
The Causes and Role of Antinatalism in Poland in the Context of Climate Change, Obstetric Care, and Mental Health

 ,
,  , , , , ,
, , , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Antinatalism and Pronatalism Definition
2.3. Measurement Tools
2.4. Data Division
2.5. Statistical Analysis
3. Results
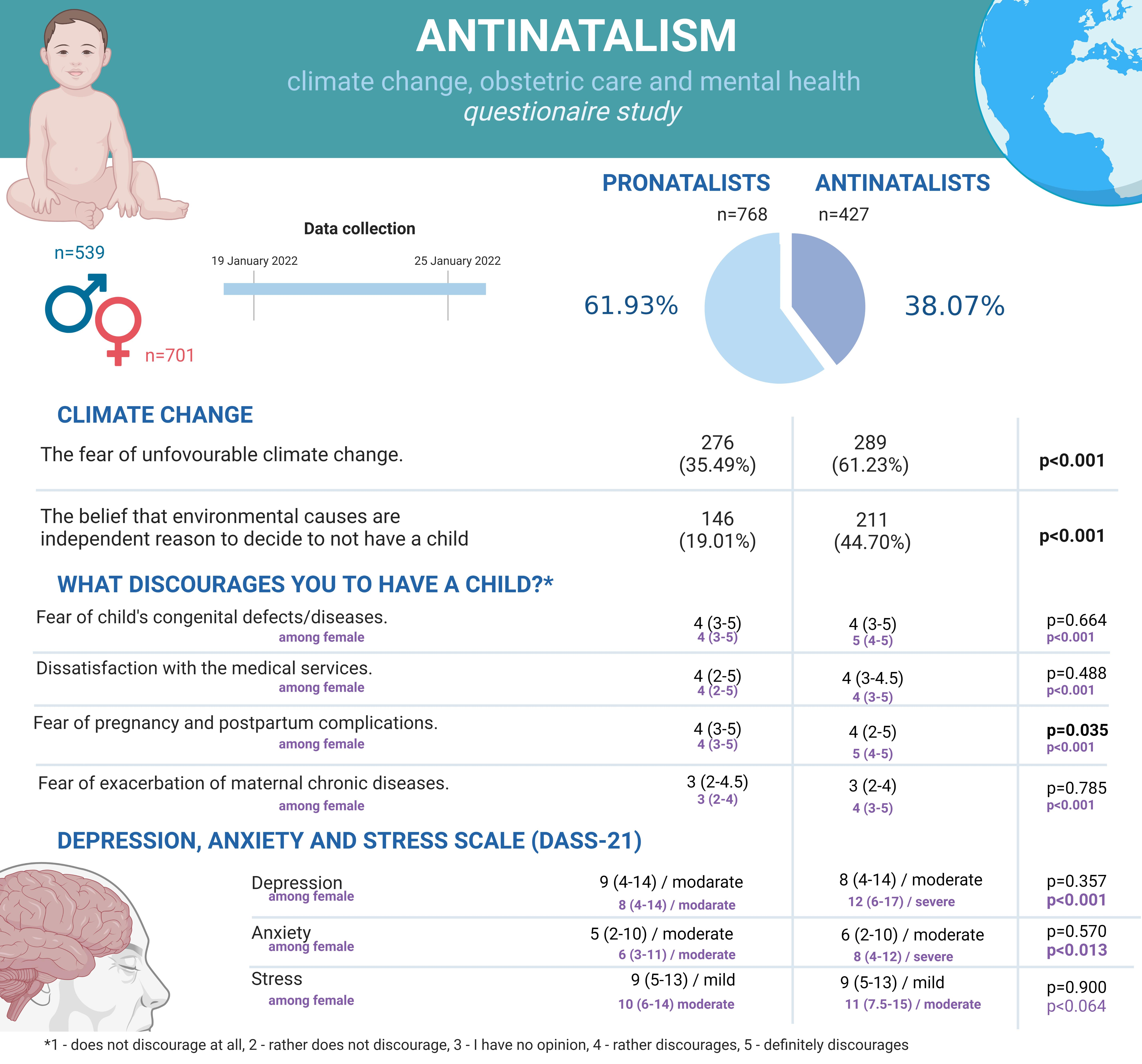
3.1. Study Group
3.2. Willingness to Have a Child
3.3. Factors Discouraging from Having a Child
3.4. The Influence of Climate Changes on Willingness to Have a Child—Environmental Antinatalism
3.5. Analysis of Facilitating Factors and Barriers to the Desire to Have a Child
4. Discussion
5. Advantages and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ashburn-Nardo, L. Parenthood as a Moral Imperative? Moral Outrage and the Stigmatization of Voluntarily Childfree Women and Men. Sex Roles 2017, 76, 393–401. [Google Scholar] [CrossRef]
- Harbison, S.F.; Robinson, W.C. Policy Implications of the Next World Demographic Transition. Stud. Fam. Plan. 2002, 33, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Brown, F.L.; Keefer, L.A. Anti-Natalism from an Evolutionary Psychological Perspective. Evol. Psychol. Sci. 2020, 6, 283–291. [Google Scholar] [CrossRef]
- Benatar, D. The Misanthropic Argument for Anti-Natalism. In Permissible Progeny? The Morality of Procreation and Parenting; UOP, Oxford Academic: New York, NY, USA, 2015; pp. 34–64. [Google Scholar] [CrossRef]
- Wiejska Droga Do Ginekologa—Najwyższa Izba Kontroli. Available online: https://www.nik.gov.pl/aktualnosci/wiejska-droga-do-ginekologa.html (accessed on 22 August 2022).
- Polska Ma Najmniej Lekarzy w Całej Unii Europejskiej—Puls Medycyny—Pulsmedycyny.Pl. Available online: https://pulsmedycyny.pl/polska-ma-najmniej-lekarzy-w-calej-unii-europejskiej-977230 (accessed on 22 August 2022).
- Kopacz, J. Niedobór Talentów w Branży Medycznej. Menedżer Zdrowia 2019, 2019, 93–95. [Google Scholar]
- Czy Medycy Uciekają z Kraju?—Menedżer Zdrowia—Termedia. Available online: https://www.termedia.pl/mz/Czy-medycy-uciekaja-z-kraju-,47293.html (accessed on 22 August 2022).
- Melender, H.L. Experiences of Fears Associated with Pregnancy and Childbirth: A Study of 329 Pregnant Women. Birth 2002, 29, 101–111. [Google Scholar] [CrossRef]
- Marin, M.F.; Lord, C.; Andrews, J.; Juster, R.P.; Sindi, S.; Arsenault-Lapierre, G.; Fiocco, A.J.; Lupien, S.J. Chronic Stress, Cognitive Functioning and Mental Health. Neurobiol. Learn. Mem. 2011, 96, 583–595. [Google Scholar] [CrossRef]
- Charlson, F.; Ali, S.; Benmarhnia, T.; Pearl, M.; Massazza, A.; Augustinavicius, J.; Scott, J.G. Climate Change and Mental Health: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 4486. [Google Scholar] [CrossRef] [PubMed]
- Ventriglio, A.; Bellomo, A.; di Gioia, I.; di Sabatino, D.; Favale, D.; de Berardis, D.; Cianconi, P. Environmental Pollution and Mental Health: A Narrative Review of Literature. CNS Spectr. 2021, 26, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Parenthood and Procreation (Stanford Encyclopedia of Philosophy). Available online: https://plato.stanford.edu/entries/parenthood/ (accessed on 22 August 2022).
- Stocker, T.F.; Qin, D.; Plattner, G.-K.; Tignor, M.M.B.; Allen, S.K.; Boschung, J.; Nauels, A.; Xia, Y.; Bex, V.; Midgley, P.M. IPCC, 2013: Climate Change 2013: The Physical Science Basis. Contribution of Working Group I to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Available online: https://www.ipcc.ch/site/assets/uploads/2018/02/WG1AR5_all_final.pdf (accessed on 22 August 2022).
- Hales, S.; Kovats, S.; Lloyd, S.; Campbell-Lendrum, D. Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s. World Health Organization. 2014. Available online: https://apps.who.int/iris/handle/10665/134014 (accessed on 22 August 2022).
- Jegasothy, R.; Sengupta, P.; Dutta, S.; Jeganathan, R. Climate Change and Declining Fertility Rate in Malaysia: The Possible Connexions. J. Basic Clin. Physiol. Pharmacol. 2021, 32, 911–924. [Google Scholar] [CrossRef]
- Główny Urząd Statystyczny/Obszary Tematyczne/Ludność/Ludność/Struktura Ludności. Available online: https://stat.gov.pl/obszary-tematyczne/ludnosc/ludnosc/struktura-ludnosci,16,1.html (accessed on 28 September 2022).
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and Behaviors towards SARS-CoV-2 Vaccination among Healthcare Workers: A Cross-Sectional Study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef]
- Cronbach’s Alpha Calculate Online | Statistics Calculator. Available online: https://datatab.net/statistics-calculator/reliability-analysis/cronbachs-alpha-calculator (accessed on 22 August 2022).
- Rybin’ska, A.; Philip Morgan, S. Childless Expectations and Childlessness Over the Life Course. Soc. Forces 2019, 97, 1571. [Google Scholar] [CrossRef]
- Neal, Z.P.; Neal, J.W. Prevalence, Age of Decision, and Interpersonal Warmth Judgements of Childfree Adults. Sci. Rep. 2022, 12, 11907. [Google Scholar] [CrossRef]
- Holroyd, E.; Chan, K.-L.; Tchounwou, P.B.; Gouni, O.; Jaraši, G.; Unait, E.-F.; Akik, B.K.; Holopainen, A.; Calleja-Agius, J. Childlessness: Concept Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1464. [Google Scholar] [CrossRef]
- 3M State of Science Index Survey | Explore the Data & Results. Available online: https://www.3m.com/3M/en_US/state-of-science-index-survey/interactive-3m-state-of-science-survey/ (accessed on 22 August 2022).
- Climate Change—Lipiec 2021—Eurobarometer Survey. Available online: https://europa.eu/eurobarometer/surveys/detail/2273 (accessed on 22 August 2022).
- Siña, M.; Wood, R.C.; Saldarriaga, E.; Lawler, J.; Zunt, J.; Garcia, P.; Cárcamo, C. Understanding Perceptions of Climate Change, Priorities, and Decision-Making among Municipalities in Lima, Peru to Better Inform Adaptation and Mitigation Planning. PLoS ONE 2016, 11, e0147201. [Google Scholar] [CrossRef]
- Smith, N.; Leiserowitz, A. The Role of Emotion in Global Warming Policy Support and Opposition. Risk Anal. 2014, 34, 937. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.E. Psychometric Properties of the Climate Change Worry Scale. Int. J. Environ. Res. Public Health 2021, 18, 494. [Google Scholar] [CrossRef]
- Searle, K.; Gow, K. Do Concerns about Climate Change Lead to Distress. Int. J. Clim. Chang. Strateg. Manag. 2010, 2, 362–379. [Google Scholar] [CrossRef]
- Rodríguez-Cruz, L.A.; Niles, M.T. Awareness of Climate Change’s Impacts and Motivation to Adapt Are Not Enough to Drive Action: A Look of Puerto Rican Farmers after Hurricane Maria. PLoS ONE 2021, 16, e0244512. [Google Scholar] [CrossRef]
- di Giusto, B.; Lavallee, J.P.; Yu, T.Y. Towards an East Asian Model of Climate Change Awareness: A Questionnaire Study among University Students in Taiwan. PLoS ONE 2018, 13, e0206298. [Google Scholar] [CrossRef]
- Gifford, R. The Dragons of Inaction: Psychological Barriers That Limit Climate Change Mitigation and Adaptation. Am. Psychol. 2011, 66, 290–302. [Google Scholar] [CrossRef]
- Grundy, E.; van den Broek, T.; Keenan, K. Number of Children, Partnership Status, and Later-Life Depression in Eastern and Western Europe. J. Gerontol. Ser. B 2019, 74, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Bonsang, E.; Skirbekk, V. Does Childbearing Affect Cognitive Health in Later Life? Evidence From an Instrumental Variable Approach. Demography 2022, 59, 975–994. [Google Scholar] [CrossRef]
- Pregnancy Mortality Surveillance System | Maternal and Infant Health | CDC. Available online: https://www.cdc.gov/reproductivehealth/maternal-mortality/pregnancy-mortality-surveillance-system.htm (accessed on 22 August 2022).
- Egelioğlu Cetişli, N.; Denizci Zirek, Z.Y.; Bakılan Abalı, F. Childbirth and Postpartum Period Fear in Pregnant Women and the Affecting Factors. Aquichan 2016, 16, 32–42. [Google Scholar] [CrossRef]
- Glinianaia, S.V.; Tennant, P.W.G.; Rankin, J. Risk Estimates of Recurrent Congenital Anomalies in the UK: A Population-Based Register Study. BMC Med. 2017, 15, 20. [Google Scholar] [CrossRef] [Green Version]
- Nayeri, N.D.; Roddehghan, Z.; Mahmoodi, F.; Mahmoodi, P. Being Parent of a Child with Congenital Heart Disease, What Does It Mean? A Qualitative Research. BMC Psychol. 2021, 9, 33. [Google Scholar] [CrossRef]
- Nicolaides, K.H. Screening for Chromosomal Defects. Ultrasound Obstet. Gynecol. 2003, 21, 313–321. [Google Scholar] [CrossRef]
- Amarin, V.N.; Akasheh, H.F. Advanced Maternal Age and Pregnancy Outcome—PubMed. East Mediterr. Health J. 2001, 646–651. [Google Scholar] [CrossRef]
- Statistics Poland/Topics/Statistical Yearbooks/Statistical Yearbooks/Demographic Yearbook of Poland. 2021. Available online: https://stat.gov.pl/en/topics/statistical-yearbooks/statistical-yearbooks/demographic-yearbook-of-poland-2021,3,15.html (accessed on 22 August 2022).
- Nybo Andersen, A.M.; Wohlfahrt, J.; Christens, P.; Olsen, J.; Melbye, M. Maternal Age and Fetal Loss: Population Based Register Linkage Study. BMJ 2000, 320, 1708–1712. [Google Scholar] [CrossRef] [Green Version]
- Brickner Rothenberg, P.; Varga, P.E. The Relationship between Age of Mother and Child Health and Development. Am. J. Public Health 1981, 71, 810–817. [Google Scholar] [CrossRef]
- Pinheiro, R.L.; Areia, A.L.; Pinto, A.M.; Donato, H. Advanced Maternal Age: Adverse Outcomes of Pregnancy, A Meta-Analysis. Acta Med. Port. 2019, 32, 219–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalugoda, Y.; Kuppa, J.; Phung, H.; Rutherford, S.; Phung, D. Effect of Elevated Ambient Temperature on Maternal, Foetal, and Neonatal Outcomes: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 1771. [Google Scholar] [CrossRef] [PubMed]
- Strzelecka, I.; Biedrzycka, M.; Karuga, F.F.; Szmyd, B.; Batarowicz, K.; Respondek-Liberska, M. Seasonality of Hypoplastic Left Heart Syndrome and Single Ventricle Heart in Poland in the Context of Air Pollution. J. Clin. Med. 2021, 10, 3207. [Google Scholar] [CrossRef] [PubMed]
- Mailloux, N.A.; Henegan, C.P.; Lsoto, D.; Patterson, K.P.; West, P.C.; Foley, J.A.; Patz, J.A. Climate Solutions Double as Health Interventions. Int. J. Environ. Res. Public Health 2021, 18, 13339. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Participants | |
|---|---|
| Total; n | 1240 |
| Male; n (%) | 539 (43.47%) |
| Median age | 24 (21–28) |
| Lives in Poland | 1183 (95.40%) |
| Stayed abroad for more than 6 months | 155 (12.50%) |
| Population of the place of employment/study; n (% of complete data): | |
| City > 500,000 residents | 631 (50.86%) |
| City > 250,000 residents | 145 (11.69%) |
| City > 100,000 residents | 159 (12.82%) |
| City > 50,000 residents | 75 (6.05%) |
| City < 50,000 residents | 148 (11.95%) |
| Countryside | 82 (6.63%) |
| Place of residence as a child: n (% of complete data) | |
| City > 500,000 residents | 257 (20.73%) |
| City > 250,000 residents | 90 (7.26%) |
| City > 100,000 residents | 139 (11.21%) |
| City > 50,000 residents | 136 (10.97%) |
| City < 50,000 residents | 297 (23.95%) |
| Countryside | 321 (25.88%) |
| Formal education: | |
| Higher | 581 (46.85%) |
| Complete secondary education | 496 (40%) |
| Incomplete secondary education | 105 (8.47%) |
| Professional training | 20 (1.62%) |
| Primary education | 38 (3.06%) |
| Income: | |
| <0.3 national average | 82 (6.61%) |
| 0.3–0.5 national average | 234 (18.87%) |
| 0.5–1.0 national average | 536 (43.23%) |
| 1.0–1.5 national average | 235 (18.95%) |
| >1.5 national average | 153 (12.34%) |
| Stable relationship (at least 6 months) | 706 (56.94%) |
| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| Total | 55 (4.45%) | 637 (51.38%) | 76 (6.14%) | 472 (38.07%) |
| Male | 31 (56.36%) | 280 (44.96%) | 45 (59.21%) | 183 (39.77%) |
| Median age | 30 (28–35.5) | 24 (21–27) | 37.5 (33–42.5) | 23 (20–27) |
| (a) how many children do they have? | 1 (1–1) | N.A. | 2 (1–2) | N.A. |
| (b) when approximately do they want to have children (in years)? Among females | 1 (0–2) 2 (0–3) | 5 (2–7) 5 (2–7) | N.A. N.A. | N.A. N.A. |
| (c) what percentage of them consider adoption [% of responses yes/no] | 11 (27.50%) | 188 (51.37%) | 4 (5.80%) | 113 (34.14%) |
| (d) percentage of infertility [% of responses yes/no] | 8 (17.78%) | 20 (17.86%) | 4 (5.88%) | 7 (6.80%) |
| The Willingness to Have a Child | p-Value | ||
|---|---|---|---|
| Pronatalists | Antinatalists | ||
| Fear of child’s congenital defects/diseases. | 4 (3–5) | 4 (3–5) | 0.664 |
| Among females: | 4 (3–5) | 5 (4–5) | <0.001 |
| Dissatisfaction with the medical services (e.g., access to gynecologists, obstetricians, pediatricians, and prenatal diagnosis) | 4 (2–5) | 4 (2–4.5) | 0.488 |
| Among females: | 4 (2–5) | 4 (3–5) | <0.001 |
| Fear that climate changes will force the offspring to live on the destroyed planet (e.g., increased global average temperature, rising seas levels, extreme weather, resources conflicts). | 3 (2–5) | 3 (2–5) | 0.843 |
| Fear of pregnancy and postpartum complications. | 4 (3–5) | 4 (2–5) | 0.035 |
| Among females: | 4 (3–5) | 5 (4–5) | <0.001 |
| Fear of exacerbation of maternal chronic diseases. | 3 (2–4.5) | 3 (2–4) | 0.785 |
| Among females: | 3 (2–4) | 4 (3–5) | <0.001 |
| The Willingness to Have a Child | p-Value | ||
|---|---|---|---|
| Pronatalists | Antinatalists | ||
| Depression Among females: | 9 (4–14) 8 (4–14) | 8 (4–14) 12 (6–17) | 0.357 <0.001 |
| Anxiety Among females: | 5 (2–10) 6 (3–11) | 6 (2–10) 8 (4–12) | 0.570 0.013 |
| Stress Among females: | 9 (5–13) 10 (6–14) | 9 (5–13) 11 (7.5–15) | 0.900 0.064 |
| The Willingness to Have a Child | p-Value | ||
|---|---|---|---|
| Pronatalists | Antinatalists | ||
| Do you think that environmental causes (increasing average temperature on Earth, extreme weather, rising seas levels, climate migration) are important reasons for not deciding to have children? | 276 (35.49%) | 289 (61.23%) | <0.001 |
| Do you think that environmental causes present an exclusively sufficient reason to decide to not have a child? | 146 (19.01%) | 211 (44.70%) | <0.001 |
| Humans cause so much harm—to other humans, animals, and the environment—that it is wrong to procreate. | 2 (1–3) | 3 (2–4) | 0.743 |
| I fear the climate disaster and the environmental conditions that my kids will have to/may live in. | 4 (2–4) | 4 (3–5) | 0.726 |
| People deciding to bear children while facing climate change are irresponsible. | 1 (1–2) | 3 (2–4) | 0.307 |
| The Earth is overpopulated, and restricted resources do not allow us to reproduce uncontrollably. | 3 (1–4) | 4 (3–5) | 0.549 |
| I am afraid that, if I decided to have children, they would witness terrible consequences of climate change. | 3 (2–4) | 4 (3–5) | 0.964 |
| The Binary Logistic Regression Model | |||
|---|---|---|---|
| OR | 95%CI | p-Value | |
| Intercept | 4.280 | 1.912–9.581 | <0.001 |
| The willingness to develop professional career | 0.372 | 0.316–0.438 | <0.001 |
| The willingness to meet the right partner | 1.735 | 1.508–1.997 | <0.001 |
| The fear of unfavorable climate change | 0.512 | 0.366–0.715 | <0.001 |
| Higher income | 1.347 | 1.194–1.519 | <0.001 |
| Higher education | 1.673 | 1.214–2.307 | <0.001 |
| The fear associated with professional duties and career | 0.827 | 0.727–0.941 | <0.001 |
| The belief that environmental causes are independent reason to decide not to have a child | 0.647 | 0.451–0.927 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karuga, F.F.; Szmyd, B.; Petroniec, K.; Walter, A.; Pawełczyk, A.; Sochal, M.; Białasiewicz, P.; Strzelecki, D.; Respondek-Liberska, M.; Tadros-Zins, M.; et al. The Causes and Role of Antinatalism in Poland in the Context of Climate Change, Obstetric Care, and Mental Health. Int. J. Environ. Res. Public Health 2022, 19, 13575. https://doi.org/10.3390/ijerph192013575
Karuga FF, Szmyd B, Petroniec K, Walter A, Pawełczyk A, Sochal M, Białasiewicz P, Strzelecki D, Respondek-Liberska M, Tadros-Zins M, et al. The Causes and Role of Antinatalism in Poland in the Context of Climate Change, Obstetric Care, and Mental Health. International Journal of Environmental Research and Public Health. 2022; 19(20):13575. https://doi.org/10.3390/ijerph192013575
Chicago/Turabian StyleKaruga, Filip Franciszek, Bartosz Szmyd, Karolina Petroniec, Aleksandra Walter, Agnieszka Pawełczyk, Marcin Sochal, Piotr Białasiewicz, Dominik Strzelecki, Maria Respondek-Liberska, Monika Tadros-Zins, and et al. 2022. "The Causes and Role of Antinatalism in Poland in the Context of Climate Change, Obstetric Care, and Mental Health" International Journal of Environmental Research and Public Health 19, no. 20: 13575. https://doi.org/10.3390/ijerph192013575