
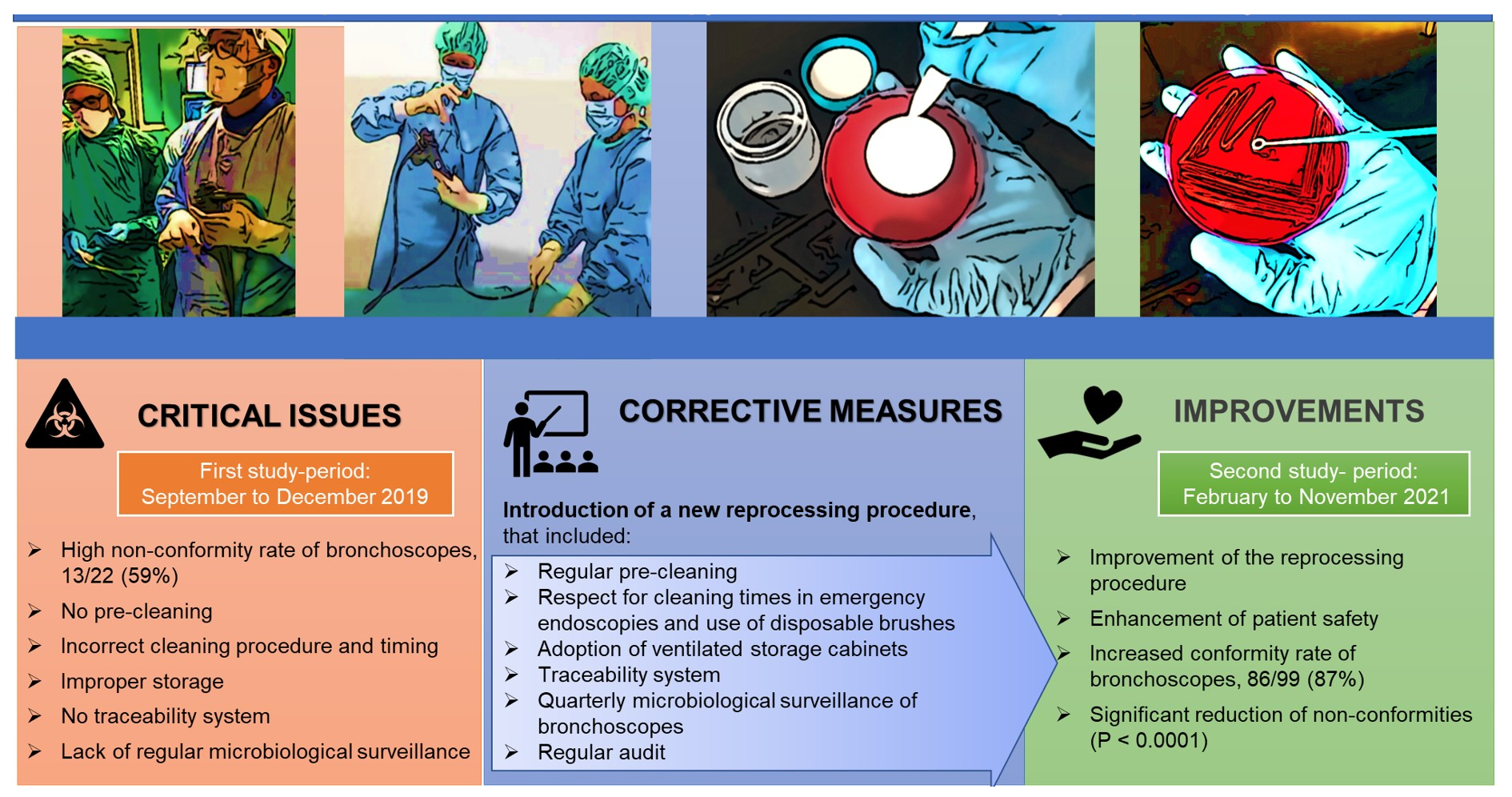
Adoption of Improved Reprocessing Decreased Microbiological Non-Compliance for Bronchoscopes
 and
and
Abstract
:
1. Introduction
2. Methods
2.1. Reprocessing Process
2.2. Sampling Method and Microbiological Analysis
2.3. Non-Compliant Bronchoscopes Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manthous, C.; Tobin, M. Flexible bronchoscopy. Am. J. Respir. Crit. Care Med. 2015, 191, 7–8. [Google Scholar] [CrossRef] [Green Version]
- Ofstead, C.L.; Quick, M.R.; Wetzler, H.P.; Eiland, J.E.; Heymann, O.L.; Sonetti, D.A.; Ferguson, J.S. Effectiveness of Reprocessing for Flexible Bronchoscopes and Endobronchial Ultrasound Bronchoscopes. Chest 2018, 154, 1024–1034. [Google Scholar] [CrossRef] [PubMed]
- Zweigner, J.; Gastmeier, P.; Kola, A.; Klefisch, F.R.; Schweizer, C.; Hummel, M. A carbapenem resistant Klebsiella pneumoniae outbreak following bronchoscopy. Am. J. Infect. Control 2014, 42, 936–937. [Google Scholar] [CrossRef]
- DiazGranados, C.A.; Jones, M.Y.; Kongphet-Tran, T.; White, N.; Shapiro, M.; Wang, Y.F.; Ray, S.M.; Blumberg, H.M. Outbreak of Pseudomonas aeruginosa infection associated with contamination of a flexible bronchoscope. Infect. Control. Hosp. Epidemiol. 2009, 30, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Kovaleva, J.; Peters, F.T.; van der Mei, H.C.; Degener, J.E. Transmission of infection by flexible gastrointestinal endoscopy and bronchoscopy. Clin. Microbiol. Rev. 2013, 26, 231–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, A.C.; Muscarella, L.F. Bronchoscope-Related “Superbug” Infections. Chest 2020, 157, 454–469. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Murata, K.; Yamamoto, M.; Ishiwata, T.; Kitazono-Saitoh, M.; Wada, A.; Takamori, M. Risk factors for post-bronchoscopy pneumonia: A case-control study. Sci. Rep. 2020, 10, 19983. [Google Scholar] [CrossRef]
- FDA. Safety Communications & Infections Associated with Reprocessed Flexible Bronchoscopes: FDA Safety Communication Infections Associated with Reprocessed Flexible Bronchoscopes: FDA Safety Communication. 2015. Available online: http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm462949.htm (accessed on 2 February 2022).
- Flexible Bronchoscopes and Updated Recommendations for Reprocessing: FDA Safety Communication FDA. 2021. Available online: https://www.fda.gov/medical-devices/safety-communications/flexible-bronchoscopes-and-updated-recommendations-reprocessing-fda-safety-communication (accessed on 2 February 2022).
- PENTAX. MAUDE Adverse Event Report: Hoya Corporation PENTAX Tokyo Office PENTAX Fiber Bronchoscope; MDR Report Key 7287335; Food and Drug Administration: Spring, MD, USA, 2017. [Google Scholar]
- Dickson, A. Enterobacter cloacae found in an endobronchial ultrasound scope (EBUS): Now what do we do? In Proceedings of the Association for Professionals in Infection Control and Epidemiology Annual Conference, Portland, OR, USA, 14–16 June 2017. [Google Scholar]
- Portland, O.R.; Ofstead, C.L.; Doyle, E.M.; Eiland, J.E.; Amelang, M.R.; Wetzler, H.P.; England, D.M.; Mascotti, K.M.; Shaw, M.J. Practical toolkit for monitoring endoscope reprocessing effectiveness: Identification of viable bacteria on gastroscopes, colonoscopes, and bronchoscopes. Am. J. Infect. Control 2016, 44, 815–819. [Google Scholar]
- Galdys, A.L.; Marsh, J.W.; Delgado, E.; Pasculle, A.W.; Pacey, M.; Ayres, A.M.; Metzger, A.; Harrison, L.H.; Muto, C.A. Bronchoscope-associated clusters of multidrug-resistant Pseudomonas aeruginosa and carbapenem-resistant Klebsiella pneumoniae. Infect. Control Hosp. Epidemiol. 2019, 40, 40–46. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, H.; Jiang, Q.; Wang, Q.; Li, S.; Huang, Y. Bronchoscope-related Pseudomonas aeruginosa pseudo-outbreak attributed to contaminated rinse water. Am. J. Infect. Control 2020, 48, 26–32. [Google Scholar] [CrossRef]
- Cowen, A.; Jones, D.; Wardle, E. Infection Control in Endoscopy, 3rd ed.; Gastroenterological Society of Australia (GESA): Melbourne, VIC, Australia, 2010; Available online: https://www.asp.com/sites/default/files/pdf/best-practices/GESA-guideline-gastrointestinal-endoscopey-(Australia).pdf (accessed on 2 February 2022).
- Saliou, P.; Le Bars, H.; Payan, C.; Narbonne, V.; Cholet, F.; Jézéquel, J.; Scotet, V.; Robaszkiewicz, M.; Cornec, D.; Héry-Arnaud, G.; et al. Measures to improve microbial quality surveillance of gastrointestinal endoscopes. Endoscopy 2016, 48, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Bisset, L.; Cossart, Y.E.; Selby, W.; West, R.; Catterson, D.; O’Hara, K.; Vickery, K. A prospective study of the efficacy of routine decontamination for gastrointestinal endoscopes and the risk factors for failure. Am. J. Infect. Control 2006, 34, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Agenzia Regionale di Sanità Toscana (ARS). Il Reprocessing in Endoscopia Digestiva: Criticità e Strumenti per la Sicurezza del Percorso. Collana dei Documenti ARS, n. 70. 2013. Available online: https://www.ars.toscana.it/files/pubblicazioni/Volumi/2013/doc_ars_70_2013_ok.pdf (accessed on 2 February 2022).
- Beilenhoff, U.; Biering, H.; Blum, R.; Brljak, J.; Cimbro, M.; Dumonceau, J.M.; Hassan, C.; Jung, M.; Kampf, B.; Neumann, C.; et al. Reprocessing of flexible endoscopes and endoscopic accessories used in gastrointestinal endoscopy: Position Statement of the European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastroenterology Nurses and Associates (ESGENA)—Update 2018. Endoscopy 2018, 50, 1205–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC) Duodenoscope Surveillance Sampling & Culturing. Reducing the Risks of Infection. 2018. Available online: https://www.fda.gov/media/111081/download (accessed on 4 March 2022).
- Centers for Disease Control and Prevention (CDC). Essential Elements of a Reprocessing Program for Flexible Endoscopes—Recommendations of the Healthcare Infection Control Practices Advisory Committee; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2016; pp. 1–12. Available online: https://www.cdc.gov/hicpac/pdf/flexible-endoscope-reprocessing.pdf (accessed on 2 February 2022).
- South Australia Health Safety & Quality Strategic Governance. Clinical Guideline for Microbiological Testing of Endoscopes. 2017. Available online: https://www.sahealth.sa.gov.au (accessed on 2 February 2022).
- Casini, B.; Tuvo, B.; Marciano, E.; Del Magro, G.; Gemignani, G.; Luchini, G.; Cristina, M.; Costa, A.; Arzilli, G.; Totaro, M.; et al. Improving the Reprocessing Quality of Flexible Thermolabile Endoscopes: How to Learn from Mistakes. Int. J. Environ. Res. Public Health 2021, 18, 2482. [Google Scholar] [CrossRef]
- Ostertagova, E. Modelling using polynomial regression. Procedia Eng. 2021, 48, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Casini, B.; Pan, A.; Guarini, A.; Rivara, C.; Zullo, A.; Monica, F.; Cimbro, M.; Casarano, S.; Inglese, A.; Vaghi, A.; et al. Multisocieties position paper: Microbiological surveillance on flexible endoscopes. Dig Liver Dis. 2021, 53, 1105–1111. [Google Scholar] [CrossRef]
- Troiano, G.; Lo Nostro, A.; Calonico, C.; Nante, N.; Magistri, L.; Pulci, M.B.; Niccolini, F. Microbiological surveillance of flexible bronchoscopes after a high-level disinfection with peracetic acid: Preliminary results from an Italian teaching hospital. Ann. Ig. 2019, 31, 13–20. [Google Scholar]
- Perumpail, R.B.; Marya, N.B.; McGinty, B.L.; Muthusamy, V.R. Endoscope reprocessing: Comparison of drying effectiveness and microbial levels with an automated drying and storage cabinet with forced filtered air and a standard storage cabinet. Am. J. Infect. Control 2019, 47, 1083–1089. [Google Scholar] [CrossRef]
- Ofstead, C.L.; Heymann, O.L.; Quick, M.R.; Eiland, J.E.; Wetzler, H.P. Residual moisture and waterborne pathogens inside flexible endoscopes: Evidence from a multisite study of endoscope drying effectiveness. Am. J. Infect. Control 2018, 46, 689–696. [Google Scholar] [CrossRef]
- ECRI Institute. Top 10 Health Technology Hazards for 2018: Executive Brief. 2018. Available online: https://www.ecri.org/Resources/Whitepapers_and_reports/Haz_18.pdf (accessed on 4 March 2022).
- Aumeran, C.; Thibert, E.; Chapelle, F.A.; Hennequin, C.; Lesens, O.; Traoré, O. Assessment on experimental bacterial biofilms and in clinical practice of the efficacy of sampling solutions for microbiological testing of endoscopes. J. Clin. Microbiol. 2012, 50, 938–942. [Google Scholar] [CrossRef] [Green Version]
- Ofstead, C.L.; Hopkins, K.M.; Buro, B.L.; Eiland, J.E.; Wetzler, H.P. Challenges in achieving effective high-level disinfection in endoscope reprocessing. Am. J. Infect. Control 2020, 48, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Dutch Advisory Board Cleaning and Disinfection Flexible Endoscopes (SFERD). Flexible Endoscopes. In Professional Standard Handbook Cleaning and Disinfection; Version 4.1. 2017. Available online: http://www.infectiepreventieopleidingen.nl/downloads/SFERDHandbook3_1.pdf (accessed on 11 March 2022).
- Empfehlung der Kommission fur Krankenhaushygiene und In- fektionspravention (KRINKO) beim Robert-Koch- Institut (RKI) und des Bundesinstituts fur Arzneimittel und Medizin- produkt (BfArM). Anforderungen Die Hyg. Bei Der Auf Bereitung Von Med. Bundesgesundheitsbl 2012, 55, 1244–1310.
- Wahidi, M.M.; Lamb, C.; Murgu, S.; Musani, A.; Shojaee, S.; Sachdeva, A.; Maldonado, F.; Mahmood, K.; Kinsey, M.; Sethi, S.; et al. American Association for Bronchology and Interventional Pulmonology (AABIP) statement on the use of bronchoscopy and respiratory specimen collection in patients with suspected or confirmed COVID-19 infection. J. Bronchol. Interv. Pulmonol. 2020, 27, e52–e54. [Google Scholar] [CrossRef] [PubMed]
- Ofstead, C.L.; Hopkins, K.M.; Smart, A.G.; Brewer, M.K. Droplet dispersal in decontamination areas of instrument reprocessing suites. Am. J. Infect. Control 2022, 50, 126–132. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Phase | Performed | Not Performed |
|---|---|---|
| Pre-cleaning is performed immediately after the procedure | X | |
| The endoscope is cleaned externally using sponge or lint-free cloth soaked in detergent solution | X | |
| The endoscope is cleaned internally with the detergent solution aspirated through all the channels until it is macroscopically cleaned. | X | |
| The dirty endoscope is transported to the reprocessing room in the recommended time | X | |
| The dirty endoscope is transported using a container that is completely closed, resistant to punctures, and labeled to indicate biohazard | X | |
| Before cleaning, the leak test is performed | X | |
| The detergent solution indicated by the manufacturer is used and the contact times is respected | X | |
| Appropriately sized brushes are used as indicated by the manufacturer | X | |
| The brushes are passed in all channels, valves, and all removable parts of the instrument | X | |
| Brushes are disposable (or if reusable they are disinfected/sterilized after each use) | X | |
| Endoscope and all removable parts are rinsed and dried | X | |
| The high-level disinfection of the endoscopes is performed | X | |
| After high level disinfection, the internal channels are dried with compressed air for medical use | X | |
| The clean endoscope is transported to the storage room in a container completely closed, resistant to punctures | X | |
| The endoscope with valves removed are stored in a dedicated cabinet | X | |
| Each reprocessing steps is traced | X |
| First Phase | ||||||
|---|---|---|---|---|---|---|
| Bronchoscope Model | Age (Years) | Storage Condition | Sampling Date | Time after Disinfection (h) | Microorganism | Total Bacterial Count (CFU/Channels) |
| OLYMPUS BF TE (Routine testing) | 9 | Transport case | 19 November | 120 | NDM-K.pneumoniae, Staphylococcus spp. | 310 |
| OLYMPUS BF TE (Retesting for non-conformity) | 9 | Non-ventilated Cabinet | 27 November | 1 | NDM-K.pneumoniae, Staphylococcus spp. | 300 |
| PENTAX EB 1530 T3 (Routine testing) | 18 | Transport case | 27 November | 140 | E. gergoviae, Staphylococcus spp. | 300 |
| PENTAX FB 18 BS (Routine testing) | 6 | Transport case | 27 November | - | Proteus vulgaris | 1 |
| PENTAX FB15 BS (Routine testing) | 2 | Transport case | 27 November | 120 | S. aureus | 331 |
| FUJIFILM EB-530S (Routine testing) | 3 | Transport case | 27 November | 1 | Enterobacter gergoviae, Staphylococcus spp. | 11 |
| PENTAX EB 1530 T3 (Retesting for non-conformity) | 18 | Transport case | 5 December | 168 | S. multivorum | 304 |
| PENTAX FB 15 BS (Routine testing) | 3 | Transport case | 5 December | 144 | S. aureus | 302 |
| PENTAX FB 18 BS (Routine testing) | 6 | Transport case | 5 December | 120 | S. aureus | 3 |
| PENTAX FB 18 V (Retesting for non-conformity) | 6 | Transport case | 5 December | 48 | S. aureus | 2 |
| OLYMPUS BF 1T 180 (Routine testing) | 11 | Non-ventilated Cabinet | 5 December | 21 | P. aeruginosa, Providencia stuartii, S. maltophilia, Vibrio alginolyticus | 300 |
| PENTAX FB 18 V (Routine testing) | 6 | Non-ventilated Cabinet | 11 December | 24 | Proteus vulgaris | 4 |
| OLYMPUS BF 1T 180 (Routine testing) | 11 | Non-ventilated Cabinet | 11 December | 43 | S. aureus, Proteus penneri, S. paucimobilis | 300 |
| SECOND PHASE | ||||||
| PENTAX FB 18 BS (Routine testing) | 3 | Ventilated Cabinet | 2 March | 1 | Serratia spp. | 6 |
| OLYMPUS BF-1T180 (Retesting for non-conformity) | 15 | Ventilated Cabinet | 24 May | 48 | K. pneumoniae | 1 |
| PENTAX 19 TV (Retesting for non-conformity) | 10 | Ventilated Cabinet | 24 May | 72 | K. pneumonae | 1 |
| PENTAX 19 TV (Retesting for non-conformity) | 10 | Ventilated Cabinet | 28 May | 96 | A. lwoffii | 1 |
| OLYMPUS BF 1T180 (Retesting for non-conformity) | 15 | Ventilated Cabinet | 28 May | 3 | P. aeruginosa | 2 |
| PENTAX 18 V (Routine testing) | 11 | Ventilated Cabinet | 30 June | 24 | K.pneumoniae | 2 |
| PENTAX FB 15 BS (Routine testing) | 8 | Non-ventilated Cabinet | 30 June | 24 | P. aeruginosa | 21 |
| FUJIFILM EB-530S (Routine testing) | 3 | Ventilated Cabinet | 30 August | 48 | K. pneumoniae | 2 |
| PENTAX 18 P (Routine testing) | 17 | Ventilated Cabinet | 28 September | 24 | S.aureus | 20 |
| FUJIFILM EB-530T (Routine testing) | 3 | Ventilated Cabinet | 5 October | 96 | V. alginolyticus | 2 |
| STORZ 11301BNI (Routine testing) | 8 | Ventilated Cabinet | 19 October | 4 | P. penneri | 3 |
| FUJIFILM EB-530 US (Routine testing) | 1 | Ventilated Cabinet | 9 November | 4 | P. penneri | 10 |
| PENTAX FB 15 BS (Routine testing) | 8 | Ventilated Cabinet | 9 November | 4 | E. gergoviae | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuvo, B.; Scarpaci, M.; Cosci, T.; Ribechini, A.; Briani, S.; Luchini, G.; Totaro, M.; Baggiani, A.; Cristina, M.L.; Barnini, S.; et al. Adoption of Improved Reprocessing Decreased Microbiological Non-Compliance for Bronchoscopes. Int. J. Environ. Res. Public Health 2022, 19, 13978. https://doi.org/10.3390/ijerph192113978
Tuvo B, Scarpaci M, Cosci T, Ribechini A, Briani S, Luchini G, Totaro M, Baggiani A, Cristina ML, Barnini S, et al. Adoption of Improved Reprocessing Decreased Microbiological Non-Compliance for Bronchoscopes. International Journal of Environmental Research and Public Health. 2022; 19(21):13978. https://doi.org/10.3390/ijerph192113978
Chicago/Turabian StyleTuvo, Benedetta, Michela Scarpaci, Tommaso Cosci, Alessandro Ribechini, Silvia Briani, Grazia Luchini, Michele Totaro, Angelo Baggiani, Maria Luisa Cristina, Simona Barnini, and et al. 2022. "Adoption of Improved Reprocessing Decreased Microbiological Non-Compliance for Bronchoscopes" International Journal of Environmental Research and Public Health 19, no. 21: 13978. https://doi.org/10.3390/ijerph192113978