
Promoting Physical Activity among Workers: A Review of Literature and Future Directions on Developing Theory-Based Interventions
 , , , , and
, , , , and 
Abstract
:
{kind=link}
{kind=link}
1. Introduction
2. Methods
3. Results
3.1. Theoretical Foundations
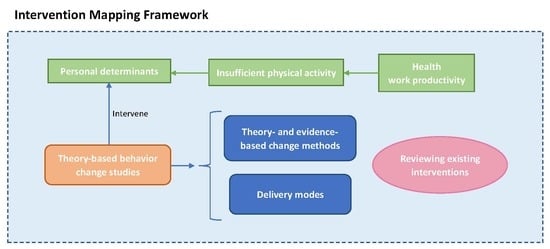
3.1.1. Intervention Mapping
3.1.2. Theories of Behavior Change and Maintenance
3.1.3. Behavior Change Techniques
3.1.4. Delivery Mode of Interventions
3.2. Existing Interventions for Physical Activity among Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Physical Activity. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 15 August 2022).
- WHO. Noncommunicable Diseases. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 15 August 2022).
- Katzmarzyk, P.T.; Friedenreich, C.; Shiroma, E.J.; Lee, I.-M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sports Med. 2022, 56, 101–106. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. The Lancet Physical Activity Series Working Group Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M. Lancet Physical Activity Series 2 Executive Committee The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Puig-Ribera, A.; Bort-Roig, J.; Giné-Garriga, M.; González-Suárez, A.M.; Martínez-Lemos, I.; Fortuño, J.; Martori, J.C.; Muñoz-Ortiz, L.; Milà, R.; Gilson, N.D.; et al. Impact of a workplace ‘sit less, move more’ program on efficiency-related outcomes of office employees. BMC Public Health 2017, 17, 455. [Google Scholar] [CrossRef]
- Clemes, S.A.; O’connell, S.E.; Edwardson, C.L. Office workers’ objectively measured sedentary behavior and physical activity during and outside working hours. J. Occup. Environ. Med. 2014, 56, 298–303. [Google Scholar] [CrossRef]
- Caputo, E.L.; Reichert, F.F. Studies of Physical Activity and COVID-19 During the Pandemic: A Scoping Review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Wilke, J.; Mohr, L.; Tenforde, A.S.; Edouard, P.; Fossati, C.; González-Gross, M.; Ramírez, C.S.; Laiño, F.; Tan, B.; Pillay, J.; et al. A pandemic within the pandemic? Physical activity levels substantially decreased in countries affected by COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2235. [Google Scholar] [CrossRef]
- Eldredge, L.K.B.; Markham, C.M.; Ruiter, R.A.; Fernández, M.E.; Kok, G.; Parcel, G.S. Planning Health Promotion Programs: An Intervention Mapping Approach; John Wiley & Sons: New York, NY, USA, 2016. [Google Scholar]
- Bardus, M.; Blake, H.; Lloyd, S.; Suggs, L.S. Reasons for participating and not participating in a e-health workplace physical activity intervention: A qualitative analysis. Int. J. Workplace Health Manag. 2014, 7, 229–246. [Google Scholar] [CrossRef]
- Mceachan, R.R.; Lawton, R.J.; Jackson, C.; Conner, M.; Lunt, J. Evidence, Theory and Context: Using intervention mapping to develop a worksite physical activity intervention. BMC Public Health 2008, 8, 326. [Google Scholar] [CrossRef]
- Hong Kong Anti-Cancer Society. Survey of the Hong Kong Anti-Cancer Society. 2017. Available online: https://hkacs.org.hk/en/medicalnews.php?id=215 (accessed on 15 August 2022).
- Hong Kong Institute of Asia-Pacific Studies. Survey Findings on Attitudes towards Physical Exercises in Hong Kong. 2016. Available online: http://www.hkiaps.cuhk.edu.hk/wd/ni/20170612-113906_1.pdf (accessed on 15 August 2022).
- Center for Health Protection. Physical Inactivity During the COVID-19 Pandemic in Non-Communicable Disease Branch. 2021. Available online: https://www.chp.gov.hk/files/pdf/ncd_watch_august_2021.pdf (accessed on 15 August 2022).
- Malik, S.H.; Blake, H.; Suggs, L.S. A systematic review of workplace health promotion interventions for increasing physical activity. Br. J. Health Psychol. 2014, 19, 149–180. [Google Scholar] [CrossRef] [PubMed]
- To, Q.G.; Chen, T.T.; Magnussen, C.G.; To, K.G. Workplace physical activity interventions: A systematic review. Am. J. Health Promot. 2013, 27, e113–e123. [Google Scholar] [CrossRef]
- Webb, T.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010, 12, e1376. [Google Scholar] [CrossRef]
- Bishop, F.L.; Fenge-Davies, A.L.; Kirby, S.; Geraghty, A.W. Context effects and behaviour change techniques in randomised trials: A systematic review using the example of trials to increase adherence to physical activity in musculoskeletal pain. Psychol. Health 2015, 30, 104–121. [Google Scholar] [CrossRef]
- McEwan, D.; Beauchamp, M.R.; Kouvousis, C.; Ray, C.M.; Wyrough, A.; Rhodes, R.E. Examining the active ingredients of physical activity interventions underpinned by theory versus no stated theory: A meta-analysis. Health Psychol. Rev. 2019, 13, 1–17. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Croot, L.; Sworn, K.; Duncan, E.; Rousseau, N.; Turner, K.; Yardley, L.; Hoddinott, P. Taxonomy of approaches to developing interventions to improve health: A systematic methods overview. Pilot Feasibility Stud. 2019, 5, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Michie, S. What works and how? Designing more effective interventions needs answers to both questions. Addiction 2008, 103, 886–887. [Google Scholar]
- Prestwich, A.; Sniehotta, F.F.; Whittington, C.; Dombrowski, S.U.; Rogers, L.; Michie, S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014, 33, 465. [Google Scholar] [CrossRef]
- Crutzen, R. The behavioral intervention technology model and intervention mapping: The best of both worlds. J. Med. Internet Res. 2014, 16, e3620. [Google Scholar] [CrossRef]
- Mohr, D.C.; Schueller, S.M.; Montague, E.; Burns, M.N.; Rashidi, P. The behavioral intervention technology model: An integrated conceptual and technological framework for eHealth and mHealth interventions. J. Med. Internet Res. 2014, 16, e3077. [Google Scholar] [CrossRef]
- Kok, G.; Schaalma, H.; Ruiter, R.A.; van Empelen, P.; Brug, J. Intervention mapping: Protocol for applying health psychology theory to prevention programmes. J. Health Psychol. 2004, 9, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Van Bokhoven, M.; Kok, G.; van der Weijden, T. Designing a quality improvement intervention: A systematic approach. BMJ Qual. Saf. 2003, 12, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Crosby, R.; Noar, S.M. Theory development in health promotion: Are we there yet? J. Behav. Med. 2010, 33, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Kok, G.; Gottlieb, N.H.; Panne, R.; Smerecnik, C. Methods for environmental change; an exploratory study. BMC Public Health 2012, 12, 1037. [Google Scholar] [CrossRef]
- Richard, L.; Potvin, L.; Kishchuk, N.; Prlic, H.; Green, L.W. Assessment of the integration of the ecological approach in health promotion programs. Am. J. Health Promot. 1996, 10, 318–328. [Google Scholar] [CrossRef]
- Garba, R.M.; Gadanya, M.A. The role of intervention mapping in designing disease prevention interventions: A systematic review of the literature. PLoS ONE 2017, 12, e0174438. [Google Scholar] [CrossRef]
- Ammendolia, C.; Côté, P.; Cancelliere, C.; Cassidy, J.D.; Hartvigsen, J.; Boyle, E.; Soklaridis, S.; Stern, P.; Amick, B. Healthy and productive workers: Using intervention mapping to design a workplace health promotion and wellness program to improve presenteeism. BMC Public Health 2016, 16, 1190. [Google Scholar] [CrossRef]
- Chen, Y.; Wu, F.; Wu, Y.; Li, J.; Yue, P.; Deng, Y.; Lamb, K.V.; Fong, S.; Liu, Y.; Zhang, Y. Development of interventions for an intelligent and individualized mobile health care system to promote healthy diet and physical activity: Using an intervention mapping framework. BMC Public Health 2019, 19, 1311. [Google Scholar] [CrossRef]
- Direito, A.; Walsh, D.; Hinbarji, M.; Albatal, R.; Tooley, M.; Whittaker, R.; Maddison, R. Using the intervention mapping and behavioral intervention technology frameworks: Development of an mHealth intervention for physical activity and sedentary behavior change. Health Educ. Behav. 2018, 45, 331–348. [Google Scholar] [CrossRef]
- Golsteijn, R.; Bolman, C.; Volders, E.; Peels, D.; de Vries, H.; Lechner, L. Development of a computer-tailored physical activity intervention for prostate and colorectal cancer patients and survivors: OncoActive. BMC Cancer 2017, 17, 446. [Google Scholar] [CrossRef]
- Hazelzet, E.; Houkes, I.; Bosma, H.; de Rijk, A. Using intervention mapping to develop ‘Healthy HR’aimed at improving sustainable employability of low-educated employees. BMC Public Health 2021, 21, 1259. [Google Scholar] [CrossRef] [PubMed]
- Mastellos, N.; Gunn, L.H.; Felix, L.M.; Car, J.; Majeed, A. Transtheoretical model stages of change for dietary and physical exercise modification in weight loss management for overweight and obese adults. Cochrane Database Syst. Rev. 2014, CD008066. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Orbell, S.; Sheeran, P. ‘Inclined abstainers’: A problem for predicting health-related behaviour. Br. J. Soc. Psychol. 1998, 37, 151–165. [Google Scholar] [CrossRef]
- Rhodes, R.E.; de Bruijn, G.J. How big is the physical activity intention–behaviour gap? A meta-analysis using the action control framework. Br. J. Health Psychol. 2013, 18, 296–309. [Google Scholar] [CrossRef]
- Hagger, M.S.; Luszczynska, A.; de Wit, J.; Benyamini, Y.; Burkert, S.; Chamberland, P.-E.; Chater, A.; Dombrowski, S.U.; van Dongen, A.; French, D.P.; et al. Implementation intention and planning interventions in Health Psychology: Recommendations from the Synergy Expert Group for research and practice. Psychol. Health 2016, 31, 814–839. [Google Scholar] [CrossRef]
- Schwarzer, R. Health action process approach (HAPA) as a theoretical framework to understand behavior change. Actual. Psicol. 2016, 30, 119–130. [Google Scholar] [CrossRef]
- Heckhausen, H.; Gollwitzer, P.M. Thought contents and cognitive functioning in motivational versus volitional states of mind. Motiv. Emot. 1987, 11, 101–120. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Chaiken, S.; Trope, Y. Dual-Process Theories in Social Psychology; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Evans, J.S.B.; Frankish, K.E. In Two Minds: Dual Processes and Beyond; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- Bargh, J.A. The four horsemen of automaticity: Intention, awareness, efficiency, and control as separate issues. In Handbook of Social Cognition; Wyer, S.T., Jr., Srull, T.K., Eds.; Psychology Press: New York, NY, USA, 1994; pp. 1–40. [Google Scholar]
- Rebar, A.L.; Dimmock, J.A.; Jackson, B.; Rhodes, R.E.; Kates, A.; Starling, J.; Vandelanotte, C. A systematic review of the effects of non-conscious regulatory processes in physical activity. Health Psychol. Rev. 2016, 10, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Strack, F.; Deutsch, R. Reflective and impulsive determinants of social behavior. Pers. Soc. Psychol. Rev. 2004, 8, 220–247. [Google Scholar] [CrossRef] [PubMed]
- Lally, P.; Gardner, B. Promoting habit formation. Health Psychol. Rev. 2013, 7, S137–S158. [Google Scholar] [CrossRef]
- Rebar, A.L.; Loftus, A.M.; Hagger, M.S. Cognitive control and the non-conscious regulation of health behavior. Front. Hum. Neurosci. 2015, 9, 122. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Carey, R.N.; Johnston, M.; Rothman, A.J.; de Bruin, M.; Kelly, M.P.; Connel, L.E. From theory-inspired to theory-based interventions: A protocol for developing and testing a methodology for linking behaviour change techniques to theoretical mechanisms of action. Ann. Behav. Med. 2018, 52, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Bohlen, L.C.; Michie, S.; de Bruin, M.; Rothman, A.J.; Kelly, M.P.; Groarke, H.N.K.; Carey, R.N.; Hale, J.; Johnston, M. Do combinations of behavior change techniques that occur frequently in interventions reflect underlying theory? Ann. Behav. Med. 2020, 54, 827–842. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379. [Google Scholar] [CrossRef]
- Kok, G.; Gottlieb, N.H.; Peters, G.-J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.; Fernández, M.E.; Markham, C.M.; Bartholomew, L.K. A taxonomy of behaviour change methods: An Intervention Mapping approach. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Michie, S.; Wood, C.E.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W. Behaviour change techniques: The development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol. Assess. 2015, 19, 1–188. [Google Scholar] [PubMed]
- Stavri, Z.; Michie, S. Classification systems in behavioural science: Current systems and lessons from the natural, medical and social sciences. Health Psychol. Rev. 2012, 6, 113–140. [Google Scholar] [CrossRef]
- Dombrowski, S.U.; Sniehotta, F.F.; Avenell, A.; Johnston, M.; MacLennan, G.; Araújo-Soares, V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychol. Rev. 2012, 6, 7–32. [Google Scholar] [CrossRef]
- Michie, S.; Johnston, M. Theories and techniques of behaviour change: Developing a cumulative science of behaviour change. Health Psychol. Rev. 2012, 6, 1–6. [Google Scholar] [CrossRef]
- Michie, S.; Hyder, N.; Walia, A.; West, R. Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addict. Behav. 2011, 36, 315–319. [Google Scholar] [CrossRef]
- West, R.; Walia, A.; Hyder, N.; Shahab, L.; Michie, S. Behavior change techniques used by the English Stop Smoking Services and their associations with short-term quit outcomes. Nicotine Tob. Res. 2010, 12, 742–747. [Google Scholar] [CrossRef]
- Michie, S.; Whittington, C.; Hamoudi, Z.; Zarnani, F.; Tober, G.; West, R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction 2012, 107, 1431–1440. [Google Scholar] [CrossRef] [PubMed]
- Carraça, E.; Encantado, J.; Battista, F.; Beaulieu, K.; Blundell, J.; Busetto, L.; van Baak, M.; Dicker, D.; Ermolao, A.; Farpour-Lambert, N.; et al. Effective behavior change techniques to promote physical activity in adults with overweight or obesity: A systematic review and meta-analysis. Obes. Rev. 2021, 22, e13258. [Google Scholar] [CrossRef]
- Howlett, N.; Trivedi, D.; Troop, N.A.; Chater, A.M. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl. Behav. Med. 2019, 9, 147–157. [Google Scholar] [CrossRef]
- Kaufman, J.; Ryan, R.; Walsh, L.; Horey, D.; Leask, J.; Robinson, P.; Hill, S. Face-to-face interventions for informing or educating parents about early childhood vaccination. Cochrane Database Syst. Rev. 2018, 5, CD010038. [Google Scholar] [CrossRef]
- Schröer, S.; Haupt, J.; Pieper, C. Evidence-based lifestyle interventions in the workplace—An overview. Occup. Med. 2014, 64, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Barak, A.; Klein, B.; Proudfoot, J.G. Defining internet-supported therapeutic interventions. Ann. Behav. Med. 2009, 38, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.W.; Grønbæk, M.; Helge, J.W.; Severin, M.; Curtis, T.; Tolstrup, J.S. Effect of a web-based intervention to promote physical activity and improve health among physically inactive adults: A population-based randomized controlled trial. J. Med. Internet Res. 2012, 14, e2109. [Google Scholar] [CrossRef] [PubMed]
- Erbe, D.; Eichert, H.-C.; Riper, H.; Ebert, D.D. Blending face-to-face and internet-based interventions for the treatment of mental disorders in adults: Systematic review. J. Med. Internet Res. 2017, 19, e6588. [Google Scholar] [CrossRef]
- Griffiths, F.; Lindenmeyer, A.; Powell, J.; Lowe, P.; Thorogood, M. Why are health care interventions delivered over the internet? A systematic review of the published literature. J. Med. Internet Res. 2006, 8, e498. [Google Scholar] [CrossRef]
- Napolitano, M.A.; Marcus, B.H. Targeting and tailoring physical activity information using print and information technologies. Exerc. Sport Sci. Rev. 2002, 30, 122–128. [Google Scholar] [CrossRef]
- Gustafson, D.H.; Bosworth, K.; Chewning, B.; Hawkins, R.P. Computer-based health promotion: Combining technological advances with problem-solving techniques to effect successful health behavior changes. Ann. Rev. Public Health 1987, 8, 387–415. [Google Scholar] [CrossRef]
- Gustafson, D.H.; Hawkins, R.P.; Boberg, E.W.; McTavish, F.; Owens, B.; Wise, M.; Berhe, H.; Pingree, S. CHESS: 10 years of research and development in consumer health informatics for broad populations, including the underserved. Int. J. Med. Inform. 2002, 65, 169–177. [Google Scholar] [CrossRef]
- Shaw, B.; Gustafson, D.H.; Hawkins, R.; McTavish, F.; McDowell, H.; Pingree, S.; Ballard, D. How underserved breast cancer patients use and benefit from eHealth programs: Implications for closing the digital divide. Am. Behav. Sci. 2006, 49, 823–834. [Google Scholar] [CrossRef]
- Kloek, C.; Bossen, D.; de Bakker, D.H.; Veenhof, C.; Dekker, J. Blended interventions to change behavior in patients with chronic somatic disorders: Systematic review. J. Med. Internet Res. 2017, 19, e8108. [Google Scholar] [CrossRef]
- Van Buul, A.R.; Kasteleyn, M.J.; Arends, J.M.; Shi, T.; Kelly, D.P.; Chavannes, N.H.; Meijer, E. eHealth only interventions and blended interventions to support self-management in adolescents with asthma: A systematic review. Clin. Health 2020, 3, 49–62. [Google Scholar] [CrossRef]
- Reed, V.A.; Schifferdecker, K.E.; Rezaee, M.E.; O’Connor, S.; Larson, R.J. The effect of computers for weight loss: A systematic review and meta-analysis of randomized trials. J. Gen. Intern. Med. 2012, 27, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Lock, M.; Post, D.; Dollman, J.; Parfitt, G. Efficacy of theory-informed workplace physical activity interventions: A systematic literature review with meta-analyses. Health Psychol. Rev. 2021, 15, 483–507. [Google Scholar] [CrossRef] [PubMed]
- Jahangiry, L.; Farhangi, M.A.; Shab-Bidar, S.; Rezaei, F.; Pashaei, T. Web-based physical activity interventions: A systematic review and meta-analysis of randomized controlled trials. Public Health 2017, 152, 36–46. [Google Scholar] [CrossRef]
- Booth, M. Assessment of physical activity: An international perspective. Res. Q. Exerc. Sport 2000, 71, 114–120. [Google Scholar] [CrossRef]
- Guertler, D.; Vandelanotte, C.; Kirwan, M.; Duncan, M.J. Engagement and nonusage attrition with a free physical activity promotion program: The case of 10,000 steps Australia. J. Med. Internet Res. 2015, 17, e4339. [Google Scholar] [CrossRef]
- Maher, C.A.; Lewis, L.K.; Ferrar, K.; Marshall, S.; de Bourdeaudhuij, I.; Vandelanotte, C. Are health behavior change interventions that use online social networks effective? A systematic review. J. Med. Internet Res. 2014, 16, e2952. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Duncan, M.J.; Kolt, G.S.; Caperchione, C.M.; Savage, T.N.; van Itallie, A.; Oldmeadow, C.; Alley, S.J.; Tague, R.; Maeder, A.J.; et al. More real-world trials are needed to establish if web-based physical activity interventions are effective. Br. J. Sports Med. 2019, 53, 1553–1554. [Google Scholar] [CrossRef]
- Allam, F.N.B.; Hamid, M.R.A.; Buhari, S.S.; Noor, H.M. Web-Based Dietary and Physical Activity Intervention Programs for Patients With Hypertension: Scoping Review. J. Med. Internet Res. 2021, 23, e22465. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Y.; Gao, Y.; Yu, S.; Wang, A.; Ou, X.; Tao, D.; Baker, J.S. Promoting Physical Activity among Workers: A Review of Literature and Future Directions on Developing Theory-Based Interventions. Int. J. Environ. Res. Public Health 2022, 19, 13594. https://doi.org/10.3390/ijerph192013594
Sun Y, Gao Y, Yu S, Wang A, Ou X, Tao D, Baker JS. Promoting Physical Activity among Workers: A Review of Literature and Future Directions on Developing Theory-Based Interventions. International Journal of Environmental Research and Public Health. 2022; 19(20):13594. https://doi.org/10.3390/ijerph192013594
Chicago/Turabian StyleSun, Yan, Yang Gao, Siyue Yu, Aiwei Wang, Xiaoting Ou, Dan Tao, and Julien S. Baker. 2022. "Promoting Physical Activity among Workers: A Review of Literature and Future Directions on Developing Theory-Based Interventions" International Journal of Environmental Research and Public Health 19, no. 20: 13594. https://doi.org/10.3390/ijerph192013594