
Weight Control Registry Using Korean Medicine: A Protocol for a Prospective Registry Study
 , , , , , , and
, , , , , , and
Abstract
:
1. Introduction
2. Methods
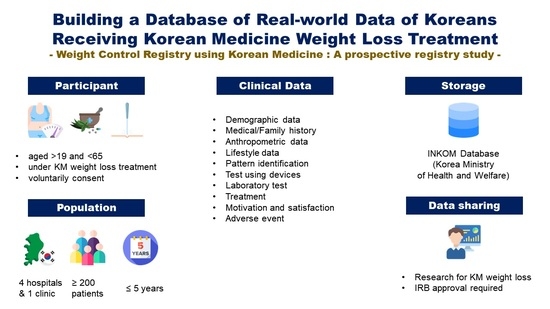
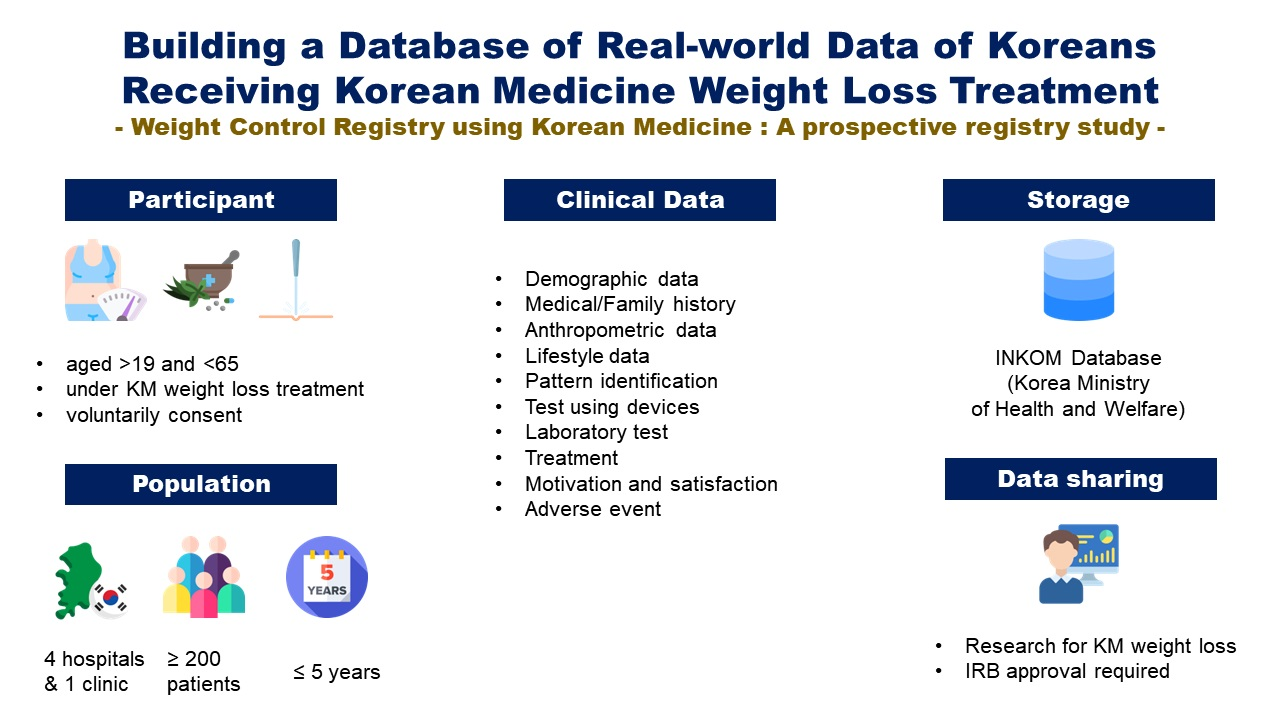
2.1. Objectives
2.2. Study Design
2.3. Study Participants
2.4. Identification and Recruitment
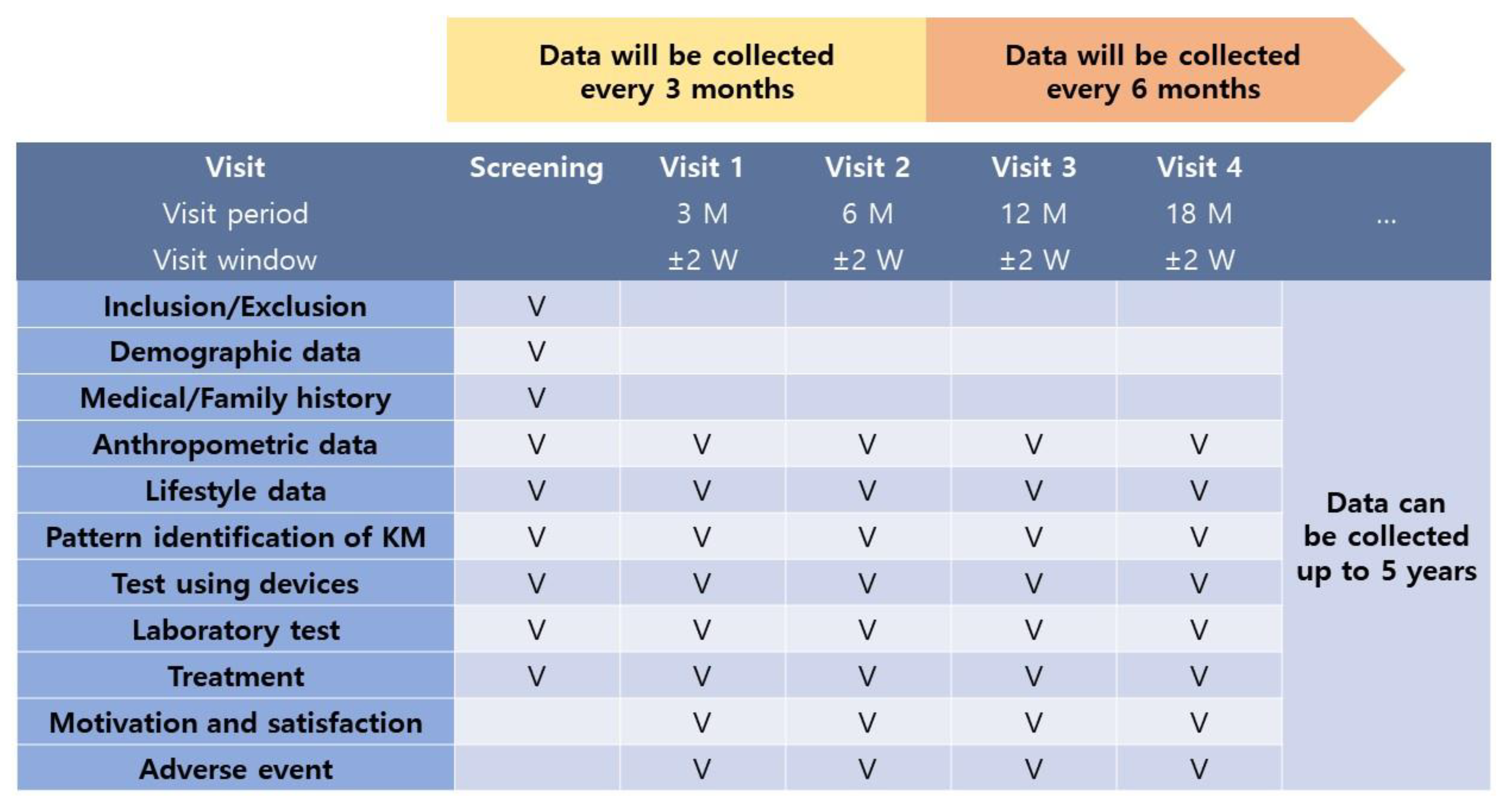
2.5. Follow-Up
2.6. Data Collection, Variables, and Definitions
2.6.1. Demographic Data
2.6.2. Anthropometric Data
2.6.3. Lifestyle Data
2.6.4. Medical/Family History
2.6.5. Pattern Identification of Korean Medicine
2.6.6. Test using devices
2.6.7. Laboratory Test
2.6.8. Treatment
2.6.9. Motivation and Satisfaction
2.6.10. Adverse Events
2.7. Quality Control
2.8. Sample Size
2.9. Data Analysis
2.10. Governance, Oversight, and Data Sharing
2.11. Ethical Approval and Trial Registration
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Health Insurance Service. Evaluation of the Socioeconomic Impact of Major Health Risk Factors and the Effectiveness of Regulatory Policies. Available online: https://www.nhis.or.kr/nhis/about/wbhaec07810m01.do?mode=view&articleNo=116002&article.offset=0&articleLimit=10&srSearchVal=%EC%A3%BC%EC%9A%94+%EA%B1%B4%EA%B0%95%EC%9C%84%ED%97%98%EC%9A%94%EC%9D%B8%EC%9D%98 (accessed on 20 July 2022).
- Deurenberg, P.; Deurenberg-Yap, M.; Guricci, S. Asians are different from Caucasians and from each other in their body mass index/body fat percent relationship. Obes. Rev. 2002, 3, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Jih, J.; Mukherjea, A.; Vittinghoff, E.; Nguyen, T.T.; Tsoh, J.Y.; Fukuoka, Y.; Bender, M.S.; Tseng, W.; Kanaya, A.M. Using appropriate body mass index cut points for overweight and obesity among Asian Americans. Prev. Med. 2014, 65, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, C.P.; Cheng, T.Y.D.; Tsai, S.P.; Chan, H.T.; Hsu, H.L.; Hsu, C.C.; Eriksen, M.P. Are Asians at greater mortality risks for being overweight than Caucasians? Redefining obesity for Asians. Public Health Nutr. 2009, 12, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Disease Control and Prevention Agency. Korea Health Statistics 2019. Korea National Health and Nutrition Examination Survey. Available online: https://knhanes.kdca.go.kr/knhanes/sub04/sub04_04_01.do (accessed on 20 July 2022).
- Liu, Y.; Sun, M.; Yao, H.; Liu, Y.; Gao, R. Herbal medicine for the treatment of obesity: An overview of scientific evidence from 2007 to 2017. Evid.-Based Complement. Alternat. Med. 2017, 2017, 8943059. [Google Scholar] [CrossRef] [PubMed]
- Martel, J.; Ojcius, D.M.; Chang, C.-J.; Lin, C.-S.; Lu, C.-C.; Ko, Y.-F.; Tseng, S.-F.; Lai, H.-C.; Young, J.D. Anti-obesogenic and antidiabetic effects of plants and mushrooms. Nat. Rev. Endocrinol. 2017, 13, 149–160. [Google Scholar] [CrossRef]
- Park, J.H.; Lee, M.J.; Song, M.Y.; Bose, S.; Shin, B.C.; Kim, H.J. Efficacy and safety of mixed oriental herbal medicines for treating human obesity: A systematic review of randomized clinical trials. J. Med. Food 2012, 15, 589–597. [Google Scholar] [CrossRef]
- Kim, S.Y.; Shin, I.S.; Park, Y.J. Effect of acupuncture and intervention types on weight loss: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1585–1596. [Google Scholar] [CrossRef] [Green Version]
- Maunder, A.; Bessell, E.; Lauche, R.; Adams, J.; Sainsbury, A.; Fuller, N.R. Effectiveness of herbal medicines for weight loss: A systematic review and meta-analysis of randomized controlled trials. Diabetes Obes. Metab. 2020, 22, 891–903. [Google Scholar] [CrossRef]
- Wong, A.R.; Yang, A.W.H.; Li, K.; Gill, H.; Li, M.; Lenon, G.B. Chinese herbal medicine for weight management: A systematic review and meta-analyses of randomised controlled trials. J. Obes. 2021, 2021, 3250723. [Google Scholar] [CrossRef]
- Zhang, G.B.; Li, Q.Y.; Chen, Q.L.; Su, S.B. Network pharmacology: A new approach for Chinese herbal medicine research. J. Evid.-Based Complement. Altern. Med. 2013, 2013, 621423. [Google Scholar] [CrossRef]
- Kim, M.K.; Lee, W.Y.; Kang, J.H.; Kang, J.H.; Kim, B.T.; Kim, S.M.; Kim, E.M.; Suh, S.H.; Shin, H.J.; Lee, K.R.; et al. 2014 clinical practice guidelines for overweight and obesity in Korea. Endocrinol. Metab. 2014, 29, 405–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Agency for Korean Medicine Innovative Technologies Development. Guidelines for Standardizing Clinical Research Data in the Development of Korean Medicine Innovation Technology. Version 1.0. Available online: http://nikom.or.kr/nckm/board/view.do?menu_idx=160&manage_idx=113&board_idx=10202&group_depth=0&parent_idx=0&group_idx=10200&search_type=title%2Bcontent&search_text=&rowCount=10&viewPage=2 (accessed on 20 July 2022).
- Chun, M.Y. Validity and reliability of Korean version of International Physical Activity Questionnaire Short Form in the elderly. Korean J. Fam. Med. 2012, 33, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.S.; Kim, H.Y.; Hwang, J.Y.; Kwon, S.; Chung, H.R.; Kwak, T.K.; Kang, M.H.; Choi, Y.S. Development of nutrition quotient for Korean adults: Item selection and validation of factor structure. J. Nutr. Health 2018, 51, 340–356. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.H.; Lee, S.J.; Hwang, S.T.; Hong, S.H.; Kim, J.H. Reliability and validity of the Beck Depression Inventory-II among Korean adolescents. Psychiatry Investig. 2017, 14, 30–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohn, S.I.; Kim, D.H.; Lee, M.Y.; Cho, Y.W. The reliability and validity of the Korean version of the Pittsburgh Sleep Quality Index. Sleep Breath 2012, 16, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.W.; Lee, J.H.; Son, H.K.; Lee, S.H.; Shin, C.; Johns, M.W. The reliability and validity of the Korean version of the Epworth Sleepiness Scale. Sleep Breath 2011, 15, 377–384. [Google Scholar] [CrossRef]
- Lee, J.H.; Jeong, H.S.; Lim, S.M.; Cho, H.B.; Ma, J.Y.; Ko, E.; Im, J.J.; Lee, S.H.; Lee, Y.J.; Lyoo, I.K.; et al. Reliability and validity of the fatigue severity scale among university student in South Korea. Korean J. Biol. Psychiatry 2013, 20, 6–11. [Google Scholar]
- Park, H.S.; Sung, S.W.; Ou, S.W.; Lee, K.Y.; Kim, B.S.; Han, J.H.; Kim, S.M.; Lee, H.R.; Yu, B.Y.; Lee, K.M.; et al. Development of Korean version of obesity-related quality of life scale. J. Korean Soc. Study Obes. 2003, 12, 280–293. [Google Scholar]
- World Health Organization. WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region. Available online: https://apps.who.int/iris/handle/10665/206952 (accessed on 20 July 2022).
- Kang, K.W.; Moon, J.S.; Kang, B.G.; Kim, B.Y.; Shin, M.S.; Choi, S.M. The comparison of pattern identification diagnosis according to symptom scale based on obesity pattern identification questionnaire. J. Korean Obes. Res. 2009, 9, 37–44. [Google Scholar]
- Bae, K.H.; Jang, E.S.; Park, K.; Lee, Y. Development on the questionnaire of cold-heat pattern identification based on usual symptoms: Reliability and validation study. J. Physiol. Pathol. Korean Med. 2018, 32, 341–346. [Google Scholar] [CrossRef]
- Jang, E.S.; Yoon, J.H.; Baek, Y.H.; Lee, S.W. Evaluation of reliability and validity for deficiency and excess pattern identification questionnaire. J. Physiol. Pathol. Korean Med. 2018, 32, 171–177. [Google Scholar] [CrossRef]
- Baek, Y.H.; Jang, E.S.; Park, K.H.; Yoo, J.H.; Jin, H.J.; Lee, S.W. Development and validation of brief KS-15 (Korea Sasang constitutional diagnostic questionnaire) based on body shape, temperament and symptoms. J. Sasang Constit. Med. 2015, 27, 211–221. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.G.; Bond, D.S.; Phelan, S.; Hill, J.O.; Wing, R.R. Weight-loss maintenance for 10 years in the National Weight Control Registry. Am. J. Prev. Med. 2014, 46, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Laddu, D.; Dow, C.; Hingle, M.; Thomson, C.; Going, S. A review of evidence-based strategies to treat obesity in adults. Nutr. Clin. Pract. 2011, 26, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Blasco, B.V.; García-Jiménez, J.; Bodoano, I.; Gutiérrez-Rojas, L. Obesity and depression: Its prevalence and influence as a prognostic factor: A systematic review. Psychiatry Investig. 2020, 17, 715. [Google Scholar] [CrossRef] [PubMed]
- Sa, J.; Choe, S.; Cho, B.Y.; Chaput, J.P.; Kim, G.; Park, C.H.; Chung, J.; Choi, Y.; Nelson, B.; Kim, Y. Relationship between sleep and obesity among U.S. and South Korean college students. BMC Public Health 2020, 20, 96. [Google Scholar] [CrossRef] [Green Version]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Hopper, K.; Lotsikas, A.; Lin, H.M.; Kales, A.; Chrousos, G.P. Sleep apnea and daytime sleepiness and fatigue: Relation to visceral obesity, insulin resistance, and hypercytokinemia. J. Clin. Endocrinol. Metab. 2000, 85, 1151–1158. [Google Scholar] [CrossRef]
- Lyu, S.; Zhang, C.S.; Zhang, A.L.; Sun, J.; Xue, C.C.; Guo, X. Migraine patients visiting Chinese medicine hospital: Protocol for a prospective, registry-based, real-world observational cohort study. PLoS ONE 2022, 17, e0265137. [Google Scholar] [CrossRef]
- Chu, H.; Jang, B.H.; Lee, E.; Moon, S.; Ham-soa Clinic KM Doctors Group. Combined Korean medicine therapies in children with allergic rhinitis: A multi-center, observational explanatory registry trial: A study protocol. Medicine 2021, 100, e28181. [Google Scholar] [CrossRef]
- Bae, K.; Kim, E.; Choi, J.J.; Kim, M.K.; Yoo, H.S. The effectiveness of anticancer traditional Korean medicine treatment on the survival in patients with lung, breast, gastric, colorectal, hepatic, uterine, or ovarian cancer: A prospective cohort study protocol. Medicine 2018, 97, e12444. [Google Scholar] [CrossRef]
- Ko, M.M.; Kim, B.Y.; Son, M.J.; Jegal, K.H.; Chung, W.S.; Kim, S. Korean medicine registry of herbal medicine for weight loss. Medicine 2022, 101, e29407. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Domain | Items |
|---|---|
| Demographic data | Age, sex, educational attainment, region, occupation, smoking status, drinking habits, exercise routine |
| Anthropometric data | Vital signs, body weight, height, BMI 1, body fat, body muscle, visceral fat level, obesity rate, total body water content |
| Lifestyle data | iPAQ 2, NQ 3, BDI-II 4, PSQI-K 5, ESS 6, FSS 7, KOQOL 8 |
| Medical/family history | History of obesity |
| Pattern identification of KM 9 | OPIQ 10, cold/heat pattern, deficiency/excess pattern, Sasang constitutions |
| Test using devices | Tongue, pulse, facial color patterns measured by devices |
| Laboratory test | Liver function, renal function, lipid and glucose level tests |
| Treatment | Herbal medicine, acupuncture, moxibustion, cupping, physical therapy, others |
| Motivation and satisfaction | Motivation to visit, willingness to revisit for weight loss, overall treatment satisfaction |
| Adverse event | Adverse events during KM 9 treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cha, J.; Ahn, E.K.; Kim, M.-J.; Jung, S.-Y.; Kim, H.-S.; Kim, E.; Sung, H.-K.; Shin, S.M.; Chung, W.-S.; Lee, J.-H.; et al. Weight Control Registry Using Korean Medicine: A Protocol for a Prospective Registry Study. Int. J. Environ. Res. Public Health 2022, 19, 13903. https://doi.org/10.3390/ijerph192113903
Cha J, Ahn EK, Kim M-J, Jung S-Y, Kim H-S, Kim E, Sung H-K, Shin SM, Chung W-S, Lee J-H, et al. Weight Control Registry Using Korean Medicine: A Protocol for a Prospective Registry Study. International Journal of Environmental Research and Public Health. 2022; 19(21):13903. https://doi.org/10.3390/ijerph192113903
Chicago/Turabian StyleCha, Jiyun, Eun Kyoung Ahn, Min-Ji Kim, So-Young Jung, Ho-Seok Kim, Eunjoo Kim, Hyun-Kyung Sung, Seon Mi Shin, Won-Seok Chung, Jun-Hwan Lee, and et al. 2022. "Weight Control Registry Using Korean Medicine: A Protocol for a Prospective Registry Study" International Journal of Environmental Research and Public Health 19, no. 21: 13903. https://doi.org/10.3390/ijerph192113903