

Epidemiological Profile and Social Welfare Index as Factors Associated with COVID-19 Hospitalization and Severity in Mexico City: A Retrospective Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Collection
2.3. Data Analytic Strategy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Oju, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lipsitch, M.; Phil, D.; Swerdlow, D.L.; Finelli, L. Defining the Epidemiology of COVID-19—Studies Needed. N. Engl. J. Med. 2020, 382, 1194–1195. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Coronavirus Disease (COVID-19) Outbreak Situation. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 16 October 2022).
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.; Alpha-Sall, A.; et al. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/region/amro/country/mx (accessed on 16 October 2022).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 16 October 2022).
- Denova, E.; López-Gatell, H.; Alomia, J.L.; López, R.; Zaragoza, C.A.; Dyer, D.D.; Cortés, R.; Villa, T.; Gutiérrez, R.; Rodríguez, K.; et al. The association between obesity, type 2 diabetes, and hypertension with severe COVID-19 on admission among Mexicans. Obesity 2020, 28, 1826–1832. [Google Scholar] [CrossRef]
- Hernández, D.R.; González, M.A.; Romo, D.K.; Lima, R.; Hernández, I.A.; Lumbreras, M.; Méndez, P. Increased Risk of Hospitalization and Death in Patients with COVID-19 and Pre-existing Noncommunicable Diseases and Modifiable Risk Factors in Mexico. Arch. Med. Res. 2020, 51, 683.e89. [Google Scholar] [CrossRef] [PubMed]
- Hernández, A.; Azañedo, D.; Vargas, R.; Bendezu, G. Association of Comorbidities with Pneumonia and Death Among COVID-19 Patients in Mexico: A Nationwide Cross-sectional Study. J. Prev. Med. Public Health 2020, 53, 211–219. [Google Scholar] [CrossRef]
- Carrillo, M.F.; Salinas, G.; García, C.; Gutiérrez, L.M.; Parra, L. Early estimation of the risk factors for hospitalization and mortality by COVID-19 in Mexico. PLoS ONE 2020, 15, e0238905. [Google Scholar] [CrossRef]
- Fernández, M.A.; Luna, M.A.; Campos, A.; Calva, D.Y.; Moreno, J.L.; Langle, A.P.; García, A.; Solís, C.J.; Canizales, A.; León, N.; et al. Epidemiology of COVID-19 in Mexico: Symptomatic profiles and presymptomatic people. Int. J. Infect. Dis. 2021, 104, 572–579. [Google Scholar] [CrossRef]
- Gershengorn, H.B.; Patel, S.; Shukla, B.; Warde, P.R.; Bhatia, M.; Parekh, D.; Ferreira, T. Association of Race and Ethnicity with COVID-19 Test Positivity and Hospitalization Is Mediated by Socioeconomic Factors. Ann. Am. Thorac. Soc. 2021, 18, 1326–1334. [Google Scholar] [CrossRef]
- Little, C.; Alsen, M.; Barlo, J.; Naymagon, L.; Tremblay, D.; Genden, E.; Trosman, S.; Iavicoli, L.; van Gerwen, M. The Impact of Socioeconomic Status on the Clinical Outcomes of COVID-19; a Retrospective Cohort Study. J. Community Health 2021, 46, 794–802. [Google Scholar] [CrossRef]
- Foster, H.; Ho, F.; Mair, F.; Jani, B.; Sattar, N.; Katikireddi, S.; Pell, J.P.; Niedzwiedz, C.L.; Hastie, C.E.; Anderson, J.; et al. The association between a lifestyle score, socioeconomic status, and COVID-19 outcomes within the UK Biobank cohort. BMC Infect. Dis. 2022, 22, 273. [Google Scholar] [CrossRef] [PubMed]
- Tang, I.W.; Vieira, V.M.; Shearer, E. Effect of socioeconomic factors during the early COVID-19 pandemic: A spatial analysis. BMC Public Health 2022, 22, 1212. [Google Scholar] [CrossRef]
- Smith, M.D.; Wesselbaum, D. COVID-19, Food Insecurity, and Migration. J. Nutr. 2020, 150, 2855–2858. [Google Scholar] [CrossRef] [PubMed]
- Burström, B.; Tao, W. Social determinants of health and inequalities in COVID-19. Eur. J. Public Health 2020, 30, 617–618. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.M., II; Anyane-Yeboa, A.; Balzora, S.; Issaka, R.B.; May, F.P. COVID-19 and the other pandemic: Populations made vulnerable by systemic inequity. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Khalatbari-Soltani, S.; Cumming, R.C.; Delpierre, C.; Kelly-Irving, M. Importance of collecting data on socioeconomic determinants from the early stage of the COVID-19 outbreak onwards. J. Epidemiol. Community Health 2020, 74, 620–623. [Google Scholar] [CrossRef] [PubMed]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Producto Interno Bruto por Entidad Federativa 2019. Comunicado de Prensa Núm. 632/20 INEGI. pp. 1–13. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/boletines/2020/OtrTemEcon/PIBEntFed2019.pdf (accessed on 9 December 2020).
- Índice de Bienestar Social de la Ciudad de México. Consejo de Evaluación del Desarrollo Social de la Ciudad de México. 2016, pp. 1–69. Available online: http://data.evalua.cdmx.gob.mx/docs/estudios/edf2016/IBS-CDMX%20Versi%C3%B3n%20Final.pdf (accessed on 13 February 2021).
- Gobierno de México. Secretaria de Salud. [Internet] Update: COVID-19 México. Available online: https://datos.covid-19.conacyt.mx/ (accessed on 2 September 2022).
- Lineamiento Estandarizado para la Vigilancia Epidemiológica y por Laboratorio de la Enfermedad Respiratoria Viral. Gobierno de México. Secretaria de Salud. Dirección General de Epidemiología. 2020, pp. 1–74. Available online: https://coronavirus.gob.mx/wp-content/uploads/2020/04/Lineamiento_de_vigilancia_epidemiologica_de_enfermedad_respiratoria-_viral.pdf (accessed on 26 February 2021).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Hernández, E. Obesity is the comorbidity more strongly associated for COVID-19 in Mexico. A case-control study. Obes. Res. Clin. Pract. 2020, 14, 375–379. [Google Scholar] [CrossRef]
- Suárez, V.; Suárez, M.; Oros, S.; Ronquillo de Jesús, E. Epidemiología de COVID-19 en México: Del 27 de febrero al 30 de abril de 2020. Rev. Clin. Esp. 2020, 220, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Ortíz, E.; Villanueva, M.; González, M.F.; Tamez, K.M.; Román, C.M.; Díaz, B.A.; Pérez, E.; Olivas, A.; Rajme, S.; Martínez, B.A.; et al. Clinical and Epidemiological Characteristics of Patients Diagnosed with COVID-19 in a Tertiary Care Center in Mexico City: A Prospective Cohort Study. Rev. Investig. Clin. 2020, 72, 165–177. [Google Scholar] [CrossRef]
- Córdoba, J.A.; Macías, A.E.; Hernández, M.; Dominguez, G.; López-Gatell, H.; Alpuche, C.; Ponce de León, S. The 2009 pandemic in Mexico: Experience and lessons regarding national preparedness policies for seasonal and epidemic influenza. Gac. Med. Mex. 2017, 153, 93–101. Available online: http://www.anmm.org.mx/GMM/2017/n1/GMM_153_2017_1_102-110.pdf (accessed on 11 March 2021).
- Parra, G.M.; López, N.; Parra, F.E. Clinical characteristics and risk factors for mortality of patients with COVID-19 in a large data set from Mexico. Ann. Epidemiol. 2020, 52, 93.e98. [Google Scholar] [CrossRef]
- Murillo, E.; Hernandez, C.M. Survival in adult inpatients with COVID-19. Public Health 2021, 190, 1.e3. [Google Scholar] [CrossRef]
- Salinas, G.; Carillo, M.F.; Granados, V.; Martínez, S.; Toledano, F.; Garduño, E. A survival analysis of COVID-19 in the Mexican population. BMC Public Heatlh 2020, 20, 1616. [Google Scholar] [CrossRef]
- Bello, O.Y.; González, A.; Antonio, N.E.; Fermín, C.A.; Márquez, A.; Vargas, A.; Bahena, J.P.; García, C.; Aguilar, C.A.; Gutiérrez, L.M. Unequal Impact of Structural Health Determinants and Comorbidity on COVID-19 Severity and Lethality in Older Mexican Adults: Considerations Beyond Chronological Aging. Gerontol. A Biol. Sci. Med. Sci. 2020, 76, e52–e59. [Google Scholar] [CrossRef]
- Antonio, N.E.; Fernandez, L.; Pisanty, J.; Mancilla, J.; Kammar, A.; Vargas, A.; González, A.; Fermín, C.A.; Márquez, A.; Guerra, E.C.; et al. Comprehensive Evaluation of the Impact of Sociodemographic Inequalities on Adverse Outcomes and Excess Mortality During the Coronavirus Disease 2019 (COVID-19) Pandemic in Mexico City. Clin. Infect. Dis. 2022, 74, 785–792. [Google Scholar] [CrossRef]
- Ortíz, L.; Pérez, M.A. Inequidades sociales en la progresión de la COVID-19 en población mexicana. Rev. Panam. Salud. Publica 2020, 44, e106. [Google Scholar] [CrossRef]
- Méndez, N.; Álvarez, A.; Carrillo, G. Demographic and Health Indicators in Correlation to Interstate Variability of Incidence, Confirmation, Hospitalization, and Lethality in Mexico: Preliminary Analysis from Imported and Community Acquired Cases during COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 4281. [Google Scholar] [CrossRef]
- Gutiérrez, J.P.; Bertozzi, S.M. Non-communicable diseases and inequalities increase risk of death among COVID-19 patients in Mexico. PLoS ONE 2020, 15, e0240394. [Google Scholar] [CrossRef]
- Irigoyen, M.E.; Velázquez, M.C.; Zepeda, M.A.; Cabrer, M.F.; Lazarevich, I.; Castaño, A. Effect of Income Level and Perception of Susceptibility and Severity of COVID-19 on Stay-at-Home Preventive Behavior in a Group of Older Adults in Mexico City. Int. J. Environ. Res. Public Health 2020, 17, 7418. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
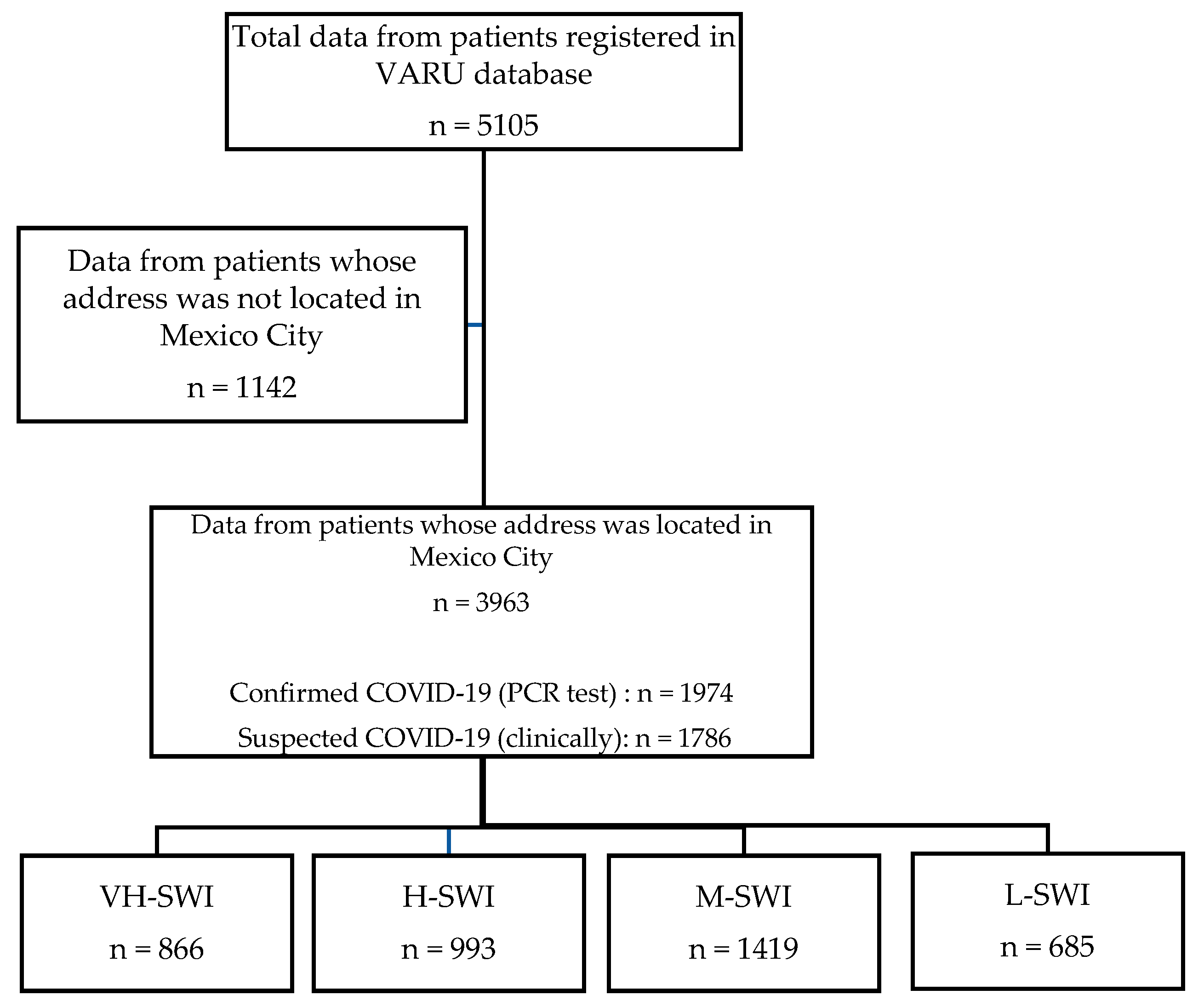
| Characteristics | All n = 3963 | VH-SWI n = 866 | H-SWI n = 993 | M-SWI n = 1419 | L-SWI n = 685 | p |
|---|---|---|---|---|---|---|
| Demographic | ||||||
| Sex n (%) | ||||||
| Female | 1770 (44.7) | 396 (45.7) | 429 (43.2) | 636 (44.8) | 309 (45.1) | 0.72 |
| Male | 2193 (55.3) | 470 (54.3) | 564 (56.8) | 783 (55.2) | 376 (54.9) | |
| Age (years) | 45 (29–56) | 43 (29–55) | 45 (29–56) | 46 (29–57) | 45 (30–57) | 0.04 |
| Age n (%) | ||||||
| <19 years | 339 (8.6) | 84 (9.7) | 83 (8.4) | 125 (8.8) | 47 (6.9) | 0.12 |
| 19–59 years | 2900 (73.2) | 647 (74.8) | 732 (73.7) | 1015 (71.6) | 506 (74.0) | |
| >60 years | 721 (18.2) | 134 (15.5) | 178 (17.9) | 278 (19.6) | 131 (19.2) | |
| Comorbidities n (%) | ||||||
| Diabetes | 1011 (25.5) | 204 (23.6) | 260 (26.2) | 382 (26.9) | 165 (24.1) | 0.03 |
| Hypertension | 1186 (29.9) | 244 (28.2) | 325 (32.7) | 425 (30.0) | 192 (28.0) | <0.01 |
| Obesity | 903 (22.8) | 176 (20.3) | 215 (21.8) | 309 (21.8) | 203 (29.6) | <0.001 |
| COPD | 169 (4.3) | 38 (4.4) | 54 (5.4) | 45 (3.2) | 32 (4.7) | <0.01 |
| Asthma | 110 (2.8) | 27 (3.1) | 31 (3.1) | 29 (2.0) | 23 (3.4) | 0.01 |
| Immunosuppression | 130 (3.3) | 21 (2.4) | 34 (3.4) | 48 (3.4) | 27 (3.9) | 0.21 |
| HIV/AIDS | 20 (0.5) | 7 (0.8) | 8 (0.8) | 2 (0.1) | 3 (0.4) | 0.01 |
| Cardiovascular Disease | 174 (4.4) | 38 (4.4) | 42 (4.2) | 51 (3.6) | 43 (6.3) | <0.01 |
| Chronic Kidney Disease | 210 (5.3) | 44 (5.1) | 48 (4.8) | 75 (5.3) | 43 (6.3) | 0.11 |
| Others | 146 (3.7) | 27 (3.1) | 42 (4.2) | 46 (3.2) | 31 (4.5) | 0.05 |
| No. of comorbidities n (%) | ||||||
| 0 | 1634 (41.2) | 369 (42.7) | 411 (41.4) | 598 (42.1) | 256 (37.4) | |
| 1 | 1092 (27.6) | 231 (26.7) | 266 (26.8) | 378 (26.6) | 217 (31.7) | 0.03 |
| 2 | 710 (17.9) | 158 (18.2) | 159 (16.0) | 262 (18.5) | 131 (19.1) | |
| >3 | 527 (13.3) | 108 (12.5) | 157 (15.8) | 181 (12.8) | 81 (11.8) | |
| Pregnancy n (%) | 19 (0.5) | 4 (1.0) | 2 (0.5) | 8 (1.3) | 5 (1.6) | 0.68 |
| Smoke history n (%) | 514 (13.0) | 125 (14.4) | 118 (11.9) | 153 (10.8) | 118 (17.2) | <0.001 |
| HAS n (%) | ||||||
| Triage | 741 (18.7) | 199 (23.0) | 184 (18.5) | 228 (16.1) | 130 (19.0) | |
| Medical specialty | 1064 (26.8) | 225 (26.0) | 249 (25.1) | 398 (28.0) | 192 (28.0) | |
| Emergency | 2073 (52.3) | 431 (49.8) | 542 (54.6) | 752 (53.0) | 348 (50.8) | |
| Pediatric ICU’s | 35 (0.9) | 3 (0.3) | 3 (0.3) | 18 (1.3) | 11 (1.6) | <0.001 |
| Adult ICU’s | 50 (1.3) | 8 (0.9) | 15 (1.5) | 23 (1.6) | 4 (0.6) | |
| Characteristics | All n = 3963 | VH-SWI n = 866 | H-SWI n = 993 | M-SWI n = 1419 | L-SWI n = 685 | p |
|---|---|---|---|---|---|---|
| Symptoms n (%) | ||||||
| Pneumonia | 2392 (60.4) | 450 (52.3) | 631 (63.7) | 938 (66.3) | 373 (54.6) | <0.001 |
| ARDS | 2578 (65.1) | 544 (62.8) | 658 (66.3) | 1014 (71.5) | 362 (52.8) | <0.001 |
| Fever | 2846 (71.8) | 586 (67.7) | 685 (69.0) | 1117 (78.7) | 458 (66.9) | <0.001 |
| Cough | 2977 (75.1) | 610 (70.4) | 738 (74.3) | 1152 (81.2) | 477 (69.6) | <0.001 |
| Dyspnea | 2342 (59.1) | 445 (51.4) | 599 (60.3) | 927 (65.3) | 371 (54.2) | <0.001 |
| Odynophagia | 1411 (35.6) | 270 (31.2) | 364 (36.7) | 573 (40.4) | 204 (28.8) | <0.001 |
| Irritability | 743 (18.7) | 139 (16.1) | 161 (16.2) | 285 (20.1) | 158 (23.1) | <0.01 |
| Diarrhea | 908 (22.9) | 178 (20.6) | 229 (23.1) | 334 (23.5) | 167 (24.4) | 0.20 |
| Chest pain | 1296 (32.7) | 255 (29.4) | 312 (31.4) | 498 (35.1) | 231 (33.7) | <0.001 |
| Tremble | 1368 (34.5) | 236 (27.3) | 332 (33.4) | 544 (38.3) | 256 (37.4) | <0.001 |
| Headache | 2763 (69.7) | 595 (68.7) | 675 (68.0) | 1045 (73.6) | 448 (65.4) | <0.001 |
| Myalgia | 2055 (51.9) | 415 (47.9) | 529 (53.3) | 782 (55.1) | 329 (48.0) | <0.001 |
| Arthralgia | 2019 (50.9) | 426 (49.2) | 505 (50.9) | 774 (54.5) | 314 (45.8) | <0.001 |
| Rhinorrhea | 1038 (26.2) | 209 (24.1) | 257 (25.9) | 406 (28.6) | 166 (24.2) | <0.001 |
| Polypnea | 687 (17.3) | 106 (12.2) | 167 (16.8) | 317 (22.3) | 97 (14.2) | <0.001 |
| Vomiting | 379 (9.6) | 72 (8.3) | 99 (10.0) | 145 (10.2) | 63 (9.2) | <0.001 |
| Abdominal pain | 607 (15.3) | 130 (15.0) | 138 (13.9) | 223 (15.7) | 116 (16.9) | <0.001 |
| Conjunctivitis | 549 (13.9) | 96 (11.1) | 125 (12.6) | 213 (15.0) | 115 (16.8) | <0.001 |
| Cyanosis | 433 (10.9) | 85 (9.8) | 94 (9.5) | 192 (13.5) | 62 (9.1) | <0.001 |
| Anosmia | 203 (5.1) | 31 (3.6) | 57 (5.7) | 67 (4.7) | 48 (7.0) | <0.001 |
| Dysgeusia | 203 (5.1) | 34 (3.9) | 52 (5.2) | 68 (4.8) | 49 (7.2) | <0.01 |
| General health discomfort | 1934 (48.8) | 402 (46.4) | 486 (48.9) | 757 (53.3) | 289 (42.4) | <0.001 |
| SOS | 1848 (46.7) | 432 (49.9) | 471 (47.4) | 741 (52.2) | 205 (29.9) | <0.001 |
| AV treatment n (%) | 837 (21.1) | 151 (18.3) | 154 (16.0) | 462 (33.7) | 70 (10.3) | <0.001 |
| AB treatment n (%) | 2364 (60.2) | 520 (60.8) | 593 (60.5) | 867 (61.6) | 384 (56.4) | 0.14 |
| CPC n (%) | 1609 (40.6) | 357 (47.9) | 399 (43.3) | 548 (42.4) | 305 (50.2) | <0.01 |
| RT-PCR test n (%) | ||||||
| Positive | 1974 (52.5) | 402 (48.5) | 521 (55.7) | 731 (54.2) | 320 (49.4) | |
| Suspected | 1657 (44.1) | 410 (49.5) | 376 (40.2) | 570 (42.3) | 301 (46.5) | <0.01 |
| NA | 129 (3.4) | 17 (2.1) | 38 (4.1) | 47 (3.5) | 27 (4.2) | |
| Clinical Outcomes n (%) | ||||||
| Ambulatory | 1080 (27.3) | 303 (35.0) | 292 (29.4) | 321 (22.6) | 164 (23.9) | <0.001 |
| Hospitalization | 2883 (72.7) | 563 (65.0) | 701 (70.6) | 1098 (77.4) | 521 (76.1) | |
| Mechanical Ventilation | 635 (16.0) | 100 (17.8) | 151 (21.6) | 265 (24.2) | 119 (22.8) | 0.02 |
| Severity Cases | 712 (18.0) | 132 (61.4) | 176 (63.3) | 295 (67.5) | 109 (43.4) | <0.001 |
| Mortality | 876 (22.1) | 155 (17.9) | 256 (25.8) | 337 (23.7) | 128 (18.7) | <0.001 |
| Recovery | 832 (21.0) | 191 (39.1) | 178 (39.1) | 323 (50.5) | 140 (46.2) | <0.001 |
| HMO | 1054 (26.6) | 297 (60.9) | 277 (60.9) | 317 (49.5) | 163 (53.8) | |
| Hospitalization | ||||||
|---|---|---|---|---|---|---|
| Variable | Non-Adjusted Model | Model 1 | Model 2 | |||
| OR | 95%CI | OR | 95%CI | OR | 95%CI | |
| VH-SWI | 1.00 | --- | 1.00 | --- | --- | |
| H-SWI | 1.29 | 1.06–1.57 | 1.27 | 1.04–1.55 | 1.24 | 1.01–1.53 |
| M-SWI | 1.84 | 1.52–2.21 | 1.85 | 1.53–2.23 | 1.90 | 1.56–2.32 |
| L-SWI | 1.71 | 1.36–2.14 | 1.73 | 1.37–2.15 | 1.73 | 1.36–2.19 |
| Mechanical Ventilation | ||||||
| Variable | Non-Adjusted Model | Model 1 | Model 2 | |||
| VH-SWI | 1.00 | --- | 1.00 | --- | 1.00 | --- |
| H-SWI | 1.26 | 0.95–1.68 | 1.24 | 0.93–1.65 | 1.24 | 0.93–1.64 |
| M-SWI | 1.47 | 1.13–1.90 | 1.43 | 1.12–1.86 | 1.45 | 1.11–1.87 |
| L-SWI | 1.36 | 1.01–1.83 | 1.34 | 0.99–1.81 | 1.35 | 1.00–1.82 |
| Severity Cases | ||||||
| Variable | Non-Adjusted Model | Model 1 | Model 2 | |||
| VH-SWI | 1.00 | --- | 1.00 | --- | 1.00 | --- |
| H-SWI | 0.92 | 0.63–1.33 | 0.90 | 0.62–1.30 | 0.90 | 0.62–1.31 |
| M-SWI | 0.76 | 0.54–1-07 | 0.75 | 0.53–1.06 | 0.75 | 0.53–1.06 |
| L-SWI | 2.07 | 1.43–3.00 | 2.04 | 1.41–2.96 | 2.04 | 1.41–2.96 |
| Mortality | ||||||
| Variable | Non-Adjusted Model | Model 1 | Model 2 | |||
| VH-SWI | 1.00 | --- | 1.00 | --- | 1.00 | --- |
| H-SWI | 1.59 | 1.27–1.99 | 1.57 | 1.25–1.97 | 1.54 | 1.22–1.94 |
| M-SWI | 1.42 | 1.15–1.76 | 1.41 | 1.14–1.75 | 1.41 | 1.13–1.76 |
| L-SWI | 1.05 | 0.81–1.36 | 1.04 | 0.80–1.35 | 1.02 | 0.78–1.33 |
| Recovery | ||||||
| Variable | Non-Adjusted Model | Model 1 | Model 2 | |||
| VH-SWI | 1.00 | --- | 1.00 | --- | 1.00 | --- |
| H-SWI | 1.00 | 0.77–1.30 | 1.03 | 0.79–1.35 | 1.06 | 0.81–1.40 |
| M-SWI | 0.63 | 0.49–0.80 | 0.60 | 0.43–0.77 | 0.59 | 0.46–0.76 |
| L-SWI | 0.74 | 0.56–1.00 | 0.73 | 0.54–0.98 | 0.73 | 0.54–1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Téllez-González, M.A.; Pineda-Juárez, J.A.; Suárez-Cuenca, J.A.; Escamilla-Tilch, M.; Santillán-Cortez, D.; García, S.; Alcaraz-Estrada, S.L.; Pérez-Razo, J.C.; Delgado-Quintana, C.A.; Vargas-Hernández, J.; et al. Epidemiological Profile and Social Welfare Index as Factors Associated with COVID-19 Hospitalization and Severity in Mexico City: A Retrospective Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14803. https://doi.org/10.3390/ijerph192214803
Téllez-González MA, Pineda-Juárez JA, Suárez-Cuenca JA, Escamilla-Tilch M, Santillán-Cortez D, García S, Alcaraz-Estrada SL, Pérez-Razo JC, Delgado-Quintana CA, Vargas-Hernández J, et al. Epidemiological Profile and Social Welfare Index as Factors Associated with COVID-19 Hospitalization and Severity in Mexico City: A Retrospective Analysis. International Journal of Environmental Research and Public Health. 2022; 19(22):14803. https://doi.org/10.3390/ijerph192214803
Chicago/Turabian StyleTéllez-González, Mario Antonio, Juan Antonio Pineda-Juárez, Juan Antonio Suárez-Cuenca, Mónica Escamilla-Tilch, Daniel Santillán-Cortez, Silvia García, Sofía Lizeth Alcaraz-Estrada, Juan Carlos Pérez-Razo, Carlos Alberto Delgado-Quintana, Joel Vargas-Hernández, and et al. 2022. "Epidemiological Profile and Social Welfare Index as Factors Associated with COVID-19 Hospitalization and Severity in Mexico City: A Retrospective Analysis" International Journal of Environmental Research and Public Health 19, no. 22: 14803. https://doi.org/10.3390/ijerph192214803