal R, Winter SJ, Hedlin H, Min Y, Zhao X, Zhu S, You S-L, Sun C-A, et al. Contemplative Practices Behavior Is Positively Associated with Well-Being in Three Global Multi-Regional Stanford WELL for Life Cohorts. International Journal of Environmental Research and Public Health. 2022; 19(20):13485. https://doi.org/10.3390/ijerph192013485
Chicago/Turabian StyleRich, Tia, Benjamin W. Chrisinger, Rajani Kaimal, Sandra J. Winter, Haley Hedlin, Yan Min, Xueyin Zhao, Shankuan Zhu, San-Lin You, Chien-An Sun, and et al. 2022. "Contemplative Practices Behavior Is Positively Associated with Well-Being in Three Global Multi-Regional Stanford WELL for Life Cohorts" International Journal of Environmental Research and Public Health 19, no. 20: 13485. https://doi.org/10.3390/ijerph192013485
APA StyleRich, T., Chrisinger, B. W., Kaimal, R., Winter, S. J., Hedlin, H., Min, Y., Zhao, X., Zhu, S., You, S.-L., Sun, C.-A., Lin, J.-T., Hsing, A. W., & Heaney, C. (2022). Contemplative Practices Behavior Is Positively Associated with Well-Being in Three Global Multi-Regional Stanford WELL for Life Cohorts. International Journal of Environmental Research and Public Health, 19(20), 13485. https://doi.org/10.3390/ijerph192013485