
Effects of Twenty-Four Weeks of Resistance Exercise Training on Body Composition, Bone Mineral Density, Functional Fitness and Isokinetic Muscle Strength in Obese Older Women: A Randomized Controlled Trial





Abstract
:1. Introduction
2. Materials and Methods
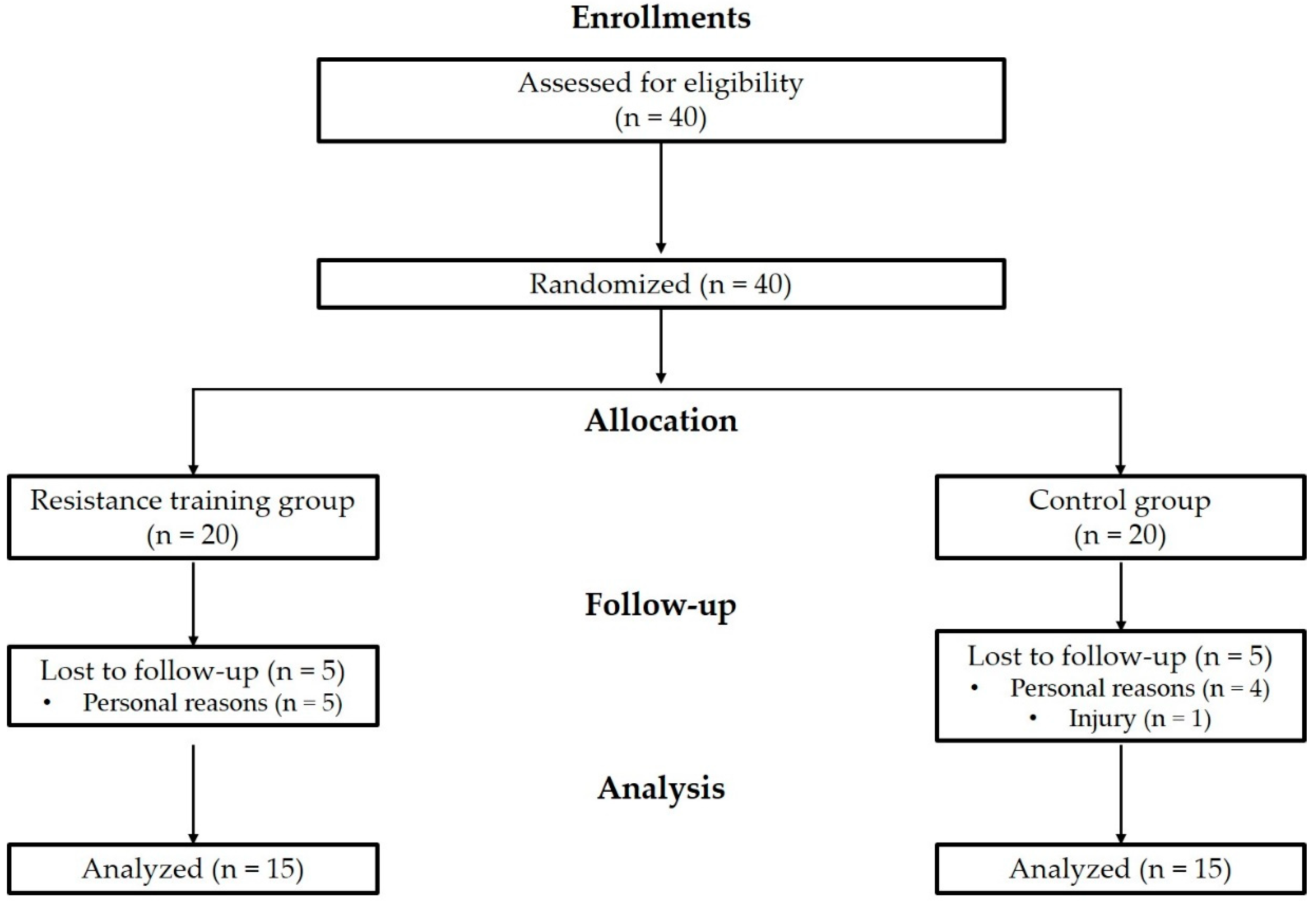
2.1. Participants
2.2. Resistance Exercise Training Program
2.3. Body Composition and Bone Mineral Density
2.4. Functional Fitness
2.5. Isokinetic Muscle Strength
2.6. Statistical Analysis
3. Results
3.1. Body Composition and Bone Mineral Density
3.2. Functional Fitness
3.3. Isokinetic Muscle Strength
4. Discussion
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Jarzebski, M.P.; Elmqvist, T.; Gasparatos, A.; Fukushi, K.; Eckersten, S.; Haase, D.; Goodness, J.; Khoshkar, S.; Saito, O.; Takeuchi, K. Ageing and population shrinking: Implications for sustainability in the urban century. npj Urban Sustain. 2021, 1, 1–11. [Google Scholar] [CrossRef]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Chia, C.W.; Egan, J.M.; Ferrucci, L. Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk. Circ. Res. 2018, 123, 886–904. [Google Scholar] [CrossRef]
- Xie, W.Q.; Xiao, G.L.; Fan, Y.B.; He, M.; Lv, S.; Li, Y.S. Sarcopenic obesity: Research advances in pathogenesis and diagnostic criteria. Aging Clin. Exp. Res. 2021, 33, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Jung, S.W.; Seo, M.W.; Park, H.Y.; Song, J.K. Effects of bone-specific physical activity on body composition, bone mineral density, and health-related physical fitness in middle-aged women. J. Exerc. Nutr. Biochem. 2019, 23, 36–42. [Google Scholar] [CrossRef]
- Kyle, U.G.; Genton, L.; Hans, D.; Karsegard, L.; Slosman, D.O.; Pichard, C. Age-related differences in fat-free mass, skeletal muscle, body cell mass and fat mass between 18 and 94 years. Eur. J. Clin. Nutr. 2001, 55, 663–672. [Google Scholar] [CrossRef]
- Ambikairajah, A.; Walsh, E.; Tabatabaei-Jafari, H.; Cherbuin, N. Fat mass changes during menopause: A metaanalysis. Am. J. Obstet. Gynecol. 2019, 221, 393–409.e350. [Google Scholar] [CrossRef]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007–2008 to 2015–2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef] [Green Version]
- Adams, K.F.; Schatzkin, A.; Harris, T.B.; Kipnis, V.; Mouw, T.; Ballard-Barbash, R.; Hollenbeck, A.; Leitzmann, M.F. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N. Engl. J. Med. 2006, 355, 763–778. [Google Scholar] [CrossRef]
- Zago, M.; Capodaglio, P.; Ferrario, C.; Tarabini, M.; Galli, M. Whole-body vibration training in obese subjects: A systematic review. PLoS ONE 2018, 13, e0202866. [Google Scholar] [CrossRef]
- Hirschfeld, H.P.; Kinsella, R.; Duque, G. Osteosarcopenia: Where bone, muscle, and fat collide. Osteoporos Int. 2017, 28, 2781–2790. [Google Scholar] [CrossRef] [PubMed]
- Genton, L.; Karsegard, V.L.; Chevalley, T.; Kossovsky, M.P.; Darmon, P.; Pichard, C. Body composition changes over 9 years in healthy elderly subjects and impact of physical activity. Clin. Nutr. 2011, 30, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Geirsdottir, O.G.; Arnarson, A.; Briem, K.; Ramel, A.; Tomasson, K.; Jonsson, P.V.; Thorsdottir, I. Physical function predicts improvement in quality of life in elderly Icelanders after 12 weeks of resistance exercise. J. Nutr. Health Aging 2012, 16, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J. Assessment of Osteoporosis at the Primary Health Care Level; Printed by the University of Sheffield; WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield Medical School: Sheffield, UK, 2007. [Google Scholar]
- Lee, E.Y.; Kim, D.; Kim, K.M.; Kim, K.J.; Choi, H.S.; Rhee, Y.; Lim, S.K. Age-related bone mineral density patterns in Koreans (KNHANES IV). J. Clin. Endocrinol. Metab. 2012, 97, 3310–3318. [Google Scholar] [CrossRef] [Green Version]
- Schwab, P.; Scalapino, K. Exercise for bone health: Rationale and prescription. Curr. Opin. Rheumatol. 2011, 23, 137–141. [Google Scholar] [CrossRef]
- Topp, R.; Fahlman, M.; Boardley, D. Healthy aging: Health promotion and disease prevention. Nurs. Clin. N. Am. 2004, 39, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Schoufour, J.D.; Echteld, M.A.; Bastiaanse, L.P.; Evenhuis, H.M. The use of a frailty index to predict adverse health outcomes (falls, fractures, hospitalization, medication use, comorbid conditions) in people with intellectual disabilities. Res. Dev. Disabil. 2015, 38, 39–47. [Google Scholar] [CrossRef]
- Liguori, G.; Medicine, A.C.o.S. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020. [Google Scholar]
- Fisher, J.P.; Steele, J.; Gentil, P.; Giessing, J.; Westcott, W.L. A minimal dose approach to resistance training for the older adult; the prophylactic for aging. Exp. Gerontol. 2017, 99, 80–86. [Google Scholar] [CrossRef]
- Daryanti Saragih, I.; Yang, Y.P.; Saragih, I.S.; Batubara, S.O.; Lin, C.J. Effects of resistance bands exercise for frail older adults: A systematic review and meta-analysis of randomised controlled studies. J. Clin. Nurs. 2022, 31, 43–61. [Google Scholar] [CrossRef]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef]
- Kim, S.W.; Jung, W.S.; Park, W.; Park, H.Y. Twelve Weeks of Combined Resistance and Aerobic Exercise Improves Cardiometabolic Biomarkers and Enhances Red Blood Cell Hemorheological Function in Obese Older Men: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 5020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiebaud, R.S.; Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Kim, D.; Abe, T.; Anderson, M.A.; Young, K.C.; Bemben, D.A.; Bemben, M.G. The effects of elastic band resistance training combined with blood flow restriction on strength, total bone-free lean body mass and muscle thickness in postmenopausal women. Clin. Physiol. Funct. Imaging 2013, 33, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Colado, J.C.; Pedrosa, F.M.; Juesas, A.; Gargallo, P.; Carrasco, J.J.; Flandez, J.; Chupel, M.U.; Teixeira, A.M.; Naclerio, F. Concurrent validation of the OMNI-Resistance Exercise Scale of perceived exertion with elastic bands in the elderly. Exp. Gerontol. 2018, 103, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Chupel, M.U.; Direito, F.; Furtado, G.E.; Minuzzi, L.G.; Pedrosa, F.M.; Colado, J.C.; Ferreira, J.P.; Filaire, E.; Teixeira, A.M. Strength Training Decreases Inflammation and Increases Cognition and Physical Fitness in Older Women with Cognitive Impairment. Front. Physiol. 2017, 8, 377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muntaner-Mas, A.; Vidal-Conti, J.; Borràs, P.A.; Ortega, F.B.; Palou, P. Effects of a Whatsapp-delivered physical activity intervention to enhance health-related physical fitness components and cardiovascular disease risk factors in older adults. J. Sports Med. Phys. Fitness 2017, 57, 90–102. [Google Scholar] [CrossRef]
- Park, H.Y.; Jung, W.S.; Kim, J.; Lim, K. Twelve weeks of exercise modality in hypoxia enhances health-related function in obese older Korean men: A randomized controlled trial. Geriatr. Gerontol. Int. 2019, 19, 311–316. [Google Scholar] [CrossRef]
- Ha, Y.C.; Yoo, J.I. Cross-Calibration of Bone Mineral Densities and Body Composition between GE Lunar Prodigy and Osteosys Primus. J. Bone Metab. 2021, 28, 215–221. [Google Scholar] [CrossRef]
- Monteiro, A.M.; Forte, P.M.; Carvalho, J. The effect of three different training programs in elderly women’s isokinetic strength. Motricidade 2020, 16, 84–93. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Thomas, E.; Gentile, A.; Lakicevic, N.; Moro, T.; Bellafiore, M.; Paoli, A.; Drid, P.; Palma, A.; Bianco, A. The effect of resistance training programs on lean body mass in postmenopausal and elderly women: A meta-analysis of observational studies. Aging Clin. Exp. Res. 2021, 33, 2941–2952. [Google Scholar] [CrossRef]
- Flandez, J.; Gene-Morales, J.; Modena, N.; Martin, F.; Colado, J.C.; Gargallo, P. Effects of power resistance training program with elastic bands on body composition, muscle strength and physical function in older women. J. Hum. Sport Exerc. 2020, 15, S1322–S1337. [Google Scholar]
- Xu, J.; Lombardi, G.; Jiao, W.; Banfi, G. Effects of Exercise on Bone Status in Female Subjects, from Young Girls to Postmenopausal Women: An Overview of Systematic Reviews and Meta-Analyses. Sports Med. 2016, 46, 1165–1182. [Google Scholar] [CrossRef] [PubMed]
- Bocalini, D.S.; Serra, A.J.; Dos Santos, L. Moderate resistive training maintains bone mineral density and improves functional fitness in postmenopausal women. J. Aging Res. 2010, 2010, 760818. [Google Scholar] [CrossRef] [PubMed]
- Chien, M.Y.; Wu, Y.T.; Hsu, A.T.; Yang, R.S.; Lai, J.S. Efficacy of a 24-week aerobic exercise program for osteopenic postmenopausal women. Calcif. Tissue Int. 2000, 67, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Oesen, S.; Halper, B.; Hofmann, M.; Jandrasits, W.; Franzke, B.; Strasser, E.M.; Graf, A.; Tschan, H.; Bachl, N.; Quittan, M.; et al. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly--A randomized controlled trial. Exp. Gerontol. 2015, 72, 99–108. [Google Scholar] [CrossRef]
- Hanson, E.D.; Srivatsan, S.R.; Agrawal, S.; Menon, K.S.; Delmonico, M.J.; Wang, M.Q.; Hurley, B.F. Effects of strength training on physical function: Influence of power, strength, and body composition. J. Strength Cond. Res. 2009, 23, 2627–2637. [Google Scholar] [CrossRef] [Green Version]
- Marcell, T.J.; Hawkins, S.A.; Wiswell, R.A. Leg strength declines with advancing age despite habitual endurance exercise in active older adults. J. Strength Cond. Res. 2014, 28, 504–513. [Google Scholar] [CrossRef]
- Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; Newman, A.B.; et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [CrossRef] [Green Version]
- Hewett, T.E.; Myer, G.D.; Zazulak, B.T. Hamstrings to quadriceps peak torque ratios diverge between sexes with increasing isokinetic angular velocity. J. Sci. Med. Sport 2008, 11, 452–459. [Google Scholar] [CrossRef] [Green Version]
- Skelton, D.A.; Kennedy, J.; Rutherford, O.M. Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age Ageing 2002, 31, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Gadelha, A.B.; Paiva, F.M.; Gauche, R.; de Oliveira, R.J.; Lima, R.M. Effects of resistance training on sarcopenic obesity index in older women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2016, 65, 168–173. [Google Scholar] [CrossRef]
- Beneka, A.; Malliou, P.; Fatouros, I.; Jamurtas, A.; Gioftsidou, A.; Godolias, G.; Taxildaris, K. Resistance training effects on muscular strength of elderly are related to intensity and gender. J. Sci. Med. Sport 2005, 8, 274–283. [Google Scholar] [CrossRef]
- Rabelo, H.T.; Bezerra, L.A.; Terra, D.F.; Lima, R.M.; Silva, M.A.; Leite, T.K.; de Oliveira, R.J. Effects of 24 weeks of progressive resistance training on knee extensors peak torque and fat-free mass in older women. J. Strength Cond. Res. 2011, 25, 2298–2303. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Campo, D.J.; Andreu-Caravaca, L.; Carrasco-Poyatos, M.; Benito, P.J.; Rubio-Arias, J.Á. Effects of circuit resistance training on body composition, strength, and cardiorespiratory fitness in middle-aged and older women: A systematic review and meta-analysis. J. Aging Phys. Act. 2021, 1, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Villa-Forte, A. Effects of aging on the musculoskeletal system. Last Full Rev./Revis. July 2014, 2015. Available online: https://www.msdmanuals.com/home/bone,-joint,-and-muscle-disorders/symptoms-of-musculoskeletal-disorders/introduction-to-symptoms-of-musculoskeletal-disorders (accessed on 3 November 2022).
- Basu, R.; Basu, A.; Nair, K.S. Muscle changes in aging. J. Nutr. Health Aging 2002, 6, 336–341. [Google Scholar]
- Faulkner, J.A.; Larkin, L.M.; Claflin, D.R.; Brooks, S.V. Age-related changes in the structure and function of skeletal muscles. Clin. Exp. Pharmacol. Physiol. 2007, 34, 1091–1096. [Google Scholar] [CrossRef]
- Office of the Surgeon, G. Reports of the Surgeon General. In Bone Health and Osteoporosis: A Report of the Surgeon General; Office of the Surgeon General (US): Rockville, MD, USA, 2004. [Google Scholar]
- Morley, J.E.; Baumgartner, R.N.; Roubenoff, R.; Mayer, J.; Nair, K.S. Sarcopenia. J. Lab. Clin. Med. 2001, 137, 231–243. [Google Scholar] [CrossRef]


{kind=link}
| Variables | RT | CON | p Value |
|---|---|---|---|
| Age (years) | 81.6 ± 4.78 | 79.6 ± 5.19 | 0.266 |
| Height (cm) | 151.33 ± 3.74 | 153.28 ± 4.74 | 0.218 |
| Weight (kg) | 57.66 ± 8.98 | 58.26 ± 5.94 | 0.578 |
| Body fat percentage (%) | 35.59 ± 4.22 | 36.88 ± 2.50 | 0.308 |
| Program | Contents | Intensity | Frequency | |
|---|---|---|---|---|
| Warm-up | Dynamic and static stretching | - | 2 sessions/week | |
| Main exercise | Upper body | Lower body | OMNI Resistance for active muscle scale: 7–9 range Resting time per set: 90 s Yellow band (3 set) 10 Rep (1–4 weeks) 12 Rep (5–8 weeks) 15 Rep (9–12 weeks) Red band (3 set) 10 Rep (13–16 weeks) 12 Rep (17–20 weeks) 15 Rep (21–24 weeks) | |
| Abdominal curl-up Biceps curl Chest press Front shoulder raise Lateral shoulder raise Seated row Triceps extension | Calf raises Chair squat Hip extension Hip flexion Hip abduction Hip adduction Toe raise | |||
| Cool down | Static stretching | - | ||
| Variables | RT | CON | F-Value (ηp2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Time | Group | Interaction | |
| Fat mass (kg) | 20.74 ± 5.47 (17.71–23.77) | 20.13 ± 5.28 (17.20–23.06) | −0.61 (−1.46–0.24) | 21.45 ± 2.84 (19.94–22.97) | 22.61 ± 2.84 (21.09–24.12) | 1.15 *** (0.77–1.53) | 1.620 (0.053) | 1.108 (0.037) | 17.205 (0.372) ††† |
| Fat-free mass (kg) | 35.15 ± 4.17 (32.85–37.46) | 35.22 ± 3.97 (33.02–37.42) | 0.07 (−0.43–0.57) | 35.03 ± 3.53 (33.15–36.90) | 34.45 ± 3.31 (32.68–36.21) | −0.58 *** (−0.89–−0.27) | 3.586 (0.110) | 0.114 (0.004) | 5.700 (0.164) † |
| Body fat percentage (%) | 35.59 ± 4.22 (33.26–37.93) | 34.83 ± 4.03 (32.60–37.07) | −0.76 (−1.64–0.12) | 36.88 ± 2.50 (35.54–38.21) | 38.46 ± 2.42 # (37.17–39.75) | 1.59 *** (1.19–1.98) | 3.499 (0.108) | 4.248 (0.128) † | 28.266 (0.494) ††† |
| Whole-body BMD (g/cm2) | 1.00 ± 0.21 (0.89–1.12) | 1.01 ± 0.20 (0.90–1.13) | 0.01 (0–0.02) | 0.97 ± 0.14 (0.89–1.04) | 0.96 ± 0.14 (0.88–1.03) | −0.01 *** (−0.02–−0.01) | 0.020 (0.001) | 0.567 (0.019) | 12.385 (0.299) ††† |
| Femur BMD (g/cm2) | 0.73 ± 0.11 (0.67–0.79) | 0.72 ± 0.12 (0.66–0.79) | −0.01 (−0.03–0.01) | 0.69 ± 0.10 (0.63–0.74) | 0.68 ± 0.10 (0.62–0.73) | −0.01 (−0.03–0.01) | 3.079 (0.096) | 1.519 (0.050) | 0.074 (0.003) |
| Lumbar BMD (g/cm2) | 0.81 ± 0.14 (0.74–0.89) | 0.82 ± 0.15 (0.74–0.90) | 0.01 (−0.03–0.04) | 0.80 ± 0.12 (0.74–0.87) | 0.81 ± 0.11 (0.76–0.87) | 0.01 (−0.01–0.03) | 0.534 (0.018) | 0.015 (0.001) | 0.027 (0.001) |
| Forearm BMD (g/cm2) | 0.42 ± 0.05 (0.39–0.45) | 0.42 ± 0.05 (0.39–0.45) | 0 (0–0.01) | 0.42 ± 0.05 (0.39–0.45) | 0.41 ± 0.05 (0.38–0.44) | −0.01 ** (−0.01–0) | 5.065 (0.149) † | 0.288 (0.010) | 6.228 (0.177) † |
| Variables | RT | CON | F-Value (ηp2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Time | Group | Interaction | |
| Hand grip strength (kg) | 21.20 ± 3.53 (19.24–23.16) | 22.90 ± 3.34 (21.05–24.75) | 1.70 ** (0.71–2.69) | 19.84 ± 4.33 (17.53–22.15) | 19.03 ± 3.45 ## (37.17–39.75) | −0.81 (−1.76–0.14) | 1.926 (0.062) | 4.110 (0.124) | 15.433 (0.347) ††† |
| Lower body flexibility (cm) | 22.43 ± 8.68 (17.63–27.24) | 24.44 ± 7.98 (20.01–28.86) | 2.01 (−0.47–4.48) | 20.91 ± 6.99 (17.18–24.63) | 17.68 ± 6.88 # (14.01–21.34) | −3.23 ** (−5.44–−1.02) | 0.627 (0.021) | 2.474 (0.079) | 11.479 (0.284) †† |
| Upper body flexibility (cm) | −11.77 ± 14.17 (−19.61-−3.92) | −11.35 ± 15.85 (−20.13-−2.57) | 0.42 (−2.46–3.20) | −11.99 ± 12.85 (−18.83-−5.14) | −12.47 ± 10.95 (−18.30–−6.63) | −0.48 (−2.42–1.46) | 0.002 (0.000) | 0.020 (0.001) | 0.330 (0.011) |
| Lower body strength (n) | 15.07 ± 4.22 (12.73–17.40) | 18.93 ± 5.69 (15.78–22.08) | 3.87 *** (1.95–5.78) | 16.19 ± 3.02 (14.58–17.79) | 15.13 ± 3.56 # (13.23–17.02) | −1.06 (−2.46–0.33) | 6.522 (0.184) † | 0.908 (0.030) | 20.154 (0.410) ††† |
| Upper body strength (n) | 18.27 ± 4.06 (16.02–20.52) | 19.47 ± 4.24 (17.12–21.81) | 1.20 (−0.70–3.10) | 19.19 ± 5.06 (16.49–21.89) | 17.13 ± 4.75 (14.60–19.65) | −2.06 *** (−3.02–−1.10) | 0.783 (0.026) | 0.206 (0.007) | 11.202 (0.279) †† |
| Agility and dynamic balance (s) | 6.48 ± 1.42 (5.70–7.27) | 6.03 ± 1.06 (5.45–6.62) | −0.45 (−1.16–0.26) | 5.90 ± 1.04 (5.34–6.45) | 6.44 ± 1.10 (5.85–7.03) | 0.54 ** (0.20–0.88) | 0.064 (0.002) | 0.057 (0.002) | 7.532 (0.206) †† |
| Aerobic endurance (n) | 109.87 ± 16.72 (100.61–119.13) | 113.80 ± 31.12 (96.57–131.03) | 3.93 (−12.33–20.19) | 107.81 ± 14.75 (99.95–115.67) | 99.44 ± 18.01 (89.84–109.03) | −8.38 (−15.11–−1.64) | 0.306 (0.007) | 1.647 (0.054) | 2.351 (0.075) |
| Variables | RT | CON | F-Value (ηp2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Time | Group | Interaction | |
| DL extensor peak torque (Nm) | 70.87 ± 23.55 (57.82–83.91) | 76.20 ± 21.91 (64.07–88.33) | 5.33 (−2.25–12.92) | 66.88 ± 15.56 (58.58–75.17) | 62.06 ± 16.60 (53.22–70.91) | −4.81 * (−8.93-−0.70) | 0.017 (0.001) | 1.801 (0.058) | 6.562 (0.185) † |
| DL extensor peak torque %BW (%) | 126.27 ± 46.52 (100.51–152.03) | 139.73 ± 48.53 (112.86–166.61) | 13.47 (−4.01–30.94) | 116.81 ± 28.65 (101.54–132.08) | 109.50 ± 31.92 # (92.49–126.51) | −7.31 * (−13.94–−0.68) | 0.523 (0.018) | 2.137 (0.069) | 5.962 (0.171) † |
| NDL extensor peak torque (Nm) | 69.20 ± 21.37 (57.36–81.04) | 75.53 ± 25.40 (61.47–89.60) | 6.33 (−2.66–15.32) | 66.38 ± 14.53 (58.63–74.11) | 64.13 ± 13.54 (56.91–71.34) | −2.25 (−6.59–2.09) | 0.799 (0.027) | 1.197 (0.040) | 3.531 (0.109) |
| NDL extensor peak torque %BW (%) | 122.33 ± 40.88 (99.69–144.97) | 135.53 ± 48.97 (108.41–161.65) | 13.20 * (−1.33–27.73) | 113.81 ± 24.60 (100.70–126.92) | 110.63 ± 25.78 (96.89–124.36) | −3.19 (−10.94–4.57) | 1.757 (0.057) | 1.802 (0.059) | 4.706 (0.140) † |
| DL flexor peak torque (Nm) | 31.13 ± 12.82 (24.04–38.23) | 35.00 ± 9.70 (29.63–40.37) | 3.87 * (0.50–7.23) | 29.56 ± 15.02 (21.56–37.57) | 28.06 ± 12.73 (21.28–34.84) | −1.50 (−4.16–1.16) | 1.410 (0.046) | 0.904 (0.030) | 7.251 (0.200) † |
| DL flexor peak torque %BW (%) | 54.80 ± 22.56 (42.31–67.29) | 62.40 ± 18.48 (52.17–72.63) | 7.60 * (1.05–14.15) | 50.88 ± 27.01 (36.48–65.27) | 46.94 ± 22.51 # (34.94–58.93) | −3.94 (−9.47–1.59) | 0.843 (0.028) | 1.472 (0.048) | 8.361 (0.224) †† |
| NDL flexor peak torque (Nm) | 32.33 ± 15.92 (23.52–41.15) | 35.13 ± 13.60 (27.60–42.67) | 2.80 (−0.26–5.86) | 28.56 ± 16.65 (19.69–37.43) | 26.19 ± 12.10 # (19.74–32.64) | −2.38 (−5.88–1.13) | 0.038 (0.001) | 1.519 (0.050) | 5.598 (0.162) † |
| NDL flexor peak torque %BW (%) | 57.53 ± 29.06 (41.44–73.62) | 62.93 ± 26.01 (48.53–77.34) | 5.40 (−0.62–11.42) | 49.94 ± 30.52 (33.67–66.20) | 44.50 ± 23.71 # (31.86–57.14) | −5.44 (−11.43–0.55) | 0.000 (0.000) | 1.814 (0.059) | 7.429 (0.204) † |
| Variables | RT | CON | F-Value (ηp2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Pre (95% CI) | Post (95% CI) | Mean Change (95% CI) | Time | Group | Interaction | |
| DL extensor peak torque (Nm) | 40.67 ± 11.88 (34.09–47.24) | 44.13 ± 13.34 (36.75–51.52) | 3.47 (−0.74–7.67) | 39.75 ± 10.51 (34.15–45.35) | 37.56 ± 10.28 (32.09–43.04) | −2.19 * (−4.97–0.59) | 0.302 (0.010) | 0.886 (0.030) | 5.902 (0.169) † |
| DL extensor peak torque %BW (%) | 72.47 ± 23.62 (59.39–85.54) | 78.53 ± 26.06 (64.10–92.97) | 6.07 (−1.09–13.23) | 68.69 ± 17.55 (59.34–78.04) | 63.63 ± 17.74 (54.17–73.08) | −5.06 * (−10.44–0.31) | 0.059 (0.002) | 1.586 (0.052) | 7.193 (0.199) † |
| NDL extensor peak torque (Nm) | 39.67 ± 11.46 (33.32–46.01) | 41.87 ± 15.09 (33.51–50.23) | 2.20 (−3.23–7.63) | 36.88 ± 8.52 (32.34–41.41) | 35.00 ± 8.66 (30.38–39.62) | −1.88 (−3.71–−0.04) | 0.016 (0.001) | 1.616 (0.053) | 2.449 (0.078) |
| NDL extensor peak torque %BW (%) | 70.20 ± 22.55 (57.71–82.69) | 75.87 ± 29.41 (59.58–92.15) | 5.67 (−3.52–14.85) | 63.56 ± 14.58 (55.79–71.33) | 58.50 ± 13.78 (51.15–65.85) | −5.06 * (−8.83–−1.29) | 0.018 (0.001) | 2.816 (0.089) | 5.618 (0.162) † |
| DL flexor peak torque (Nm) | 19.93 ± 7.81 (15.61–24.26) | 20.60 ± 7.06 (16.69–24.51) | 0.67 (−2.33–3.66) | 18.75 ± 7.46 (14.77–22.73) | 16.56 ± 6.96 (12.86–20.27) | −2.19 (−3.86–−0.51) | 0.931 (0.031) | 1.080 (0.036) | 3.279 (0.102) |
| DL flexor peak torque %BW (%) | 35.60 ± 15.38 (27.09–44.11) | 36.40 ± 13.07 (29.16–43.64) | 0.80 (−5.27–6.87) | 33.19 ± 13.66 (25.91–40.47) | 27.38 ± 13.14 (20.37–34.38) | −5.81 ** (−9.34–−2.29) | 2.412 (0.077) | 1.480 (0.049) | 4.197 (0.126) † |
| NDL flexor peak torque (Nm) | 22.33 ± 10.39 (16.58–28.09) | 23.60 ± 9.72 (18.22–28.98) | 1.27 (−0.36–2.89) | 20.81 ± 9.56 (15.72–25.91) | 18.63 ± 7.21 (14.78–22.47) | −2.19 * (−4.16–−0.21) | 0.582 (0.020) | 0.983 (0.033) | 8.183 (0.220) †† |
| NDL flexor peak torque %BW (%) | 39.93 ± 20.43 (28.62–51.24) | 42.33 ± 19.01 (31.81–52.86) | 2.40 (−0.28–5.08) | 36.56 ± 17.33 (27.33–45.80) | 30.75 ± 12.51 (24.08–37.42) | −5.81 ** (−9.79–−1.83) | 2.246 (0.072) | 1.462 (0.048) | 13.009 (0.310) ††† |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-W.; Park, H.-Y.; Jung, W.-S.; Lim, K. Effects of Twenty-Four Weeks of Resistance Exercise Training on Body Composition, Bone Mineral Density, Functional Fitness and Isokinetic Muscle Strength in Obese Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 14554. https://doi.org/10.3390/ijerph192114554
Kim S-W, Park H-Y, Jung W-S, Lim K. Effects of Twenty-Four Weeks of Resistance Exercise Training on Body Composition, Bone Mineral Density, Functional Fitness and Isokinetic Muscle Strength in Obese Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(21):14554. https://doi.org/10.3390/ijerph192114554
Chicago/Turabian StyleKim, Sung-Woo, Hun-Young Park, Won-Sang Jung, and Kiwon Lim. 2022. "Effects of Twenty-Four Weeks of Resistance Exercise Training on Body Composition, Bone Mineral Density, Functional Fitness and Isokinetic Muscle Strength in Obese Older Women: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 21: 14554. https://doi.org/10.3390/ijerph192114554
APA StyleKim, S.-W., Park, H.-Y., Jung, W.-S., & Lim, K. (2022). Effects of Twenty-Four Weeks of Resistance Exercise Training on Body Composition, Bone Mineral Density, Functional Fitness and Isokinetic Muscle Strength in Obese Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(21), 14554. https://doi.org/10.3390/ijerph192114554