
How Does Environmental Information Disclosure Affect Public Health? Evidence from the New Ambient Air Quality Standards
Abstract
:1. Introduction
2. Policy Background and Research Hypothesis
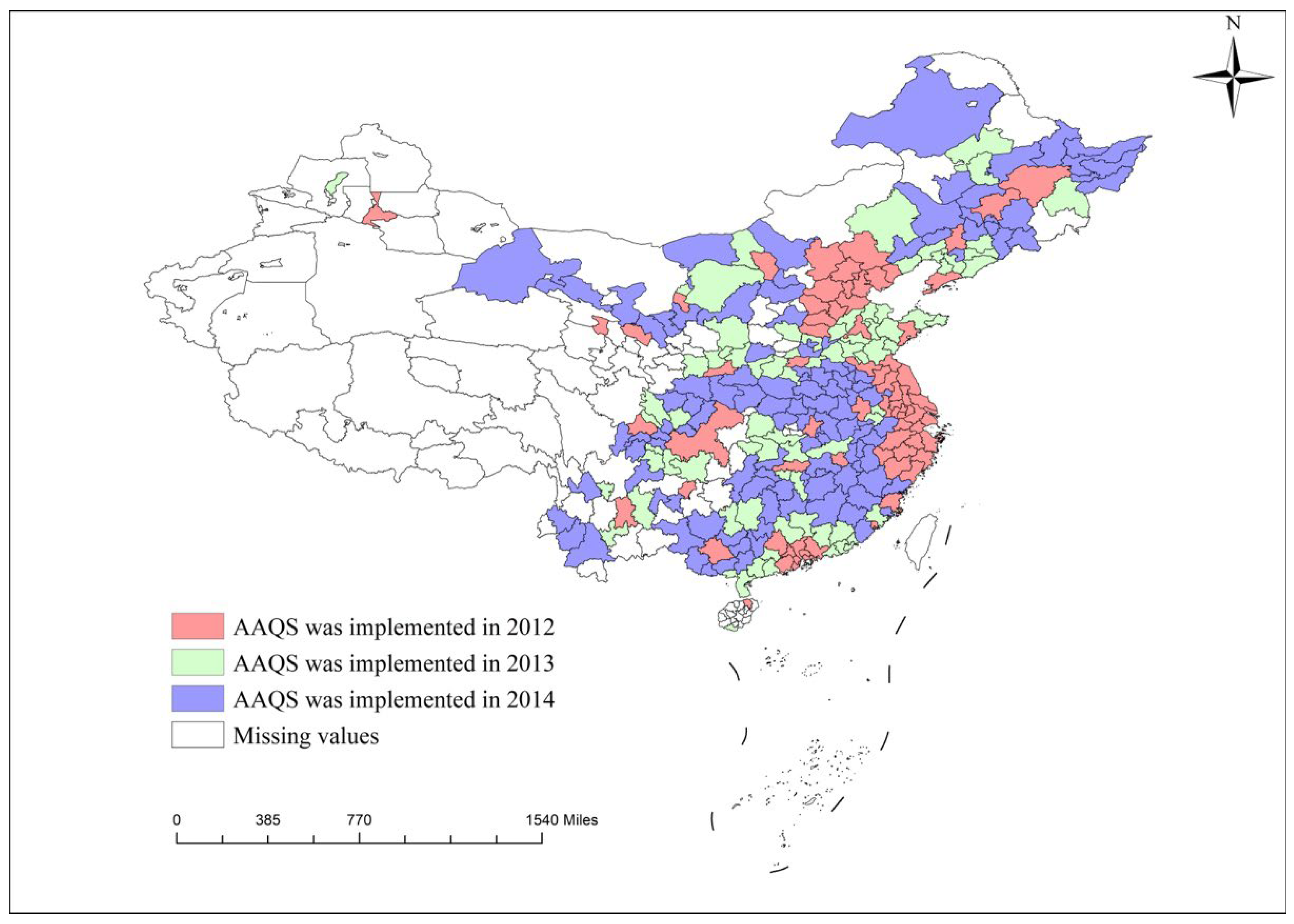
2.1. Policy Background
2.2. Research Hypothesis
3. Methods and Data
3.1. Data
3.2. Econometric Model
3.2.1. Baseline Model
3.2.2. Mediating Effect Model
3.2.3. Moderating Effect Model
3.3. Measurement of Variables
3.3.1. Public Health
3.3.2. Independent Variables
4. Empirical Results
4.1. Results of Baseline Regressions
4.2. Impact Mechanism between EID and Public Health
4.3. Heterogeneity Analysis
4.3.1. Individual Characteristics
4.3.2. Public Environmental Concerns
4.3.3. Group Analysis of Urban Administrative Rank and Economic Development Level
4.4. Robustness Tests
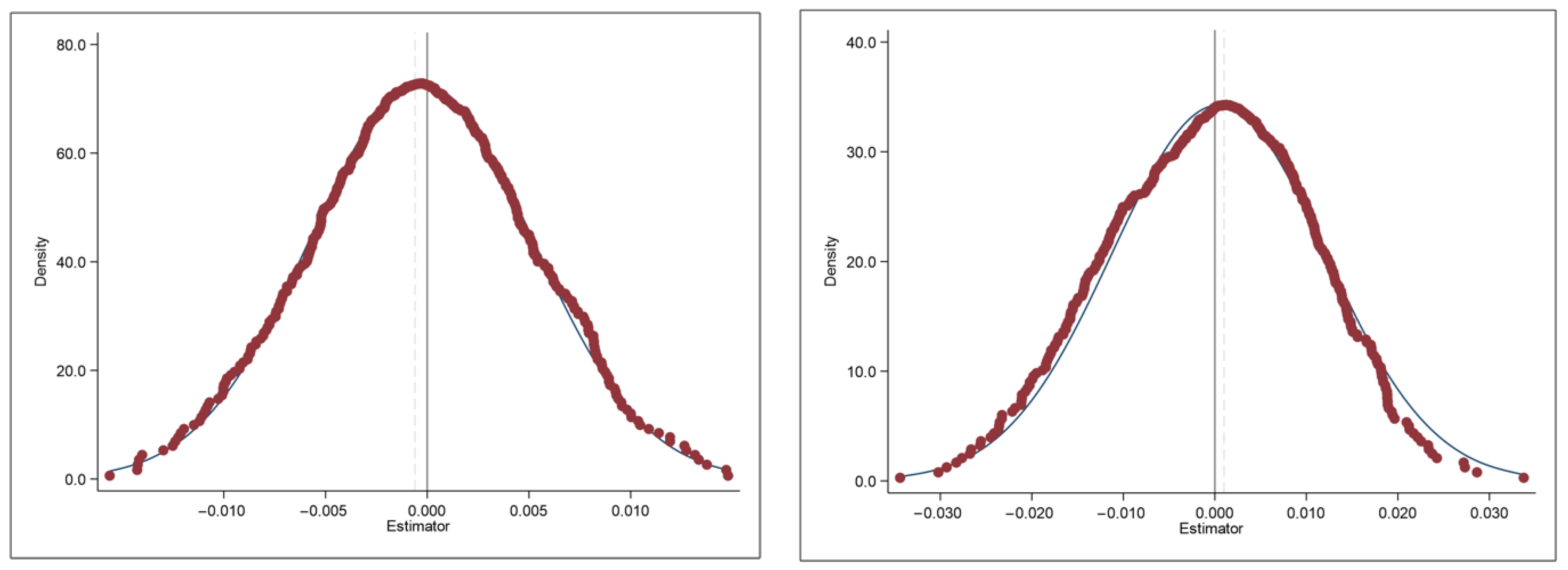
4.4.1. Placebo Test
4.4.2. Re-Estimation Based on PSM-DID
4.4.3. Re-Estimation Using Different Dependent Variable
4.4.4. Control of Family-Related Economic Variables
4.4.5. Control of Family Fixed Effect
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wang, Y. Environmental degradation and environmental threats in China. Environ. Monit. Assess. 2004, 90, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.T.; Klenow, P.J. Misallocation and manufacturing TFP in China and India. Q. J. Econ. 2007, 124, 1403–1448. [Google Scholar] [CrossRef] [Green Version]
- Sarwar, S.; Shahzad, U.; Chang, D.; Tang, B. Economic and non-economic sector reforms in carbon mitigation: Empirical evidence from Chinese provinces. Struct. Chang. Econ. Dyn. 2019, 49, 146–154. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, L. Price for clean air: Empirical evidence from Qingdao, China. J. World Econ. 2012, 4, 140–160. [Google Scholar]
- Amegah, A.K.; Agyei, M.S. Urban air pollution in sub-Saharan Africa: Time for action. Environ. Pollut. 2017, 220, 738–743. [Google Scholar] [CrossRef]
- Li, H.; Lu, J.; Li, B. Does pollution-intensive industrial agglomeration increase residents’ health expenditure? Sustain. Cities Soc. 2020, 56, 102092. [Google Scholar] [CrossRef]
- Chen, H.; Hao, Y.; Li, J.; Song, X. The impact of environmental regulation, shadow economy, and corruption on environmental quality: Theory and empirical evidence from China. J. Clean. Prod. 2018, 195, 200–214. [Google Scholar] [CrossRef]
- Chen, W.; Tang, H.; Zhao, H. Urban air quality evaluations under two versions of the national ambient air quality standards of China. Atmos. Pollut. Res. 2016, 7, 49–57. [Google Scholar] [CrossRef]
- Zhang, F.; Shi, Y.; Fang, D.; Ma, G.; Nie, C.; Krafft, T.; He, L.; Wang, Y. Monitoring history and change trends of ambient air quality in China during the past four decades. J. Environ. Manag. 2020, 260, 110031. [Google Scholar] [CrossRef]
- Bai, Y.; Ni, Y.; Zeng, Q. Impact of ambient air quality standards revision on the exposure-response of air pollution in Tianjin, China. Environ. Res. 2021, 198, 111269. [Google Scholar] [CrossRef]
- Wang, K.; Yin, H.; Chen, Y. The effect of environmental regulation on air quality: A study of new ambient air quality standards in China. J. Clean. Prod. 2019, 215, 268–279. [Google Scholar] [CrossRef]
- Yao, L.; Luo, Y.; Wang, Y.; Liu, H. Market response to the hierarchical water environment regulations on heavily polluting firm: Evidence from China. Water Resour. Econ. 2022, 39, 100201. [Google Scholar] [CrossRef]
- Gangwar, C.; Choudhari, R.; Chauhan, A.; Kumar, A.; Singh, A.; Tripathi, A. Assessment of air pollution caused by illegal e-waste burning to evaluate the human health risk. Environ. Int. 2019, 125, 191–199. [Google Scholar] [CrossRef]
- Li, H.; Lu, J. Can stable environmental protection officials’ tenure reduce illegal emissions? Socioecon. Plann. Sci. 2021, 78, 101055. [Google Scholar] [CrossRef]
- Tian, X.-L.; Guo, Q.-G.; Han, C.; Ahmad, N. Different extent of environmental information disclosure across Chinese cities: Contributing factors and correlation with local pollution. Glob. Environ. Chang. 2016, 39, 244–257. [Google Scholar] [CrossRef]
- Anenberg, S.C.; Horowitz, L.W.; Tong, D.Q. An Estimate of the Global Burden of Anthropogenic Ozone and Fine Particulate Matter on Premature Human Mortality Using Atmospheric Modeling. Environ. Health Perspect. 2010, 118, 1189–1195. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Sun, K.; Li, L.; Lei, Y.; Wu, S.; Jiang, Y.; Mi, Y.; Yang, J. The impacts of economic level and air pollution on public health at the micro and macro level. J. Clean. Prod. 2022, 366, 132932. [Google Scholar] [CrossRef]
- Liu, T.; Zhou, Y.; Wei, J. Association between short-term exposure to ambient air pollution and dementia mortality in Chinese adults. Sci. Total Environ. 2022, 849, 157860. [Google Scholar] [CrossRef]
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The mechanisms of air pollution and particulate matter in cardiovascular diseases. Heart Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef]
- Kim, K.H.; Jahan, S.A.; Kabir, E. A review on human health perspective of air pollution with respect to allergies and asthma. Environ. Int. 2013, 59, 41–52. [Google Scholar] [CrossRef]
- Wei, Y.; Zhang, J.J.; Li, Z.; Gow, A.; Chung, K.F.; Hu, M.; Tang, X. Chronic exposure to air pollution particles increases the risk of obesity and metabolic syndrome: Findings from a natural experiment in Beijing. FASEB J. 2016, 30, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Calderon-Garciduenas, L.; Calderon-Garciduenas, A.; Torres-Jardon, R.; Avila-Ramirez, J.; Kulesza, R.J.; Angiulli, A.D. Air pollution and your brain: What doyou need to know right now. Prim. Health Care Res. Dev. 2015, 16, 329–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Yang, B.; Liu, P.; Zhang, J.; Liu, Y.; Yao, Y.; Lu, Y. The longitudinal relationship between exposure to air pollution and depression in older adults. Int. J. Geriatr. Psychiatr. 2020, 35, 610–616. [Google Scholar] [CrossRef]
- Buoli, M.; Grassi, S.; Caldiroli, A.; Carnevali, G.S.; Mucci, F.; Iodice, S.; Bollati, V. Is there a link between air pollution and mental disorders? Environ. Int. 2018, 118, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, I.; Zhang, S.; Kirkbride, J.B.; Osborn, D.P.J.; Hayes, J.F. Air pollution (particulate matter) exposure and associations with depression, anxiety, bipolar, psychosis and suicide risk: A systematic review and meta-analysis. Environ. Health Perspect. 2019, 127, 126002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanner, J.; Pollack, A.Z.; Ranasinghe, S.; Stevens, D.R.; Mendola, P. Chronic exposure to air pollution and risk of mental health disorders complicating pregnancy. Environ. Res. 2021, 196, 110937. [Google Scholar] [CrossRef]
- Ao, C.-K.; Dong, Y.; Kuo, P.-F. Industrialization, indoor and ambient air quality, and elderly mental health. China Econ. Rev. 2021, 69, 101676. [Google Scholar] [CrossRef]
- Lu, B.; Yang, M.; Cumming, R.G.; Stanaway, F.F. Falls and impact on disability and healthy life expectancy in China: Evidence from the China health and retirement longitudinal survey (Charls). China Econ. Rev. 2020, 61, 101426. [Google Scholar] [CrossRef]
- Shen, W.-T.; Yu, X.; Zhong, S.-B.; Ge, H.-R. Population Health Effects of Air Pollution: Fresh Evidence From China Health and Retirement Longitudinal Survey. Front. Public Health 2021, 9, 779552. [Google Scholar] [CrossRef]
- Yu, C.; Long, H.; Zhang, X.; Tu, C.; Tan, Y.; Zhou, Y.; Zang, C. Regional integration and city-level energy efficiency: Evidence from China. Sustain. Cities Soc. 2022, 88, 104285. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Year | Name of Cities |
|---|---|
| 2012 | Beijing, Tianjin, Shijiazhuang, Tangshan, Qinhuangdao, Handan, Xingtai, Baoding, Zhangjiakou, Chengde, Cangzhou, Langfang, Hengshui, Taiyuan, Huhehaote, Shenyang, Dalian, Changchun, Harbin, Shanghai, Nanjing, Wuxi, Xuzhou, Changzhou, Suzhou, Nantong, Lianyungang, Huaian, Yancheng, Yangzhou, Zhenjiang, Taizhou, Suqian, Hangzhou, Ningbo, Wenzhou, Jiaxing, Huzhou, Shaoxing, Jinhua, Quzhou, Zhoushan, Taizhou, Lishui, Hefei, Fuzhou, Xiamen, Nanchang, Jinan, Qingdao, Zhengzhou, Wuhan, Changsha, Guangzhou, Shenzhen, Zhuhai, Foshan, Jiangmen, Zhaoqing, Huizhou, Dongguan, Zhongshan, Nanning, Haikou, Chongqing, Chengdu, Guiyang, Kunming, Lhasa, Xian, Lanzhou, Xining, Yinchuan, Urumqi |
| 2013 | Datong, Yangquan, Changzhi, Linfen, Baotou, Chifeng, Erdos, Anshan, Fushun, Benxi, Dandong, Jinzhou, Yingkou, Panjin, Huludao, Qiqihar, Daqing, Mudanjiang, Wuhu, Maanshan, Quanzhou, Jiujiang, Zibo, Zaozhuang, Dongying, Yantai, Weifang, Jining, Taian, Weihai, Rizhao, Linyi, Dezhou, Liaocheng, Binzhou, Heze, Kaifeng, Luoyang, Pingdingshan, Anyang, Jiaozuo, Sanmenxia, Yichang, Jingzhou, Zhuzhou, Xiangtan, Yueyang, Changde, Zhangjiajie, Shaoguan, Shantou, Zhanjiang, Maoming, Meizhou, Shanwei, Heyuan, Yangjiang, Qingyuan, Chaozhou, Jieyang, Yunfu, Liuzhou, Guilin, Beihai, Sanya, Zigong, Panzhihua, Luzhou, Deyang, Mianyang, Nanchong, Yibin, Zunyi, Qujing, Yuxi, Tongchuan, Baoji, Xianyang, Weinan, Yanan, Jiayuguan, Jinchang, Shizuishan, Karamay, Laiwu |
| 2014 | Jincheng, Shuozhou, Jinzhong, Yuncheng, Xinzhou, Lvliang, Wuhai, Tongliao, Hulunbeier, Bayan Nur, Ulaanchab, Fuxin, Liaoyang, Tieling, Chaoyang, Jilin, Siping, Liaoyuan, Tonghua, Baishan, Songyuan, Baicheng, Jixi, Hegang, Shuangyashan, Yichun, Jiamusi, Qitaihe, Hehe, Suihua, Bengbu, Huainan, Huabei, Tongling, Anqing, Huangshan, Chuzhou, Fuyang, SuZhou, Liuan, Bozhou, Chizhou, Xuancheng, Putian, Sanming, Zhangzhou, Nanping, Longyan, Ningde, Jingdezhen, Pingxiang, Xinyu, Yingtan, Ganzhou, jian, Yichun, Fuzhou, Shangrao, Hebi, xinxiang, Puyang, Xuchang, Luohe, Nanyang, Shangqiu, Xinyang, Zhoukou, Zhumadian, Huangshi, Shiyan, Xiangyang, Ezhou, Jingmen, Xiaogan, Huanggang, Xianning, Suizhou, Xiantao, Qianjiang, Tianmen, Shennongjia Forestry Area, Hengyang, Shaoyang, Yiyang, Chenzhou, Yongzhou, Huaihua, Loudi, Wuzhou, Fangchenggang, Qinzhou, Guigang, Yulin, Baise, Hezhou, Hechi, Laibin, Chongzuo, Sansha, Danzhou, Wuzhishan, Qionghai, Wenchang, Wanning, Dongfang, Guangyuan, Suining, Neijiang, Leshan, Meishan, Guangan, Dazhou, Yaan, Bazhong, Ziyang, Liupanshui, Anshun, Bijie, Tongren, Baoshan, Zhaotong, Lijiang, Puer, Lincang, Shigatse, Changdu, Linzhi, Shannan, Nagqu, Hanzhong, Yulin, Ankang, Shangluo, Baiyin, Tianshui, Wuwei, Zhangye, Pingliang, Jiuquan, Qingyang, Dingxi, Longnan, Haidong, Wuzhong, Guyuan, Zhongwei, Turpan, Hami, Shihezi, Aral, Tumushuk, Wujiaqu, Beitun, Tiemenguan, Shuanghe, Kekodara, Kunyu, Huyang River, Chaohu |
| Public Health | Indicators | Range of Values | Properties |
|---|---|---|---|
| Physical health | Acute shock | [0,3] | Negative |
| Chronic shock | [0,9] | Negative | |
| Mental health | Situational memory | [0,20] | Positive |
| Mental cognition | [0,12] | Positive | |
| Depression self-assessment | [10,40] | Negative |
| Variables | Variable Description | N | Mean | Min | Max | Std | |
|---|---|---|---|---|---|---|---|
| Dependent variable | Physical health | Physical health level | 69,758 | 0.970 | 0.222 | 1 | 0.073 |
| Mental health | Mental health level | 69,758 | 0.471 | 0.059 | 1 | 0.149 | |
| Independent variable | EID | Implementation of EID | 69,758 | 0.612 | 0 | 1 | 0.487 |
| PM2.5 | Logarithmic value of PM2.5 concentration | 69,758 | 0.471 | 0.059 | 1 | 0.149 | |
| PEC | Logarithmic values of the Baidu index | 69,758 | 3.749 | 1.692 | 4.641 | 0.424 | |
| Control variable | lnage | Logarithmic value of age | 69,758 | 4.092 | 3.807 | 4.771 | 0.162 |
| gender | Male = 1, female = 0 | 69,758 | 0.516 | 0 | 1 | 0.500 | |
| marital | Married = 1, otherwise = 0 | 69,758 | 0.863 | 0 | 1 | 0.344 | |
| residence | Rural = 1, urban = 0 | 69,758 | 0.126 | 0 | 1 | 0.332 | |
| lncost | Logarithmic value of hospitalization Costs | 69,758 | 1.045 | 0 | 14.152 | 2.811 | |
| toilet | No toilet = 0, otherwise = 1 | 69,758 | 0.778 | 0 | 1 | 0.416 | |
| water | No running water = 0, otherwise = 1 | 69,758 | 0.731 | 0 | 1 | 0.444 | |
| Variables | Physical Health | Mental Health | ||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| EID | 0.039 *** | 0.041 *** | 0.015 *** | 0.009 *** |
| (0.001) | (0.001) | (0.001) | (0.001) | |
| lnage | −0.023 *** | 0.195 *** | ||
| (0.002) | (0.004) | |||
| gender | −0.003 *** | 0.053 *** | ||
| (0.001) | (0.001) | |||
| marital | −0.001 | −0.036 *** | ||
| (0.001) | (0.002) | |||
| residence | −0.018 *** | −0.036 *** | ||
| (0.001) | (0.002) | |||
| lncost | −0.002 *** | 0.002 *** | ||
| (0.000) | (0.000) | |||
| toilet | 0.001 | 0.016 *** | ||
| (0.001) | (0.001) | |||
| water | 0.003 *** | 0.020 *** | ||
| (0.001) | (0.001) | |||
| C | 0.946 *** | 1.046 *** | 0.462 *** | −0.407 *** |
| (0.001) | (0.008) | (0.001) | (0.018) | |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Observation | 69,758 | 69,758 | 69,758 | 69,758 |
| F | 3858.434 | 563.852 | 177.037 | 820.614 |
| R2 | 0.081 | 0.096 | 0.069 | 0.173 |
| Variables | Acute Shock | Chronic Shock | Situational Memory | Mental Cognition | Depression Self-Assessment |
|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | |
| EID | −0.050 *** | −0.597 *** | 0.145 *** | 0.151 | −0.253 *** |
| (0.002) | (0.007) | (0.031) | (0.132) | (0.041) | |
| C | −0.168 *** | 1.360 *** | 24.682 *** | 14.485 *** | 23.791 *** |
| (0.025) | (0.076) | (0.422) | (0.759) | (0.541) | |
| Control | Y | Y | Y | Y | Y |
| City FE | Y | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y | Y |
| Observation | 75,816 | 75,816 | 75,816 | 75,816 | 75,816 |
| F | 131.068 | 982.150 | 632.131 | 52.093 | 205.546 |
| R2 | 0.036 | 0.129 | 0.129 | 0.672 | 0.064 |
| Variables | PM2.5 | Physical Health | Mental Health |
|---|---|---|---|
| (1) | (2) | (3) | |
| EID | −0.201 *** | 0.006 *** | 0.004 *** |
| (0.013) | (0.000) | (0.001) | |
| PM2.5 | −0.045 *** | −0.080 *** | |
| (0.002) | (0.005) | ||
| C | 3.872 *** | 1.747 *** | −0.765 *** |
| (0.008) | (0.040) | (0.124) | |
| Control | Y | Y | Y |
| City FE | Y | Y | Y |
| Year FE | Y | Y | Y |
| Sobel Z-score | −10.88 | 22.89 | |
| Observation | 69,758 | 69,758 | 69,758 |
| F | 254.016 | 275.123 | 449.077 |
| R2 | 0.907 | 0.456 | 0.752 |
| Variables | Physical Health | Mental Health | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| (1) | (2) | (3) | (4) | |
| EID | 0.044 *** | 0.038 *** | 0.013 *** | 0.004 *** |
| (0.001) | (0.001) | (0.001) | (0.001) | |
| C | 1.039 *** | 1.041 *** | −0.512 *** | −0.145 *** |
| (0.011) | (0.010) | (0.025) | (0.025) | |
| SUR test | 23.24 *** | 8.42 *** | ||
| Control | Y | Y | Y | Y |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Observation | 35,976 | 33,782 | 35,976 | 33,782 |
| F | 350.34 | 296.09 | 542.54 | 188.53 |
| R2 | 0.103 | 0.092 | 0.214 | 0.095 |
| Variables | Physical Health | Mental Health | ||
|---|---|---|---|---|
| Rural | Urban | Rural | Urban | |
| (1) | (2) | (3) | (4) | |
| EID | 0.079 *** | 0.038 *** | 0.006 | 0.009 *** |
| (0.003) | (0.001) | (0.004) | (0.001) | |
| C | 1.047 *** | 1.044 *** | −0.187 *** | −0.448 *** |
| (0.025) | (0.008) | (0.047) | (0.019) | |
| SUR test | 203.99 *** | 6.57 ** | ||
| Control | Y | Y | Y | Y |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Observation | 8,782 | 60,976 | 8,782 | 60,976 |
| F | 114.70 | 533.54 | 59.47 | 924.37 |
| R2 | 0.173 | 0.087 | 0.119 | 0.177 |
| Variables | Physical Health | Mental Health | ||
|---|---|---|---|---|
| 45–60 | Above 60 | 45–60 | Above 60 | |
| (1) | (2) | (3) | (4) | |
| EID | 0.037 *** | 0.047 *** | 0.006 *** | 0.015 *** |
| (0.001) | (0.001) | (0.001) | (0.002) | |
| C | 0.953 *** | 0.945 *** | 0.402 *** | 0.405 *** |
| (0.002) | (0.002) | (0.005) | (0.004) | |
| SUR test | 60.95 *** | 10.48 ** | ||
| Control | Y | Y | Y | Y |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Observation | 36,838 | 32,920 | 36,838 | 32,920 |
| F | 350.91 | 299.68 | 130.56 | 405.65 |
| R2 | 0.097 | 0.098 | 0.094 | 0.176 |
| Variables | Physical Health | Mental Health | ||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| PEC | 0.047 *** | −0.021 *** | 0.046 *** | 0.036 *** |
| (0.008) | (0.002) | (0.009) | (0.004) | |
| EID | 0.060 *** | 0.030 | ||
| (0.008) | (0.022) | |||
| EID×PEC | 0.007 *** | 0.009 *** | ||
| (0.001) | (0.002) | |||
| C | 0.538 *** | 2.111 *** | 0.039 | −2.071 *** |
| (0.074) | (0.037) | (0.079) | (0.088) | |
| Control | Y | Y | Y | Y |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Observation | 69,758 | 69,758 | 69,758 | 69,758 |
| F | 33.659 | 223.202 | 29.715 | 325.673 |
| R2 | 0.031 | 0.451 | 0.063 | 0.750 |
| Variables | Physical Health | Mental Health | ||
|---|---|---|---|---|
| Non-Ordinary Prefecture-Level Cities | Ordinary Prefecture-Level Cities | Non-Ordinary Prefecture-Level Cities | Ordinary Prefecture-Level Cities | |
| (1) | (2) | (4) | (5) | |
| EID | 0.075 *** | 0.037 *** | 0.018 *** | 0.011 *** |
| (0.002) | (0.001) | (0.003) | (0.001) | |
| C | 0.951 *** | 0.967 *** | −0.074 *** | −0.170 *** |
| (0.011) | (0.013) | (0.024) | (0.026) | |
| Control | Y | Y | Y | Y |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Observation | 11,448 | 58,310 | 11,448 | 58,310 |
| F | 173.638 | 413.536 | 84.425 | 768.846 |
| R2 | 0.214 | 0.081 | 0.119 | 0.183 |
| Variables | Physical Health | Mental Health | ||||
|---|---|---|---|---|---|---|
| Eastern | Central | Western | Eastern | Central | Western | |
| (1) | (2) | (3) | (4) | (5) | (6) | |
| EID | 0.047 *** | 0.039 *** | 0.039 *** | 0.003 *** | 0.008 *** | 0.015 *** |
| (0.001) | (0.001) | (0.001) | (0.000) | (0.002) | (0.002) | |
| C | 1.068 *** | 1.052 *** | 1.017 *** | −0.424 *** | −0.454 *** | −0.348 *** |
| (0.012) | (0.014) | (0.014) | (0.030) | (0.031) | (0.031) | |
| Control | Y | Y | Y | Y | Y | Y |
| City FE | Y | Y | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y | Y | Y |
| Observation | 24,020 | 22,953 | 22,785 | 24,020 | 22,953 | 22,785 |
| F | 219.190 | 168.099 | 187.401 | 263.913 | 282.139 | 283.258 |
| R2 | 0.122 | 0.079 | 0.093 | 0.143 | 0.160 | 0.191 |
| Variables | Physical Health | Mental Health |
|---|---|---|
| (1) | (2) | |
| EID | 0.057 *** | 0.009 *** |
| (0.003) | (0.003) | |
| lnage | −0.014 *** | 0.205 *** |
| (0.002) | (0.005) | |
| gender | −0.000 | 0.054 *** |
| (0.001) | (0.002) | |
| marital | −0.000 | −0.036 *** |
| (0.001) | (0.002) | |
| residence | −0.012 *** | −0.037 *** |
| (0.001) | (0.002) | |
| lncost | −0.002 *** | 0.002 *** |
| (0.000) | (0.000) | |
| toilet | 0.000 | 0.014 *** |
| (0.001) | (0.002) | |
| water | −0.002 *** | 0.025 *** |
| (0.001) | (0.002) | |
| C | 0.992 *** | −0.453 *** |
| (0.008) | (0.022) | |
| City FE | Y | Y |
| Year FE | Y | Y |
| Observation | 44,929 | 44,929 |
| F | 129.765 | 585.025 |
| R2 | 0.083 | 0.189 |
| Variables | Health | Health |
|---|---|---|
| (1) | (2) | |
| EID | 0.464 *** | 0.448 *** |
| (0.009) | (0.009) | |
| lnage | −0.313 *** | |
| (0.035) | ||
| gender | −0.173 *** | |
| (0.010) | ||
| marital | −0.056 *** | |
| (0.017) | ||
| residence | 0.265 *** | |
| (0.016) | ||
| lncost | −0.053 *** | |
| (0.002) | ||
| toilet | 0.059 *** | |
| (0.012) | ||
| water | 0.107 *** | |
| (0.012) | ||
| C | 1.512 *** | 3.011 *** |
| (0.006) | (0.152) | |
| City FE | Y | Y |
| Year FE | Y | Y |
| Observation | 69,758 | 69,758 |
| F | 2676.329 | 595.881 |
| R2 | 0.066 | 0.094 |
| Physical_Health | Physical_Health | Mental_Health | Mental_Health | |
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| EID | 0.039 *** | 0.024 *** | 0.015 *** | 0.014 *** |
| (0.001) | (0.001) | (0.001) | (0.001) | |
| lnage | −0.024 *** | 0.194 *** | ||
| (0.002) | (0.004) | |||
| gender | −0.003 *** | 0.053 *** | ||
| (0.001) | (0.001) | |||
| marital | −0.001 | −0.036 *** | ||
| (0.001) | (0.002) | |||
| residence | −0.016 *** | −0.038 *** | ||
| (0.001) | (0.002) | |||
| lncost | −0.002 *** | 0.002 *** | ||
| (0.000) | (0.000) | |||
| toilet | −0.000 | 0.016 *** | ||
| (0.001) | (0.001) | |||
| water | 0.003 *** | 0.020 *** | ||
| (0.001) | (0.001) | |||
| income | −0.036 *** | 0.050 *** | ||
| (0.002) | (0.003) | |||
| consumption | 0.117 *** | −0.075 *** | ||
| (0.003) | (0.004) | |||
| C | 0.946 *** | 0.256 *** | 0.462 *** | −0.133 *** |
| (0.001) | (0.026) | (0.001) | (0.045) | |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Observation | 69,758 | 69,758 | 69,758 | 69,758 |
| F | 3858.434 | 616.222 | 177.037 | 715.535 |
| R2 | 0.081 | 0.125 | 0.069 | 0.177 |
| Lnpm25 | Physical_Health | Mental_Health | |
|---|---|---|---|
| (1) | (2) | (3) | |
| EID | −0.201 *** | 0.001 * | 0.006 *** |
| (0.013) | (0.001) | (0.002) | |
| PM2.5 | −0.040 *** | −0.075 *** | |
| (0.002) | (0.005) | ||
| lnage | −0.133*** | 0.325 *** | |
| (0.010) | (0.027) | ||
| gender | −0.002 | 0.028 ** | |
| (0.003) | (0.014) | ||
| marital | 0.007 *** | −0.027 *** | |
| (0.002) | (0.004) | ||
| residence | −0.001 | −0.008 *** | |
| (0.001) | (0.002) | ||
| lncost | −0.001 *** | 0.001 *** | |
| (0.000) | (0.000) | ||
| toilet | 0.000 | 0.027 *** | |
| (0.001) | (0.002) | ||
| water | −0.002 ** | 0.038 *** | |
| (0.001) | (0.002) | ||
| income | −0.017 *** | 0.023 *** | |
| (0.002) | (0.004) | ||
| consumption | 0.019 *** | −0.049 *** | |
| (0.003) | (0.005) | ||
| C | 3.872 *** | 1.601 *** | −0.379 *** |
| (0.008) | (0.045) | (0.132) | |
| City FE | Y | Y | Y |
| Year FE | Y | Y | Y |
| Sobel Z-score | −12.58 | 24.96 | |
| Observation | 68,719 | 48,359 | 48,359 |
| F | 254.016 | 228.666 | 379.502 |
| R2 | 0.907 | 0.458 | 0.752 |
| F | 254.016 | 228.666 | 379.502 |
| Physical_Health | Physical_Health | Mental_Health | Mental_Health | |
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| EID | 0.016 *** | 0.005 *** | 0.041 *** | 0.019 *** |
| (0.000) | (0.001) | (0.001) | (0.002) | |
| lnage | −0.104 *** | 0.238 *** | ||
| (0.006) | (0.015) | |||
| gender | −0.006 *** | 0.055 *** | ||
| (0.000) | (0.001) | |||
| marital | 0.008 *** | −0.014 *** | ||
| (0.002) | (0.004) | |||
| residence | −0.003 *** | −0.002 | ||
| (0.001) | (0.002) | |||
| lncost | −0.002 *** | 0.002 *** | ||
| (0.000) | (0.000) | |||
| toilet | 0.001 | 0.027 *** | ||
| (0.001) | (0.002) | |||
| water | −0.003 *** | 0.041 *** | ||
| (0.001) | (0.002) | |||
| income | −0.041 *** | 0.068 *** | ||
| (0.002) | (0.004) | |||
| consumption | 0.023 *** | −0.057 *** | ||
| (0.003) | (0.006) | |||
| C | 0.968 *** | 1.549 *** | 0.442 *** | −0.704 *** |
| (0.000) | (0.036) | (0.001) | (0.080) | |
| City FE | Y | Y | Y | Y |
| Year FE | Y | Y | Y | Y |
| Family FE | Y | Y | Y | Y |
| Observation | 69,758 | 69,758 | 69,758 | 69,758 |
| F | 1107.604 | 183.818 | 798.714 | 443.252 |
| R2 | 0.404 | 0.427 | 0.355 | 0.409 |
| lnpm25 | Physical_Health | Mental_Health | |
|---|---|---|---|
| (1) | (2) | (3) | |
| EID | −0.201 *** | 0.001 * | 0.010 *** |
| (0.013) | (0.000) | (0.002) | |
| PM2.5 | −0.050 *** | −0.100 *** | |
| (0.002) | (0.005) | ||
| lnage | −0.054 *** | 0.136 *** | |
| (0.006) | (0.015) | ||
| gender | −0.004 *** | 0.051 *** | |
| (0.000) | (0.001) | ||
| marital | 0.005 ** | −0.008 * | |
| (0.002) | (0.004) | ||
| residence | −0.002 | −0.005 ** | |
| (0.001) | (0.002) | ||
| lncost | −0.002 *** | 0.002 *** | |
| (0.000) | (0.000) | ||
| toilet | 0.001 | 0.026 *** | |
| (0.001) | (0.002) | ||
| water | −0.002 ** | 0.038 *** | |
| (0.001) | (0.002) | ||
| income | −0.021 *** | 0.030 *** | |
| (0.002) | (0.004) | ||
| consumption | 0.020 *** | −0.052 *** | |
| (0.003) | (0.006) | ||
| C | 3.872 *** | 1.314 *** | 0.398 *** |
| (0.008) | (0.037) | (0.098) | |
| City FE | Y | Y | Y |
| Year FE | Y | Y | Y |
| Family FE | Y | Y | Y |
| Sobel Z-score | -15.23 | 20.38 | |
| Observation | 68,719 | 48,359 | 48,359 |
| F | 254.016 | 228.666 | 379.502 |
| R2 | 0.907 | 0.434 | 0.413 |
| F | 254.016 | 181.359 | 434.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Wang, Y.; Zhang, Z.; Long, H. How Does Environmental Information Disclosure Affect Public Health? Evidence from the New Ambient Air Quality Standards. Int. J. Environ. Res. Public Health 2022, 19, 15141. https://doi.org/10.3390/ijerph192215141
Zhang X, Wang Y, Zhang Z, Long H. How Does Environmental Information Disclosure Affect Public Health? Evidence from the New Ambient Air Quality Standards. International Journal of Environmental Research and Public Health. 2022; 19(22):15141. https://doi.org/10.3390/ijerph192215141
Chicago/Turabian StyleZhang, Xiang, Yanan Wang, Zongyi Zhang, and Hongyu Long. 2022. "How Does Environmental Information Disclosure Affect Public Health? Evidence from the New Ambient Air Quality Standards" International Journal of Environmental Research and Public Health 19, no. 22: 15141. https://doi.org/10.3390/ijerph192215141