
Loneliness and Social Support among the Middle-Aged and Elderly People with Visual Impairment

Abstract
:1. Introduction
2. Research Materials and Methods
2.1. Design
2.2. Recruitment
2.3. Measures
2.3.1. Basic Personal Information
2.3.2. The UCLA Loneliness Scale Version 3
2.3.3. The Social Support Scale
2.4. Statistical Analyses
3. Results
3.1. Analysis of Participant Demographics
3.2. Analysis of the Differences in Loneliness Scores and the Loneliness Degree of the Participants according to Different Sociodemographic Characteristics
3.3. Analysis of Variance in Social Support Scores
3.4. Analysis of the Relationship between Loneliness and Social Support
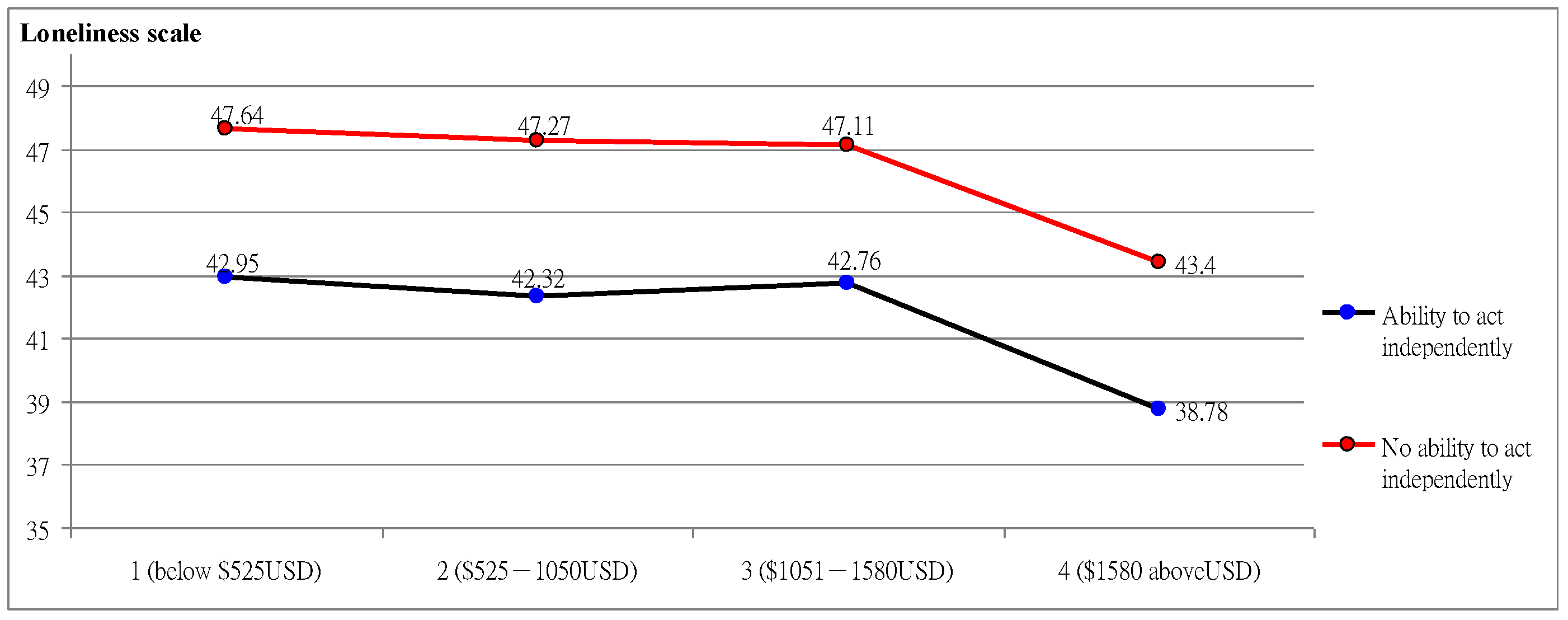
3.5. Demographic Interaction Analysis
3.6. Regression Analysis of Social Support on Loneliness
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Blindness and Vision Impairment. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment/ (accessed on 18 July 2022).
- Vision Loss Expert Group of the Global Burden of Disease Study; GBD 2019 Blindness and Vision Impairment Collaborators. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The right to sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 2, 144–160. [Google Scholar] [CrossRef]
- Vision Loss Expert Group of the Global Burden of Disease Study. Trends in prevalence of blindness and distance and near vision impairment over 30 years: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2020, 9, e130–e143. [Google Scholar] [CrossRef]
- Zhao, J.; Ellwein, L.B.; Cui, H.; Ge, J.; Guan, H.; Lv, J.; Ma, X.; Yin, J.; Yin, Z.Q.; Yuan, Y.; et al. Prevalence of vision impairment in older adults in rural China, the China Nine-Province Survey. Ophthalmology 2010, 117, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Sun, X.; Shao, Z.; Zhou, X.; Kang, Y.; Sui, H.; Yuan, H. Prevalence and causes of visual impairment in a rural North-east China adult population: A population-based survey in Bin County, Harbin. Acta Ophthalmol. 2010, 88, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Wang, X.; Wang, J.; Huang, W.; Gao, Y.; Luo, Y.; Lu, Y. Prevalence and causes of visual impairment in a Chinese adult population: The taizhou eye study. Ophthalmology 2015, 122, 1480–1488. [Google Scholar] [CrossRef]
- American Foundation for the Blind. Estimates of Older People with Vision Loss from the American Community Survey (ACS) Estimated Population with Vision Loss. 2022. Available online: https://www.afb.org/research-and-initiatives/statistics/statistics-older-vision-loss/statistics-older-vision-loss-acs (accessed on 2 July 2022).
- Estimates of Older People with Vision Loss from the American Community Survey (ACS), Data Source: Table B1310, 2010–2019 Single-Year Data Release. Available online: http://data.census.gov (accessed on 2 July 2022).
- Ministry of Health and Welfare. Disability Statistics Section. Available online: https://dep.mohw.gov.tw (accessed on 2 February 2022).
- Killeen, C. Loneliness: An epidemic in modern society. J. Adv. Nurs. 1998, 28, 762–770. [Google Scholar] [CrossRef]
- Rokach, A. Surviving and coping with loneliness. J. Psychol. 1990, 124, 39–54. [Google Scholar] [CrossRef]
- Rokach, A.; Matalon, R.; Rokach, B.; Safarov, A. The effects of gender and marital status on loneliness of the aged. Soc. Behav. Pers. 2007, 35, 243–254. [Google Scholar] [CrossRef]
- Blazer, D. Depression in late life: Review and commentary. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 249–265. [Google Scholar] [CrossRef] [Green Version]
- Ernst, J.M.; Cacioppo, J.T. Lonely hearts: Psychological perspectives on loneliness. Appl. Prev. Psychol. 1999, 8, 1–22. [Google Scholar] [CrossRef]
- Lynch, T.R.; Compton, J.S.; Mendelson, T.; Robins, C.J.; Krishnan, K.R.R. Anxious depression among the elderly: Clinical and phenomenological correlates. Aging Ment. Health 2000, 4, 268–274. [Google Scholar] [CrossRef]
- Heppe, E.C.; Kef, S.; de Moor, M.H.; Schuengel, C. Loneliness in young adults with a visual impairment: Links with perceived social support in a twenty-year longitudinal study. Res. Dev. Disabil. 2020, 101, 103634. [Google Scholar] [CrossRef] [PubMed]
- Brunes, A.; Hansen, M.B.; Heir, T. Post-traumatic stress reactions among individuals with visual impairments: A systematic review. Disabil. Rehabil. 2018, 41, 2111–2118. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C. Loneliness. In Handbook of Individual Differences in Social Behavior; Leary, M.R., Hoyle, R.H., Eds.; Guilford Press: New York, NY, USA, 2009; pp. 227–240. [Google Scholar]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef] [PubMed]
- Peplau, L.A.; Perlman, D. Theoretical approaches to loneliness. In Loneliness: A Sourcebook of Current Theory, Research and Therapy; Peplau, L.A., Perlman, D., Eds.; Wiley: New York, NY, USA, 1982; pp. 123–134. [Google Scholar]
- Weiss, R.S. Reflections on the present state of loneliness research. In Loneliness: Theory, Research, and Applications; Hojat, M., Crandall, R., Eds.; Sage: Thousand Oaks, CA, USA, 1987; pp. 1–16. [Google Scholar]
- Weiss, R.S. Issues in the study of loneliness. In Loneliness: A Sourcebook of Current Theory, Research and Therapy; Peplau, L.A., Perlman, D., Eds.; Wiley: New York, NY, USA, 1982; pp. 71–80. [Google Scholar]
- Jindal-Snape, D. Generalization and maintenance of social skills of children with visual impairments: Self-evaluation and the role of feedback. J. Vis. Impair. Blind. 2004, 98, 470–483. [Google Scholar] [CrossRef]
- Cumberland, P.M.; Rahi, J.S. Visual function, social position, and health and life chances: The UK biobank study. JAMA Ophthalmol. 2016, 134, 959–966. [Google Scholar] [CrossRef]
- Brunes, A.B.; Hansen, M.; Heir, T. Loneliness among adults with visual impairment: Prevalence, associated factors, and relationship to life satisfaction. Health Qual. Life Outcomes 2019, 17, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen-Mansfield, J.; Hazan, H.; Lerman, Y.; Shalom, V. Correlates and predictors of loneliness in older-adults: A review of quantitative results informed by qualitative insights. Int. Psychogeriatr. 2016, 28, 557–576. [Google Scholar] [CrossRef]
- Cauce, A.M.; Mason, C.; Gonzales, N.; Hiraga, Y.; Liu, G. Social support during adolescence: Methodological and theoretical considerations. In Social Networks and Social Support in Childhood and Adolescence; Nestmann, F., Hurrelmann, K., Eds.; Walter de Gruyter: New York, NY, USA, 1994; pp. 89–108. [Google Scholar]
- Meeus, W. Psychosocial problems and social support in adolescence. In Social Networks and Social Support in Childhood and Adolescence; Walter de Gruyter & Co.: Berlin, Germany, 1994; pp. 241–255. [Google Scholar]
- Robinson, N.S. Evaluating the nature of perceived support and its relation to perceived self-worth in adolescents. J. Res. Adolesc. 1995, 5, 253–280. [Google Scholar] [CrossRef]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310. [Google Scholar] [CrossRef]
- House, J.S. Work Stress and Social Support; Addison Wesley Publishing Company: Boston, MA, USA, 1981. [Google Scholar]
- Heller, K.; Swindle, R.W.; Dusenbury, L. Component social support processes: Comments and integration. J. Consult. Clin. Psychol. 1986, 54, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Li, J.W. Association between, social support and attitude towards aging among the elderly in China. Chin. Gen. Pract. 2017, 20, 852–858. [Google Scholar]
- Howie, L.O.; Troutman-Jordan, M.; Newman, A.M. Social support and successful aging in assisted living residents. Educ. Gerontol. 2014, 40, 61–70. [Google Scholar] [CrossRef]
- Cohen, S.; Syme, S.L. Issues in the study and application of social support. In Social Support and Health; Cohen, S., Syme, S.L., Eds.; Academic Press: Orlando, FL, USA, 1985; pp. 3–22. [Google Scholar]
- Hale, C.J.; Hannum, J.W.; Espelage, D.L. Social support and physical health: The importance of belonging. J. Am. Coll. Health 2005, 53, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Hurdle, D.E. Social support: A critical factor in women’s health and health promotion. Health Soc. Work 2001, 26, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; p. 413. [Google Scholar]
- Russell, D.W. UCLA loneliness scale (version 3): Reliability, validity, and factor structure. J. Pers. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Mermelstein, R.; Kamarch, T.; Hoberman, H.M. Measuring thefunctional components of social support. In Social Support: Theory, Research and Applications; Sarason, I.G., Sarason, B.R., Eds.; Martinus Nijhoff: Boston, MA, USA, 1985; pp. 73–94. [Google Scholar]
- Chang, S.H.; Yang, M.S. The relationships between the elderly loneliness and its factors of personal attributes, perceived health status and social support. Kaohsiung J. Med. Sci. 1999, 15, 337–347. [Google Scholar]
- Perry, G.R. Loneliness and coping among tertiary-level adult cancer patients in the home. Cancer Nurs. 1990, 13, 293–302. [Google Scholar] [CrossRef]
- Chen, C.H.; Tseng, Y.F.; Wang, S.Y.; Lee, J.N. The prevalence and predictors of postpartum depression. J. Nurs. Res. 1994, 2, 263–274. [Google Scholar]
- Chiu, T.S. The overlooked historical facts: An examination of the judicial yuan interpretation no. 649 in light of changes in work by the visually impaired in Taiwan. Soc. Policy Soc. Work 2009, 13, 55–86. [Google Scholar] [CrossRef]
- Chiu, T.S. Who are the disabled: An examination of the application of icf in light of the history of disability evaluations in Taiwan. Soc. Policy Soc. Work 2011, 15, 187–213. [Google Scholar] [CrossRef]
- Wang, Y.Y. The evolving working styles of visually impaired massage workers and the types of their disadvantaged positions. Taiwan Soc. Res. Q. 2011, 83, 37–93. [Google Scholar] [CrossRef]
- Macdonald, S.J.; Deacon, L.; Nixon, J.; Akintola, A.; Gillingham, A.; Kent, J.; Highmore, L. ‘The invisible enemy’: Disability, loneliness and isolation. Disabil. Soc. 2018, 33, 1138–1159. [Google Scholar] [CrossRef]
- Kirchner, C.; Schmeidler, E.; Todorov, A. Looking at Employment through a Lifespan Telescope: Age, Health and Employment Status of People with Serious Visual Impairment; American Foundation for the Blind: New York, NY, USA, 1999. [Google Scholar]
- Lee, I.S.; Park, S.K. Employment status and predictors among people with visual impairments in South Korea: Results of a national survey. J. Vis. Impair. Blind. 2008, 102, 147–159. [Google Scholar] [CrossRef]
- La Grow, S.J. Employment among working-age members of the Royal New Zealand Foundation for the Blind. J. Vis. Impair. Blind. 2003, 97, 429–433. [Google Scholar] [CrossRef]
- Pavey, S.; Douglas, G.; Corcoran, C. Transition into adulthood and work—Findings from Network 1000. Br. J. Vis. Impair. 2008, 26, 202–216. [Google Scholar] [CrossRef]
- Verstraten, P.F.J.; Brinkmann, W.L.J.H.; Stevens, N.L.; Schouten, J.S.A.G. Loneliness, adaptation to vision impairment, social support and depression among visually impaired elderly. In International Congress Series; Elsevier: London, UK, 2005; pp. 317–321. [Google Scholar]
- De Jong Gierveld, J.; Van Tilburg, T.; Dykstra, P.A. Loneliness and social isolation. In Cambridge Handbook of Personal Relationships; Vangelisti, A., Perlman, D., Eds.; Cambridge University Press: Cambridge, UK, 2006; pp. 485–500. [Google Scholar]
- Golden, J.; Conroy, R.M.; Bruce, I.; Denihan, A.; Greene, E.; Kirby, M.; Lawlor, B.A. Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. Int. J. Geriatr. Psychiatry 2009, 24, 694–700. [Google Scholar] [CrossRef]
- Heravi-Karimooi, M.; Anoosheh, M.; Foroughan, M.; Sheykhi, M.T.; Hajizadeh, E. Understanding loneliness in the lived experiences of Iranian elders. Scand. J. Caring. Sci. 2010, 24, 274–280. [Google Scholar] [CrossRef]
- Nilsson, B.; Lindström, U.A.; Naden, D. Is loneliness a psychological dysfunction? A literary study of the phenomenon of loneliness. Scand. J. Caring. Sci. 2006, 20, 93–101. [Google Scholar] [CrossRef]
- Fenwick, E.; Rees, G.; Pesudovs, K.; Dirani, M.; Kawasaki, R.; Wong, T.Y. Social and emotional impact of diabetic retinopathy: A review. Clin. Exp. Ophthalmol. 2012, 40, 27–38. [Google Scholar] [CrossRef] [Green Version]
- Nelson, J.; Kleiner, B.H. How to accommodate common disabilities in organizations. Equal Oppor. Int. 2001, 20, 146–151. [Google Scholar] [CrossRef]
- Rumrill, P.D.; Scheft, C.M. Increasing participation in the accommodation process among persons with visual impairments and blindness: A call to action in the ADA era. J. Vis. Impair. Blind. 1989, 91, 460–466. [Google Scholar] [CrossRef]
- Mellor, D.; Stokes, M.; Firth, L.; Hayashi, Y.; Cummins, R. Need for belonging, relationship satisfaction, loneliness, and life satisfaction. Pers. Individ. Differ. 2008, 45, 213–218. [Google Scholar] [CrossRef]
- Krause, N. Common facets of religion, unique facets of religion, and life satisfaction among older African Americans. J. Gerontol. B Psychol. Sci. Soc. Sci. 2004, 59, S109–S117. [Google Scholar] [CrossRef] [Green Version]
- Koenig, H.G.; Cohen, H.J.; George, L.K.; Hays, J.C.; Larson, D.B.; Blazer, D.G. Attendance at religious services, interleukin-6, and other biological parameters of immune function in older adults. Int. J. Psychiatry Med. 1997, 27, 233–250. [Google Scholar] [CrossRef]
- Levin, J.S.; Chatters, L.M. (Religion, health, and psychological well-being in older adults: Findings from three national surveys. J. Aging Health 1998, 10, 504–531. [Google Scholar] [CrossRef] [Green Version]
- McCullough, M.E.; Hoyt, W.T.; Larson, D.B.; Koenig, H.G.; Thoresen, C. Religious involvement and mortality: A meta-analytic review. Health Psychol. 2000, 19, 211–222. [Google Scholar] [CrossRef]
- Strawbridge, W.J.; Shema, S.J.; Cohen, R.D.; Kaplan, G.A. Religious attendance increases survival by improving and maintaining good health behaviors, mental health, and social relationships. Ann. Behav. Med. 2001, 23, 68–74. [Google Scholar] [CrossRef]
- Brennan, M. Spirituality and psychosocial development in middle-age and older adults with vision loss. J. Adult. Dev. 2002, 9, 31–46. [Google Scholar] [CrossRef]
- Cohen, S. Social relationships and health. Am. Psychol. 2004, 59, 676. [Google Scholar] [CrossRef]
- Tsai, C.F. A Study of Social Support and Resilience in Visually Impaired Adults. Master’s Thesis, Institute for Rehabilitation Counseling, National Taiwan Normal University, Taipei, Taiwan, 2016. Unpublished Master’s Thesis. [Google Scholar]
- Wang, C.W.; Chan, C.L.W.; Ho, A.H.Y.; Xiong, Z. Social networks and health-related quality of life among Chinese older adults with vision impairment. J. Aging Health 2008, 20, 804–823. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.W.; Chan, C.L.W.; Ho, A.H.Y.; Xiong, Z. The impact of spirituality on health-related quality of life among Chinese older adults with vision impairment. Aging Ment. Health 2008, 12, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Wortman, C.B.; Conway, T.L. The role of social support in adaptation and recovery from physical illness. In Social Support and Health; Cohen, S., Syme, S.L., Eds.; Academic Press: Cambridge, MA, USA, 1985; pp. 281–302. [Google Scholar]
- Huurre, T.; Aro, H. The psychosocial Weil-being of Finnish adolescents with visual impairments versus those with chronic conditions and those with no disabilities. J. Vis. Impair. Blind. 2000, 94, 625–637. [Google Scholar] [CrossRef]
- Beach, J.D.; Robinet, J.M.; Hakim-Larson, J. Self-esteem and independent living skills of adults with visual impairments. J. Vis. Impair. Blind. 1995, 89, 531–540. [Google Scholar] [CrossRef]
- Ponchillia, P.E.; Strause, B.; Ponchillia, S.V. Athletes with visual impairments: Attributes and sports participation. J. Vis. Impair. Blind. 2002, 96, 267–272. [Google Scholar] [CrossRef]
- Tuttle, D.W.; Tuttle, N.R. Self-Esteem and Adjusting with Blindness; Charles C Thomas: Springfield, IL, USA, 1996. [Google Scholar]
- Chen, M.J.; Ke, R.Y. A Preliminary Study of Career Resilience of Adults with Visual Impairment. J. Disabil. Res. 2017, 15, 164–181. [Google Scholar]
- Johnson, C.L.; Catalano, D.J. Childless elderly and their family supports. Gerontologist 1981, 21, 610–618. [Google Scholar] [CrossRef]
- Jones, N.; Barlett, H.E.; Cooke, R. An analysis of the impact of visual impairment on activities of daily living and vision related quality of life in a visually impaired adult population. Br. J. Vis. Impair. 2018, 37, 50–63. [Google Scholar] [CrossRef] [Green Version]
- Barron, C.R.; Foxall, M.J.; Dollen, K.; Jones, P.A.; Shull, K.A. Marital status, social support, and loneliness in visually impaired elderly people. J. Adv. Nurs. 1994, 19, 272–280. [Google Scholar] [CrossRef]
- Huang, J.H. A Study of Blind Individuals’ Perception of Marriage. Master’s Thesis, The Institute of Science Education, National Changhua Normal University, Changhua, Taiwan, 2003. [Google Scholar]
- Chu, S.Y.; Li, P.Y. Restrictive world of the vision, lightened road in the future—A narrative research of the interactive experience between the employers and the paracounselor with visual impairment. Disabil. Res. Q. 2010, 8, 275–290. [Google Scholar]
- Mai, H.L. Perspectives from Inside: Employment Experience of Acquired Visually Impaired under the Ecological System Theory. Master’s Thesis, Institute of Labor Relations, National Chung Cheng University, Chiayi, Taiwan, 2014. [Google Scholar]
- Kuo, M.L.; Lin, H.C. The construction of working models for the capacity for resilience in adults with acquired blindness. Bul. Spec. Educ. 2009, 34, 47–80. [Google Scholar]
- Shanas, E. The family as a social support system in old age. Gerontologist 1979, 19, 169–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, D.; Rhind, D.J.A. Barriers and enablers for visually impaired students at a UK Higher Education Institution. Br. J. Vis. Impair. 2011, 29, 177–195. [Google Scholar] [CrossRef]
- Gong, X.; Ni, Z.; Wu, B. The mediating roles of functional limitations and social support on the relationship between vision impairment and depressive symptoms in older adults. Ageing Soc. 2020, 40, 465–479. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.L.; Gao, Y.; Wan, B.H.; Zou, L.H. Analysis on the social support to the elderly in empty-nest families in city. Med. Soc. 2008, 21, 11–12. [Google Scholar]
- McLaughlin, D.; Adams, J.; Vagenas, D.; Dobson, A. Factors which enhance or inhibit social support: A mixed-methods analysis of social networks in older women. Ageing Soc. 2011, 31, 18–33. [Google Scholar] [CrossRef] [Green Version]
- Van Huijgevoort, T. Coping with a visual impairment through self-investigation. J. Vis. Impair. Blind. 2002, 96, 783–795. [Google Scholar] [CrossRef]
- Papakonstantinou, D. Relationships between individual characteristics and occupational possibilities for young adults with visual impairments. Br. J. Vis. Impair. 2020, 38, 137–150. [Google Scholar] [CrossRef]
- Chu, M.H.; Lu, S.C.; Chen, C.H.; Wu, H.C. The difficulties between life rehabilitation and vocational rehabilitation of visual impairment in Taiwan. Disabil. Res. Q. 2018, 16, 220–233. [Google Scholar]
- McQuaid, R.J.; Cox, S.M.; Ogunlana, A.; Jaworska, N. The burden of loneliness: Implications of the social determinants of health during COVID-19. Psychiatry Res. 2020, 296, 113648. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Gender | |
| Male | 272 (59.6) |
| Female | 184 (40.4) |
| Average age | 54.1 (7.8) years |
| Educational level | |
| Junior and below | 122 (26.8) |
| Senior high | 196 (42.9) |
| College and university | 94 (20.6) |
| Graduate school | 44 (9.6) |
| Marital status | |
| Single | 154 (33.8) |
| Married | 240 (52.6) |
| Others (divorced) | 62 (13.6) |
| Types of job | |
| White collar | 20 (4.4) |
| Blue collar | 254 (55.7) |
| Others | 22 (4.8) |
| Unemployed | 160 (35.0) |
| Monthly salary | |
| USD 525 and below | 182 (37.9) |
| USD 526–1050 | 135 (29.6) |
| USD 1051~1580 | 83 (18.2) |
| USD 158~2100 | 36 (7.9) |
| USD 2100 and above | 20 (4.4) |
| Average salary | USD 737.2 |
| Religion | |
| Buddhism | 96 (21.1) |
| Taoism | 128 (28.1) |
| Christianity | 42 (9.2) |
| Catholic | 10 (2.2) |
| Other religions | 28 (6.1) |
| None | 152 (33.3) |
| Living Style | |
| Living alone | 72 (15.8) |
| Living with family | 350 (76.8) |
| Living with friends and family | 16 (3.5) |
| Other | 18 (3.9) |
| Ability to move independently | |
| Able to act independently | 302 (66.2) |
| Not able to act independently | 154 (33.8) |
| Ability to go out alone (n = 302) | |
| Using the cane | 249 (82.5) |
| Using residual vision | 44 (14.6) |
| Using guide dogs | 9 (2.9) |
| Causes of Blindness | |
| Disease | 250 (54.8) |
| Congenital blindness | 154 (33.8) |
| Other (accidental injury) | 52 (11.4) |
| Important support and companionship in life | |
| Parents | 158 (34.64) |
| Spouse | 146 (32.01) |
| Children | 65 (14.25) |
| Siblings | 64 (14.03) |
| Relatives and friends | 14 (0.30) |
| Volunteers | 9 (0.01) |
| Loneliness Classification | Minimum Value | Maximum Value | n | (%) |
|---|---|---|---|---|
| Low level | 22 | 34 | 90 | 19.7% |
| Indicated a moderate level | 36 | 47 | 224 | 49.1% |
| Indicated a moderately high level | 52 | 64 | 134 | 29.4% |
| Indicated a high level | 65 | 70 | 8 | 1.8% |
| Variable | Groups | n | Mean ± SD 44.05 ± 8.62 | p-Value | Scheffe’s Post Hoc |
|---|---|---|---|---|---|
| Gender | Male | 272 | 43.15 ± 9.72 | T = 1.539 | |
| Female | 184 | 44.47 ± 9.55 | |||
| Age (years) | 45–50 | 190 | 43.99 ± 9.02 | F = 2.424 | |
| 51–60 | 160 | 45.98 ± 8.83 | |||
| 61–70 | 106 | 41.24 ± 8.26 | |||
| Educational level | Junior and below | 122 | 43.48 ± 8.39 | F = 1.834 | |
| Senior high | 196 | 44.62 ± 9.36 | |||
| College and university | 94 | 46.05 ± 6.74 | |||
| Graduate school | 44 | 45.05 ± 8.62 | |||
| Marital status | Single | 154 | 44.30 ± 9.00 | F = 2.394 | |
| Married | 240 | 43.77 ± 8.63 | |||
| Others (divorced) | 62 | 45.19 ± 6.74 | |||
| Have a job or not | Yes | 296 | 43.20 ± 8.35 | T = −3.211 *** | 2 > 1 |
| No | 160 | 47.16 ± 8.76 | |||
| Types of job | White collar | 20 | 44.00 ± 7.19 | F = 1.118 | |
| Blue collar | 254 | 43.95 ± 8.47 | |||
| Others | 22 | 43.36 ± 8.68 | |||
| Unemployed | 160 | 47.76 ± 8.76 | |||
| Monthly salary | USD 525 and below | 182 | 45.21 ± 8.84 | F = 11.344 *** | 4 > 3, 4 > 2, 4 > 1 |
| USD 526–1050 | 135 | 44.96 ± 9.32 | p = 0.000 | ||
| USD 1051~1580 | 83 | 43.56 ± 8.84 | |||
| USD 1580~2100 (and above) | 56 | 39.20 ± 5.50 | |||
| Religious | Yes | 304 | 43.97 ± 7.16 | T = −3.204 *** | |
| No | 152 | 48.68 ± 7.31 | p = 0.000 | ||
| Religion | Buddhism | 96 | 41.27 ± 7.34 | F = 1.594 | |
| Taoism | 128 | 44.14 ± 7.59 | |||
| Christianity | 42 | 40.76 ± 9.64 | |||
| Catholic | 10 | 45.40 ± 7.29 | |||
| Other religions | 28 | 45.20 ± 11.76 | |||
| Lifestyle | Living alone | 72 | 47.40 ± 7.38 | F = 10.528 *** | 1 > 2, 1 > 3 |
| Living with family | 350 | 40.88 ± 8.80 | p = 0.000 | ||
| Living with friends and family | 16 | 42.87 ± 4.30 | |||
| Others | 18 | 41.00 ± 7.83 | |||
| Ability to move independently | Yes | 302 | 42.64 ± 8.48 | T = −5.042 *** | 1 > 2 |
| No | 154 | 47.83 ± 8.25 | p = 0.000 | ||
| Cause of visual impairment | Disease | 250 | 43.56 ± 9.78 | F = 1.901 | |
| Congenital blindness | 154 | 45.29 ± 11.00 | p = 0.151 | ||
| Other (accidental injury) | 52 | 42.88 ± 10.14 |
| Four Dimensions of Social Support | Minimum Value | Maximum Value | Mean ± SD | Ranking |
|---|---|---|---|---|
| Emotional or appraisal support | 4.00 | 16.00 | 9.56 ± 2.89 | 3 |
| Instrumental or tangible support | 4.00 | 18.00 | 9.20 ± 3.52 | 4 |
| Companionship or belonging support | 4.00 | 39.00 | 9.74 ± 3.54 | 2 |
| Self-esteem support | 4.00 | 16.00 | 9.96 ± 2.94 | 1 |
| Total score and mean ± SD | 16.00 | 63.00 | 38.63 ± 9.95 |
| Variable | Groups | n | Mean ± SD 38.63 ± 9.95 | p-Value | Scheffe’s Post hoc |
|---|---|---|---|---|---|
| Gender | Male | 272 | 37.86 ± 9.39 | T = −1.358 | |
| Female | 184 | 39.15 ± 10.30 | |||
| Age (years) | 45–50 | 190 | 38.32 ± 9.71 | F = 2.191 | |
| 51–60 | 160 | 39.86 ± 10.93 | p = 0.113 | ||
| 61–70 | 106 | 37.35 ± 8.20 | |||
| Educational level | Junior and below | 122 | 35.96 ± 10.06 | F = 4.519 ** | 4 > 1 |
| Senior high | 196 | 38.45 ± 9.86 | p = 0.004 | ||
| College and university | 94 | 39.43 ± 9.69 | |||
| Graduate school | 44 | 42.98 ± 10.01 | |||
| Marital status | Single | 154 | 36.97 ± 10.18 | F = 7.697 ** | 2 > 1 |
| Married | 240 | 40.08 ± 10.05 | p = 0.001 | ||
| Others (divorced) | 62 | 39.18 ± 7.45 | |||
| Have a job or not | Yes | 296 | 39.90 ± 9.32 | T = −3.360 *** | 1 > 2 |
| No | 160 | 37.04 ± 8.88 | p = 0.000 | ||
| Types of job | White collar | 20 | 39.60 ± 6.49 | F = 2.504 | |
| Blue collar | 254 | 37.94 ± 10.09 | p = 0.054 | ||
| Others | 22 | 38.36 ± 10.81 | |||
| Unemployed | 160 | 37.74 ± 8.88 | |||
| Monthly salary | USD 525 and below | 182 | 36.66 ± 9.41 | F = 6.865 * | 4 > 1 |
| USD 526–1050 | 135 | 39.55 ± 9.90 | p = 0.023 | ||
| USD 1051~1580 | 83 | 38.94 ± 10.07 | |||
| USD 1580~2100 (and above) | 56 | 41.27 ± 9.70 | |||
| Religious | Yes | 304 | 39.25 ± 7.16 | T = 1.586 | |
| No | 152 | 37.75 ± 7.31 | |||
| Religion | Buddhism | 96 | 39.33 ± 10.91 | F = 1.856 | |
| Taoism | 128 | 39.69 ± 8.27 | p = 0.118 | ||
| Christianity | 42 | 42.00 ± 11.24 | |||
| Catholic | 10 | 34.20 ± 11.45 | |||
| Other religions | 28 | 37.42 ± 7.95 | |||
| Lifestyle | Living alone | 72 | 35.47 ± 9.47 | F = 7.719 *** | 2 > 1, 2 > 4 |
| Living with family | 350 | 39.34 ± 10.07 | p = 0.000 | ||
| Living with friends and family | 16 | 37.00 ± 4.06 | |||
| Other (placement) | 18 | 35.00 ± 7.09 | |||
| Ability to move independently | Yes | 302 | 39.44 ± 10.85 | T = 3.116 * | 1 > 2 |
| No | 154 | 37.16 ± 7.75 | p = 0.035 | ||
| Cause of visual impairment | Disease | 250 | 38.75 ± 10.03 | F = 1.850 | |
| Congenital blindness | 154 | 37.73 ± 9.40 | p = 0.159 | ||
| Other (accidental injury) | 52 | 40.76 ± 10.98 |
| Loneliness | 1 | 2 | 3 | |
|---|---|---|---|---|
| Social support | −0.572 *** | |||
| Emotional or appraisal support | −0.471 *** | |||
| Instrumental or tangible support | −0.556 *** | 0.752 *** | ||
| Companionship or belonging support | −0.521 *** | 0.726 *** | 0.736 *** | |
| Self-esteem | −0.608 *** | 0.628 *** | 0.484 *** | 0.529 *** |
| Order of Variables Entered | R | R Square R2 | R Square Change | F Change | Sig. F Change | Standardized Coefficients Beta |
|---|---|---|---|---|---|---|
| Self-esteem | 0.342 | 0.117 | 0.117 | 40.118 | 0.000 | −0.227 |
| Instrumental or tangible support | 0.410 | 0.168 | 0.050 | 30.326 | 0.001 | −0.204 |
| Companionship or belonging support | 0.457 | 0.198 | 0.040 | 26.385 | 0.001 | −0.193 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, H.-Y.; Chan, H.-S. Loneliness and Social Support among the Middle-Aged and Elderly People with Visual Impairment. Int. J. Environ. Res. Public Health 2022, 19, 14600. https://doi.org/10.3390/ijerph192114600
Chu H-Y, Chan H-S. Loneliness and Social Support among the Middle-Aged and Elderly People with Visual Impairment. International Journal of Environmental Research and Public Health. 2022; 19(21):14600. https://doi.org/10.3390/ijerph192114600
Chicago/Turabian StyleChu, Hui-Ying, and Hui-Shan Chan. 2022. "Loneliness and Social Support among the Middle-Aged and Elderly People with Visual Impairment" International Journal of Environmental Research and Public Health 19, no. 21: 14600. https://doi.org/10.3390/ijerph192114600