
The Effects of Cognitive Behavioral Therapy for Insomnia among College Students with Irritable Bowel Syndrome: A Randomized Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Randomization
2.3. Sample Size Calculation
2.4. Intervention
2.5. Primary Outcomes
Insomnia Severity
2.6. Secondary Outcomes
2.6.1. Sleeping Pattern
2.6.2. GI Symptoms during Sleep
2.6.3. Pre-Sleep Arousal
2.6.4. Sleep-Related Dysfunctional Cognitions
2.6.5. Maladaptive Sleep Habits
2.6.6. Inflammation
2.6.7. Severity of IBS Symptoms
2.6.8. IBS Quality of Life
2.6.9. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. General Characteristics of Participants and the Pre-Test for Homogeneity
3.2. Primary Hypothesis Test
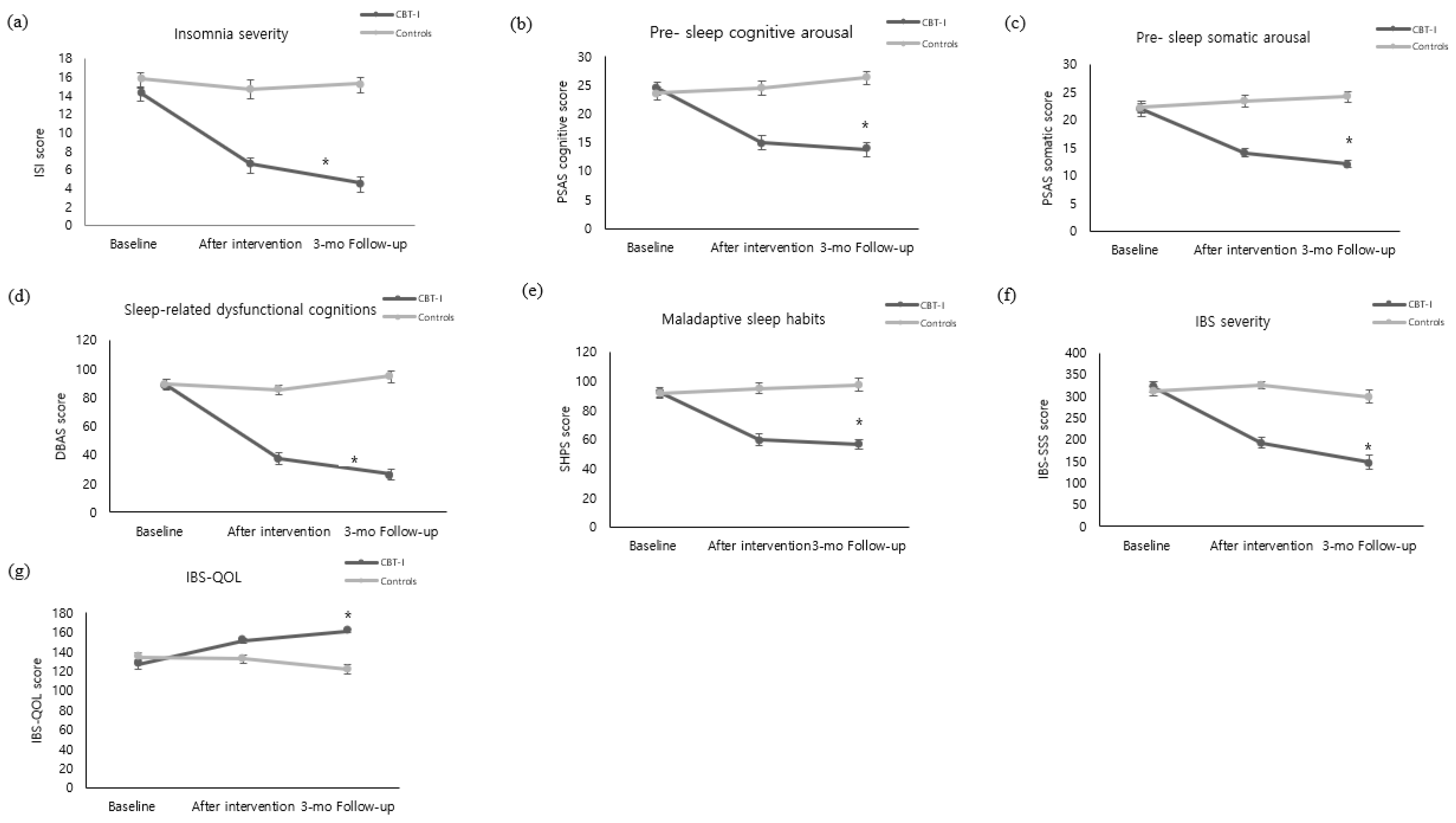
Insomnia Severity
3.3. Secondary Hypothesis Test
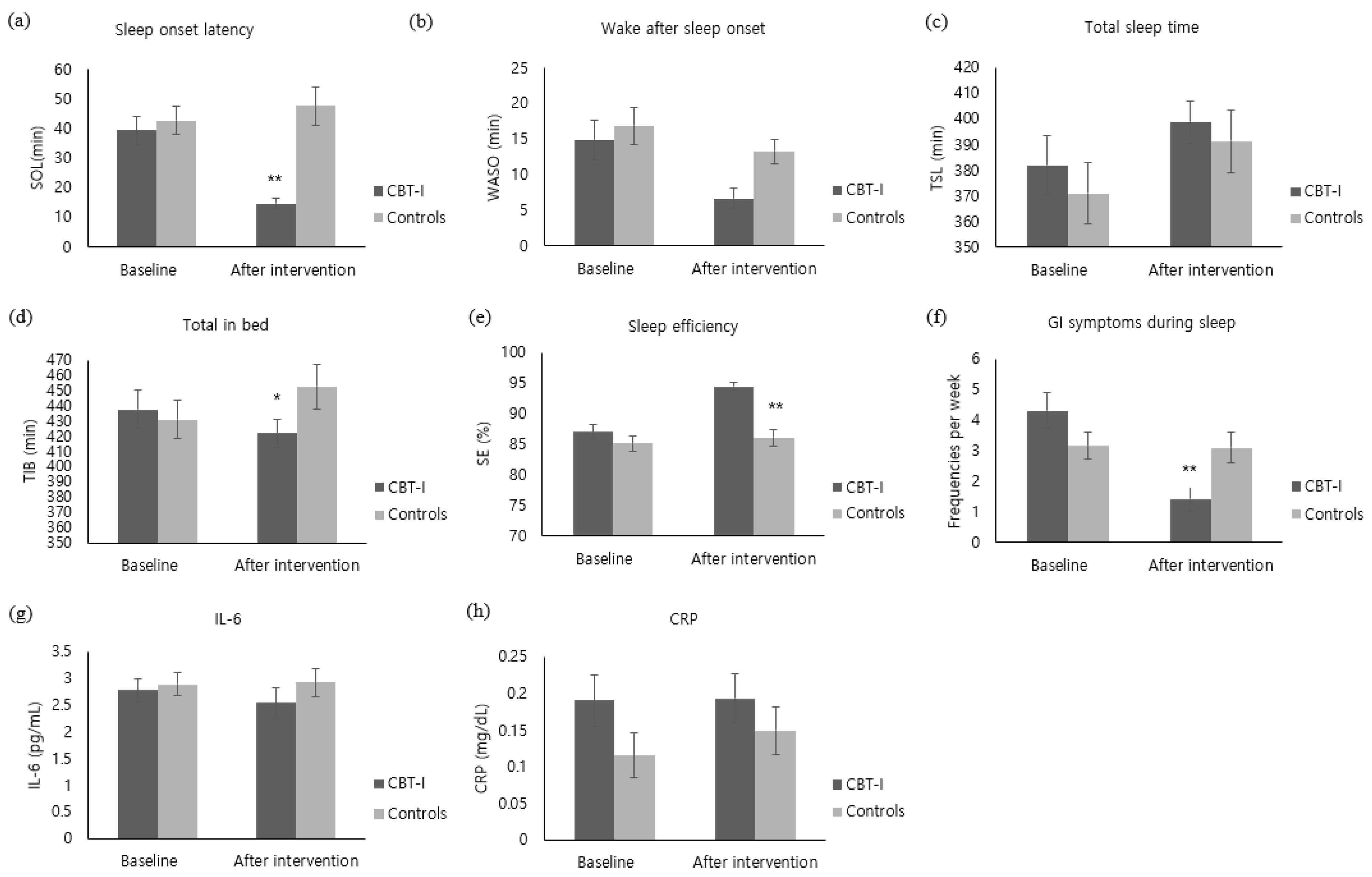
3.3.1. Sleeping Patterns and GI Symptoms during Sleep
3.3.2. Pre-Sleep Arousal
3.3.3. Sleep-Related Dysfunctional Cognitions
3.3.4. Maladaptive Sleep Habits
3.3.5. Inflammation
3.3.6. Severity of IBS Symptoms
3.3.7. IBS Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Drossman, D.A. The Functional Gastrointestinal Disorders and the Rome III Process. Gastroenterology 2006, 130, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Canavan, C.; West, J.; Card, T. The epidemiology of irritable bowel syndrome. Clin. Epidemiol. 2014, 6, 71. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Liu, L.; Yang, Y.; He, Y.; Zhang, Y.; Wang, M.; Chen, S.; Yao, S. A School-Based Study of Irritable Bowel Syndrome in Medical Students in Beijing, China: Prevalence and Some Related Factors. Gastroenterol. Res. Pract. 2014, 2014, 124261. [Google Scholar] [CrossRef] [Green Version]
- Shiotani, A.; Miyanishi, T.; Takahashi, T. Sex differences in irritable bowel syndrome in Japanese university students. J. Gastroenterol. 2006, 41, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Tu, Q.; Heitkemper, M.M.; Jarrett, M.E.; Buchanan, D.T. Sleep disturbances in irritable bowel syndrome: A systematic review. Neurogastroenterol. Motil. 2017, 29, e12946. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-Y.; Jun, S. Prevalence and Associated Factors of Insomnia in College Students with Irritable Bowel Syndrome. Korean J. Adult Nurs. 2018, 30, 235–244. [Google Scholar] [CrossRef]
- Duan, L.; Wang, B.; Duan, R. Prevalence of sleep disorder in irritable bowel syndrome: A systematic review with meta-analysis. Saudi J. Gastroenterol. 2018, 24, 141–150. [Google Scholar] [CrossRef]
- Miglis, M.G. Autonomic dysfunction in primary sleep disorders. Sleep Med. 2016, 19, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Tobaldini, E.; Costantino, G.; Solbiati, M.; Cogliati, C.; Kara, T.; Nobili, L.; Montano, N. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci. Biobehav. Rev. 2017, 74, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Chrousos, G.P. Sleep, the hypothalamic–pituitary–adrenal axis, and cytokines: Multiple interactions and dis-turbances in sleep disorders. Endocrinol. Metab. Clin. 2002, 31, 15–36. [Google Scholar] [CrossRef]
- Kim, M. Applying cognitive behavioral therapy to the treatment of insomnia. Korean J. Health Psychol. 2010, 15, 601–615. [Google Scholar]
- Parthasarathy, S.; Vasquez, M.M.; Halonen, M.; Bootzin, R.; Quan, S.F.; Martinez, F.D.; Guerra, S. Persistent Insomnia is Associated with Mortality Risk. Am. J. Med. 2015, 128, 268–275.e2. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.T.; Huang, M.I.; Manber, R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin. Psychol. Rev. 2005, 25, 559–592. [Google Scholar] [CrossRef] [PubMed]
- Song, G.H.; Leng, P.H.; Gwee, K.A.; Moochhala, S.M.; Ho, K.Y. Melatonin improves abdominal pain in irritable bowel syndrome patients who have sleep disturbances: A random-ised, double blind, placebo controlled study. Gut 2005, 54, 1402–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarrett, M.E.; Cain, K.C.; Burr, R.L.; Hertig, V.L.; Rosen, S.N.; Heitkemper, M.M. Comprehensive self-management for irritable bowel syndrome: Randomized trial of in-person vs. combined in-person and telephone sessions. Am. J. Gastroenterol. 2009, 104, 3004. [Google Scholar] [CrossRef] [Green Version]
- Ljótsson, B.; Hesser, H.; Andersson, E.; Lindfors, P.; Hursti, T.; Rück, C.; Lindefors, N.; Andersson, G.; Hedman, E. Mechanisms of change in an exposure-based treatment for irritable bowel syndrome. J. Consult. Clin. Psychol. 2013, 81, 1113. [Google Scholar] [CrossRef] [PubMed]
- Morgenthaler, T.; Kramer, M.; Aless, C.; Friedman, L.; Boehlecke, B.; Brown, T.; Coleman, J.; Kapur, V.; Lee-Chiong, T.; Owens, J.; et al. Practice parameters for the psychological and behavioral treatment of insomnia: An update. An American Academy of Sleep Medicine report. Sleep 2006, 29, 1415–1419. [Google Scholar] [CrossRef] [Green Version]
- Morin, C.M. Cognitive-behavioral approaches to the treatment of insomnia. J. Clin. Psychiatry 2004, 65 (Suppl. 16), 33–40. [Google Scholar] [PubMed]
- Pigeon, W.R.; Moynihan, J.; Matteson-Rusby, S.; Jungquist, C.R.; Xia, Y.; Tu, X.; Perlis, M.L. Comparative effectiveness of CBT interventions for co-morbid chronic pain & insomnia: A pilot study. Behav. Res. Ther. 2012, 50, 685–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitiello, M.V.; McCurry, S.M.; Shortreed, S.M.; Balderson, B.H.; Baker, L.D.; Keefe, F.J.; Rybarczyk, B.D.; Korff, M.V. Cognitive-behavioral treatment for comorbid insomnia and osteoarthritis pain in primary care: The lifestyles randomized controlled trial. J. Am. Geriatr. Soc. 2013, 61, 947–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCurry, S.M.; Shortreed, S.M.; Von Korff, M.; Balderson, B.H.; Baker, L.D.; Rybarczyk, B.D.; Vitiello, M.V. Who Benefits From CBT for Insomnia in Primary Care? Important Patient Selection and Trial Design Lessons from Longitudinal Results of the Lifestyles Trial. Sleep 2014, 37, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Orr, W.C.; Elsenbruch, S.; Harnish, M.J. Autonomic regulation of cardiac function during sleep in patients with irritable bowel syndrome. Am. J. Gastroenterol. 2000, 95, 2865–2871. [Google Scholar] [CrossRef] [PubMed]
- Ranjbaran, Z.; Keefer, L.; Farhadi, A.; Stepanski, E.; Sedghi, S.; Keshavarzian, A. Impact of sleep disturbances in inflammatory bowel disease. J. Gastroenterol. Hepatol. 2007, 22, 1748–1753. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geiger-Brown, J.M.; Rogers, V.E.; Liu, W.; Ludeman, E.M.; Downton, K.D.; Diaz-Abad, M. Cognitive behavioral therapy in persons with comorbid insomnia: A meta-analysis. Sleep Med. Rev. 2015, 23, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Spielman, A.J.; Saskin, P.; Thorpy, M.J. Treatment of Chronic Insomnia by Restriction of Time in Bed. Sleep 1987, 10, 45–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlis, M.L.; Perlis, M.L.; Jungquist, C.; Smith, M.T.; Posner, D. Cognitive Behavioral Treatment of Insomnia: A Session-by-Session Guide; Springer Science & Business Media: Berlin, Germany, 2006; Volume 1. [Google Scholar]
- Suh, S. Case Study Book of Cognitive-Behavioral Therapy for Insomnia; Sigma Press: Seoul, Korea, 2017. [Google Scholar]
- Tang, N.K.; Goodchild, C.E.; Salkovskis, P.M. Hybrid cognitive-behaviour therapy for individuals with insomnia and chronic pain: A pilot randomised controlled trial. Behav. Res. Ther. 2012, 50, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Jang, A.L.; Hwang, S.-K.; Kim, D.U. The effects of cognitive behavioral therapy in female nursing students with irritable bowel syndrome: A randomized trial. Eur. J. Gastroenterol. Hepatol. 2014, 26, 918–926. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Nicassio, P.M.; Mendlowitz, D.R.; Fussell, J.J.; Petras, L. The phenomenology of the pre-sleep state: The development of the pre-sleep arousal scale. Behav. Res. Ther. 1985, 23, 263–271. [Google Scholar] [CrossRef]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional Beliefs and Attitudes about Sleep (DBAS): Validation of a Brief Version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef]
- Yang, C.-M.; Lin, S.-C.; Hsu, S.-C.; Cheng, C.-P. Maladaptive Sleep Hygiene Practices in Good Sleepers and Patients with Insomnia. J. Health Psychol. 2010, 15, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bow-el syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrick, D.L.; Drossman, D.A.; Frederick, I.O.; Dicesare, J.; Puder, K.L. Quality of Life in Persons with Irritable Bowel Syndrome (Development and Validation of a New Measure). Dig. Dis. Sci. 1998, 43, 400–411. [Google Scholar] [CrossRef] [PubMed]
- Peoples, A.R.; Garland, S.N.; Perlis, M.L.; Savard, J.; Heckler, C.E.; Kamen, C.S.; Ryan, J.L.; Mustian, K.M.; Janelsins, M.C.; Peppone, L.J.; et al. Effects of cognitive behavioral therapy for insomnia and armodafinil on quality of life in cancer survivors: A ran-domized placebo-controlled trial. J. Cancer Surviv. 2017, 11, 401–409. [Google Scholar] [CrossRef]
- Becker, P.M. Insomnia: Prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr. Clin. 2006, 29, 855–870. [Google Scholar] [CrossRef]
- Espie, C.A.; Inglis, S.J.; Tessier, S.; Harvey, L. The clinical effectiveness of cognitive behaviour therapy for chronic insomnia: Implementation and evaluation of a sleep clinic in general medical practice. Behav. Res. Ther. 2001, 39, 45–60. [Google Scholar] [CrossRef]
- Morin, C.M.; Hauri, P.J.; Espie, C.A.; Spielman, A.J.; Buysse, D.J.; Bootzin, R.R. Nonpharmacologic Treatment of Chronic Insomnia. Sleep 1999, 22, 1134–1156. [Google Scholar] [CrossRef]
- Morin, C.; Blais, F.; Savard, J. Are changes in beliefs and attitudes about sleep related to sleep improvements in the treatment of insomnia? Behav. Res. Ther. 2002, 40, 741–752. [Google Scholar] [CrossRef]
- Carney, C.E.; Waters, W.F. Effects of a Structured Problem-Solving Procedure on Pre-Sleep Cognitive Arousal in College Students With Insomnia. Behav. Sleep Med. 2006, 4, 13–28. [Google Scholar] [CrossRef]
- Kim, E.S.; Cheong, K.J. A Comparative on the Effects of Mind-body Healing of Internal Organ Massage and Lactic Acid Bacteria for Irritable Bowel Syndrome. J. Holist. Mind Body Ther. 2015, 2, 1–20. [Google Scholar]
- Craske, M.G.; Wolitzky-Taylor, K.B.; Labus, J.; Wu, S.; Frese, M.; Mayer, E.A.; Naliboff, B.D. A cognitive-behavioral treatment for irritable bowel syndrome using interoceptive exposure to visceral sensations. Behav. Res. Ther. 2011, 49, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Song, M. Development and Effects of Cognitive Behavioral Therapy for Insomnia on Patients with Restless Legs Syndrome; Keimyung University: Taegu, Korea, 2018. [Google Scholar]
- Cain, K.C.; Headstrom, P.; Jarrett, M.E.; Motzer, S.A.; Park, H.; Burr, R.L.; Surawicz, C.M.; Heitkemper, M.M. Abdominal Pain Impacts Quality of Life in Women with Irritable Bowel Syndrome. Am. J. Gastroenterol. 2006, 101, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Medzhitov, R. Inflammation 2010: New Adventures of an Old Flame. Cell 2010, 140, 771–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.-Y.; Chiang, C.-K.; Wang, H.-H.; Hung, K.-Y.; Lee, Y.-J.; Peng, Y.-S.; Wu, K.-D.; Tsai, T.-J. Cognitive-Behavioral Therapy for Sleep Disturbance in Patients Undergoing Peritoneal Dialysis: A Pilot Randomized Controlled Trial. Am. J. Kidney Dis. 2008, 52, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Olmstead, R.; Breen, E.C.; Witarama, T.; Carrillo, C.; Sadeghi, N.; Arevalo, J.M.; Ma, J.; Nicassio, P.; Bootzin, R.; et al. Cognitive Behavioral Therapy and Tai Chi Reverse Cellular and Genomic Markers of Inflammation in Late-Life Insomnia: A Randomized Controlled Trial. Biol. Psychiatry 2015, 78, 721–729. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Themes and Objectives | Contents |
|---|---|
| Session 1. Understanding and improving the environment and behaviors that disturb sleep | |
| Improving maladaptive sleep habits | ▸ Sleep education for understanding insomnia and IBS |
| ▸ Sleep hygiene education for IBS | |
| Improving GI symptoms during sleep | ▸ Relaxation training for IBS |
| Session 2. Improving the thoughts and behaviors that disturb sleep | |
| Improving sleep-related dysfunctional cognitions | ▸ Cognitive therapy for sleep-related dysfunctional cognitions |
| Improving maladaptive sleep habits | ▸ Sleep compression and stimulus control for IBS |
| Session 3. Improving the thoughts and behaviors about GI symptoms that disturb sleep | |
| Improving pre-sleep hyper-arousal | ▸ Cognitive therapy for dysfunctional cognitions about GI symptoms during sleep |
| ▸ Creating buffer zone and setting a time for worries for IBS | |
| Improving the GI symptoms during sleep | ▸ Evening diet education for IBS |
| Session 4. Establishing plans for preventing reoccurrence and recapping the program | |
| Improving the sleep-related dysfunctional cognitions, maladaptive sleep habits, GI symptoms during sleep, pre-sleep hyper-arousal | ▸ Summary and identify sleep pattern change |
| ▸ Establishing the measure for reoccurrence and maintenance | |
| Characteristics | Categories | CBT-I (n = 29) | Controls (n = 30) | χ2/t | p |
|---|---|---|---|---|---|
| n (%) or Mean ± SD | n (%) or Mean ± SD | ||||
| Age (years) | 20.50 ± 3.31 | 20.42 ± 2.31 | 0.17 | 0.908 * | |
| Gender | Male | 3(10.3) | 4(13.3) | 0.13 | 1.00 † |
| woman | 26(89.7) | 26(86.7) | |||
| IBS subtypes | Diarrhea-predominant | 0(0.0) | 2(6.7) | 2.40 | 0.303 † |
| Constipation -predominant | 1(3.4) | 2(6.7) | |||
| Mixed | 28(96.6) | 26(86.7) | |||
| Smoking | Yes | 4(13.8) | 6(20.0) | 0.40 | 0.731 † |
| No | 25(86.2) | 24(80.0) | |||
| Drinking | Yes | 16(55.2) | 11(13.7) | 2.04 | 0.154 ‡ |
| No | 13(44.8) | 19(63.3) | |||
| Sleep partner | Yes | 6(20.7) | 11(36.7) | 1.84 | 0.252 ‡ |
| No | 23(79.3) | 19(63.3) | |||
| Night duty | Yes | 4(13.8) | 11(36.7) | 4.07 | 0.071 ‡ |
| No | 25(86.2) | 19(63.3) | |||
| Insomnia severity | 14.35 ± 3.37 | 15.83 ± 3.37 | 1.69 | 0.096 | |
| Sleeping pattern | Sleep onset latency (min) | 39.48 ± 26.01 | 42.80 ± 26.80 | −0.46 | 0.644 * |
| Wake time after sleep onset (min) | 14.90 ± 15.00 | 16.90 ± 14.49 | −0.75 | 0.452 * | |
| Total sleep time (min) | 382.00 ± 61.16 | 370.87 ± 65.58 | −0.68 | 0.503 | |
| Total time in bed (min) | 437.48 ± 67.48 | 431.00 ± 67.72 | −0.37 | 0.714 | |
| Sleep efficiency (%) | 87.07 ± 5.98 | 85.17 ± 6.96 | −1.12 | 0.265 | |
| Pre-sleep arousal | Cognitive | 24.45 ± 6.04 | 23.57 ± 6.29 | −0.55 | 0.585 |
| Somatic | 21.86 ± 6.10 | 22.33 ± 4.90 | 0.33 | 0.744 | |
| GI symptoms during sleep | 4.31 ± 3.15 | 3.17 ± 2.36 | −1.39 | 0.164 * | |
| Sleep-related dysfunctional cognitions | 89.00 ± 20.68 | 89.30 ± 18.66 | 0.06 | 0.954 | |
| Maladaptive sleep habits | 92.48 ± 18.47 | 91.40 ± 15.45 | −0.25 | 0.808 | |
| Inflammation | IL-6 (pg/mL) | 2.78 ± 1.13 | 2.89 ± 1.20 | −1.02 | 0.310 * |
| CRP (mg/dL) | 0.19 ± 0.19 | 0.12 ± 0.17 | −1.75 | 0.080 * | |
| IBS severity | 320.52 ± 63.18 | 312.50 ± 60.56 | −0.50 | 0.621 | |
| IBS QOL | 126.48 ± 25.94 | 134.73 ± 21.70 | 1.33 | 0.190 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.-Y.; Jun, S. The Effects of Cognitive Behavioral Therapy for Insomnia among College Students with Irritable Bowel Syndrome: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 14174. https://doi.org/10.3390/ijerph192114174
Yang Y-Y, Jun S. The Effects of Cognitive Behavioral Therapy for Insomnia among College Students with Irritable Bowel Syndrome: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(21):14174. https://doi.org/10.3390/ijerph192114174
Chicago/Turabian StyleYang, Yun-Yi, and Sangeun Jun. 2022. "The Effects of Cognitive Behavioral Therapy for Insomnia among College Students with Irritable Bowel Syndrome: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 21: 14174. https://doi.org/10.3390/ijerph192114174
APA StyleYang, Y.-Y., & Jun, S. (2022). The Effects of Cognitive Behavioral Therapy for Insomnia among College Students with Irritable Bowel Syndrome: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(21), 14174. https://doi.org/10.3390/ijerph192114174