
The Medication Experience of TB/HIV Coinfected Patients: Qualitative Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Characterization of the Study Participants
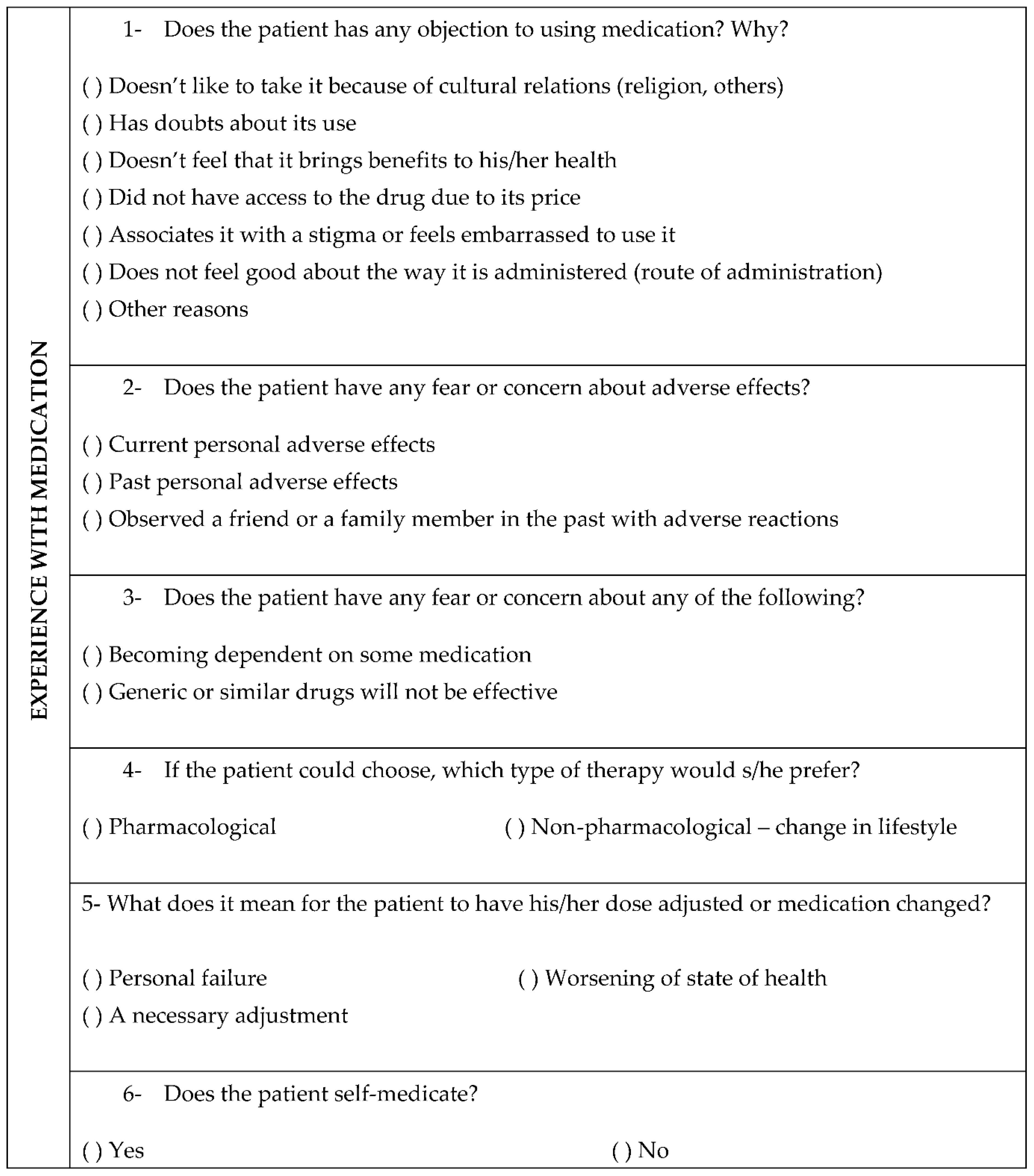
3.2. Medication Experience
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rossetto, M.; Maffacciolli, R.; Rocha, C.M.F.; Oliveira, D.L.L.C.; Serrant, L. Tuberculosis/HIV/AIDS coinfection in Porto Alegre, RS/Brazil-invisibility and silencing of the most affected groups. Rev. Gauch. Enferm. 2019, 40, e20180033. [Google Scholar] [CrossRef] [PubMed]
- Picelli, I.; Díaz-Bermúdez, X.P. Will these drugs be worthwhile? An anthropological study of adherence to antiretroviral therapies among support groups for people living with HIV and AIDS. Saúde Soc. 2014, 23, 496–509. [Google Scholar]
- Rodrigues, I.L.; Monteiro, L.L.; Pacheco, R.H.; da Silva, S.E. Abandonment of tuberculosis treatment among patients co-infected with TB/HIV. Rev. Esc. Enferm. USP 2010, 44, 383–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, L.M.; Harter, J.; Tomberg, J.O.; Vieira, D.A.; Antunes, M.L.; Cardozo-Gonzales, R.I. Monitoring and assessment of outcome in cases of tuberculosis in a municipality of Southern Brazil. Rev. Gauch. Enferm. 2016, 37, e51467. [Google Scholar]
- Cipolle, R.J.; Strand, L.M.; Morley, P.C. Pharmaceutical Care Practice: The Patient Centered to Medication Management, 3rd ed.; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Shoemaker, S.J.; Ramalho de Oliveira, D. Understanding the meaning of medications for patients: The medication experience. Pharm. World Sci. 2008, 30, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, Y.A.; Silva, L.D.; Ramalho-de-Oliveira, D. Experiences with the daily use of medications among chronic hepatitis C patients. Res. Soc. Adm. Pharm. 2020, 16, 33–40. [Google Scholar] [CrossRef]
- Hillman, L.A.; Peden-McAlpine, C.; Ramalho-de-Oliveira, D.; Schommer, J.C. The Medication Experience: A Concept Analysis. Pharmacy 2020, 9, 7. [Google Scholar] [CrossRef]
- Freire, P. Educação e Mudança, 48th ed.; Paz & Terra: São Paulo, Brazil, 2020. [Google Scholar]
- Shoemaker, S.J.; Ramalho de Oliveira, D.; Alves, M.; Ekstrand, M. The medication experience: Preliminary evidence of its value for patient education and counseling on chronic medications. Patient Educ. Couns. 2011, 83, 443–450. [Google Scholar] [CrossRef]
- Mohammed, M.A.; Moles, R.J.; Chen, T.F. Medication-related burden and patients’ lived experience with medicine: A systematic review and metasynthesis of qualitative studies. BMJ Open 2016, 6, e010035. [Google Scholar] [CrossRef] [Green Version]
- Silva, J.B.; Cardoso, G.C.P.; Netto, A.R.; Kritski, A.L. The meanings of comorbidity for patients living with TB / HIV: Implications in the treatment. Physis 2015, 25, 209–229. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. Sep. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Resende, N.H.; Miranda, S.S.; Ceccato, M.G.B.; Haddad, J.P.A.; Reis, A.M.M.; Silva, D.I.; Carvalho, W.S. Drug therapy problems for patients with tuberculosis and HIV/AIDS at a reference hospital. Einstein 2019, 17, eAO4696. [Google Scholar] [CrossRef] [PubMed]
- Resende, N.H.; Souza, J.A.; Martins, U.C.; Reis, A.M.; Miranda, S.S.; Carvalho, W.S. Medication therapy management in patients with tuberculosis and HIV/AIDS: Case series. Rev. Bras. Farm. Hosp. Serv. Saude 2021, 12, 0681. [Google Scholar] [CrossRef]
- Minayo, M.C.S. O Desafio do conhecimento. In Pesquisa Qualitativa em Saúde, 14th ed.; Rucitec: São Paulo, Brazil, 2014. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psych. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Minayo, M.C.S. Qualitative analysis: Theory, steps and reliability. Cienc. Saude Coletiva 2012, 17, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, Y.A.; Ramalho-de-Oliveira, D. The Subjective Experience of Using Medications: What We Know and the Paths Forward. Pharmacy 2021, 9, 50. [Google Scholar] [CrossRef]
- Nascimento, Y.A.; Filard, A.F.R.; Abath, A.J.; Silva, L.D.; Ramalho-de-Oliveira, D. The phenomenology of Merleau-Ponty in investigations about medication use: Constructing a methodological cascade. Rev. Esc. Enferm. USP 2017, 51, e03296. [Google Scholar] [CrossRef]
- Brasil. Manual de Recomendações para o Controle da Tuberculose No Brasil, 2nd ed.; Ministério da Saúde: Térreo, Brazil, 2019.
- Brasil. Agenda Estratégica para Ampliação do Acesso e Cuidado Integral das Populações-Chave em HIV. In Hepatites Virais e outras Infecções Sexualmente Transmissíveis; Ministério da Saúde: Térreo, Brazil, 2018. [Google Scholar]
- Shah, G.H.; Ewetola, R.; Etheredge, R.; Maluantesa, L.; Waterfield, K.; Engetele, E.; Kilundu, A. Risk factors for TB/HIV coinfection and consequences for patients outcomes: Evidence from 241 clinics in the Democratic Republic of Congo. Int. J. Environ. Res. Public Health 2021, 18, 5165. [Google Scholar] [CrossRef]
- Ewetola, R.; Shah, G.H.; Maluantesa, L.; Etheredge, G.; Waterfield, K.; Mulenga, A.; Kilundu, A. Disparities in HIV Clinical Stage progression of patients at outpatients clinics in Democratic Republic of Congo. Int. J. Environ. Res. Public Health 2021, 18, 5341. [Google Scholar] [CrossRef]
- Brasil. Panorama Epidemiológico da Coinfecção TB-HIV No Brasil 2020; Ministério da Saúde: Térreo, Brazil, 2021.
- Fleury-Teixeira, P.; Vaz, F.A.C.; Campos, F.C.C.; Álvares, J.; Aguiar, R.A.T.; Oliveira, V.A. Autonomy as a central criterion in the concept of health promotion. Ciência Saúde Coletiva 2008, 3, 2115–2122. [Google Scholar] [CrossRef]
- Soares, J.C.R.S.; Camargo Junior, K.R. Patient autonomy in the therapeutic process as a value for health. Interface 2007, 11, 1165–1178. [Google Scholar]
- Conrad, P. The meaning of medications. Another look at compliance. Soc. Sci. Med. 1985, 20, 29–37. [Google Scholar]
- Figueiras, M.J.; Marcelino, D.; Cortes, M.A.; Horne, R.; Weinman, J. Crenças do Senso Comum sobre medicamento genérico vs. medicamentos de marca: Um estudo piloto sobre diferenças de género. Análise Psicológica 2007, 25, 427–437. [Google Scholar] [CrossRef] [Green Version]
- Fauk, N.K.; Hawke, K.; Mwanri, L.; Ward, P.R. Stigma and discrimination towards people livingwith HIV in the context of families, communities, and healthcare settings: A qualitative study in Indonesia. Int. J. Environ. Public Health 2021, 18, 5424. [Google Scholar] [CrossRef] [PubMed]
- Pinho, C.M.; Dâmaso, B.F.R.; Gomes, E.T.; Trajano, M.F.C.; Andrade, M.S.; Valença, M.P. Religious and spiritual coping in people living with HIV/Aids. Rev. Bras. Enferm. 2017, 70, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Guimarães, A.M.V.; Neto, A.C.S.; Vilar, A.T.S.; Almeida, B.G.C.; Albuquerque, C.M.F.; Fermoseli, A.F.O. Transtornos de ansiedade: Um estudo de prevalência sobre as fobias específicas e a importância da ajuda psicológica. Cad. Grad.-Ciências Biológicas Saúde 2015, 3, 115–128. [Google Scholar]
- Redmond, S.; Paterson, N.; Shoemaker-Hunt, S.J.; Ramalho-de-Oliveira, D. Development, Testing and Results of a Patient Medication Experience Documentation Tool for Use in Comprehensive Medication Management Services. Pharmacy 2019, 7, 71. [Google Scholar] [CrossRef]
- Ramalho-de-Oliveira, D. Overview and Prospect of Autoethnography in Pharmacy Education and Practice. Am. J. Pharm. Educ. 2020, 84, 7127. [Google Scholar] [CrossRef]
- Pinto, P.F.P.S.; Santos, B.P.S.D.; Teixeira, C.S.S.; Nery, J.S.; Amorim, L.D.A.F.; Sanchez, M.N.; Barreto, M.L.; Pescarini, J.M. Performance evaluation of tuberculosis control in Brazilian municipalities. Rev. Saude Publica 2022, 56, 53. [Google Scholar] [CrossRef]


{kind=link}
| Theme 1: Treatment Abandonment |
|---|
| Patient states that if s/he had not abandoned the treatment, s/he would not have been hospitalized (P25). |
| Patient associates the dose adjustment or inclusion of a new drug in the therapy as a personal failure because s/he had experienced treatment failure due to non-adherence in the past. Patient reports non-adherence to antiretroviral therapy because of a personal preference not to use the medications (P68). |
| “I didn’t value the medication”. S/He is an alcoholic and a smoker, lives alone with no family support “in a little shed with two rooms, a bathroom and a washing tank area”. Patient has a history of poor treatment adherence and multiple dropouts. Patient has no option to pick up medications elsewhere when they are not available at the primary healthcare unit (P51). |
| Young patient with a history of sexual violence at the age of 13 (probable source of HIV/AIDS transmission). Patient expressed to an aunt no intention to be treated and a will to die, thus “throwing in the towel”. Patient did not continue the treatment, even though the medications were available. The follow-up nursing technician reported that this patient refuses the medications and sometimes throws them away and feels “very confused” (P3). |
| Variable | n | % |
|---|---|---|
| Does the patient have any objection to using the medication? | ||
| Does not like to take it for cultural reasons (religion, others) | 0 | 0.0 |
| Has doubts regarding its use | 7 | 8.6 |
| Does not feel that it brings benefits to his/her health | 1 | 1.2 |
| Did not have access to the drug due to its price | 9 | 11.1 |
| Associates it with a stigma or feels embarrassed to use it | 4 | 4.9 |
| Does not feel comfortable with the way it is administered (route of administration) | 10 | 12.4 |
| Price and route of administration | 3 | 3.7 |
| Has no objection | 45 | 55.6 |
| Other reasons | 1 | 1.2 |
| Did not answer | 1 | 1.2 |
| Is the patient afraid or concerned about adverse effects? | ||
| Current personal adverse effects | 15 | 18.5 |
| Past personal adverse effects | 15 | 18.5 |
| Observed a friend or a family member in the past with adverse reactions | 2 | 2.4 |
| Current and past personal adverse effects | 2 | 2.4 |
| No fear or concern about adverse effects | 46 | 56.7 |
| Did not answer | 1 | 1.2 |
| Is the patient afraid or concerned about any of these below? | ||
| Becoming dependent on some medication | 16 | 19.7 |
| Becoming dependent on some medication and generic or similar drugs are not effective | 4 | 4.9 |
| Generic or similar drugs are not effective | 8 | 9.9 |
| No fear or concern about these aspects | 52 | 64.2 |
| Did not answer | 1 | 1.2 |
| If the patient could choose, which type of therapy would s/he prefer? | ||
| Pharmacological | 24 | 29.6 |
| Non-pharmacological—change in lifestyle | 41 | 50.6 |
| Pharmacological and non-pharmacological | 8 | 9.9 |
| None | 3 | 3.7 |
| Did not answer or does not know | 5 | 6.2 |
| What does it mean for the patient to have his/her dose adjusted or medication changed? | ||
| Personal failure | 5 | 6.2 |
| Worsening in state of health | 19 | 23.5 |
| Personal failure and worsening in state of health | 1 | 1.2 |
| A necessary adjustment | 50 | 61.7 |
| Did not answer or does not know | 6 | 7.4 |
| Does the patient self-medicate? | ||
| No | 29 | 35.8 |
| Yes | 48 | 59.3 |
| Did not answer | 4 | 4.9 |
| Theme 2: Adversity |
|---|
| “They didn’t tell me the name (of the medicine), as if I was a doormat… experimenting the shot [in me]” (P15). |
| Patient stated that s/he felt like a “guinea pig” with the withdrawal and introduction of medications (P2). |
| Patient stated that when s/he took the medication at night s/he had neuropsychiatric effects, and this prevented him/her from working. S/He was a machine operator and was off the antiretroviral drugs for three years. When s/he returned to the hospital, s/he had AIDS and tuberculosis. S/He claims to be afraid of the adverse effects s/he had in the past with a yellow pill that caused him/her insomnia (P37). |
| Theme 3: Socially Constructed Aspects |
|---|
| “I feel embarrassed to take (the medicines) in front of other people” (P51). |
| “It’s hard for me to take home so many medicines” (P68). |
| “I’m afraid of becoming dependent on medications, even though I have already become (drug cocktail)” (P76). |
| Patient states that s/he is afraid of becoming dependent on any medication and that s/he is “anti-drug” (P34). |
| Patient was healthy before (…) and vented “Now I’ll have to be dependent on medication.” (P22) |
| Patient claims to be afraid or concerned that generic or similar drugs are not effective, because “in Brazil (they) don’t believe in generic drugs; (they) always prefer the original” (P40). |
| Theme 4: Resolvability |
|---|
| Patient states that s/he has no problems with using medications and states that s/he “takes up to ten pills at once.” Has observed adverse drug reactions in his/her spouse but reports no fear or concern. S/He prefers a change in lifestyle to taking medications but understands that antiretroviral treatment is of continuous use (P12). |
| Patient states, regarding antiretrovirals, that “will never stop [taking them]; only when there is a cure” (P10). |
| Theme 5: Ambivalence |
|---|
| “I find it strange to use this much medication, I feel hostage to using these medicines. I avoid getting drugs into my body as much as possible” (P17). |
| Patient stated that the medications s/he uses are very strong and that s/he gets worried about getting worse with the use of these drugs (P23). |
| S/He also claimed that the medications bring benefits, but “s/he doesn’t like to take them very much” (P5). |
| In relation to the medications, patient states that “s/he takes them with fear indeed” (P53). |
| S/He reported concern about using the medications, since s/he did not take any before being hospitalized and knows that when s/he is discharged s/he will have to use many (P20). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Resende, N.H.d.; Martins, U.C.d.M.; Ramalho-de-Oliveira, D.; Silva, D.I.d.; de Miranda, S.S.; Reis, A.M.M.; Carvalho, W.d.S.; Mendonça, S.d.A.M. The Medication Experience of TB/HIV Coinfected Patients: Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 15153. https://doi.org/10.3390/ijerph192215153
Resende NHd, Martins UCdM, Ramalho-de-Oliveira D, Silva DId, de Miranda SS, Reis AMM, Carvalho WdS, Mendonça SdAM. The Medication Experience of TB/HIV Coinfected Patients: Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(22):15153. https://doi.org/10.3390/ijerph192215153
Chicago/Turabian StyleResende, Natália Helena de, Ursula Carolina de Morais Martins, Djenane Ramalho-de-Oliveira, Dirce Inês da Silva, Silvana Spíndola de Miranda, Adriano Max Moreira Reis, Wânia da Silva Carvalho, and Simone de Araújo Medina Mendonça. 2022. "The Medication Experience of TB/HIV Coinfected Patients: Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 22: 15153. https://doi.org/10.3390/ijerph192215153
APA StyleResende, N. H. d., Martins, U. C. d. M., Ramalho-de-Oliveira, D., Silva, D. I. d., de Miranda, S. S., Reis, A. M. M., Carvalho, W. d. S., & Mendonça, S. d. A. M. (2022). The Medication Experience of TB/HIV Coinfected Patients: Qualitative Study. International Journal of Environmental Research and Public Health, 19(22), 15153. https://doi.org/10.3390/ijerph192215153