
Spine Fragility Fracture Prediction Using TBS and BMD in Postmenopausal Women: A Bayesian Approach
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Diagnostic Concordance between the Two Tests
3.2. Diagnostic Accuracy Measurement of the TBS and LS-BMD in the Entire Sample of Women (Fracture Prevalence 8.67%)
3.3. Diagnostic Accuracy Measurement of TBS in the Women Who Tested Negative to LS-BMD (Fracture Prevalence of 5.05%)
3.4. Diagnostic Accuracy Measurement of LS-BMD in the Women Who Tested Negative to the TBS (Fracture Prevalence 4.60%)
3.5. Diagnostic Accuracy Measurement of the Entire Sample of Women (Fracture Prevalence 8.67%), Combining the Two Tests According to the “OR-Rule” (Fracture Prevalence 8.67%)
3.6. Diagnostic Accuracy Measurement of the Entire Sample of Women, Combining the Two Tests According to the “AND-Rule” (Fracture Prevalence 8.67%)
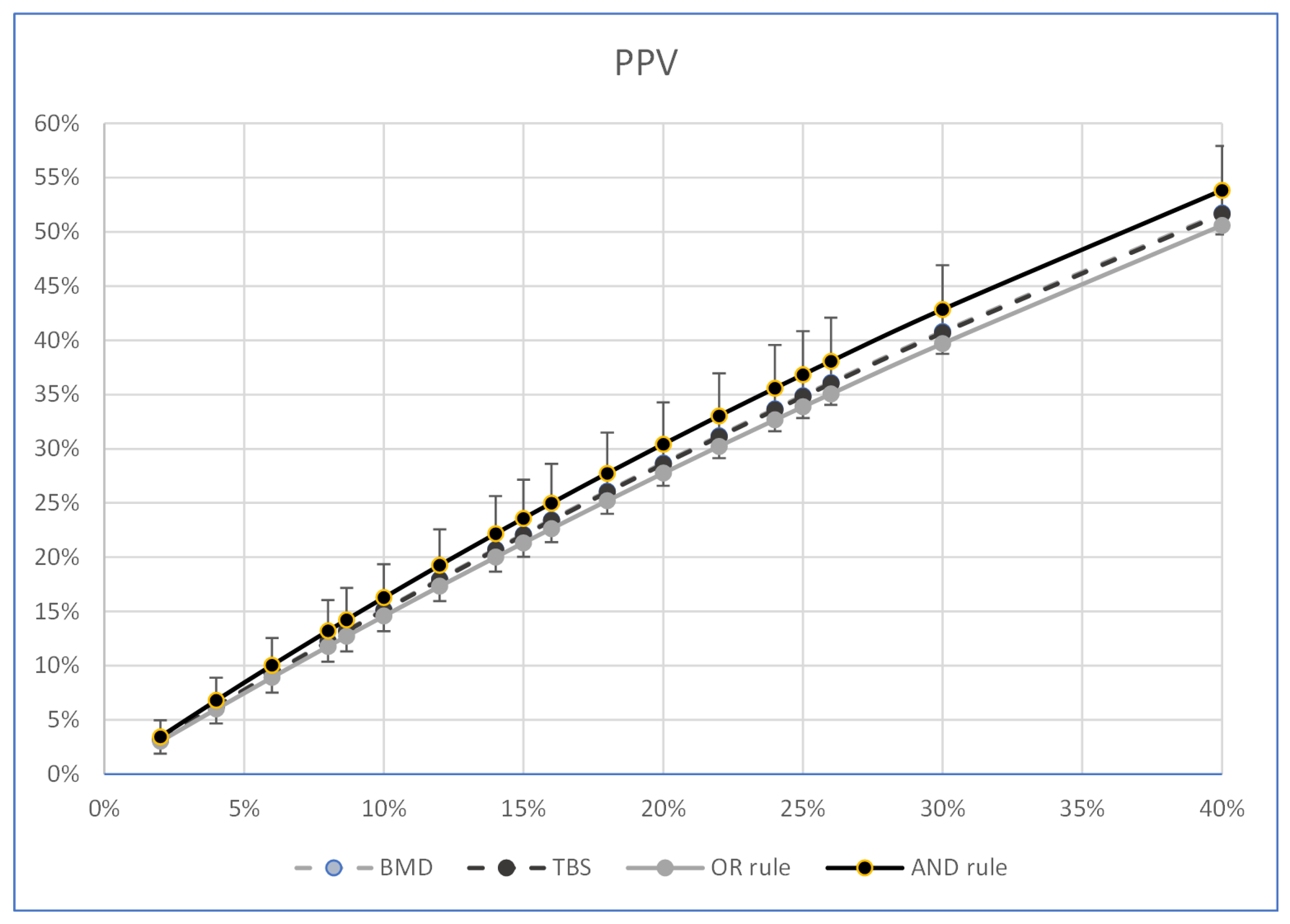
3.7. Calculation of the Post-Test Probability of Fracture at Different Percentages of the Pre-Test Probability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harvey, N.C.; Glüer, C.C.; Binkley, N.; McCloskey, E.V.; Brandi, M.L.; Cooper, C.; Kendler, D.; Lamy, O.; Laslop, A.; Camargos, B.M. Trabecular bone score (TBS) as a new complementary approach for osteoporosis evaluation in clinical practice. Bone 2015, 78, 216–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hans, D.; Barthe, N.; Boutroy, S.; Pothuaud, L.; Winzenrieth, R.; Krieg, M.A. Correlations between trabecular bone score, measured using anteroposterior dual-energy X-ray absorptiometry acquisition, and 3-dimensional parameters of bone microarchitecture: An experimental study on human cadaver vertebrae. J. Clin. Densitom. 2011, 14, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Winzenrieth, R.; Michelet, F.; Hans, D. Three-dimensional (3D) microarchitecture correlations with 2D projection image gray-level variations assessed by trabecular bone score using high-resolution computed tomographic acquisitions: Effects of resolution and noise. J. Clin. Densitom. 2013, 16, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Popp, A.; Hans, D.; Krieg, M.-A.; Perrelet, R.; Lippuner, K.; Meer, S. Bone mineral density (BMD) and vertebral trabecular bone score (TBS) for the identification of elderly women at high risk for fracture: The SEMOF cohort study. Eur. Spine J. 2016, 25, 3432–3438. [Google Scholar] [CrossRef] [PubMed]
- Hans, D.; Goertzen, A.L.; Krieg, M.A.; Leslie, W.D. Bone microarchitecture assessed by TBS predicts osteoporotic fractures independent of bone density: The Manitoba study. J. Bone Miner. Res. 2011, 26, 2762–2769. [Google Scholar] [CrossRef]
- Iki, M.; Tamaki, J.; Kadowaki, E.; Sato, Y.; Dongmei, N.; Winzenrieth, R.; Kagamimori, S.; Kagamimori, S.; Yoneshima, H. Trabecular bone score (TBS) predicts vertebral fractures in Japanese women over 10 years independently of bone density and prevalent vertebral deformity: The Japanese Population-Based Osteoporosis (JPOS) cohort study. J. Bone Miner. Res. 2014, 29, 399–407. [Google Scholar] [CrossRef]
- Briot, K.; Paternotte, S.; Kolta, S.; Eastell, R.; Reid, D.M.; Felsenberg, D.; Glüer, C.C.; Roux, C. Added value of trabecular bone score to bone mineral density for prediction of osteoporotic fractures in postmenopausal women: The OPUS study. Bone 2013, 57, 232–236. [Google Scholar] [CrossRef]
- Vasic, J.; Petranova, T.; Povoroznyuk, V.; Barbu, C.G.; Karadzic, M.; Gojkovic, F.; Elez, J.; Winzenrieth, R.; Hans, D.; CulaficVojinovic, V.; et al. Evaluating spine micro-architectural texture (via TBS) discriminates major osteoporotic fractures from controls both as well as and independent of site matched BMD: The Eastern European TBS study. J. Bone Miner. Metab. 2014, 32, 556–562. [Google Scholar] [CrossRef]
- Boutroy, S.; Hans, D.; Sornay-Rendu, E.; Vilayphiou, N.; Winzenrieth, R.; Chapurlat, R. Trabecular bone score improves fracture risk prediction in non-osteoporotic women: The OFELY study. Osteoporos. Int. 2013, 24, 77–85. [Google Scholar] [CrossRef]
- Nassar, K.; Paternotte, S.; Kolta, S.; Fechtenbaum, J.; Roux, C.; Briot, K. Added value of trabecular bone score over bone mineral density for identification of vertebral fractures in patients with areal bone mineral density in the non-osteoporotic range. Osteoporos. Int. 2014, 25, 243–249. [Google Scholar] [CrossRef]
- Winzenrieth, R.; Dufour, R.; Pothuaud, L.; Hans, D. A retrospective case-control study assessing the role of trabecular bone score in postmenopausal Caucasian women with osteopenia: Analyzing the odds of vertebral fracture. Calcif. Tissue Int. 2010, 86, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Touvier, J.; Winzenrieth, R.; Johansson, H.; Roux, J.-P.; Chaintreuil, J.; Toumi, H.; Jennane, R.; Hans, D.; Lespessailles, E. Fracture discrimination by combined bone mineral density (BMD) and microarchitectural texture analysis. Calcif. Tissue Int. 2015, 96, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Rabier, B.; Héraud, A.; Grand-Lenoir, C.; Winzenrieth, R.; Hans, D. A multicentre, retrospective case-control study assessing the role of trabecular bone score (TBS) in menopausal Caucasian women with low areal bone mineral density (BMDa): Analysing the odds of vertebral fracture. Bone 2010, 46, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Ripamonti, C.; Lisi, L.; Buffa, A.; Gnudi, S.; Caudarella, R. The Trabecular Bone Score Predicts Spine Fragility Fractures in Postmenopausal Caucasian Women Without Osteoporosis Independently of Bone Mineral Density. Med. Arch. 2018, 72, 46–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, S.L.; Slemenda, C.W.; Johnston, C.C., Jr. Age and bone mass as predictors of fracture in a prospective study. J. Clin. Investig. 1988, 81, 1804–1809. [Google Scholar] [CrossRef] [Green Version]
- Mallett, S.; Halligan, S.; Thompson, M.; Collins, G.; Altman, D.G. Interpreting diagnostic accuracy studies for patient care. BMJ 2012, 345, e3999. [Google Scholar] [CrossRef] [Green Version]
- Kong, S.H.; Hong, N.; Kim, J.-W.; Kim, D.Y.; Kim, J.H. Application of the Trabecular Bone Score in Clinical Practice. J. Bone Metab. 2021, 28, 101–113. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Šimundić, A.M. Measures of Diagnostic Accuracy: Basic Definitions. Ejifcc 2009, 19, 203–211. [Google Scholar]
- Clopper, C.J.; Pearson, E.S. The Use of Confidence or Fiducial Limits Illustrated in the Case of the Binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- Nofuentes, J.A.; Del Castillo Jde, D. Comparison of the likelihood ratios of two binary diagnostic tests in paired designs. Stat. Med. 2007, 26, 4179–4201. [Google Scholar] [CrossRef] [PubMed]
- Mercaldo, N.D.; Lau, K.F.; Zhou, X.H. Confidence intervals for predictive values with an emphasis to case-control studies. Stat. Med. 2007, 26, 2170–2183. [Google Scholar] [CrossRef]
- Kosinski, A.S. A weighted generalized score statistic for comparison of predictive values of diagnostic tests. Stat. Med. 2013, 32, 964–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackinnon, A.; Khalilian, A.; Jorm, A.F.; Korten, A.E.; Christensen, H.; Mulligan, R. Improving screening accuracy for dementia in a community sample by augmenting cognitive testing with informant report. J. Clin. Epidemiol. 2003, 56, 358–366. [Google Scholar] [CrossRef]
- Arabi, A.; Baddoura, R.; Awada, H.; Khoury, N.; Haddad, S.; Ayoub, G.; El-Hajj Fuleihan, G. Discriminative ability of dual-energy X-ray absorptiometry site selection in identifying patients with osteoporotic fractures. Bone 2007, 40, 1060–1065. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 1: Sensitivity, specificity and predictive values. Acta Paediatr. 2007, 96, 338–341. [Google Scholar] [CrossRef]
- Krueger, D.; Fidler, E.; Libber, J.; Aubry-Rozier, B.; Hans, D.; Binkley, N. Spine trabecular bone score subsequent to bone mineral density improves fracture discrimination in women. J. Clin. Densitom. 2014, 17, 60–65. [Google Scholar] [CrossRef]
- Wang, H.; Wang, B.; Zhang, X.; Feng, C. Relations among sensitivity, specificity and predictive values of medical tests based on biomarkers. Gen. Psychiatr. 2021, 34, e100453. [Google Scholar] [CrossRef]
- Piscitelli, P.; Tarantino, U.; Chitano, G.; Argentiero, A.; Neglia, C.; Agnello, N.; Saturnino, L.; Feola, M.; Celi, M.; Raho, C.; et al. Updated incidence rates of fragility fractures in Italy: Extension study 2002–2008. Clin. Cases Miner. Bone Metab. 2011, 8, 54–61. [Google Scholar]


{kind=link}
{kind=link}
| Whole Population (n = 992) | Women with Fractures (n = 86) | Women without Fractures (n = 906) | p-Value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 68.5 ± 6.8 | 69.6 ± 6.8 | 68.4 ± 6.8 | 0.140 |
| Height (cm), mean ± SD | 159.5 ± 6.2 | 158.1 ± 6.4 | 159.6 ± 6.1 | 0.032 |
| Weight (kg), mean ± SD | 63.3 ± 10.4 | 62.6 ± 10.6 | 63.4 ± 10.4 | 0.501 |
| BMI, mean ± SD | 24.9 ± 3.7 | 25.0 ± 4.1 | 24.8 ± 3.7 | 0.553 |
| Age at menopause (years), mean ± SD | 49.4 ± 4.7 | 48.4 ± 5.5 | 49.5 ± 4.6 | 0.046 |
| TBS, mean ± SD | 1.210 ± 0.101 | 1.165 ± 0.095 | 1.214 ± 0.100 | 0.001 |
| LS-BMD (g/cm−2), mean ± SD | 0.823 ± 0.122 | 0.771 ± 0.127 | 0.828 ± 0.120 | 0.001 |
| LS-BMD T-score, mean ± SD | −2.02 ± 1.11 | −2.49 ± 1.15 | −1.98 ± 1.09 | 0.001 |
| TBS Positive % | TBS Negative % | Total % | |
|---|---|---|---|
| LS-BMD Positive | 29.8 | 14.4 | 44.2 |
| LS-BMD Negative | 17.6 | 38.2 | 55.8 |
| Total | 47.4 | 52.6 | 100 |
| Women with Fractures | Women without Fracturs | |||||
|---|---|---|---|---|---|---|
| TBS Positive % | TBS Negative % | Total % | TBS Positive % | TBS Negative % | Total % | |
| LS-BMD Positive test | 48.8 | 18.6 | 67.4 | 27.9 | 14.0 | 41.9 |
| LS-BMD negative test | 23.3 | 9.3 | 32.6 | 17.1 | 41.0 | 58.1 |
| Total | 72.1 | 27.9 | 100 | 45.0 | 55.0 | 100 |
| TBS Diagnostic Accuracy Values | LS-BMD Diagnostic Accuracy Values | p-Value TBS vs. LS-BMD | |
|---|---|---|---|
| SE% (95% CI) | 72.09 (61.38–81.23) | 67.44 (56.48–77.16) | ns ( = 0.446) |
| SP% (95% CI) | 54.97 (51.66–58.24) | 58.06 (54.77–61.30) | 0.09 ( = 2.788) |
| PPV% (95% CI) | 13.19 (11.48–14.91) | 13.24 (11.34–15.15) | ns (TVpp WGS = 0.001) |
| NPV% (95% CI) | 95.40 (93.63–96.70) | 94.95 (93.24–96.24) | ns (TVpn WGS = 0.16) |
| OR (95% CI) | 3.15 (1.93–5.14) | 2.87 (1.79–4.59) | ns |
| BMD | TBS | OR Rule | AND Rule | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prevalence | PPV (95% CI) | PPV (95% CI) | PPV (95% CI) | PPV (95% CI) | ||||||||
| 2.0% | 3.2% | 3.0% | 6.5% | 3.2% | 3.0% | 6.3% | 3.0% | 2.7% | 5.6% | 3.4% | 1.9% | 5.0% |
| 4.0% | 6.3% | 5.4% | 10.0% | 6.3% | 5.4% | 9.8% | 6.0% | 5.4% | 6.7% | 6.8% | 4.7% | 8.9% |
| 6.0% | 9.3% | 7.7% | 10.9% | 9.3% | 7.8% | 10.7% | 8.9% | 8.1% | 9.7% | 10.0% | 7.5% | 12.6% |
| 8.0% | 12.3% | 10.4% | 14.1% | 12.2% | 10.6% | 13.9% | 11.8% | 10.9% | 12.7% | 13.2% | 10.4% | 16.0% |
| 8.67% | 13.2% | 11.3% | 15.1% | 13.2% | 11.5% | 14.9% | 12.7% | 11.8% | 13.7% | 14.2% | 11.3% | 17.2% |
| 10.0% | 15.2% | 13.1% | 17.2% | 15.1% | 13.3% | 16.9% | 14.6% | 13.5% | 15.6% | 16.3% | 13.2% | 19.4% |
| 12.0% | 18.0% | 15.8% | 20.2% | 17.9% | 16.0% | 19.9% | 17.3% | 16.2% | 18.5% | 19.3% | 16.0% | 22.6% |
| 14.0% | 20.7% | 18.4% | 23.0% | 20.7% | 18.6% | 22.8% | 20.0% | 18.8% | 21.2% | 22.2% | 18.7% | 25.6% |
| 15.0% | 22.1% | 19.7% | 24.5% | 22.0% | 19.9% | 24.2% | 21.3% | 20.0% | 22.6% | 23.6% | 20.0% | 27.1% |
| 16.0% | 23.4% | 21.0% | 25.9% | 23.4% | 21.2% | 25.6% | 22.6% | 21.3% | 24.0% | 25.0% | 21.4% | 28.6% |
| 18.0% | 26.1% | 23.6% | 28.6% | 26.0% | 23.7% | 28.3% | 25.2% | 23.8% | 26.6% | 27.7% | 24.0% | 31.5% |
| 20.0% | 28.7% | 26.1% | 31.3% | 28.6% | 26.2% | 30.9% | 27.7% | 26.3% | 29.2% | 30.4% | 26.6% | 34.3% |
| 22.0% | 31.2% | 28.5% | 33.9% | 31.1% | 28.7% | 33.5% | 30.2% | 28.7% | 31.8% | 33.0% | 29.1% | 36.9% |
| 24.0% | 33.7% | 31.0% | 36.4% | 33.6% | 31.1% | 36.1% | 32.7% | 31.1% | 34.3% | 35.6% | 31.6% | 39.6% |
| 25.0% | 34.9% | 32.1% | 37.6% | 34.8% | 32.3% | 37.3% | 33.9% | 32.3% | 35.5% | 36.8% | 32.8% | 40.8% |
| 26.0% | 36.1% | 33.3% | 38.9% | 36.0% | 33.5% | 38.5% | 35.1% | 33.4% | 36.7% | 38.1% | 34.0% | 42.1% |
| 30.0% | 40.8% | 38.0% | 43.6% | 40.7% | 38.1% | 43.3% | 39.7% | 38.0% | 41.4% | 42.8% | 38.8% | 46.9% |
| 40.0% | 51.7% | 48.8% | 54.6% | 51.6% | 48.9% | 54.3% | 50.6% | 48.7% | 52.4% | 53.8% | 49.8% | 57.9% |
| BMD | TBS | OR Rule | AND Rule | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prevalence | NPV (95% CI) | NPV (95% CI) | NPV (95% CI) | NPV (95% CI) | ||||||||
| 2.0% | 98.9% | 96.7% | 98.6% | 99.0% | 96.8% | 98.6% | 99.5% | 97.0% | 98.6% | 98.6% | 98.0% | 99.2% |
| 4.0% | 97.7% | 95.3% | 97.8% | 97.9% | 95.4% | 97.9% | 99.1% | 98.2% | 100.0% | 97.1% | 96.3% | 98.0% |
| 6.0% | 96.5% | 95.3% | 97.8% | 96.9% | 95.6% | 98.1% | 98.6% | 97.4% | 99.7% | 95.7% | 94.6% | 96.7% |
| 8.0% | 95.4% | 93.9% | 96.8% | 95.8% | 94.3% | 97.2% | 98.1% | 96.7% | 99.4% | 94.2% | 93.0% | 95.4% |
| 8.67% | 94.9% | 93.5% | 96.4% | 95.4% | 93.9% | 96.9% | 97.9% | 96.5% | 99.3% | 93.7% | 92.4% | 94.9% |
| 10.0% | 94.1% | 92.5% | 95.7% | 94.7% | 93.0% | 96.3% | 97.5% | 96.1% | 99.0% | 92.7% | 91.4% | 94.0% |
| 12.0% | 92.9% | 91.2% | 94.6% | 93.5% | 91.7% | 95.3% | 97.0% | 95.3% | 98.6% | 91.2% | 89.7% | 92.6% |
| 14.0% | 91.6% | 89.7% | 93.5% | 92.4% | 90.4% | 94.3% | 96.4% | 94.6% | 98.2% | 89.6% | 88.1% | 91.2% |
| 15.0% | 91.0% | 89.0% | 92.9% | 91.8% | 89.8% | 93.8% | 96.1% | 94.3% | 98.0% | 88.9% | 87.3% | 90.5% |
| 16.0% | 90.3% | 88.3% | 92.4% | 91.2% | 89.1% | 93.3% | 95.9% | 93.9% | 97.8% | 88.1% | 86.4% | 89.7% |
| 18.0% | 89.0% | 86.9% | 91.2% | 90.0% | 87.8% | 92.2% | 95.3% | 93.1% | 97.4% | 86.5% | 84.8% | 88.3% |
| 20.0% | 87.7% | 85.5% | 90.0% | 88.7% | 86.4% | 91.1% | 94.6% | 92.4% | 96.9% | 84.9% | 83.1% | 86.8% |
| 22.0% | 86.3% | 84.0% | 88.7% | 87.5% | 85.0% | 89.9% | 94.0% | 91.6% | 96.4% | 83.3% | 81.4% | 85.2% |
| 24.0% | 85.0% | 82.5% | 87.4% | 86.2% | 83.6% | 88.7% | 93.3% | 90.8% | 95.8% | 81.7% | 79.7% | 83.7% |
| 25.0% | 84.3% | 81.7% | 86.8% | 85.5% | 82.9% | 88.1% | 93.0% | 90.4% | 95.6% | 80.9% | 78.9% | 82.9% |
| 26.0% | 83.5% | 81.0% | 86.1% | 84.9% | 82.2% | 87.5% | 92.6% | 89.9% | 95.3% | 80.0% | 78.0% | 82.1% |
| 30.0% | 80.6% | 77.9% | 83.4% | 82.1% | 79.3% | 85.0% | 91.1% | 88.2% | 94.1% | 76.7% | 74.5% | 78.8% |
| 40.0% | 72.8% | 69.7% | 75.9% | 74.7% | 71.4% | 78.0% | 86.8% | 83.2% | 90.5% | 67.9% | 65.5% | 70.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ripamonti, C.; Lisi, L.; Ciaffi, J.; Buffa, A.; Caudarella, R.; Ursini, F. Spine Fragility Fracture Prediction Using TBS and BMD in Postmenopausal Women: A Bayesian Approach. Int. J. Environ. Res. Public Health 2022, 19, 14315. https://doi.org/10.3390/ijerph192114315
Ripamonti C, Lisi L, Ciaffi J, Buffa A, Caudarella R, Ursini F. Spine Fragility Fracture Prediction Using TBS and BMD in Postmenopausal Women: A Bayesian Approach. International Journal of Environmental Research and Public Health. 2022; 19(21):14315. https://doi.org/10.3390/ijerph192114315
Chicago/Turabian StyleRipamonti, Claudio, Lucia Lisi, Jacopo Ciaffi, Angela Buffa, Renata Caudarella, and Francesco Ursini. 2022. "Spine Fragility Fracture Prediction Using TBS and BMD in Postmenopausal Women: A Bayesian Approach" International Journal of Environmental Research and Public Health 19, no. 21: 14315. https://doi.org/10.3390/ijerph192114315