
Young Adult Carers in the UK—New Evidence from the UK Household Longitudinal Study

Abstract
:1. Introduction
2. Variations in Informal Care Provision
3. Materials and Methods
3.1. Study Population
3.2. Measures of Caregiving
3.3. Control Variables
3.4. Statistical Analysis
4. Results
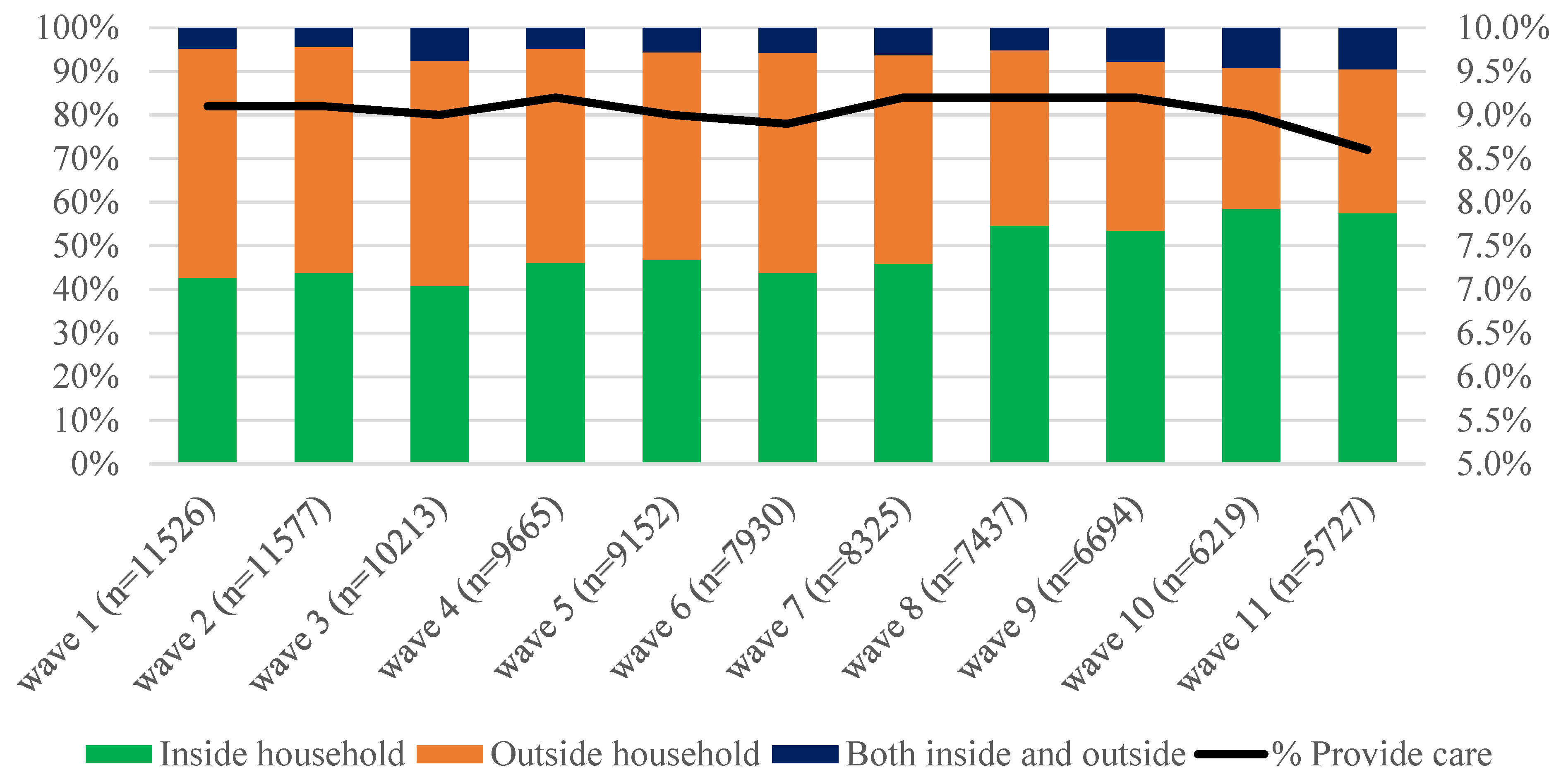
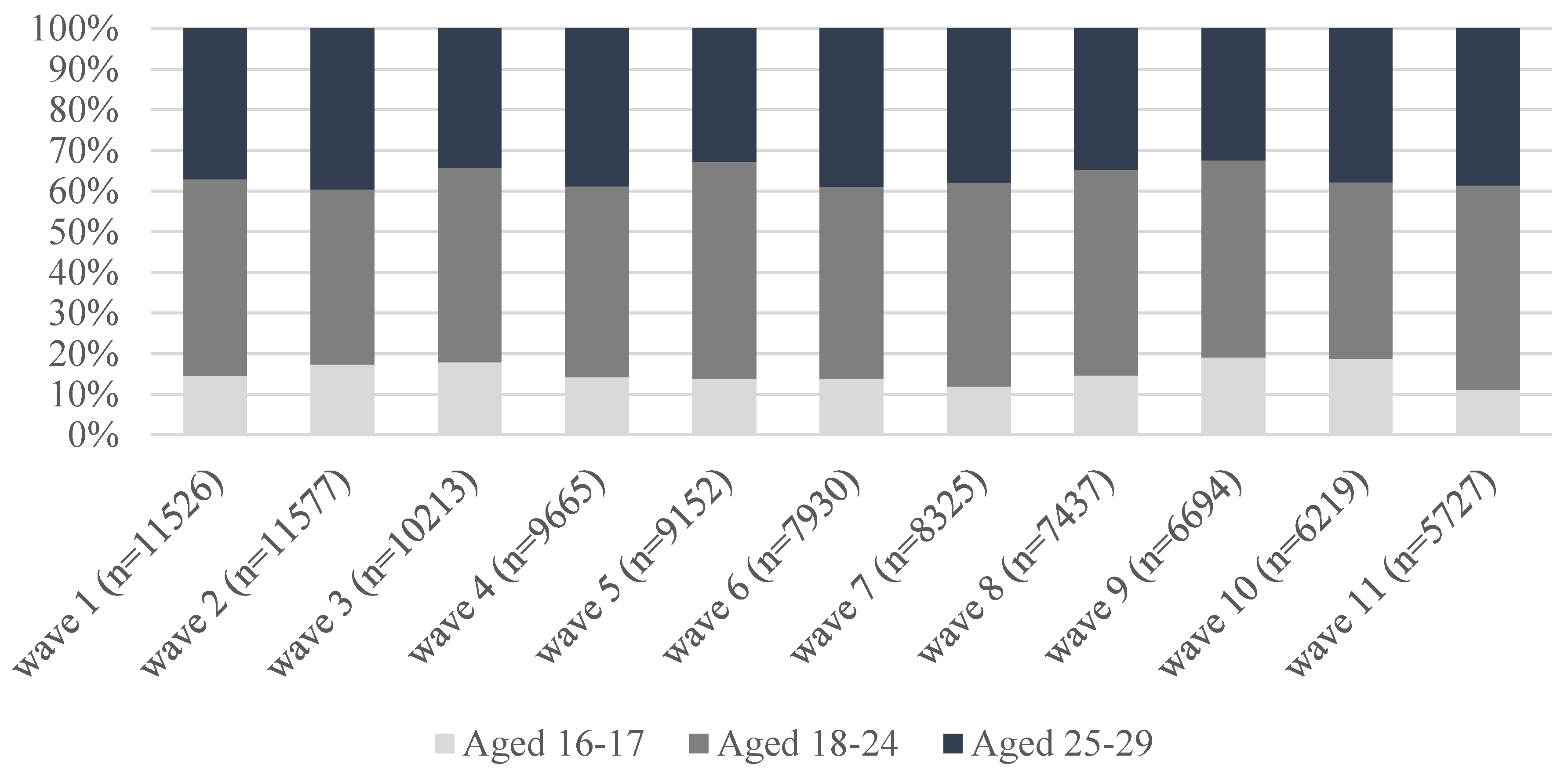
4.1. Trends of the Prevalence of Care among Young Adults Aged 16–29—Descriptive Findings
4.2. Associations between Demographic, Socioeconomic, Health Factors and Duration of Care
4.3. Caregiving Characteristics by Sex, Age Groups, and Urbanicity
5. Discussion
Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kavanaugh, M.S.; Stamatopoulos, V.; Cohen, D.; Zhang, L. Unacknowledged Caregivers: A Scoping Review of Research on Caregiving Youth in the United States. Adolesc. Res. Rev. 2016, 1, 29–49. [Google Scholar] [CrossRef] [Green Version]
- Brimblecombe, N.; Knapp, M.; King, D.; Stevens, M.; Cartagena Farias, J. The High Cost of Unpaid Care by Young People: Health and Economic Impacts of Providing Unpaid Care. BMC Public Health 2020, 20, 1115. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Sempik, J. Young Adult Carers: The Impact of Caring on Health and Education. Child. Soc. 2019, 33, 377–386. [Google Scholar] [CrossRef] [Green Version]
- Becker, S. Global Perspectives on Children’s Unpaid Caregiving in the Family: Research and Policy on ‘Young Carers’ in the UK, Australia, the USA and Sub-Saharan Africa. Glob. Soc. Policy 2007, 7, 23–50. [Google Scholar] [CrossRef] [Green Version]
- Nagl-Cupal, M.; Daniel, M.; Koller, M.M.; Mayer, H. Prevalence and Effects of Caregiving on Children. J. Adv. Nurs. 2014, 70, 2314–2325. [Google Scholar] [CrossRef]
- Murphy, M. Long-term Effects of the Demographic Transition on Family and Kinship Networks in Britain. Popul. Dev. Rev. 2011, 37 (Suppl. 1), 55–80. [Google Scholar] [CrossRef]
- Post, W.; van Poppel, F.; van Imhoff, E.; Kruse, E. Reconstructing the Extended Kin-network in the Netherlands with Genealogical Data: Methods, Problems, and Results. Popul. Stud. 1997, 51, 263–278. [Google Scholar] [CrossRef]
- Margolis, R.; Wright, L. Healthy Grandparenthood: How Long Is It, and How Has It Changed? Demography 2017, 54, 2073–2099. [Google Scholar] [CrossRef]
- Beaujouan, É.; Toulemon, L. European Countries with Delayed Childbearing Are Not Those with Lower Fertility. Genus 2021, 77, 2. [Google Scholar] [CrossRef]
- McMunn, A.; Lacey, R.; Webb, E. Life Course Partnership and Employment Trajectories and Parental Caregiving at Age 55: Prospective Findings from a British Birth Cohort Study. Longitud. Life Course Stud. 2020, 11, 495–518. [Google Scholar] [CrossRef]
- Pasqualini, M.; Di Gessa, G.; Tomassini, C. A Change Is (Not) Gonna Come: A 20-year Overview of Italian Grandparent–Grandchild exchanges. Genus 2021, 77, 33. [Google Scholar] [CrossRef]
- Glaser, K.; Stuchbury, R.; Price, D.; Di Gessa, G.; Ribe, E.; Tinker, A. Trends in the Prevalence of Grandparents Living with Grandchild(ren) in Selected European Countries and the United States. Eur. J. Ageing 2018, 15, 237–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leu, A.; Frech, M.; Wepf, H.; Sempik, J.; Joseph, S.; Helbling, L.; Moser, U.; Becker, S.; Jung, C. Counting Young Carers in Switzerland—A Study of Prevalence. Child. Soc. 2019, 33, 53–67. [Google Scholar] [CrossRef] [Green Version]
- Hunt, G.; Levine, C.; Naiditch, L. Young Caregivers in the U.S.: Findings from a National Survey; National Alliance for Caregiving and the United Hospital Fund: Bethesda, MD, USA, 2005. [Google Scholar]
- Australian Bureau of Statistics. Young Carers; Australian Bureau of Statistics: Canberra, Australia, 2018.
- Stamatopoulos, V. One Million and Counting: The Hidden Army of Young Carers in Canada. J. Youth Stud. 2015, 18, 809–822. [Google Scholar] [CrossRef]
- Kelly, G.; Devine, P.; McKnight, M. Lost in Translation? The Challenges of Measuring Informal Care Among Children and Young People. Int. J. Care Caring 2017, 1, 388–406. [Google Scholar] [CrossRef] [Green Version]
- Leu, A.; Becker, S. Young Carers. In Oxford Bibliographies in Childhood Studies; Montgomery, H., Ed.; Oxford University Press: Oxford, UK, 2019. [Google Scholar] [CrossRef]
- van Groenou, M.I.B.; De Boer, A. Providing Informal Care in a Changing Society. Eur. J. Ageing 2016, 13, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.M.; Sousa-Poza, A. Impacts of Informal Caregiving on Caregiver Employment, Health, and Family. J. Popul. Ageing 2015, 8, 113–145. [Google Scholar] [CrossRef] [Green Version]
- Brouwer, W.B.F.; Exel, N.J.A.V.; Berg, B.V.D.; Bos, G.A.M.V.D.; Koopmanschap, M.A. Process Utility from Providing Informal Care: The Benefit of Caring. Health Policy 2005, 74, 85–99. [Google Scholar] [CrossRef]
- Carmichael, F.; Charles, S.; Hulme, C. Who Will Care? Employment Participation and Willingness to Supply Informal Care. J. Health Econ. 2010, 29, 182–190. [Google Scholar] [CrossRef]
- Rand, S.; Malley, J.; Forder, J. Are Reasons for Care-giving Related to Carers’ Care-related Quality of Life and Strain? Evidence From a Survey of Carers in England. Health Soc. Care Community 2019, 27, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Stöckel, J.; Bom, J. Revisiting Longer-term Health Effects of Informal Caregiving: Evidence From the UK. J. Econ. Ageing 2022, 21, 100343. [Google Scholar] [CrossRef]
- ONS. Milestones: Journeying into Adulthood; Office for National Statistics: London, UK, 2019.
- Hamilton, M.; Cass, B. Capturing the Centrality of Age and Life-course Stage in the Provision of Unpaid Care. J. Sociol. 2017, 53, 79–93. [Google Scholar] [CrossRef]
- Craig, L.; Mullan, K. How Mothers and Fathers Share Childcare:A Cross-National Time-Use Comparison. Am. Sociol. Rev. 2011, 76, 834–861. [Google Scholar] [CrossRef] [Green Version]
- McMunn, A.; Bird, L.; Webb, E.; Sacker, A. Gender Divisions of Paid and Unpaid Work in Contemporary UK Couples. Work Employ. Soc. 2020, 34, 155–173. [Google Scholar] [CrossRef]
- Di Gessa, G.; Zaninotto, P.; Glaser, K. Looking After Grandchildren: Gender Differences in ‘When’,’What’, and ‘Why’: Evidence from the English Longitudinal Study of Ageing. Demogr. Res. 2020, 43, 1545–1562. [Google Scholar] [CrossRef]
- Evertsson, M. Gender Ideology and the Sharing of Housework and Child Care in Sweden. J. Fam. Issues 2014, 35, 927–949. [Google Scholar] [CrossRef]
- Kühhirt, M. Childbirth and the Long-Term Division of Labour within Couples: How do Substitution, Bargaining Power, and Norms affect Parents’ Time Allocation in West Germany? Eur. Sociol. Rev. 2011, 28, 565–582. [Google Scholar] [CrossRef]
- Young, H.; Grundy, E.; Kalogirou, S. Who Cares? Geographic Variation in Unpaid Caregiving in England and Wales: Evidence from the 2001 Census. Popul. Trends 2005, 120, 23–34. [Google Scholar]
- Warren, D.; Edwards, B. Young carers. In Growing Up in Australia. The Longitudinal Study of Australian Children Annual Statistical Report 2016; Australian Institute of Family Studies: Melbourne, Australia, 2017; pp. 85–118. [Google Scholar]
- Arber, S.; Ginn, J. Gender Differences in Informal Caring. Health Soc. Care Community 1995, 3, 19–31. [Google Scholar] [CrossRef]
- Cohen, S.A.; Ahmed, N.; Brown, M.J.; Meucci, M.R.; Greaney, M.L. Rural-urban Differences in Informal Caregiving and Health-related Quality of Life. J. Rural. Health 2022, 38, 442–456. [Google Scholar] [CrossRef]
- Being a Young Carer in Rural England: Summary Report; Commission for Rural Communities: Cheltenham, UK, 2012.
- University of Essex. Understanding Society: Waves 1–11, 2009–2020 and Harmonised BHPS: Waves 1–18, 1991–2009: Special Licence Access; UK Data Service: Institute for Social and Economic Research: Colchester, UK, 2022. [Google Scholar] [CrossRef]
- Young, H.; Grundy, E.; Jitlal, M. Care Providers, Care Receivers: A Longitudinal Perspective; Joseph Rowntree Foundation: York, UK, 2006. [Google Scholar]
- Fruhauf, C.A.; Orel, N.A. Developmental Issues of Grandchildren Who Provide Care to Grandparents. Int. J. Aging Hum. Dev. 2008, 67, 209–230. [Google Scholar] [CrossRef]
- Dellmann-Jenkins, M.; Blankemeyer, M.; Pinkard, O. Young Adult Children and Grandchildren in Primary Caregiver Roles to Older Relatives and Their Service Needs. Fam. Relat. 2000, 49, 177–186. [Google Scholar] [CrossRef]
- Maclean, C.; Hay, N. Young, Caring and Struggling to Make Ends Meet: The Worsening Economic Circumstances of Scotland’s Young Carers; UWS-Oxfam Partnership: Paisley, Scotland, 2021. [Google Scholar]
- Vizard, P.; Obolenskaya, P.; Burchardt, T. Child Poverty Amongst Young Carers in the UK: Prevalence and Trends in the Wake of the Financial Crisis, Economic Downturn and Onset of Austerity. Child Indic. Res. 2019, 12, 1831–1854. [Google Scholar] [CrossRef] [Green Version]
- Zygouri, I.; Cowdell, F.; Ploumis, A.; Gouva, M.; Mantzoukas, S. Gendered Experiences of Providing Informal Care for Older People: A Systematic Review and Thematic Synthesis. BMC Health Serv. Res. 2021, 21, 730. [Google Scholar] [CrossRef] [PubMed]
- Becker, F.; Becker, S. Young Adult Carers in the UK; Princess Royal Trust for Carers: London, UK, 2008. [Google Scholar]
- Grundy, E.; Murphy, M.; Shelton, N. Looking Beyond the Household: Intergenerational Perspectives on Living Kin and Contacts with Kin in Great Britain. Popul. Trends 1999, 97, 19–27. [Google Scholar]
- Dearden, C.N.; Becker, S. Growing Up Caring: Vulnerability and Transition to Adulthood: Young Carers’ Experiences; Youth Work Press: Leicester, UK, 2000. [Google Scholar]

{kind=link}
{kind=link}
| Non-Carer (N = 11277) | Cared Once (N = 1573) | Care for 2+ Waves (N = 1612) | p Value | |
|---|---|---|---|---|
| Age when first observed | ||||
| 16–17 | 37.8 | 40.5 | 35.3 | <0.001 |
| 18–24 | 35.1 | 42.2 | 43.6 | |
| 25–29 | 27.1 | 17.3 | 21.2 | |
| Mean | 20.84 | 20.05 | 20.56 | <0.001 |
| Sex | ||||
| Male | 52.9 | 50.0 | 42.4 | <0.001 |
| Female | 47.1 | 50.0 | 57.6 | |
| Ethnicity | ||||
| White | 89.0 | 86.8 | 86.9 | <0.001 |
| Black | 3.3 | 3.9 | 3.0 | |
| Indian | 2.3 | 3.3 | 2.3 | |
| Pakistani/Bangladeshi | 2.4 | 3.7 | 5.8 | |
| Other Asian | 2.9 | 2.3 | 2.0 | |
| Marital status | ||||
| Married | 8.4 | 6.1 | 7.8 | <0.001 |
| Cohabiting | 15.5 | 10.9 | 14.3 | |
| Single | 76.2 | 83.0 | 78.0 | |
| Place of Living | ||||
| Rural Area | 21.4 | 20.4 | 16.7 | 0.011 |
| Urban Area | 78.6 | 79.6 | 83.3 | |
| HH income quintiles | ||||
| 1 (lowest) | 16.8 | 23.8 | 26.6 | <0.001 |
| 2 | 19.1 | 24.1 | 24.3 | |
| 3 | 21.5 | 18.0 | 23.4 | |
| 4 | 23.5 | 19.4 | 16.2 | |
| 5 (highest) | 19.2 | 14.7 | 9.6 | |
| Occupation class | ||||
| Management/Professional | 14.9 | 9.5 | 8.6 | <0.001 |
| Intermediate | 9.4 | 7.5 | 7.1 | |
| Routine/manual | 19.0 | 20.6 | 20.9 | |
| Not working | 56.7 | 62.4 | 63.5 | |
| Parental occupational class (at age 14) | ||||
| Management/Professional | 44.2 | 36.9 | 25.4 | <0.001 |
| Intermediate | 22.5 | 20.4 | 19.3 | |
| Routine/manual | 24.0 | 25.6 | 29.9 | |
| Not working | 8.8 | 16.5 | 25.1 | |
| Not in household | 0.5 | 0.6 | 0.4 | |
| Self-reported health | ||||
| Excellent | 25.1 | 21.3 | 19.3 | <0.001 |
| Very good | 41.1 | 38.8 | 34.1 | |
| Good | 25.2 | 27.9 | 32.8 | |
| Fair/poor | 8.6 | 12.0 | 13.8 | |
| Physical health | ||||
| No long-standing illness | 85.0 | 80.8 | 74.6 | <0.001 |
| With long-standing illness | 15.0 | 19.2 | 25.4 |
| OR | p-Value | 95% CI | ||
|---|---|---|---|---|
| Age: 16–17 | Ref | |||
| 18–24 | 1.14 | 0.078 | 0.99 | 1.31 |
| 25–29 | 0.70 | 0.001 | 0.57 | 0.87 |
| Sex: Male | Ref | |||
| Female | 1.24 i | <0.001 | 1.10 | 1.38 |
| 1.42 ii | <0.001 | 1.22 | 1.64 | |
| Ethnicity: White | Ref | |||
| Black | 0.89 | 0.368 | 0.68 | 1.15 |
| Indian | 1.30 | 0.121 | 0.93 | 1.81 |
| Pakistani/Bangladeshi | 1.46 | 0.011 | 1.09 | 1.97 |
| Other Asian | 0.74 | 0.093 | 0.52 | 1.05 |
| Marital status: Married | Ref | |||
| Cohabiting | 0.95 | 0.670 | 0.73 | 1.22 |
| Single | 1.08 | 0.513 | 0.86 | 1.36 |
| Place of Living: Rural Area | Ref | |||
| Urban Area | 0.92 | 0.305 | 0.78 | 1.08 |
| Household income quintiles | ||||
| 1 (lowest) | 1.56 | <0.001 | 1.23 | 1.98 |
| 2 | 1.55 | <0.001 | 1.24 | 1.93 |
| 3 | 1.29 | 0.028 | 1.03 | 1.61 |
| 4 | 1.11 | 0.349 | 0.89 | 1.38 |
| 5 (highest) | Ref | |||
| Occupation class | ||||
| Management/Professional | Ref | |||
| Intermediate | 1.08 | 0.611 | 0.81 | 1.43 |
| Routine/manual | 1.36 | 0.013 | 1.07 | 1.73 |
| Not working | 1.22 | 0.106 | 0.96 | 1.55 |
| Parental occupational class (at age 14) | ||||
| Management/Professional | Ref | |||
| Intermediate | 1.15 i | 0.111 | 0.97 | 1.37 |
| 1.38 ii | 0.005 | 1.10 | 1.72 | |
| Routine/manual | 1.40 i | <0.001 | 1.20 | 1.65 |
| 1.81 ii | <0.001 | 1.46 | 2.24 | |
| Not working | 2.68 i | <0.001 | 2.18 | 3.29 |
| 3.42 ii | <0.001 | 2.67 | 4.37 | |
| Not in household | 1.14 i | 0.724 | 0.56 | 2.30 |
| 1.00 ii | 0.997 | 0.42 | 2.38 | |
| Self-reported health: Excellent | Ref | |||
| Very good | 1.03 | 0.742 | 0.87 | 1.21 |
| Good | 1.28 | 0.004 | 1.08 | 1.52 |
| Fair/poor | 1.33 | 0.013 | 1.06 | 1.67 |
| Physical health: | ||||
| No long-standing illness | Ref | |||
| With long-standing illness | 1.46 | <0.001 | 1.26 | 1.69 |
| Carers n = 3185 | Male n = 1332 | Female n = 1853 | p Value | 16/17 n = 1246 | 18/24 n = 1333 | 25/29 n = 606 | p Value | Urban n = 2668 | Rural n = 517 | p Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weekly hours | |||||||||||
| 0–4 | 50.2 | 57.1 | 44.2 | <0.001 | 55.5 | 48.2 | 44.0 | <0.001 | 48.4 | 57.8 | 0.026 |
| 5–9 | 20.0 | 18.7 | 21.1 | 20.4 | 20.9 | 17.3 | 20.3 | 19.0 | |||
| 10 to 19 | 14.4 | 13 | 15.7 | 13.8 | 14.4 | 15.6 | 14.8 | 12.6 | |||
| 20–34 | 7.2 | 6.1 | 8.1 | 5.0 | 7.6 | 10.6 | 7.6 | 5.4 | |||
| 35 or more | 8.2 | 5.1 | 10.8 | 5.2 | 8.8 | 12.6 | 8.8 | 5.2 | |||
| N of people | |||||||||||
| 1 | 91.6 | 93.1 | 90.4 | 0.087 | 91.9 | 93.3 | 87.3 | 0.002 | 91.7 | 91.3 | 0.231 |
| 2 | 7.2 | 6.2 | 8.1 | 6.3 | 5.9 | 12.1 | 7.3 | 6.8 | |||
| 3 or more | 1.1 | 0.7 | 1.5 | 1.8 | 0.8 | 0.6 | 0.9 | 1.9 | |||
| Years of care | |||||||||||
| 1 | 49.2 | 53.3 | 45.6 | 0.003 | 52.6 | 48.3 | 44.2 | 0.169 | 48.0 | 54.2 | 0.232 |
| 2 | 21.5 | 22.4 | 20.8 | 22.1 | 21.3 | 20.8 | 22.0 | 19.5 | |||
| 3 | 12.9 | 10.4 | 14.9 | 11.8 | 13 | 14.7 | 13.3 | 10.9 | |||
| 4 or more | 16.4 | 13.9 | 18.6 | 13.4 | 17.4 | 20.3 | 16.7 | 15.4 | |||
| Age care onset | |||||||||||
| 16/17 | 21.2 | 22.6 | 20.1 | 0.406 | 56.1 | 0.0 | 0.0 | <0.001 | 20.2 | 25.9 | 0.240 |
| 18/19 | 13.6 | 14 | 13.2 | 22.6 | 11.7 | 0.0 | 13.4 | 14.2 | |||
| 20/21 | 13.2 | 13.8 | 12.6 | 13.5 | 18.7 | 0.0 | 13.7 | 10.9 | |||
| 22/23 | 11.8 | 11.4 | 12.3 | 5.3 | 22.9 | 0.0 | 11.8 | 12.1 | |||
| 24/25 | 13.5 | 14.2 | 12.8 | 2.3 | 24.2 | 11.4 | 13.7 | 12.2 | |||
| 26/27 | 12.4 | 11.9 | 12.7 | 0.1 | 13.5 | 34.0 | 13.1 | 9.2 | |||
| 28/29 | 14.4 | 12.1 | 16.3 | 0.0 | 9.0 | 54.6 | 14.1 | 15.5 | |||
| Care recipient | |||||||||||
| Parent | 41.5 | 42.2 | 40.8 | 0.588 | 40.2 | 40.3 | 46.6 | 0.229 | 42.5 | 37.0 | 0.147 |
| Grandparent | 40.5 | 41.3 | 39.8 | 0.559 | 43.3 | 40.7 | 34.3 | 0.09 | 39.7 | 43.7 | 0.279 |
| Partner | 4.7 | 4.4 | 4.9 | 0.636 | 1.3 | 5.8 | 8.6 | <0.001 | 4.6 | 4.7 | 0.955 |
| Sibling | 6.6 | 7.7 | 5.8 | 0.056 | 12.6 | 3.8 | 1.3 | <0.001 | 7.0 | 5.2 | 0.207 |
| Child | 5.5 | 2.9 | 7.6 | <0.001 | 0.8 | 7.0 | 11.2 | <0.001 | 5.5 | 5.3 | 0.896 |
| Other kin | 9.8 | 7.4 | 11.8 | 0.001 | 7.8 | 8.7 | 16.0 | <0.001 | 10.1 | 8.3 | 0.373 |
| Non-relative | 15.9 | 16.0 | 15.9 | 0.991 | 16.3 | 15.4 | 16.5 | 0.258 | 14.8 | 20.9 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Gessa, G.; Xue, B.; Lacey, R.; McMunn, A. Young Adult Carers in the UK—New Evidence from the UK Household Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 14076. https://doi.org/10.3390/ijerph192114076
Di Gessa G, Xue B, Lacey R, McMunn A. Young Adult Carers in the UK—New Evidence from the UK Household Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(21):14076. https://doi.org/10.3390/ijerph192114076
Chicago/Turabian StyleDi Gessa, Giorgio, Baowen Xue, Rebecca Lacey, and Anne McMunn. 2022. "Young Adult Carers in the UK—New Evidence from the UK Household Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 21: 14076. https://doi.org/10.3390/ijerph192114076