
Mindfulness on Rumination in Patients with Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
 , ,
, ,
Abstract
:1. Introduction
2. Method
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Methodological Quality of Studies and Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Article Screening Process and Results
3.2. Basic Characteristics of Included Articles
3.3. Risk of Bias of Included Studies
3.4. Meta-Analysis
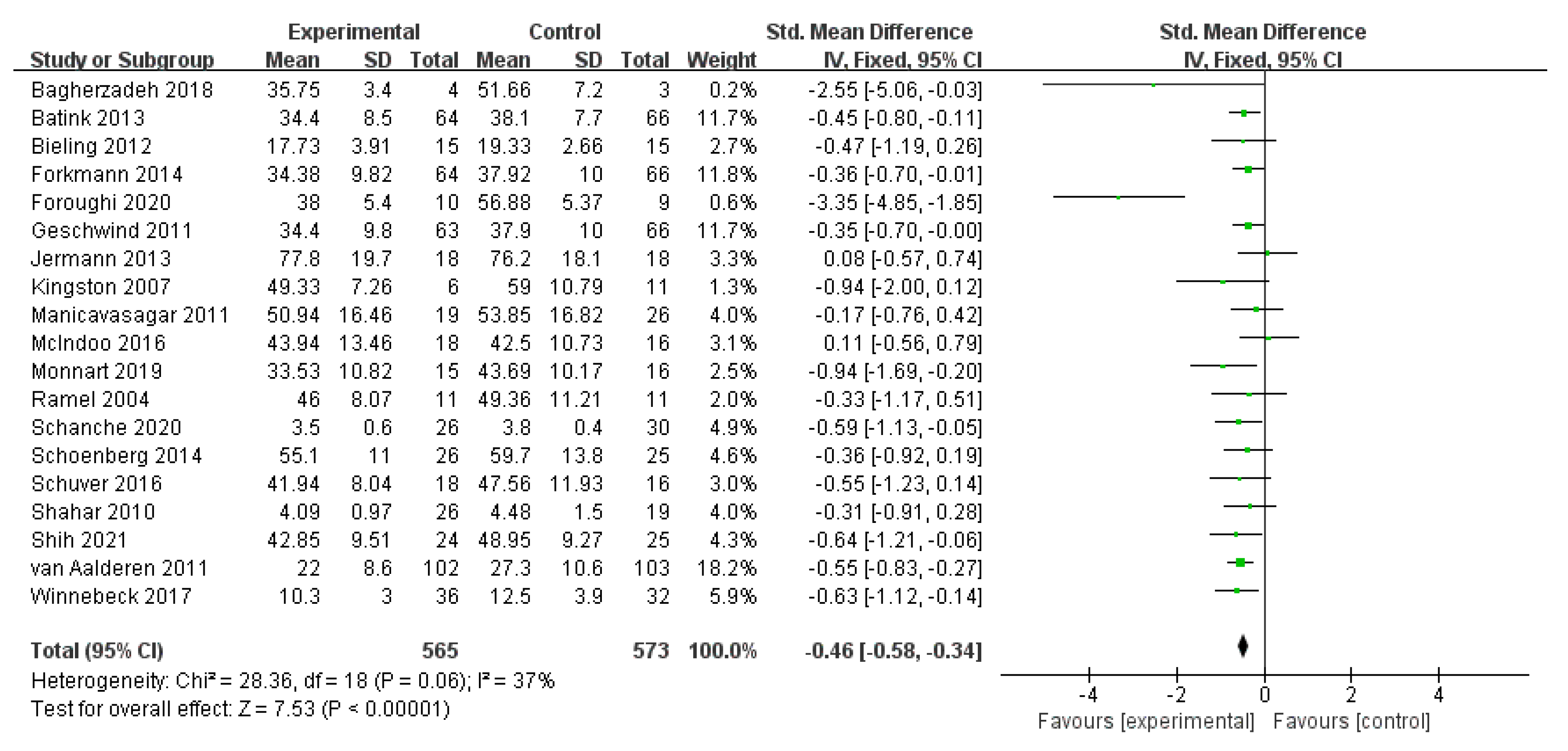
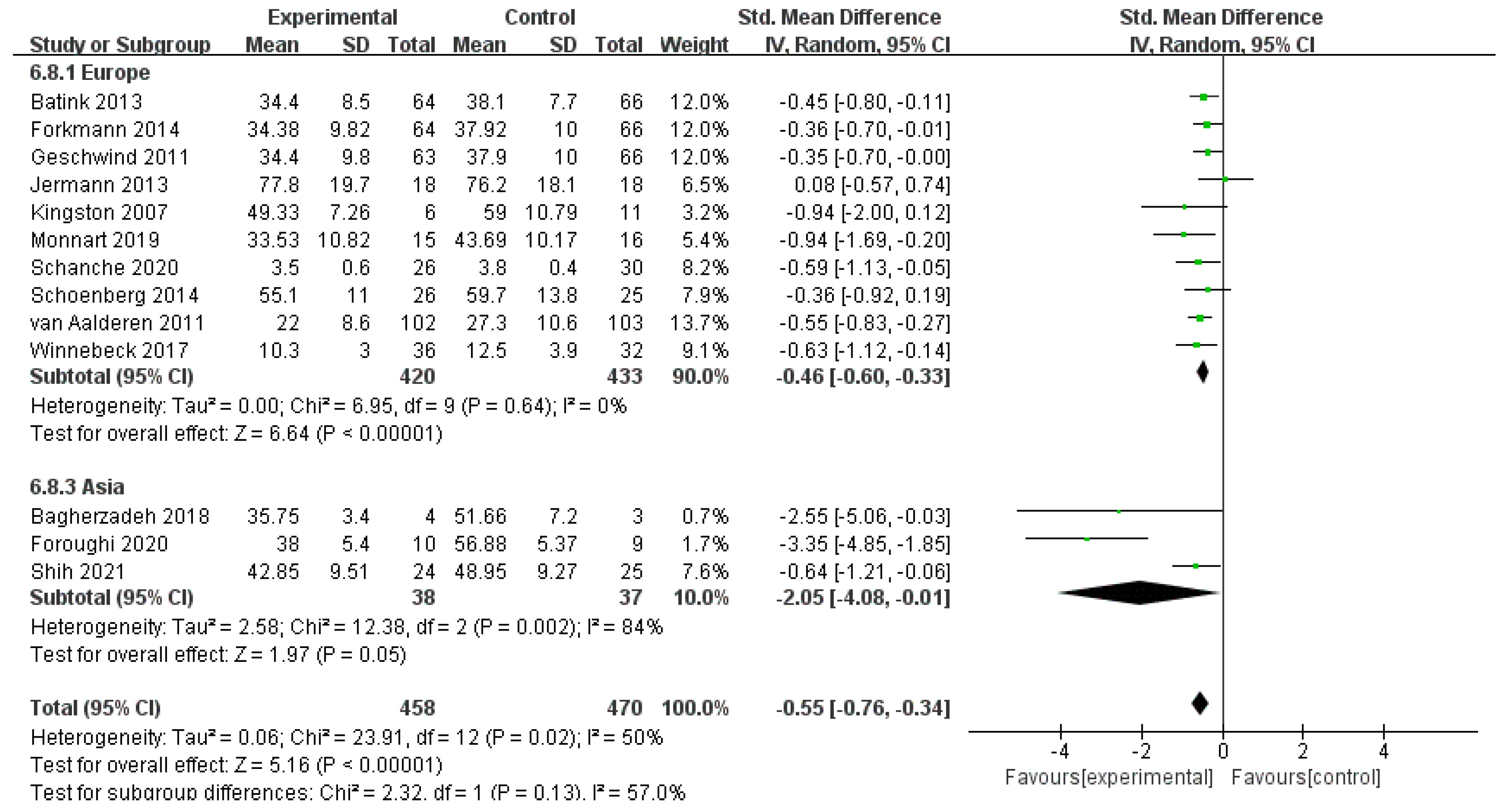
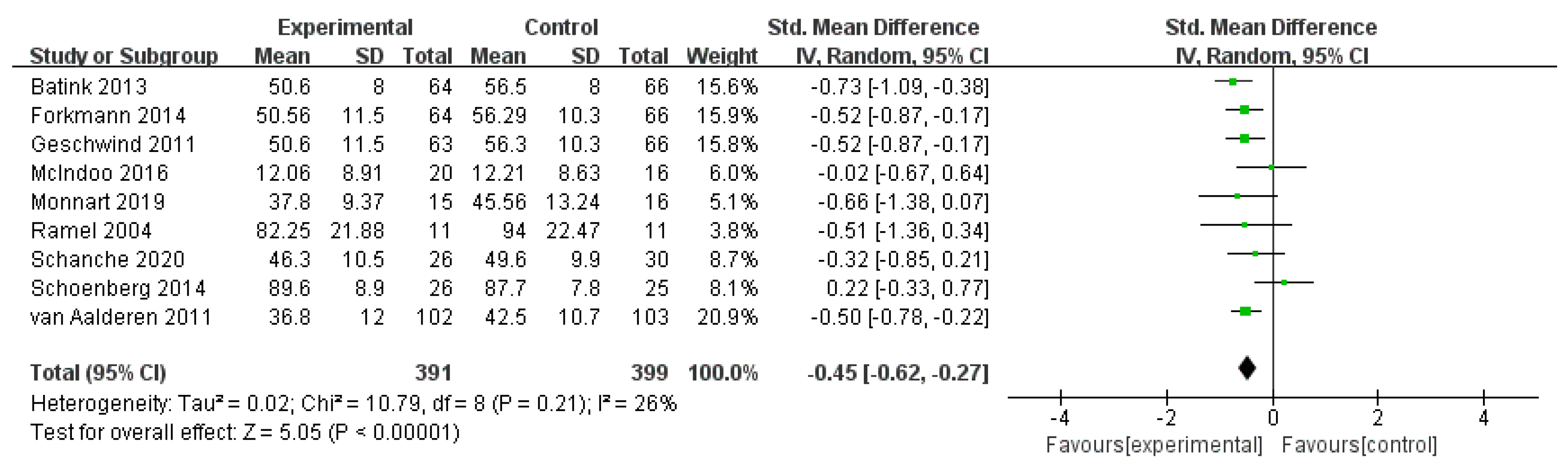
3.4.1. Effects of MBIs on Rumination in Patients with Depressive Disorder
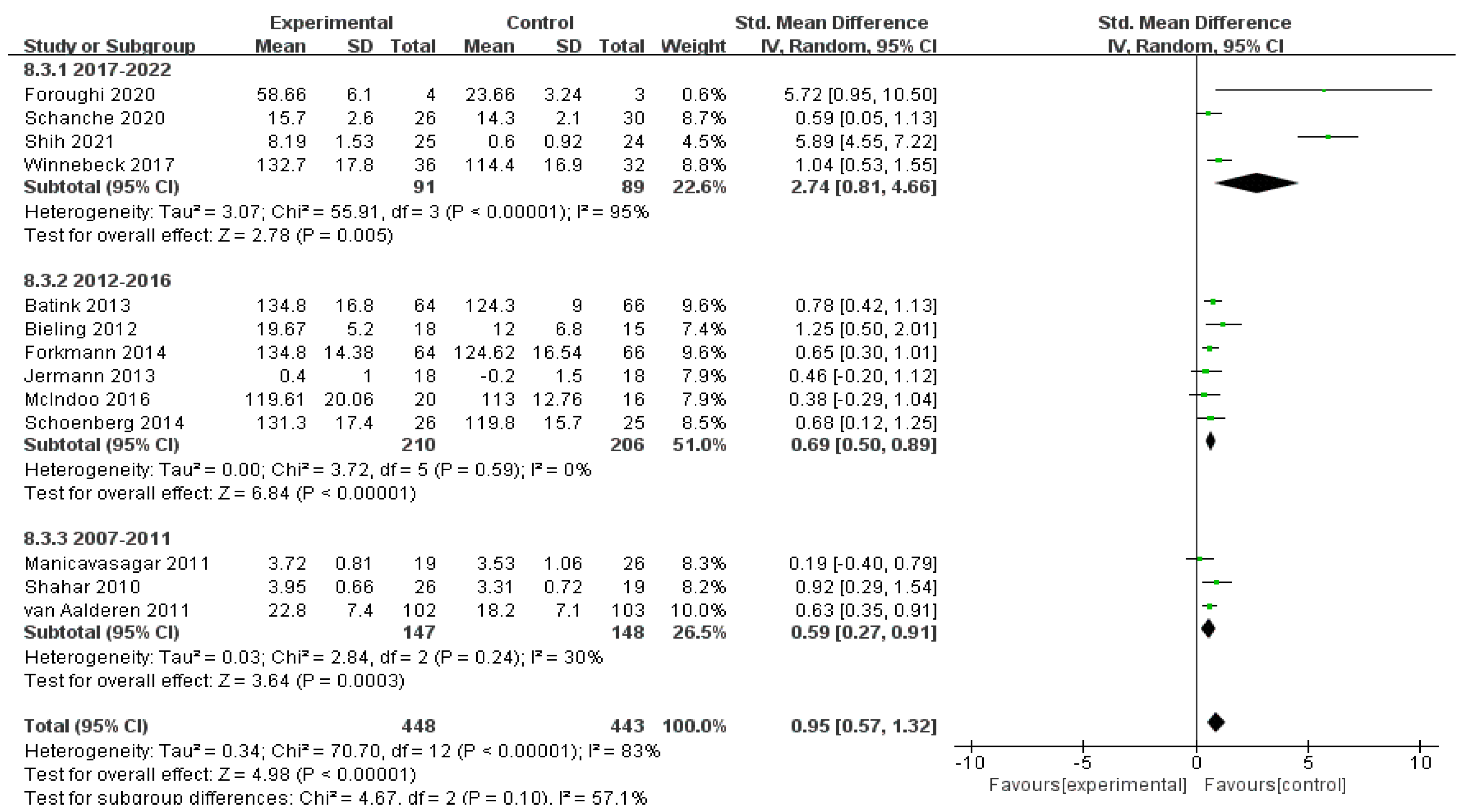
3.4.2. Effects of MBIs on Mindfulness in Patients with Depressive Disorder
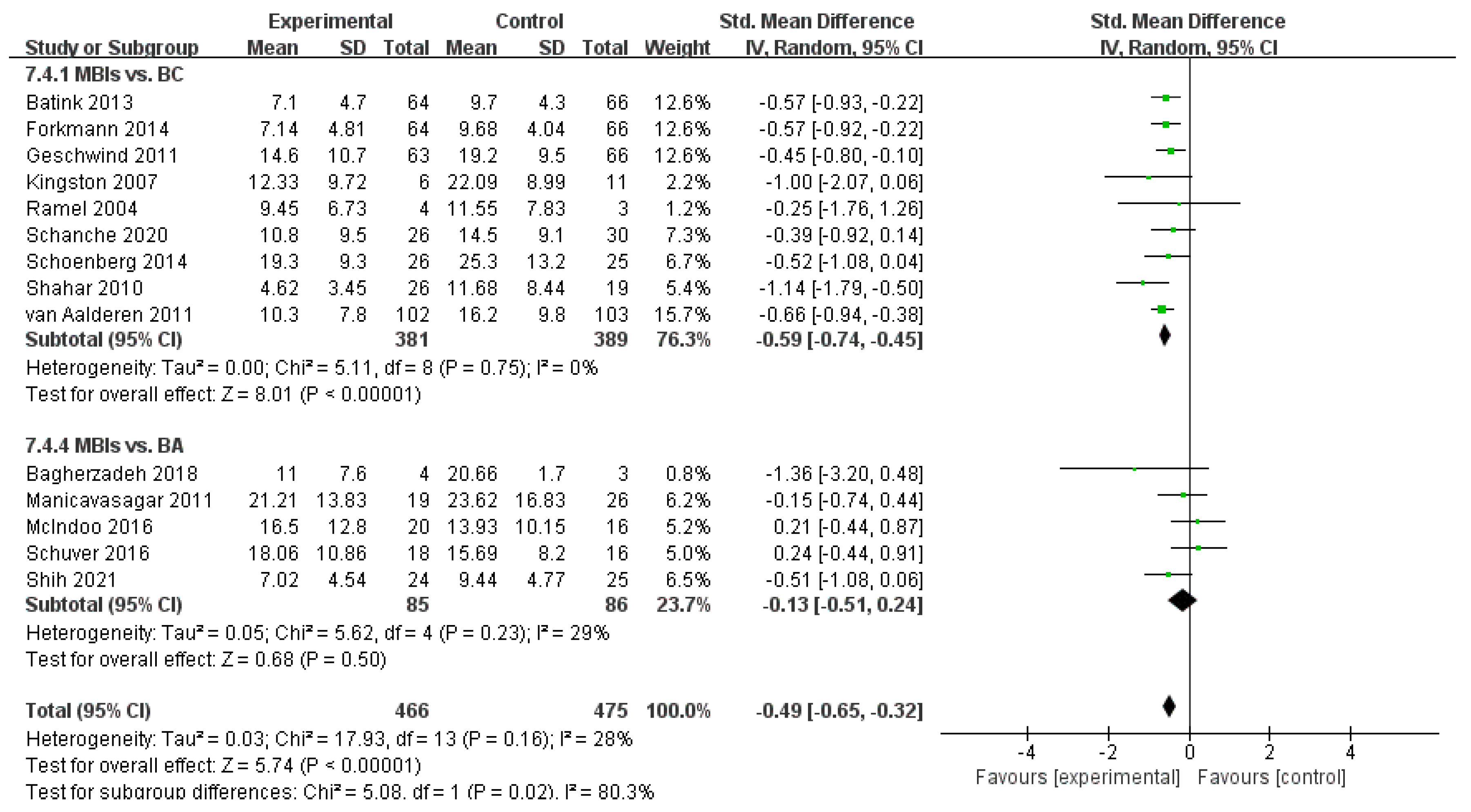
3.4.3. Effects of MBIs on Depression in Patients with Depressive Disorder
3.4.4. Effects of MBIs on Anxiety in Patients with Depressive Disorder
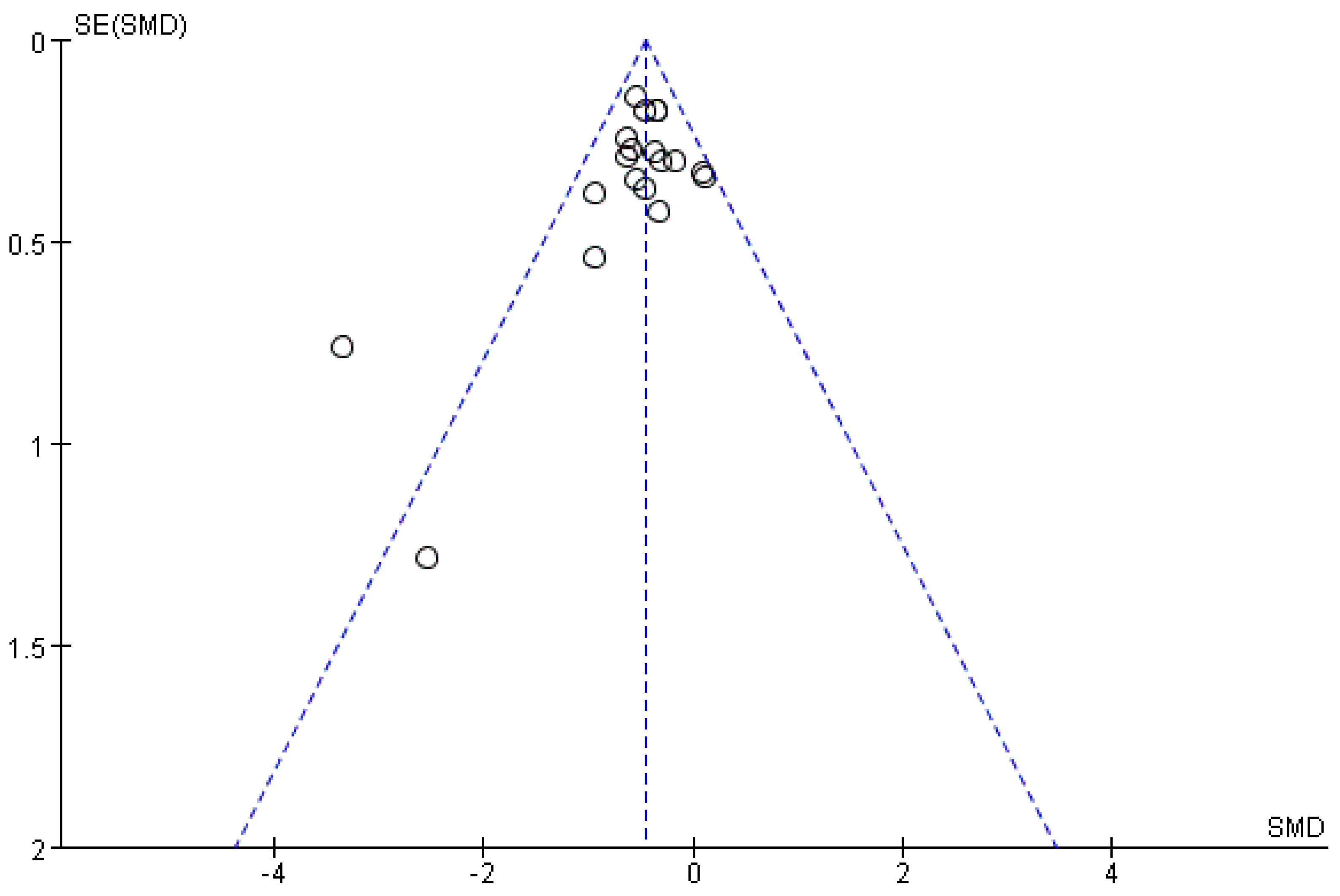
3.4.5. Analysis of Article Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haeffel, G.J. After Further Deliberation: Cognitive Vulnerability Predicts Changes in Event-Specific Negative Inferences for a Poor Midterm Grade. Cogn. Ther. Res. 2011, 35, 285–292. [Google Scholar] [CrossRef]
- Young, C.C.; Lamontagne, L.L.; Dietrich, M.S.; Wells, N. Cognitive Vulnerabilities, Negative Life Events, and Depressive Symptoms in Young Adolescents. Arch. Psychiatr. Nurs. 2012, 26, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Gotlib, I.H.; Joormann, J. Cognition and depression: Current status and future directions. Annu. Rev. Clin. Psychol. 2010, 6, 285–312. [Google Scholar] [CrossRef] [Green Version]
- Nolen-Hoeksema, S.; Wisco, B.E.; Lyubomirsky, S. Rethinking Rumination. Perspect. Psychol. Sci. 2008, 3, 400–424. [Google Scholar] [CrossRef]
- Watkins, E.R.; Roberts, H. Reflecting on rumination: Consequences, causes, mechanisms and treatment of rumination. Behav. Res. Ther. 2020, 127, 103528–103573. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S. Responses to depression and their effects on the duration of depressive episodes. J. Abnorm. Psychol. (1965) 1991, 100, 569. [Google Scholar] [CrossRef] [PubMed]
- Rimes, K.A.; Watkins, E. The effects of self-focused rumination on global negative self-judgements in depression. Behav. Res. Ther. 2005, 43, 1673–1681. [Google Scholar] [CrossRef] [PubMed]
- Lyubomirsky, S.; Kasri, F.; Zehm, K. Dysphoric Rumination Impairs Concentration on Academic Tasks. Cogn. Ther. Res. 2003, 27, 309. [Google Scholar] [CrossRef]
- Reilly, E.E.; Lavender, J.M.; Berner, L.A.; Brown, T.A.; Wierenga, C.E.; Kaye, W.H. Could repetitive negative thinking interfere with corrective learning? The example of anorexia nervosa. Int. J. Eat. Disord. 2019, 52, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Creswell, J.D. Mindfulness Interventions. Annu. Rev. Psychol. 2017, 68, 491–516. [Google Scholar] [CrossRef]
- Hu, Z.; Yu, H.; Zou, J.; Zhang, Y.; Lu, Z.; Hu, M. Relationship among self-injury, experiential avoidance, cognitive fusion, anxiety, and depression in Chinese adolescent patients with nonsuicidal self-injury. Brain Behav. 2021, 11, e2419. [Google Scholar] [CrossRef]
- Xiong, A.; Lai, X.; Wu, S.; Yuan, X.; Tang, J.; Chen, J.; Liu, Y.; Hu, M. Relationship Between Cognitive Fusion, Experiential Avoidance, and Obsessive-Compulsive Symptoms in Patients With Obsessive-Compulsive Disorder. Front. Psychol. 2021, 12, 655154. [Google Scholar] [CrossRef] [PubMed]
- Erisman, S.M.; Roemer, L. A preliminary investigation of the effects of experimentally induced mindfulness on emotional responding to film clips. Emotion 2010, 10, 72–82. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.; Posner, M.I. Attention training and attention state training. Trends Cogn. Sci. 2009, 13, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Watkins, E.; Teasdale, J.D.; Williams, R.M. Decentring and distraction reduce overgeneral autobiographical memory in depression. Psychol. Med. 2000, 30, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.A.; Rainville, P. Pain sensitivity and analgesic effects of mindful states in Zen meditators: A cross-sectional study. Psychosom. Med. 2009, 71, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, S.L.C.L. Mechanisms of mindfulness. J. Clin. Psychol. 2006, 62, 373–386. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.M.; Feldman, G. Clarifying the Construct of Mindfulness in the Context of Emotion Regulation and the Process of Change in Therapy. Clin. Psychol. 2004, 11, 255–262. [Google Scholar] [CrossRef]
- Thoma, N.; Pilecki, B.; Mckay, D. Contemporary Cognitive Behavior Therapy: A Review of Theory, History, and Evidence. Psychodyn. Psychiatry 2015, 43, 423–461. [Google Scholar] [CrossRef]
- Murfield, J.; Moyle, W.; O’donovan, A. Mindfulness- and compassion-based interventions for family carers of older adults: A scoping review. Int. J. Nurs. Stud. 2021, 116, 103495. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr. Clin. N. Am. 2017, 40, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Flynn, D.; Kells, M.; Joyce, M. Dialectical behaviour therapy: Implementation of an evidence-based intervention for borderline personality disorder in public health systems. Curr. Opin. Psychol. 2021, 37, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C. Acceptance and Commitment Therapy, Relational Frame Theory, and the Third Wave of Behavioral and Cognitive Therapies—Republished Article. Behav. Ther. 2016, 47, 869–885. [Google Scholar] [CrossRef] [PubMed]
- Hilcove, K.; Marceau, C.; Thekdi, P.; Larkey, L.; Brewer, M.A.; Jones, K. Holistic Nursing in Practice: Mindfulness-Based Yoga as an Intervention to Manage Stress and Burnout. J. Holist. Nurs. 2021, 39, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Beerse, M.E.; Van Lith, T.; Pickett, S.M.; Stanwood, G.D. Biobehavioral Utility of Mindfulness-Based Art Therapy: Neurobiological Underpinnings and Mental Health Impacts; SAGE Publications: London, UK, 2020; Volume 245, pp. 122–130. [Google Scholar]
- Kertz, S.J.; Koran, J.; Stevens, K.T.; Bj€orgvinsson, T. Repetitive negative thinking predicts depression and anxiety symptom improvement during brief cognitive behavioral therapy. Behav. Res. Ther. 2015, 68, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Michalak, J.; Holz, A.; Teismann, T. Rumination as a predictor of relapse in mindfulness-based cognitive therapy for depression. Psychol. Psychother. 2011, 84, 230–236. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Knoll, T.; Omar, M.I.; Maclennan, S.; Hernández, V.; Canfield, S.; Yuan, Y.; Bruins, M.; Marconi, L.; Poppel, H.V.; Dow, J.N.; et al. Key Steps in Conducting Systematic Reviews for Underpinning Clinical Practice Guidelines: Methodology of the European Association of Urology. Eur. Urol. 2018, 73, 290–300. [Google Scholar] [CrossRef] [Green Version]
- Foroughi, A.; Sadeghi, K.; Parvizifard, A.; Moghadam, A.P.; Davarinejad, O.; Farnia, V.; Azar, G. The effectiveness of mindfulness-based cognitive therapy for reducing rumination and improving mindfulness and self-compassion in patients with treatment-resistant depression. Trends Psychiatry Psychother. 2020, 42, 138–146. [Google Scholar] [CrossRef]
- Monnart, A.; Vanderhasselt, M.A.; Schroder, E.; Campanella, S.; Fontaine, P.; Kornreich, C. Treatment of Resistant Depression: A Pilot Study Assessing the Efficacy of a tDCS-Mindfulness Program Compared With a tDCS-Relaxation Program. Front. Psychiatry 2019, 10, 730. [Google Scholar] [CrossRef]
- Batink, T.; Peeters, F.; Geschwind, N.; van Os, J.; Wichers, M. How does MBCT for depression work? studying cognitive and affective mediation pathways. PLoS ONE 2013, 8, e72778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahar, B.; Britton, W.B.; Sbarra, D.A.; Figueredo, A.J.; Bootzin, R.R. Mechanisms of Change in Mindfulness-Based Cognitive Therapy for Depression: Preliminary Evidence from a Randomized Controlled Trial. Int. J. Cogn. Ther. 2010, 3, 402–418. [Google Scholar] [CrossRef]
- Bieling, P.J.; Hawley, L.L.; Bloch, R.T.; Corcoran, K.M.; Levitan, R.D.; Young, L.T.; Macqueen, G.M.; Segal, Z.V. Treatment-specific changes in decentering following mindfulness-based cognitive therapy versus antidepressant medication or placebo for prevention of depressive relapse. J. Consult. Clin. Psychol. 2012, 80, 365–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcindoo, C.C.; File, A.A.; Preddy, T.; Clark, C.G.; Hopko, D.R. Mindfulness-based therapy and behavioral activation: A randomized controlled trial with depressed college students. Behav. Res. Ther. 2016, 77, 118–128. [Google Scholar] [CrossRef]
- Schanche, E.; Vøllestad, J.; Visted, E.; Svendsen, J.L.; Osnes, B.; Binder, P.E.; Franer, P.; Sørensen, L. The effects of mindfulness-based cognitive therapy on risk and protective factors of depressive relapse—A randomized wait-list controlled trial. BMC Psychol. 2020, 8, 1–57. [Google Scholar] [CrossRef]
- Winnebeck, E.; Fissler, M.; Gärtner, M.; Chadwick, P.; Barnhofer, T. Brief training in mindfulness meditation reduces symptoms in patients with a chronic or recurrent lifetime history of depression: A randomized controlled study. Behav. Res. Ther. 2017, 99, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Jermann, F.; Van der Linden, M.; Gex-Fabry, M.; Guarin, A.; Kosel, M.; Bertschy, G.; Aubry, J.M.; Bondolfi, G. Cognitive Functioning in Patients Remitted from Recurrent Depression: Comparison with Acutely Depressed Patients and Controls and Follow-up of a Mindfulness-Based Cognitive Therapy Trial. Cogn. Ther. Res. 2013, 37, 1004–1014. [Google Scholar] [CrossRef] [Green Version]
- Schuver, K.J.; Lewis, B.A. Mindfulness-based yoga intervention for women with depression. Complement. Ther. Med. 2016, 26, 85–91. [Google Scholar] [CrossRef]
- Geschwind, N.; Peeters, F.; Drukker, M.; van Os, J.; Wichers, M. Mindfulness Training Increases Momentary Positive Emotions and Reward Experience in Adults Vulnerable to Depression: A Randomized Controlled Trial. J. Consult. Clin. Psychol. 2011, 79, 618–628. [Google Scholar] [CrossRef] [Green Version]
- Bagherzadeh Ledari, R.; Masjedi, A.; Bakhtyari, M.; Zarghami, M.; Nouri, R.; Hosseini, H. A Comparison Between the Effectiveness of Acceptance and Commitment Treatment and Behavioral Activation Treatment for Depression on Symptoms Severity and Rumination Among Patients with Treatment-Resistant Depression. Iran. J. Psychiatry Behav. Sci. 2018, 12, e10742. [Google Scholar] [CrossRef]
- Kingston, T.; Dooley, B.; Bates, A.; Lawlor, E.; Malone, K. Mindfulness-based cognitive therapy for residual depressive symptoms. Psychol. Psychother. Theory Res. Pract. 2007, 80, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forkmann, T.; Wichers, M.; Geschwind, N.; Peeters, F.; van Os, J.; Mainz, V.; Collip, D. Effects of mindfulness-based cognitive therapy on self-reported suicidal ideation: Results from a randomised controlled trial in patients with residual depressive symptoms. Compr. Psychiatry 2014, 55, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- van Aalderen, J.R.; Donders, A.R.; Giommi, F.; Spinhoven, P.; Barendregt, H.P.; Speckens, A. The efficacy of mindfulness-based cognitive therapy in recurrent depressed patients with and without a current depressive episode: A randomized controlled trial. Psychol. Med. 2012, 42, 989–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manicavasagar, V.; Perich, T.; Parker, G. Cognitive Predictors of Change in Cognitive Behaviour Therapy and Mindfulness-Based Cognitive Therapy for Depression. Behav. Cogn. Psychother. 2012, 40, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Shih, V.; Chan, W.C.; Tai, O.K.; Wong, H.L.; Cheng, C.; Wong, C. Mindfulness-Based Cognitive Therapy for Late-Life Depression: A Randomised Controlled Trial. East Asian Arch. Psychiatry 2021, 31, 27–35. [Google Scholar] [CrossRef]
- Ramel, W.; Goldin, P.R.; Carmona, P.E.; McQuaid, J.R. The effects of mindfulness meditation on cognitive processes and affect in patients with past depression. Cogn. Ther. Res. 2004, 28, 433–455. [Google Scholar] [CrossRef]
- Schoenberg, P.L.; Speckens, A.E. Modulation of induced frontocentral theta (Fm-theta) event-related (de-)synchronisation dynamics following mindfulness-based cognitive therapy in Major Depressive Disorder. Cogn. Neurodyn. 2014, 8, 373–388. [Google Scholar] [CrossRef] [Green Version]
- Perestelo-Perez, L.; Barraca, J.; Peñate, W.; Rivero-Santana, A.; Alvarez-Perez, Y. Mindfulness-based interventions for the treatment of depressive rumination: Systematic review and meta-analysis. Int. J. Clin. Health Psychol. 2017, 17, 282–295. [Google Scholar] [CrossRef]
- Whitmer, A.J.; Gotlib, I.H. Switching and backward inhibition in major depressive disorder: The role of rumination. J. Abnorm. Psychol. (1965) 2012, 121, 570. [Google Scholar] [CrossRef] [Green Version]
- Dimidjian, S.; Beck, A.; Felder, J.N.; Boggs, J.M.; Gallop, R.; Segal, Z.V. Web-based Mindfulness-based Cognitive Therapy for reducing residual depressive symptoms: An open trial and quasi-experimental comparison to propensity score matched controls. Behav. Res. Ther. 2014, 63, 83–89. [Google Scholar] [CrossRef]
- Quaglia, J.T.; Brown, K.W.; Lindsay, E.K.; Creswell, J.D.; Goodman, R.J. From conceptualization to operationalization of mindfulness. In Handbook of Mindfulness: Theory, Research, and Practice; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Crego, A.; Yela, J.R.; Gómez-Martínez, M.Á.; Riesco-Matías, P.; Petisco-Rodríguez, C. Relationships between Mindfulness, Purpose in Life, Happiness, Anxiety, and Depression: Testing a Mediation Model in a Sample of Women. Int. J. Environ. Res. Public Health 2021, 18, 925. [Google Scholar] [CrossRef] [PubMed]
- Hartstone, J.M.; Medvedev, O.N. The Role of Mindfulness and Life Satisfaction in Psychological Distress During the COVID-19 Lockdown in New Zealand: A Quasi-experimental Study. Mindfulness 2021, 12, 2693–2706. [Google Scholar] [CrossRef] [PubMed]
- Mayer, B.; Polak, M.; Remmerswaal, D. Mindfulness, interpretation bias, and levels of anxiety and depression: Two mediation studies. Mindfulness 2018, 10, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Servaas, M.N.; Riese, H.; Ormel, J.; Aleman, A. The neural correlates of worry in association with individual differences in neuroticism: Neuroticism and Worry in the Brain. Hum. Brain Mapp. 2014, 35, 4303–4315. [Google Scholar] [CrossRef] [PubMed]
- Mcevoy, P.M.; Watson, H.; Watkins, E.R.; Nathan, P. The relationship between worry, rumination, and comorbidity: Evidence for repetitive negative thinking as a transdiagnostic construct. J. Affect. Disord. 2013, 151, 313–320. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | N | Female | Intervention Measures | Follow-Up Time (Months) | Ex vs. Con | Outcome Measure | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author, Year | Ex/Con | % | Ex | Con | Rumination | Depression | Mindfulness | Anxiety | |||
| Foroughi et al. [30], 2020 | Iran | 10/9 | 72.2 | MBCT | WL | 1 | > | RRS | BDI-II | SMQ | / |
| Monnart et al. [31], 2019 | Belgium | 15/16 | 64.5 | MBCT | relaxation | / | > | SARI | MADRS | / | STAI |
| Batink et al. [32], 2013 | Netherlands | 64/66 | 75.4 | MBCT | TAU | / | > | RSS | HDRS | KIMS | PSWQ |
| Shahar et al. [33], 2010 | USA | 26/19 | 84.4 | MBCT | WL | / | = | RRS | BDI | MAAS | / |
| Bieling et al. [34], 2012 | Canada | 15/15 | 58 | MBCT | pill placebo | / | = | EQ-R | / | TMS | / |
| McIndoo et al. [35], 2016 | USA | 18/12 | 58.8 | MBT | BA | 1 | = | RRS | BDI-II | FFMQ | BAI |
| Schanche et al. [36], 2020 | Norway | 26/30 | 73.4 | MBCT | WL | / | > | RRQ | BDI-II | FFMQ | STAI |
| Winnebeck et al. [37], 2017 | Germany | 36/32 | 60.3 | MBI | psycho education | / | > | RRS | BDI-II | FFMQ | / |
| Jermann et al. [38], 2013 | switzerland | 18/18 | 69.4 | MBCT | TAU | 6 | = | RRQ | BDI-II | MAAS | / |
| Schuver et al. [39], 2016 | USA | 18/16 | 100 | MBYI | walking control | 1 | = | RSS | BDI | / | / |
| Geschwind et al. [40], 2011 | Netherlands | 63/66 | 75.6 | MBCT | WL | / | > | RRS | IDS | / | STAI |
| Bagherzadeh et al. [41], 2018 | Iran | 4/3 | 85.7 | ACT | BA | 1.5 | > | RRS | BDI-II | / | / |
| Kingston et al. [42], 2007 | Ireland | 6/11 | 88.2 | MBCT | TAU | / | = | RRS | BDI | / | / |
| Forkmann et al. [43], 2014 | Germany | 64/66 | 75.4 | MBCT | TAU | / | > | RSS | HDRS | KIMS | PSWQ |
| van Aalderen et al. [44], 2011 | Netherlands | 102/103 | 70.7 | MBCT | TAU | / | > | RSS | BDI | KIMS | PSWQ |
| Manicavasagar et al. [45], 2011 | Australian | 19/26 | 64.4 | MBCT | CBT | / | = | RRS | BDI-II | MAAS | / |
| Shih et al. [46], 2021 | China | 24/25 | 87.7 | MBCT | BA | / | > | RRS | HDRS | MAAS | / |
| Ramel et al. [47], 2004 | USA | 11/11 | 45.5 | MBSR | WL | / | = | RSQ | BDI | / | STAI |
| Schoenberg et al. [48], 2014 | Netherlands | 26/25 | 62.8 | MBCT | WL | / | = | RRS | IDS | FFMQ | STAI |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, P.; Mao, L.; Hu, M.; Lu, Z.; Yuan, X.; Zhang, Y.; Hu, Z. Mindfulness on Rumination in Patients with Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 16101. https://doi.org/10.3390/ijerph192316101
Li P, Mao L, Hu M, Lu Z, Yuan X, Zhang Y, Hu Z. Mindfulness on Rumination in Patients with Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(23):16101. https://doi.org/10.3390/ijerph192316101
Chicago/Turabian StyleLi, Pan, Lingyun Mao, Maorong Hu, Zihang Lu, Xin Yuan, Yanyan Zhang, and Zhizhong Hu. 2022. "Mindfulness on Rumination in Patients with Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 23: 16101. https://doi.org/10.3390/ijerph192316101