
“Football- It’s in Your Blood”—Lived Experiences of Undertaking Recreational Football for Health in Older Adults


{kind=link}
Abstract
1. Introduction
- (1)
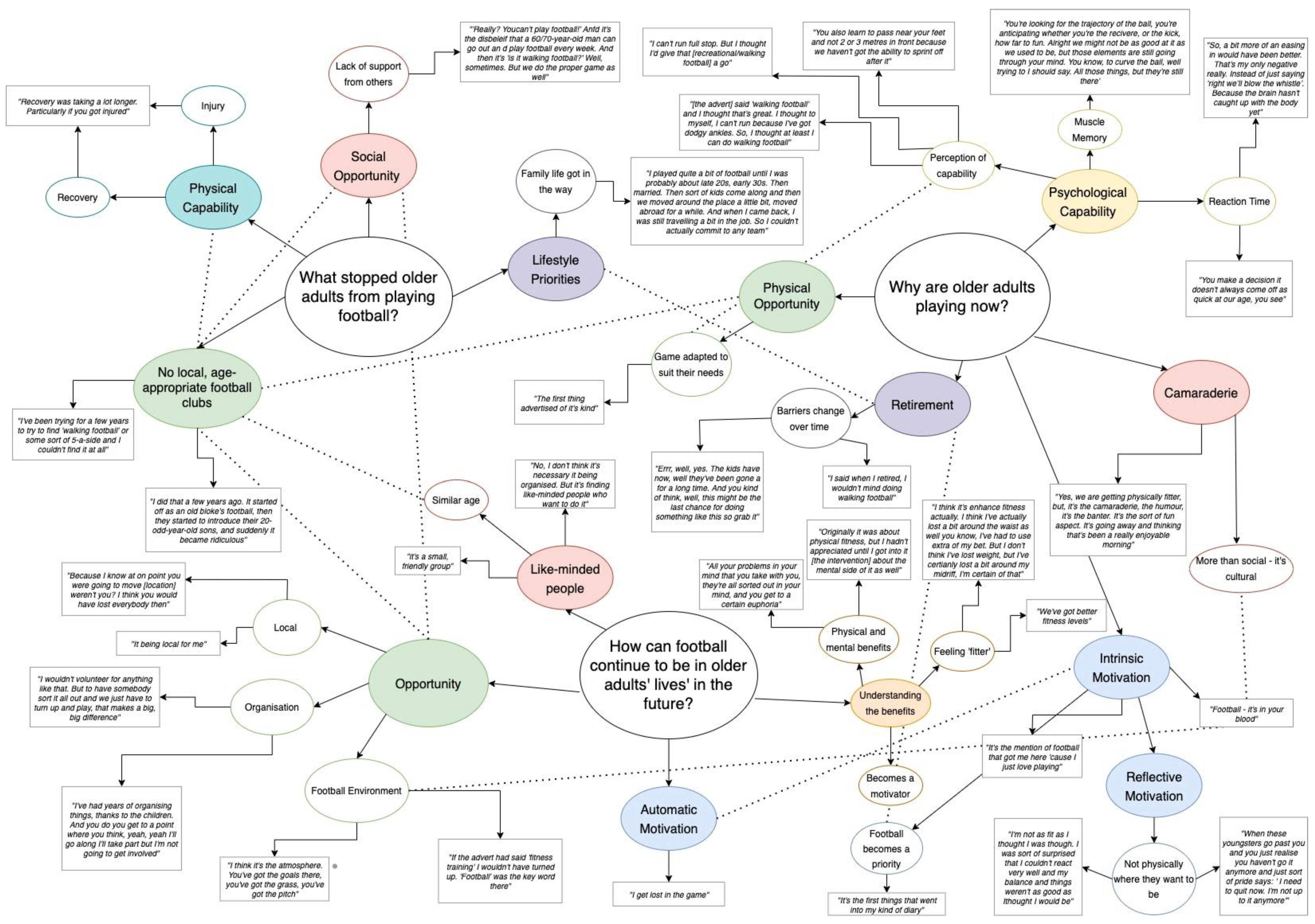
- What stopped older adults from playing football?
- (2)
- Why are older adults playing football now?
- (3)
- How can football continue to be in older adults’ lives in the future?
2. Materials and Methods
2.1. Participants
2.2. Procedure
- When it came to playing football regularly, what do you think it needed for you to take part in it?
- Why did you choose to take part in the project?
- How did you find the experience of this project?
- What has changed as a result of the intervention?
- If we were to offer this again for other people of your age, what changes do you think we need to make to the programme?
- When it comes to continuing to play football, what do you think it would take for you to continue to play?
2.3. Collection of Responses
2.4. Data Analysis
3. Results
3.1. What Stopped Older Adults from Playing Football?
‘Recovery was taking a lot longer. Particularly if you got injured.’(Participant 3)
“‘Really? You can’t play football!’ And it’s the disbelief that a 60/70-year-old man can go out and play football every week. And then it’s ‘Is it walking football?’ Well, sometimes. But we do the proper game as well.”(Participant 3)
‘I did that a few years ago. It started off as an old bloke’s football, then they started to introduce their 20-odd-year-old sons, and suddenly it became ridiculous.’(Participant 14)
“I’ve been trying for a few years to try to find ‘walking football’ or some sort of 5-a-side and I couldn’t find it at all.”(Participant 4)
‘I played quite a bit of football until I was probably late 20s, early 30s. Then married. Then sort of kids come along and then we moved around the place a little bit, moved abroad for a while. And then when I came back, I was still travelling a bit in the job. So I couldn’t actually commit to any team.’(Participant 4)
3.2. Why Are Older Adults Playing Now?
‘Errr, well, yes. The kids have now, well they’ve been gone for a long time. And you kind of think, well, this might be the last chance of doing something like this so grab it.’(Participant 3)
‘I said when I retired, I wouldn’t mind doing walking football or whatever. The trouble was trying to find it.’(Participant 9)
‘Yes, we are getting physically fitter, but, it’s the camaraderie, the humour, it’s the banter. It’s the sort of fun aspect. It’s going away and thinking that’s been a really enjoyable morning.’(Participant 19)
‘It’s become the highlight of my week.’(Participant 14)
‘It’s been very enjoyable, incredibly enjoyable.’(Participant 2)
‘Football—it’s in your blood.’(Participant 16)
‘It’s the mention of football that got me here ‘cause I just love playing.’(Participant 6)
“It’s the first thing that kind of went in my diary.”(Participant 11)
‘When these youngsters go past you and you just realise you haven’t got it anymore and just sort of pride says: “I need to quit now. I’m not up to it anymore.”’(Participant 19)
‘I’m not as fit as I thought I was though. I was sort of surprised that I couldn’t react very well and my balance and things weren’t as good as I thought I would be.’(Participant 10)
‘So, a bit more of an easing in would have been better. That’s my only negative really. Instead of just saying ‘right we’ll blow the whistle’. Because the brain hasn’t caught up with the body yet.’(Participant 19)
‘You make a decision it doesn’t always come off as quick at our age, you see.’(Participant 14)
‘You’re looking for the trajectory of the ball, you’re anticipating whether you’re the receiver, or the kick, how far to run. Alright we might not be as good at it as we used to be but those elements are still going through your mind. You know, to curve the ball, well trying to I should say. All those things, but they’re still there.’(Participant 14)
‘[the advert] said “walking football” and I thought that’s great. I thought to myself, I can’t run because I’ve got dodgy ankles. So, I thought at least I can do walking football.’(Participant 11)
‘But you also learn to pass near your feet and not 2 or 3 m in front because we haven’t got the ability to sprint off after it.’(Participant 19)
‘I can’t run full stop. But I thought I’d give that [recreational football] a go.’(Participant 11)
‘You also thought you could do more than you could do as well.’(Participant 9)
‘The first thing advertised of its kind.’(Participant 10)
3.3. How Can Football Continue to Be in Older Adults’ Lives in the Future?
‘No, I don’t think it’s necessary about it being organised. But it’s finding like-minded people who want to do it.’(Participant 9)
‘It is quite a small, friendly group, which helps.’(Participant 1)
‘Originally it was about physical fitness, but I hadn’t appreciated until I got into it [the intervention] about the mental side of it as well.’(Participant 19)
‘To me, exercise has always been a big escape valve.’(Participant 16)
‘We’ve got better fitness levels.’(Participant 9)
‘I think its enhanced fitness actually. I think I’ve actually lost a bit around the waist as well you know I’ve had to use extra of my belt. But I don’t think I’ve lost weight, but I’ve certainly lost a bit around my midriff, I’m certain of that.’(Participant 14)
‘I get lost in the game.’(Participant 19)
‘I’ve had years of organizing things, thanks to the children. And you do you get to a point where you think, yeah, yeah I’ll go along I’ll take part but I’m not going to get involved.’(Participant 1)
‘I wouldn’t volunteer for anything like that. But to have somebody sort it all out and we just have to turn up and play, that makes a big, big difference.’(Participant 16)
‘Because I know at one point you were going to move weren’t you? I think you would have lost everybody then.’(Participant 23)
‘It being local for me.’(Participant 14)
‘I think it’s the atmosphere. You’ve got the goals there, you’ve got the grass, you’ve got the pitch.’(Participant 10)
‘If it [the advert] has said “fitness training” I wouldn’t have turned up. “Football” was the keyword there.’(Participant 14)
4. Discussion
4.1. Barriers
4.2. Facilitators
4.3. Sustaining Behaviour Change through Recreational Football
4.4. Strengths and Limitations
5. Conclusions
6. Application
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation (WHO). NCDs Physical Inactivity: A Global Public Health Problem; WHO: Geneva, Switzerland, 2018; Available online: http://www.who.int/ncds/prevention/physical-activity/inactivity-global-health-problem/en/ (accessed on 30 October 2022).
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Lohne-Seiler, H.; Hansen, B.H.; Kolle, E.; Anderssen, S.A. Accelerometer-determined physical activity and self-reported health in a population of older adults (65–85 years): A cross-sectional study. BMC Public Health 2014, 14, 284. [Google Scholar] [CrossRef]
- Physical Activity Guidelines: UK Chief Medical Officers’ Report—GOV.UK. 2019. Available online: https://www.gov.uk/government/publications/physical-activity-guidelines-uk-chief-medical-officers-report (accessed on 30 October 2022).
- NHS England. NHS England Practical Guide to Healthy Ageing; Department for Health: London, UK, 2019. Available online: https://www.england.nhs.uk/publication/practical-guide-to-healthy-ageing/ (accessed on 30 October 2022).
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Geda, Y.E.; Roberts, R.O.; Knopman, D.S.; Christianson, T.J.; Pankratz, V.S.; Ivnik, R.J.; Boeve, B.F.; Tangalos, E.G.; Petersen, R.C.; Rocca, W.A. Physical exercise, aging, and mild cognitive impairment: A population-based study. Arch. Neurol. 2010, 67, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Ruuskanen, J.M.; Ruoppila, I. Physical Activity and Psychological Well-being among People Aged 65 to 84 Years. Age Ageing 1995, 24, 292–296. [Google Scholar] [CrossRef]
- Reddy, P.; Dias, I.; Holland, C.; Campbell, N.; Nagar, I.; Connolly, L.; Krustrup, P.; Hubball, H. Walking football as sustainable exercise for older adults—A pilot investigation. Eur. J. Sport Sci. 2017, 17, 638–645. [Google Scholar] [CrossRef]
- Sundstrup, E.; Jakobsen, M.D.; Andersen, L.L.; Andersen, T.R.; Randers, M.B.; Helge, J.W.; Suetta, C.; Schmidt, J.F.; Bangsbo, J.; Krustrup, P.; et al. Positive effects of 1-year football and strength training on mechanical muscle function and functional capacity in elderly men. Eur. J. Appl. Physiol. 2016, 116, 1127–1138. [Google Scholar] [CrossRef]
- Arnold, J.T.; Bruce-Low, S.; Sammut, L. The impact of 12 weeks walking football on health and fitness in males over 50 years of age. BMJ Open Sport Exerc. Med. 2015, 1. [Google Scholar] [CrossRef]
- Duncan, M.J.; Mowle, S.; Noon, M.; Eyre, E.; Clarke, N.D.; Hill, M.; Tallis, J.; Julin, M. The Effect of 12-Weeks Recreational Football (Soccer) for Health Intervention on Functional Movement in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 13625. [Google Scholar] [CrossRef]
- Bruun, D.M.; Bjerre, E.J.; Krustrup, P.; Brasso, K.; Johansen, C.; Rørth, M.; Midtgaard, J. Community-Based Recreational Football: A Novel Approach to Promote Physical Activity and Quality of Life in Prostate Cancer Survivors. Int. J. Environ. Res. Public Health 2014, 11, 5567–5585. [Google Scholar] [CrossRef] [PubMed]
- Helge, E.W.; Andersen, T.R.; Schmidt, J.F.; Jørgensen, N.R.; Hornstrup, T.; Krustrup, P.; Bangsbo, J. Recreational football improves bone mineral density and bone turnover marker profile in elderly men. Scand. J. Med. Sci. Sports 2014, 24, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Loadman, A. “He’s running, Ref!” An ethnogrpahic study of walking football. Soccer Soc. 2019, 4, 675–693. [Google Scholar] [CrossRef]
- French, D.P.; Olander, E.; Chisholm, A.; Mc Sharry, J. Which Behaviour Change Techniques Are Most Effective at Increasing Older Adults’ Self-Efficacy and Physical Activity Behaviour? A Systematic Review. Ann. Behav. Med. 2014, 48, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Hochbaun, G. Public Participaiton in Medical Screening Programs: A Socio-Psychological Study; US Department of Health: Washington, DC, USA, 1958.
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.; Norcorss, J. Systems of Psychotherapy: A Trasntheoretical Analysis; Cengage Learning: London, UK, 1990. [Google Scholar]
- Michie, S.; Wood, C.E.; Johnston, M.; Abraham, C.; Francis, J.J.; Hardeman, W. Behaviour change techniques: The development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol. Assess. 2015, 19, 1–188. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Andersen, T.R.; Schmidt, J.F.; Nielsen, J.J.; Randers, M.B.; Sundstrup, E.; Jakobsen, M.D.; Andersen, L.L.; Suetta, C.; Aagaard, P.; Bangsbo, J.; et al. Effect of football or strength training on functional ability and physical performance in untrained old men. Scand. J. Med. Sci. Sports 2014, 24, 76–85. [Google Scholar] [CrossRef]
- World Health Organization. Ageing. Available online: https://www.who.int/health-topics/ageing#tab=tab_1 (accessed on 30 October 2022).
- IPAQ. Guidelines for Data Processing Analysis of the International Physical Activity Questionnaire (IPAQ): Short and Long Forms. 2005. Available online: http://www.ipaq.ki.se/ (accessed on 30 October 2022).
- McIntosh, M.J.; Morse, J.M. Situating and Constructing Diversity in Semi-Structured Interviews. Glob. Qual. Nurs. Res. 2015, 2. [Google Scholar] [CrossRef]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of data collection in qualitative research: Interviews and focus groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research; Sage: London, UK, 2000. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Smith, B.; Sparkes, A.C. Narrative enquiry in psychology: Exploring the thensions within. Qual. Res. Psychol. 2006, 3, 169–192. [Google Scholar] [CrossRef]
- Smith, B.; McGannon, K.R. Developing rigour in qualitative research: Problems and opportunities within sport and exercise psychology. Int. Rev. Sport Exerc. Psychol. 2018, 11, 101–121. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Weate, P. Using thematic analysis in sport and exercise research. In Routledge Handbook of Qualitative Research in Sport and Exercise; Smith, B., Sparkes, A.C., Eds.; Routledge: London, UK, 2016; pp. 191–205. [Google Scholar]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Publications: Newbury Park, CA, USA, 1985. [Google Scholar]
- Graebner, M.; Martin, J.A.; Roundy, P. Qualitative data: Cooking without a recipe. Strat. Organ. 2012, 10, 276–284. [Google Scholar] [CrossRef]
- NICE. Behaviour Change: Individual Approaches Public Health Guideline [PH49]; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; Sage: London, UK, 2013. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- Bingham, A.J.; Witkowsky, P. Deductive and inductive approaches to qualitative data analysis. In Analyzing and Interpreting Qualitative Data: After the Interview; Vanover, C., Mihas, P., Saldaña, J., Eds.; Sage: London, UK, 2022; pp. 133–146. [Google Scholar]
- Lees, F.D.; Clark, P.G.; Nigg, C.R.; Newman, P. Barriers to Exercise Behavior among Older Adults: A Focus-Group Study. J. Aging Phys. Act. 2005, 13, 23–33. [Google Scholar] [CrossRef]
- Rasinaho, M.; Hirvensalo, M.; Leinonen, R.; Lintunen, T.; Rantanen, T. Motives for and Barriers to Physical Activity among Older Adults with Mobility Limitations. J. Aging Phys. Act. 2007, 15, 90–102. [Google Scholar] [CrossRef]
- Lamont, E.; Harris, J.; McDonald, G.; Kerin, T.; Dickens, G. Qualitative investigation of the role of collaborative football and walking football groups in mental health recovery. Ment. Health Phys. Act. 2017, 12, 116–123. [Google Scholar] [CrossRef]
- Battaglia, G.; Alesi, M.; Inguglia, M.; Roccella, M.; Caramazza, G.; Bellafiore, M.; Palma, A. Soccer practice as an add-on treatment in the management of individuals with a diagnosis of schizophrenia. Neuropsychiatr. Dis. Treat. 2013, 9, 595–603. [Google Scholar] [CrossRef]
- NICE. Depression in Adults: Recognition and Management Guidance; National Institute for Health and Care Excellence: London, UK, 2009. [Google Scholar]
- De Cates, A.; Stranges, S.; Blake, A.; Weich, S. Mental well-being: An important outcome for mental health services? Br. J. Psychiatry 2015, 207, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.B.; Richeson, N.E.; Croteau, K.A.; Farmer, B.C. Focus groups to explore the perceptions of older adults on a pedometer-based intervention. Res. Q. Exerc. Sport 2009, 80, 710–717. [Google Scholar] [CrossRef] [PubMed]
- McKeown, M.; Roy, A.; Spandler, H. ‘You’ll never walk alone’: Supportive social relations in a football and mental health project. Int. J. Ment. Health Nurs. 2015, 24, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Parnell, D.; Pringle, A.; McKenna, J.; Zwolinsky, S.; Rutherford, Z.; Hargreaves, J.; Trotter, L.; Rigby, M.; Richardson, D. Reaching older people with PA delivered in football clubs: The reach, adoption and implementation characteristics of the Extra Time Programme. BMC Public Health 2015, 15, 220. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mowle, S.; Eyre, E.; Noon, M.; Tallis, J.; Duncan, M.J. “Football- It’s in Your Blood”—Lived Experiences of Undertaking Recreational Football for Health in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 14816. https://doi.org/10.3390/ijerph192214816
Mowle S, Eyre E, Noon M, Tallis J, Duncan MJ. “Football- It’s in Your Blood”—Lived Experiences of Undertaking Recreational Football for Health in Older Adults. International Journal of Environmental Research and Public Health. 2022; 19(22):14816. https://doi.org/10.3390/ijerph192214816
Chicago/Turabian StyleMowle, Sophie, Emma Eyre, Mark Noon, Jason Tallis, and Michael J. Duncan. 2022. "“Football- It’s in Your Blood”—Lived Experiences of Undertaking Recreational Football for Health in Older Adults" International Journal of Environmental Research and Public Health 19, no. 22: 14816. https://doi.org/10.3390/ijerph192214816
APA StyleMowle, S., Eyre, E., Noon, M., Tallis, J., & Duncan, M. J. (2022). “Football- It’s in Your Blood”—Lived Experiences of Undertaking Recreational Football for Health in Older Adults. International Journal of Environmental Research and Public Health, 19(22), 14816. https://doi.org/10.3390/ijerph192214816