
Age-Based Differences in Sleep Quality, Pre-Sleep Arousal, and Psychosocial Factors during the Second Wave Lockdown of the COVID-19 Pandemic in Georgia—A Higher Vulnerability of Younger People

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Sleep-Wake Patterns
3.3. Sleep Quality
3.4. PSQI Component Scores
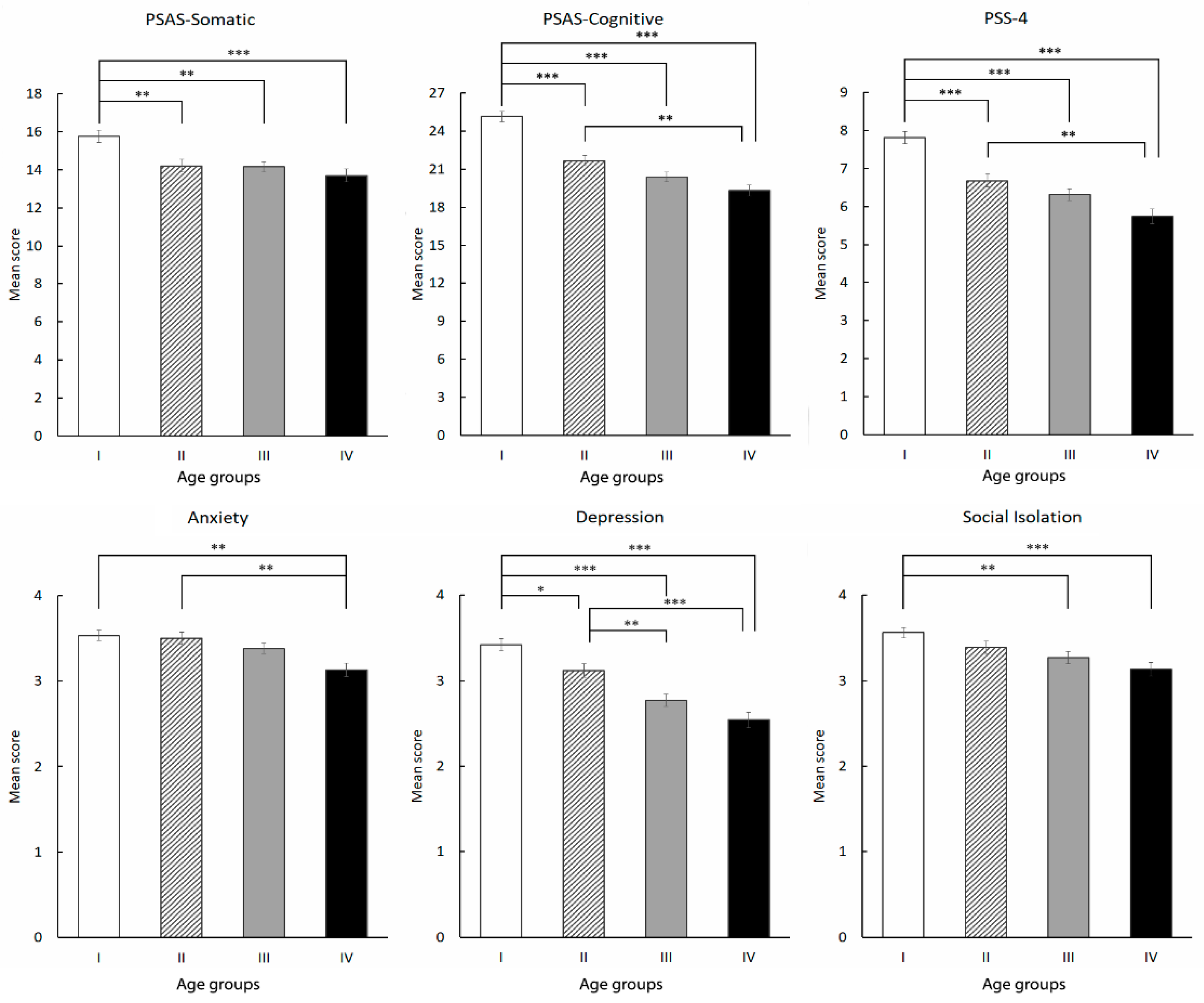
3.5. Pre-Sleep Arousal and Psychosocial Variables
3.6. Risk Factors of Poor Sleep Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jahrami, H.; BaHammam, A.S.; Bragazzi, N.L.; Saif, Z.; Faris, M.; Vitiello, M.V. Sleep problems during the COVID-19 pandemic by population: A systematic review and meta-analysis. J. Clin. Sleep Med. 2021, 17, 299–313. [Google Scholar] [CrossRef]
- Liu, C.; Pan, W.; Li, L.; Li, B.; Ren, Y.; Ma, X. Prevalence of depression, anxiety, and insomnia symptoms among patients with COVID-19: A meta-analysis of quality effects model. J. Psychosom. Res. 2021, 147, 110516. [Google Scholar] [CrossRef]
- Morin, C.M.; Bjorvatn, B.; Chung, F.; Holzinger, B.; Partinen, M.; Penzel, T.; Ivers, H.; Wing, Y.K.; Chan, N.Y.; Merikanto, I.; et al. Insomnia, anxiety, and depression during the COVID-19 pandemic: An international collaborative study. Sleep Med. 2021, 87, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Blume, C.; Schmidt, M.H.; Cajochen, C. Effects of the COVID-19 lockdown on human sleep and rest-activity rhythms. Curr. Biol. 2020, 30, R795–R797. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Alfonsi, V.; Gorgoni, M.; Scarpelli, S.; Zivi, P.; Sdoia, S.; Mari, E.; Fraschetti, A.; Ferlazzo, F.; Giannini, A.M.; De Gennaro, L. COVID-19 lockdown and poor sleep quality: Not the whole story. J. Sleep Res. 2021, 30, e13368. [Google Scholar] [CrossRef]
- Cellini, N.; Conte, F.; De Rosa, O.; Giganti, F.; Malloggi, S.; Reyt, M.; Guillemin, C.; Schmidt, C.; Muto, V.; Ficca, G. Changes in sleep timing and subjective sleep quality during the COVID-19 lockdown in Italy and Belgium: Age, gender and working status as modulating factors. Sleep Med. 2021, 77, 112–119. [Google Scholar] [CrossRef]
- Gorgoni, M.; Scarpelli, S.; Mangiaruga, A.; Alfonsi, V.; Bonsignore, M.R.; Fanfulla, F.; Ferini-Strambi, L.; Nobili, L.; Plazzi, G.; De Gennaro, L.; et al. Pre-sleep arousal and sleep quality during the COVID-19 lockdown in Italy. Sleep Med. 2021, 88, 46–57. [Google Scholar] [CrossRef]
- Gorgoni, M.; Scarpelli, S.; Mangiaruga, A.; Alfonsi, V.; Bonsignore, M.R.; Fanfulla, F.; Ferini-Strambi, L.; Nobili, L.; Plazzi, G.; De Gennaro, L.; et al. Persistence of the Effects of the COVID-19 Lockdown on Sleep: A Longitudinal Study. Brain Sci. 2021, 11, 1520. [Google Scholar] [CrossRef]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020, 29, e13052. [Google Scholar] [CrossRef]
- Roma, P.; Monaro, M.; Colasanti, M.; Ricci, E.; Biondi, S.; Di Domenico, A.; Cristina Verrocchio, M.; Napoli, C.; Ferracuti, S.; Mazza, C. A 2-month follow-up study of psychological distress among italian people during the COVID-19 lockdown. Int. J. Environ. Res. Public Health 2020, 17, 8180. [Google Scholar] [CrossRef] [PubMed]
- Wright, K.P., Jr.; Linton, S.K.; Withrow, D.; Casiraghi, L.; Lanza, S.M.; Iglesia, H.; Vetter, C.; Depner, C.M. Sleep in university students prior to and during COVID-19 Stay-at-Home orders. Curr. Biol. 2020, 30, R797–R798. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. [Google Scholar] [CrossRef] [PubMed]
- Bruni, O.; Malorgio, E.; Doria, M.; Finotti, E.; Spruyt, K.; Melegari, M.G.; Villa, M.P.; Ferri, R. Changes in sleep patterns and disturbances in children and adolescents in Italy during the COVID-19 outbreak. Sleep Med. 2022, 91, 166–174. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Beck, F.; Léger, D.; Fressard, L.; Peretti-Watel, P.; Verger, P.; Coconel Group. COVID-19 health crisis and lockdown associated with high level of sleep complaints and hypnotic uptake at the population level. J. Sleep Res. 2021, 30, e13119. [Google Scholar] [CrossRef]
- Quaglieri, A.; Lausi, G.; Fraschetti, A.; Burrai, J.; Barchielli, B.; Pizzo, A.; Cordellieri, P.; De Gennaro, L.; Gorgoni, M.; Ferlazzo, F.; et al. “Stay at Home” in Italy during the COVID-19 Outbreak: A Longitudinal Study on Individual Well-Being among Different Age Groups. Brain Sci. 2021, 11, 993. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Amicucci, G.; Salfi, F.; D’Atri, A.; Viselli, L.; Ferrara, M. The Differential Impact of COVID-19 Lockdown on Sleep Quality, Insomnia, Depression, Stress, and Anxiety among Late Adolescents and Elderly in Italy. Brain Sci. 2021, 11, 1336. [Google Scholar] [CrossRef]
- NCDC. Report of the National Center for Disease Control and Public Health; One Year with COVID-19. 5th Revision; NCDC: Tbilisi, Georgia, 2021. Available online: https://www.ncdc.ge/#/pages/content/24000387-0559-4268-bbcb-4310ebe67dec (accessed on 8 July 2022).
- Basishvili, T.; Oniani, N.; Sakhelashvili, I.; Eliozishvili, M.; Khizanashvili, M.; Arabidze, M.; Tsaava, M.; Charekishvili, T.; Tsertsvadze, N.; Darchia, N. Insomnia, Pre-Sleep Arousal, Psychosocial Factors and Changes in Sleep Pattern during the Second Wave Lockdown of the COVID-19 Pandemic in Georgia. Brain Sci. 2021, 12, 17. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Nicassio, P.M.; Mendlowitz, D.R.; Fussell, J.J.; Petras, L. The phenomenology of the pre-sleep state: The development of the pre-sleep arousal scale. Behav. Res. Ther. 1985, 23, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Puzino, K.; Amatrudo, G.; Sullivan, A.; Vgontzas, A.N.; Fernandez-Mendoza, J. Clinical Significance and Cut-Off Scores for the Pre-Sleep Arousal Scale in Chronic Insomnia Disorder: A Replication in a Clinical Sample. Behav. Sleep Med. 2020, 18, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapam, S., Oskamp, S., Eds.; Sage: Newbury Park, CA, USA, 1988; pp. 31–67. [Google Scholar]
- Sakhelashvili, I.; Eliozishvili, M.; Basishvili, T.; Datunashvili, M.; Oniani, N.; Cervena, K.; Darchia, N. Sleep-wake patterns and sleep quality in urban Georgia. Transl. Neurosci. 2016, 7, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Darchia, N.; Oniani, N.; Sakhelashvili, I.; Supatashvili, M.; Basishvili, T.; Eliozishvili, M.; Maisuradze, L.; Cervena, K. Relationship between Sleep Disorders and Health Related Quality of Life-Results from the Georgia SOMNUS Study. Int. J. Environ. Res. Public Health 2018, 15, 1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakhelashvili, I.; Eliozishvili, M.; Oniani, N.; Darchia, N.; Bruni, O. Sleep and psycho-behavioral problems in internally displaced children in Georgia. Sleep Med. 2018, 50, 42–47. [Google Scholar] [CrossRef]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef]
- Matricciani, L.; Bin, Y.S.; Lallukka, T.; Kronholm, E.; Dumuid, D.; Paquet, C.; Olds, T. Past, present, and future: Trends in sleep duration and implications for public health. Sleep Health 2017, 3, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Gregory, A.M.; Van der Ende, J.; Willis, T.A.; Verhulst, F.C. Parent-reported sleep problems during development and self-reported anxiety/depression, attention problems, and aggressive behavior later in life. Arch. Pediatr. Adolesc. Med. 2008, 162, 330–335. [Google Scholar] [CrossRef] [Green Version]
- Kohyama, J. Neural Basis of Brain Dysfunction Produced by Early Sleep Problems. Brain Sci. 2016, 6, 5. [Google Scholar] [CrossRef]
- Conte, F.; Cellini, N.; de Rosa, O.; Rescott, M.L.; Malloggi, S.; Giganti, F.; Ficca, G. Dissociated profiles of sleep timing and sleep quality changes across the first and second wave of the COVID-19 pandemic. J. Psychiatr. Res. 2021, 143, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, M.; Favieri, F.; Tambelli, R. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Lan, M.; Li, H.; Yang, J. Perceived stress and sleep quality among the non-diseased general public in China during the 2019 coronavirus disease: A moderated mediation model. Sleep Med. 2021, 77, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Akıncı, T.; Melek Başar, H. Relationship between sleep quality and the psychological status of patients hospitalised with COVID-19. Sleep Med. 2021, 80, 167–170. [Google Scholar] [CrossRef]
- Salfi, F.; Lauriola, M.; D’Atri, A.; Amicucci, G.; Viselli, L.; Tempesta, D.; Ferrara, M. Demogr aphic, psychological, chronobiological, and work-related predictors of sleep disturbances during the COVID-19 lockdown in Italy. Sci. Rep. 2021, 11, 11416. [Google Scholar] [CrossRef]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.; Nissen, C. The hyperarousal model of insomnia: A review of the concept and its evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef]
- Wuyts, J.; De Valck, E.; Vandekerckhove, M.; Pattyn, N.; Bulckaert, A.; Berckmans, D.; Haex, B.; Verbraecken, J.; Cluydts, R. The influence of pre-sleep cognitive arousal on sleep onset processes. Int. J. Psychophysiol. 2012, 83, 8–15. [Google Scholar] [CrossRef]
- Morin, C.M.; Rodrigue, S.; Ivers, H. Role of stress, arousal, and coping skills in primary insomnia. Psychosom. Med. 2003, 65, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Garde, A.H.; Albertsen, K.; Persson, R.; Hansen, A.M.; Rugulies, R. Bi-directional associations between psychological arousal, cortisol, and sleep. Behav. Sleep Med. 2011, 10, 28–40. [Google Scholar] [CrossRef]
- Salfi, F.; D’Atri, A.; Tempesta, D.; Ferrara, M. Sleeping under the waves: A longitudinal study across the contagion peaks of the COVID-19 pandemic in Italy. J. Sleep Res. 2021, 30, e13313. [Google Scholar] [CrossRef]
- Nadareishvili, I.; Syunyakov, T.; Smirnova, D.; Sinauridze, A.; Tskitishvili, A.; Tskitishvili, A.; Zhulina, A.; Patsali, M.E.; Manafis, A.; Fountoulakis, N.K.; et al. University students’ mental health amidst the COVID-19 pandemic in Georgia. Int. J. Soc. Psychiatry 2022, 5, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.J.; Wang, L.L.; Yang, R.; Yang, X.J.; Zhang, L.G.; Guo, Z.C.; Chen, J.C.; Wang, J.Q.; Chen, J.X. Sleep problems among Chinese adolescents and young adults during the coronavirus-2019 pandemic. Sleep Med. 2020, 74, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Rossell, S.L.; Neill, E.; Phillipou, A.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Meyer, D. An overview of current mental health in the general population of Australia during the COVID-19 pandemic: Results from the COLLATE project. Psychiatry Res. 2021, 296, 113660. [Google Scholar] [CrossRef] [PubMed]
- Varma, P.; Junge, M.; Meaklim, H.; Jackson, M.L. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Prog. Neuropsychopharmacol. Biol. Psychiatry. 2021, 109, 110236. [Google Scholar] [CrossRef] [PubMed]
- GEOSTAT. Information and Communication Technologies Usage in Households. Available online: https://www.geostat.ge/en/modules/categories/106/information-and-communication-technologies-usage-in-households (accessed on 20 October 2022).


{kind=link}
{kind=link}
| Total Sample n = 1117 | |
|---|---|
| Age | 38.50 ± 13.30 |
| Sex | |
| Male | 150 (13.4%) |
| Female | 967 (86.6%) |
| Marital status | |
| Married/cohabiting | 546 (48.9%) |
| Single/divorced/widowed | 571 (51.1%) |
| Education | |
| University degree | 902 (80.7%) |
| High school | 59 (5.3%) |
| Student | 156 (14.0%) |
| Employment | |
| Yes | 802 (71.8%) |
| No | 315 (28.2%) |
| Economic status | |
| Good | 213 (19.1%) |
| Average | 683 (61.1%) |
| Bad | 221 (19.8%) |
| Chronic disease | |
| Yes | 196 (17.5%) |
| No | 921 (82.5%) |
| Access to medical services | |
| Worse | 379 (33.9%) |
| No change | 718 (64.3%) |
| Better | 20 (1.8%) |
| Family environment | |
| Worse | 509 (45.6%) |
| No change | 570 (51.0%) |
| Better | 38 (3.4%) |
| PSQI global score | 7.19 ± 4.17 |
| PSAS-somatic | 14.62 ± 5.40 |
| PSAS-cognitive | 22.07 ± 7.28 |
| PSS-4 | 6.80 ± 2.95 |
| Anxiety | 3.41 ± 1.17 |
| Depression | 3.03 ± 1.33 |
| Social Isolation | 3.37 ± 1.19 |
| Predictors | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Age | 1.02 | 1.01–1.04 | 0.001 | 1.04 | 1.02–1.05 | 0.000 |
| Sex | ||||||
| Female | Reference | |||||
| Male | 0.68 | 0.45–1.03 | 0.069 | 0.66 | 0.42–1.03 | 0.067 |
| Marital status | ||||||
| Married/cohabiting | Reference | |||||
| Single/divorced/widowed | 1.14 | 0.85–1.53 | 0.392 | 1.14 | 0.81–1.59 | 0.446 |
| Education | ||||||
| University | Reference | |||||
| High school | 1.54 | 0.82–2.92 | 0.183 | 1.50 | 0.74–3.05 | 0.259 |
| Student | 1.85 | 1.09–3.15 | 0.022 | 1.47 | 0.79–2.74 | 0.227 |
| Employment | ||||||
| Employed | Reference | |||||
| Unemployed | 0.76 | 0.54–1.07 | 0.119 | 0.83 | 0.56–1.23 | 0.352 |
| Economic status | ||||||
| Good | Reference | |||||
| Average | 1.13 | 0.79–1.62 | 0.493 | 1.07 | 0.72–1.59 | 0.739 |
| Bad | 0.84 | 0.53–1.33 | 0.456 | 0.87 | 0.52–1.46 | 0.588 |
| Chronic disease | ||||||
| No | Reference | |||||
| Yes | 1.19 | 0.82–1.73 | 0.350 | 1.06 | 0.70–1.62 | 0.775 |
| COVID-19 infection | ||||||
| No | Reference | |||||
| Yes | 1.86 | 1.38–2.52 | 0.000 | 1.64 | 1.16–2.31 | 0.005 |
| Access to medical services | ||||||
| No change | Reference | |||||
| Worse | 1.29 | 0.96–1.74 | 0.095 | 1.24 | 0.88–1.74 | 0.213 |
| Better | 1.24 | 0.43–3.54 | 0.687 | 1.44 | 0.44–4.66 | 0.543 |
| Family environment | ||||||
| No change | Reference | |||||
| Worse | 1.34 | 0.99–1.80 | 0.053 | 1.45 | 1.03–2.03 | 0.032 |
| Better | 0.83 | 0.39–1.76 | 0.620 | 0.71 | 0.29–1.79 | 0.473 |
| Anxiety | 1.20 | 1.03–1.40 | 0.017 | 0.96 | 0.81–1.15 | 0.685 |
| Depression | 1.31 | 1.13–1.51 | 0.000 | 1.14 | 0.96–1.35 | 0.129 |
| Social isolation | 1.14 | 1.00–1.30 | 0.045 | 1.12 | 0.96–1.30 | 0.148 |
| PSS-4 | 1.25 | 1.18–1.33 | 0.000 | 1.12 | 1.05–1.20 | 0.001 |
| PSAS-somatic | 1.11 | 1.07–1.16 | 0.000 | |||
| PSAS-cognitive | 1.20 | 1.16–1.24 | 0.000 | |||
| Nagelkerke R2 | 0.286 | 0.490 | ||||
| Correct classification (%) | 71.5% | 77.7% | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsaava, M.; Oniani, N.; Eliozishvili, M.; Sakhelashvili, I.; Tkemaladze, N.; Aladashvili, T.; Basishvili, T.; Darchia, N. Age-Based Differences in Sleep Quality, Pre-Sleep Arousal, and Psychosocial Factors during the Second Wave Lockdown of the COVID-19 Pandemic in Georgia—A Higher Vulnerability of Younger People. Int. J. Environ. Res. Public Health 2022, 19, 16221. https://doi.org/10.3390/ijerph192316221
Tsaava M, Oniani N, Eliozishvili M, Sakhelashvili I, Tkemaladze N, Aladashvili T, Basishvili T, Darchia N. Age-Based Differences in Sleep Quality, Pre-Sleep Arousal, and Psychosocial Factors during the Second Wave Lockdown of the COVID-19 Pandemic in Georgia—A Higher Vulnerability of Younger People. International Journal of Environmental Research and Public Health. 2022; 19(23):16221. https://doi.org/10.3390/ijerph192316221
Chicago/Turabian StyleTsaava, Mariam, Nikoloz Oniani, Marine Eliozishvili, Irine Sakhelashvili, Nino Tkemaladze, Tamar Aladashvili, Tamar Basishvili, and Nato Darchia. 2022. "Age-Based Differences in Sleep Quality, Pre-Sleep Arousal, and Psychosocial Factors during the Second Wave Lockdown of the COVID-19 Pandemic in Georgia—A Higher Vulnerability of Younger People" International Journal of Environmental Research and Public Health 19, no. 23: 16221. https://doi.org/10.3390/ijerph192316221
APA StyleTsaava, M., Oniani, N., Eliozishvili, M., Sakhelashvili, I., Tkemaladze, N., Aladashvili, T., Basishvili, T., & Darchia, N. (2022). Age-Based Differences in Sleep Quality, Pre-Sleep Arousal, and Psychosocial Factors during the Second Wave Lockdown of the COVID-19 Pandemic in Georgia—A Higher Vulnerability of Younger People. International Journal of Environmental Research and Public Health, 19(23), 16221. https://doi.org/10.3390/ijerph192316221