
Global, Regional, and National Burden of Road Injuries from 1990 to 2019


Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview and Definition
2.2. Socio-Demographic Index
2.3. Data Sources
2.4. Statistical Analyses
3. Results
3.1. Incidence of RIs Increased Globally from 1990 to 2019
3.2. Death of RIs Decreased from 1990 to 2019 Globally
3.3. Age-Standardized DALYs attributable to RIs Decreased from 1990 to 2019 Globally
3.4. Correlation between SDI Index and EAPC
3.5. The Features of RIs in Different Age Groups
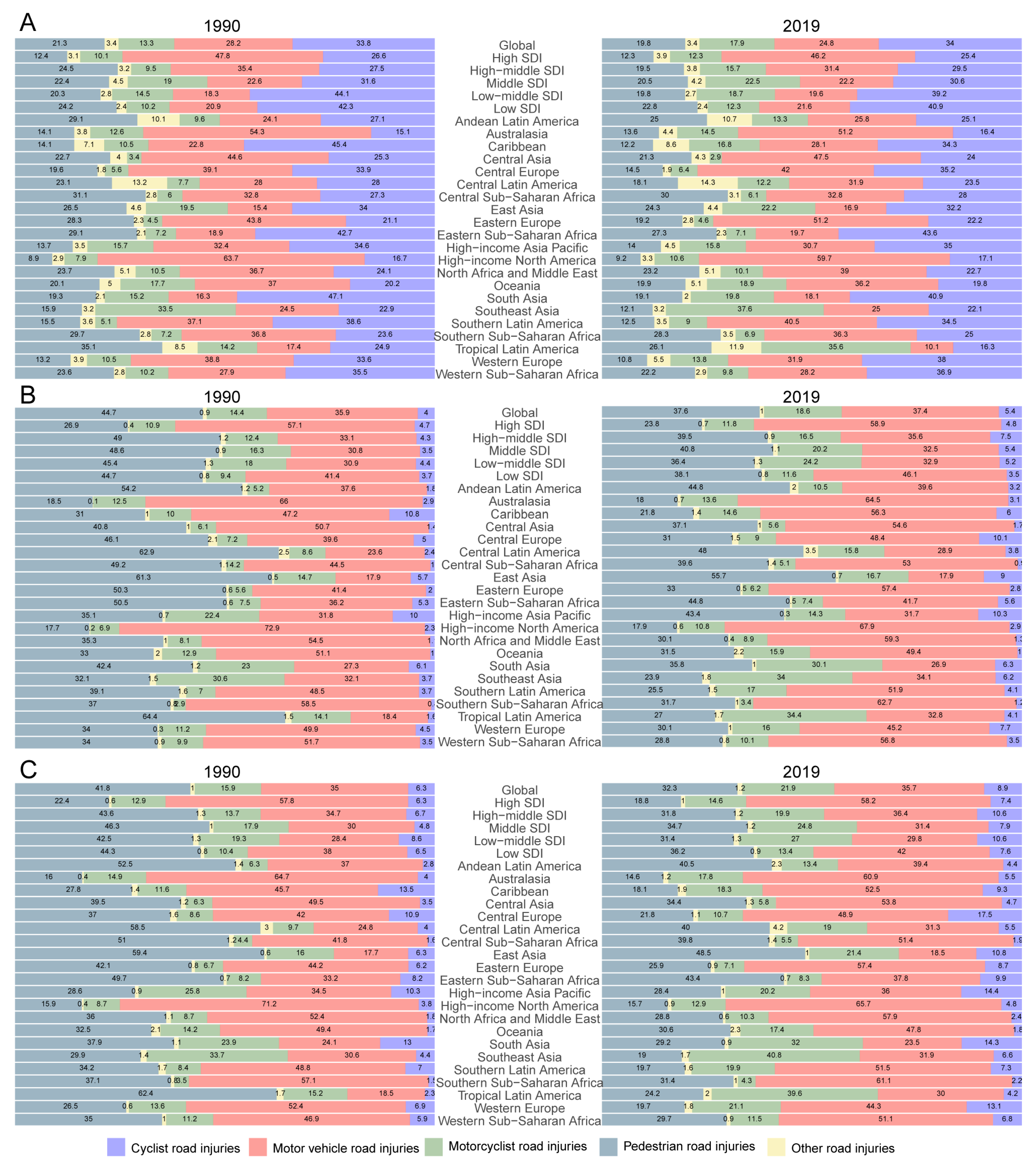
3.6. The Proportion of Five Different Subgroups of Road Injuries
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lancet, T. Road safety: More than reducing injuries. Lancet 2022, 400, 73. [Google Scholar] [CrossRef] [PubMed]
- Hyder, A.A.; Hoe, C.; Hijar, M.; Peden, M. The political and social contexts of global road safety: Challenges for the next decade. Lancet 2022, 400, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Vecino-Ortiz, A.I.; Nagarajan, M.; Elaraby, S.; Guzman-Tordecilla, D.N.; Paichadze, N.; Hyder, A.A. Saving lives through road safety risk factor interventions: Global and national estimates. Lancet 2022, 400, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Beck, B.; Cameron, P.A.; Fitzgerald, M.C.; Judson, R.T.; Teague, W.; Lyons, R.A.; Gabbe, B.J. Road safety: Serious injuries remain a major unsolved problem. Med. J. Aust. 2017, 207, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Chong, S.L.; Tyebally, A.; Chew, S.Y.; Lim, Y.C.; Feng, X.Y.; Chin, S.T.; Lee, L.K. Road traffic injuries among children and adolescents in Singapore—Who is at greatest risk? Accid. Anal. Prev. 2017, 100, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Symons, J.; Howard, E.; Sweeny, K.; Kumnick, M.; Sheehan, P. Reduced Road Traffic Injuries for Young People: A Preliminary Investment Analysis. J. Adolesc. Health 2019, 65, S34–s43. [Google Scholar] [CrossRef]
- Ang, B.H.; Chen, W.S.; Lee, S.W.H. Global burden of road traffic accidents in older adults: A systematic review and meta-regression analysis. Arch. Gerontol. Geriatr. 2017, 72, 32–38. [Google Scholar] [CrossRef]
- Rissanen, R.; Berg, H.Y.; Hasselberg, M. Quality of life following road traffic injury: A systematic literature review. Accid. Anal. Prev. 2017, 108, 308–320. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, X.; Liao, K.; Luo, B.; Luo, J. The burden of endometriosis in China from 1990 to 2019. Front. Endocrinol. 2022, 13, 935931. [Google Scholar] [CrossRef]
- Rosen, H.E.; Bari, I.; Paichadze, N.; Peden, M.; Khayesi, M.; Monclús, J.; Hyder, A.A. Global road safety 2010–18: An analysis of Global Status Reports. Injury 2022, S0020, 1383. [Google Scholar] [CrossRef]
- Adeloye, D.; Thompson, J.Y.; Akanbi, M.A.; Azuh, D.; Samuel, V.; Omoregbe, N.; Ayo, C.K. The burden of road traffic crashes, injuries and deaths in Africa: A systematic review and meta-analysis. Bull. World Health Organ. 2016, 94, 510–521a. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Eastern Mediterranean Region Transportation Injuries Collaborators. Transport injuries and deaths in the Eastern Mediterranean Region: Findings from the Global Burden of Disease 2015 Study. Int. J. Public Health 2018, 63, 187–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passmore, J.; Yon, Y.; Mikkelsen, B. Progress in reducing road-traffic injuries in the WHO European region. Lancet Public Health 2019, 4, e272–e273. [Google Scholar] [CrossRef] [Green Version]
- Alghnam, S.; Alkelya, M.; Aldahnim, M.; Aljerian, N.; Albabtain, I.; Alsayari, A.; Da’ar, O.B.; Alsheikh, K.; Alghamdi, A. Healthcare costs of road injuries in Saudi Arabia: A quantile regression analysis. Accid. Anal. Prev. 2021, 159, 106266. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, R.; Nosratnejad, S.; Sadeghi-Bazargani, H.; Dalal, K.; Yousefi, M. The economic burden of road traffic injuries until one-year after hospitalization: A survey study. Accid. Anal. Prev. 2021, 163, 106459. [Google Scholar] [CrossRef]
- Alemany, R.; Ayuso, M.; Guillén, M. Impact of road traffic injuries on disability rates and long-term care costs in Spain. Accid. Anal. Prev. 2013, 60, 95–102. [Google Scholar] [CrossRef]
- Tan, H.; Zhao, F.; Hao, H.; Liu, Z. Cost analysis of road traffic crashes in China. Int. J. Inj. Control Saf. Promot. 2020, 27, 385–391. [Google Scholar] [CrossRef]
- Ainy, E.; Soori, H.; Ganjali, M.; Le, H.; Baghfalaki, T. Estimating cost of road traffic injuries in Iran using willingness to pay (WTP) method. PLoS ONE 2014, 9, e112721. [Google Scholar] [CrossRef] [Green Version]
- Banstola, A.; Kigozi, J.; Barton, P.; Mytton, J. Economic Burden of Road Traffic Injuries in Nepal. Int. J. Environ. Res. Public Health 2020, 17, 4571. [Google Scholar] [CrossRef]
- Gu, J.; Fei, G.; Meng, Y.; Sun, Q.; Qian, Y.; Jiang, X.; Wang, X.; Stallones, L.; Xiang, H.; Zhang, X. Revised road traffic safety law and years of life lost due to traffic deaths in China, 2002–2019. Accid. Anal. Prev. 2021, 161, 106344. [Google Scholar] [CrossRef]
- James, S.L.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; NL, S.R.; Sylte, D.O.; Henry, N.J.; LeGrand, K.E.; et al. Global injury morbidity and mortality from 1990 to 2017: Results from the Global Burden of Disease Study 2017. Inj. Prev. 2020, 26, i96–i114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, F.R.; Antunes, J.L.F. Trends in the number of traffic accident victims on Brazil’s federal highways before and after the start of the Decade of Action for Road Safety. Cad. Saúde Pública 2019, 35, e00250218. [Google Scholar] [CrossRef]
- Rapoport, M.J.; Chee, J.N.; Aljenabi, N.; Byrne, P.A.; Naglie, G.; Ilari, F.; Elzohairy, Y.; Vingilis, E.; Mulsant, B.H. Impact of COVID-19 on motor vehicle injuries and fatalities in older adults in Ontario, Canada. Accid. Anal. Prev. 2021, 157, 106195. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Xiang, H.; Jing, R.; Tu, Z. Road traffic injuries in the People’s Republic of China, 1951–2008. Traffic Inj. Prev. 2011, 12, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Mortality due to road injuries in the states of India: The Global Burden of Disease Study 1990–2017. Lancet Public Health 2020, 5, e86–e98. [CrossRef] [Green Version]
- Chisholm, D.; Naci, H.; Hyder, A.A.; Tran, N.T.; Peden, M. Cost effectiveness of strategies to combat road traffic injuries in sub-Saharan Africa and South East Asia: Mathematical modelling study. BMJ 2012, 344, e612. [Google Scholar] [CrossRef] [Green Version]
- James, S.L.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; Roberts, N.L.S.; Sylte, D.O.; Bertolacci, G.J.; Cunningham, M.; et al. Estimating global injuries morbidity and mortality: Methods and data used in the Global Burden of Disease 2017 study. Inj. Prev. 2020, 26, i125–i153. [Google Scholar] [CrossRef]
- Jin, X.; Ren, J.; Li, R.; Gao, Y.; Zhang, H.; Li, J.; Zhang, J.; Wang, X.; Wang, G. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. EClinicalMedicine 2021, 37, 100986. [Google Scholar] [CrossRef]
- Chen, L.; Wang, L.; Wang, Y.; Hu, H.; Zhan, Y.; Zeng, Z.; Liu, L. Global, Regional, and National Burden and Trends of Down Syndrome From 1990 to 2019. Front. Genet. 2022, 13, 908482. [Google Scholar] [CrossRef]
- Xue, Y.; Zhou, J.; Wang, P.; Lan, J.H.; Lian, W.Q.; Fan, Y.Y.; Xu, B.N.; Yin, J.P.; Feng, Z.H.; Zhou, J.; et al. Burden of tuberculosis and its association with socio-economic development status in 204 countries and territories, 1990–2019. Front. Med. 2022, 9, 905245. [Google Scholar] [CrossRef]
- Xue, Y.; Zhou, J.; Xu, B.N.; Li, Y.; Bao, W.; Cheng, X.L.; He, Y.; Xu, C.P.; Ren, J.; Zheng, Y.R.; et al. Global Burden of Bacterial Skin Diseases: A Systematic Analysis Combined With Sociodemographic Index, 1990–2019. Front. Med. 2022, 9, 861115. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.R.; Stevenson, D.; Fryback, D.G. HALYS and QALYS and DALYS, Oh My: Similarities and differences in summary measures of population Health. Annu. Rev. Public Health 2002, 23, 115–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estimates, trends, and drivers of the global burden of type 2 diabetes attributable to PM(2·5) air pollution, 1990–2019: An analysis of data from the Global Burden of Disease Study 2019. Lancet Planet. Health 2022, 6, e586–e600. [CrossRef] [PubMed]
- Behera, D.K.; Singh, S.K.; Choudhury, D.K. The burden of transport injury and risk factors in India from 1990 to 2019: Evidence from the global burden of disease study. Arch. Public Health 2022, 80, 204. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Ferguson, R.W.; Henderson, S.J.; Jung, P. Road traffic injuries in Peace Corps Volunteers, 1996–2014. Inj. Prev. 2017, 23, 75–80. [Google Scholar] [CrossRef]
- Pérez-Núñez, R.; Hidalgo-Solórzano, E.; Híjar, M. Impact of Mexican Road Safety Strategies implemented in the context of the UN’s Decade of Action. Accid. Anal. Prev. 2021, 159, 106227. [Google Scholar] [CrossRef]
- Morgan, A.; Mannering, F.L. The effects of road-surface conditions, age, and gender on driver-injury severities. Accid. Anal. Prev. 2011, 43, 1852–1863. [Google Scholar] [CrossRef]
- Ichikawa, M.; Inada, H.; Nakahara, S. Increased traffic injuries among older unprotected road users following the introduction of an age-based cognitive test to the driver’s license renewal procedure in Japan. Accid. Anal. Prev. 2020, 136, 105440. [Google Scholar] [CrossRef]
- Al Saad, N.A.; Sondorp, E. Road traffic injuries in Iraq. Lancet 2013, 381, 1720. [Google Scholar] [CrossRef]
- Rissanen, R.; Ifver, J.; Hasselberg, M.; Berg, H.Y. Quality of life following road traffic injury: The impact of age and gender. Qual. Life Res. 2020, 29, 1587–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengoelge, M.; Laflamme, L.; El-Khatib, Z. Ecological study of road traffic injuries in the eastern Mediterranean region: Country economic level, road user category and gender perspectives. BMC Public Health 2018, 18, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mateos-Granados, J.; Martín-delosReyes, L.M.; Rivera-Izquierdo, M.; Jiménez-Mejías, E.; Martínez-Ruiz, V.; Lardelli-Claret, P. Sex Differences in the Amount and Patterns of Car-Driving Exposure in Spain, 2014 to 2017: An Application of a Quasi-Induced Exposure Approach. Int. J. Environ. Res. Public Health 2021, 18, 13255. [Google Scholar] [CrossRef] [PubMed]
- Gwyther, H.; Holland, C. The effect of age, gender and attitudes on self-regulation in driving. Accid. Anal. Prev. 2012, 45, 19–28. [Google Scholar] [CrossRef]
- Rhodes, N.; Pivik, K. Age and gender differences in risky driving: The roles of positive affect and risk perception. Accid. Anal. Prev. 2011, 43, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Leveau, C.M.; Tapia Granados, J.A.; Dos Santos, M.I.; Castillo-Riquelme, M.; Alazraqui, M. Are Wealthier Times Healthier in Cities? Economic Fluctuations and Mortality in Urban Areas of Latin America. Int. J. Public Health 2021, 66, 1604318. [Google Scholar] [CrossRef] [PubMed]
- Ning, P.; Zong, H.; Li, L.; Cheng, P.; Schwebel, D.C.; Yang, Y.; Yang, L.; Wu, Y.; Zhao, M.; Hu, G. Effectiveness of a helmet promotion campaign, China. Bull. World Health Organ. 2022, 100, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chu, Y.; Yeung, D.; Wang, W.; Wang, L.; Yin, P.; Liu, J.; Zhou, M.; Liu, L. National and sub-national levels and causes of mortality among 5–19-year-olds in China in 2004–2019: A systematic analysis of evidence from the Disease Surveillance Points System. J. Glob. Health 2022, 12, 11008. [Google Scholar] [CrossRef]
- Flaherty, M.R.; Raybould, T.; Kelleher, C.M.; Seethala, R.; Lee, J.; Kaafarani, H.M.A.; Masiakos, P.T. Age Legislation and Off-Road Vehicle Injuries in Children. Pediatrics 2017, 140, e20171164. [Google Scholar] [CrossRef] [Green Version]
- Kwan, I.; Mapstone, J.; Roberts, I. Interventions for increasing pedestrian and cyclist visibility for the prevention of death and injuries. Cochrane Database Syst. Rev. 2002, 2, Cd003438. [Google Scholar] [CrossRef]
- Sauber-Schatz, E.K.; Ederer, D.J.; Dellinger, A.M.; Baldwin, G.T. Vital Signs: Motor Vehicle Injury Prevention—United States and 19 Comparison Countries. MMWR Morb. Mortal. Wkly Rep. 2016, 65, 672–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanthosh, J.; Rogers, K.; Lung, T.; Brown, J.; Ivers, R.; Wilson, A.; Jan, S. Effectiveness of child restraint legislation to reduce motor vehicle related serious injuries and fatalities: A national interrupted time series analysis. Accid. Anal. Prev. 2020, 142, 105553. [Google Scholar] [CrossRef] [PubMed]
- Abdi, N.; Robertson, T.; Petrucka, P.; Crizzle, A.M. Do motorcycle helmets reduce road traffic injuries, hospitalizations and mortalities in low and lower-middle income countries in Africa? A systematic review and meta-analysis. BMC Public Health 2022, 22, 824. [Google Scholar] [CrossRef] [PubMed]
- Chikritzhs, T.; Livingston, M. Alcohol and the Risk of Injury. Nutrients 2021, 13, 2777. [Google Scholar] [CrossRef]
- Simmons, S.M.; Caird, J.K.; Sterzer, F.; Asbridge, M. The effects of cannabis and alcohol on driving performance and driver behaviour: A systematic review and meta-analysis. Addiction 2022, 117, 1843–1856. [Google Scholar] [CrossRef]
- Paudel, M.; Yap, F.F.; Rosli, T.B.M.; Tan, K.H.; Xu, H.; Vahdati, N.; Butt, H.; Shiryayev, O. A computational study on the basis for a safe speed limit for bicycles on shared paths considering the severity of pedestrian head injuries in bicyclist-pedestrian collisions. Accid. Anal. Prev. 2022, 176, 106792. [Google Scholar] [CrossRef]
- Ling, R.; Rothman, L.; Cloutier, M.S.; Macarthur, C.; Howard, A. Cyclist-motor vehicle collisions before and after implementation of cycle tracks in Toronto, Canada. Accid. Anal. Prev. 2020, 135, 105360. [Google Scholar] [CrossRef]
- Tait, C.; Beecham, R.; Lovelace, R.; Barber, S. Contraflows and cycling safety: Evidence from 22 years of data involving 508 one-way streets. Accid. Anal. Prev. 2022, 179, 106895. [Google Scholar] [CrossRef]
- Beyer, F.R.; Ker, K. Street lighting for preventing road traffic injuries. Cochrane Database Syst. Rev. 2009, 1, Cd004728. [Google Scholar] [CrossRef] [Green Version]
- Marchant, P.; Hale, J.D.; Sadler, J.P. Does changing to brighter road lighting improve road safety? Multilevel longitudinal analysis of road traffic collision frequency during the relighting of a UK city. J. Epidemiol. Community Health 2020, 74, 467–472. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1990 | 2019 | 1990–2019 | |||
|---|---|---|---|---|---|
| Incidence Cases No. ×102(95%UI) | ASIR per 100,000 No. (95%UI) | Incidence Cases No. ×102(95%UI) | ASIR per 100,000 No. (95%UI) | EAPC No. (95%CI) | |
| Global | 632,111.48 [534,279.84–738,477.05] | 1,192.7 [1,017.76–1,389.27] | 1,032,196 [868,741.7–1,212,732.78] | 1,298.55 [1,092.23–1,529.42] | 0.4 [0.26 to 0.55] |
| Gender | |||||
| Female | 227,723 [193,850.64–266,947.98] | 872.97 [750.27–1,016.94] | 355,983.71 [302,250.53–417,143.88] | 896.32 [759.59–1,050.35] | 0.11 [0 to 0.21] |
| Male | 404,388.49 [338,821.93–472,587.08] | 1,507.91 [1,285.08–1,755.44] | 676,212.28 [567,121.62–796,660.96] | 1,697 [1,418.87–1,996.22] | 0.57 [0.39 to 0.74] |
| SDI region | |||||
| High SDI | 83,420.3 [73,261.69–94,943.33] | 1,002.16 [879.75–1,145.59] | 74,520.51 [64,333.9–86,089.78] | 739.88 [629.42–865.09] | −1.37 [−1.47 to −1.27] |
| High-middle SDI | 172,153.71 [145,735.49–201,179.03] | 1,451.94 [1,237.87–1,693.16] | 198,445.66 [168,498.82–233,544.11] | 1,301.8 [1,095.24–1,533.14] | −0.19 [−0.33 to −0.05] |
| Middle SDI | 163,427.1 [136,804.4–192,338.55] | 958.7 [812.76–1,115.91] | 302,824.2 [256,388.68–355,815] | 1,200.4 [1,020.29–1,408.07] | 0.99 [0.83 to 1.15] |
| Low-middle SDI | 150,368.13 [124,535.41–178,961.84] | 1,443.53 [1,216.45–1,694.36] | 311,099.29 [258,062.91–370,624.82] | 1,752.61 [1,464.86–2,079.37] | 0.73 [0.46 to 1.01] |
| Low SDI | 62,463.85 [52,539.49–73,608.15] | 1,386.14 [1,191.35–1,604.27] | 144,936.04 [120,963.11–171,604] | 1,473.35 [1,263.76–1,711.09] | 0.29 [0.16 to 0.41] |
| GBD region | |||||
| Andean Latin America | 2,142.89 [1,842.92–2,490.35] | 563.9 [494.76–640.38] | 3,389.42 [2,948.02–3,918.23] | 528.33 [461.67–607.85] | −0.15 [−0.22 to −0.08] |
| Australasia | 1,775.7 [1,587.67–1,991.45] | 860.83 [766.98–968.86] | 1,692 [1,502.5–1,894.93] | 602.97 [528.45–682.65] | −1.59 [−1.74 to −1.45] |
| Caribbean | 3,759.52 [3,265.35–4,263.76] | 1,023.9 [895.9–1,149.68] | 4,178.09 [3,600.9–4,805.63] | 876.96 [755.05–1,011.48] | −0.6 [−0.69 to −0.52] |
| Central Asia | 7,724.6 [6,807.15–8,730.75] | 1,130.78 [1,004.87–1,270.77] | 10,033.69 [8,702.93–11,393.91] | 1,044.48 [909.34–1,184.87] | 0.14 [−0.18 to 0.47] |
| Central Europe | 30,977.29 [27,246.53–34,999.4] | 2,512.34 [2,200.15–2,836.12] | 20,351.62 [17,811.08–23,152.95] | 1,901.41 [1,632.18–2,194.28] | −0.85 [−0.9 to −0.81] |
| Central Latin America | 19,490.57 [16,872.57–22,881.13] | 1,170.11 [1,028.29–1,331.16] | 23,804.54 [20,537.54–27,381.97] | 939.89 [811.76–1,080.33] | 0.97 [0.33 to 1.62] |
| Central sub-Saharan Africa | 5,244.46 [4,430.16–6,209.81] | 1,063.55 [921.06–1,222.63] | 11,620.96 [9774.84–13,635.69] | 982.99 [844.21–1,127.36] | −0.25 [−0.35 to −0.16] |
| East Asia | 66,252.68 [55,395.21–79,014.95] | 535.26 [450.72–630.33] | 165,348.28 [140,454.57–195,050.6] | 981.68 [834.63–1,151.85] | 2.28 [2.12 to 2.45] |
| Eastern Europe | 80,751.81 [67,297.17–96,218.08] | 3,472.2 [2,884.07–4,151.44] | 54,906.65 [45,310.1–65,704.95] | 2,600.36 [2,123.05–3,142.83] | −0.74 [−0.93 to −0.56] |
| Eastern sub-Saharan Africa | 22,790.29 [19,383.17–27,061.2] | 1,423.41 [1,243.35–1,630.04] | 44,563.76 [37,677.55–52,692.72] | 1,246.46 [1,085.85–1,425.4] | −0.53 [−0.59 to −0.47] |
| High-income Asia Pacific | 15,449.57 [13,467.61–17,857.37] | 850.09 [739.36–980.16] | 8,908.91 [7,646.85–10,369.65] | 473.34 [397.64–566.77] | −2.53 [−2.71 to −2.35] |
| High-income North America | 31,454.02 [26,222.4–37,432.42] | 1,101.94 [917.37–1,322.72] | 33,623.21 [28,261.27–39,729.03] | 904.78 [746.11–1,084.43] | −1.08 [−1.23 to −0.93] |
| North Africa and Middle East | 31847.22 [27275.74–37739.36] | 939.35 [818.92–1,077.33] | 47,396.43 [40,723.74–54,593.42] | 768.97 [667.85–880.58] | −0.68 [−0.71 to −0.66] |
| Oceania | 399.74 [336.7–464.14] | 684.75 [589.31–783] | 859.61 [729.26–993.93] | 688.42 [592.23–789.11] | −0.06 [−0.13 to 0.02] |
| South Asia | 190,939.53 [156,205.16–230,241.28] | 1,894 [1,577.63–2,252.26] | 435,654.1 [356,932.82–524,541.88] | 2,370.89 [1,954.52–2,843.26] | 0.87 [0.47 to 1.27] |
| Southeast Asia | 48,033.54 [40,763.7–56,349.51] | 1,040.34 [898.56–1,196.41] | 64,886.26 [56,005.63–74,700.39] | 924.25 [800.78–1,065.94] | −0.61 [−0.69 to −0.52] |
| Southern Latin America | 3,648.36 [3,180.23–4,137.28] | 729.78 [637.51–824.49] | 5,342.3 [4,589.81–6,193.28] | 795.91 [681.36–923.04] | 0.23 [0.18 to 0.29] |
| Southern sub-Saharan Africa | 4,846.08 [3,955.63–5,848.59] | 1,045.54 [877.96–1,244.39] | 6,510.67 [5,391.37–7,818.8] | 859.26 [721.53–1,029.01] | 0.15 [−0.34 to 0.63] |
| Tropical Latin America | 12,035.92 [9,918.84–14,511.47] | 777.18 [654.29–920.91] | 17,635.05 [14,706.66–20,862.07] | 764.07 [638.5–904.25] | 0.25 [−0.03 to 0.54] |
| Western Europe | 33,159.89 [29,235.18–36,893.92] | 883.04 [769.89–992.81] | 20,486.47 [17,899.47–23,393.64] | 522.36 [446.51–612.42] | −2.24 [−2.4 to −2.07] |
| Western sub-Saharan Africa | 19,387.8 [16,599.37–22,443.2] | 1,237.86 [1,080.4–1,413.6] | 51,003.99 [43,080.08–59,410.26] | 1,366.64 [1,189.24–1,563.32] | 0.51 [0.42 to 0.6] |
| 1990 | 2019 | 1990–2019 | |||
|---|---|---|---|---|---|
| Deaths Cases No. ×102 (95% UI) | ASDR per 100,000 No. (95% UI) | Deaths Cases No. ×102 (95% UI) | ASDR per 100,000 No.(95% UI) | EAPC No. (95% CI) | |
| Overall | 11,134.11 [10,470.07–12,096.11] | 21.92 [20.65–23.86] | 11,982.89 [10,600.41–13,048.31] | 14.99 [13.29–16.32] | −1.29 [−1.44 to −1.14] |
| Gender | |||||
| Female | 3,049.17 [2,841.52–3,274.21] | 11.92 [11.16–12.71] | 2,976.31 [2,709.96–3,265.94] | 7.36 [6.7–8.06] | −1.73 [−1.88 to −1.58] |
| Male | 8,084.94 [7,565.01–9,072.09] | 32.23 [30.14–36.22] | 9,006.59 [7,639.42–9,906.22] | 22.79 [19.37–25.11] | −1.14 [−1.29 to −0.98] |
| SDI region | |||||
| High SDI | 1,518.09 [1,488.69–1,546.7] | 17.37 [17.04–17.7] | 1,095.11 [1,017.34–1,184.18] | 9.26 [8.59–10.08] | −2.47 [−2.61 to −2.33] |
| High-middle SDI | 2,373.83 [2,247.55–2,646.26] | 20.53 [19.43–22.87] | 1,970.78 [1,762.01–2,152.88] | 11.96 [10.77–12.98] | −1.91 [−2.21 to −1.6] |
| Middle SDI | 4,120.39 [3,838.79–4,590.16] | 26.25 [24.42–29.36] | 4,380.76 [3,820.35–4,807.44] | 17.45 [15.32–19.13] | −1.28 [−1.48 to −1.08] |
| Low-middle SDI | 2,018.53 [1,835.67–2,255.58] | 21.11 [19.25–23.4] | 2,837.15 [2,419.48–3,162.24] | 17.24 [14.69–19.14] | −0.67 [−0.79 to −0.54] |
| Low SDI | 1,096.89 [918.07–1,274.98] | 25.47 [21.84–28.65] | 1,691.9 [1,403.31–2,013.27] | 19.9 [16.76–23.22] | −0.85 [−0.95 to −0.76] |
| GBD Region | |||||
| Andean Latin America | 81.79 [73.62–94.25] | 25.42 [22.98–29.47] | 115.79 [91.79–140.56] | 18.75 [14.9–22.81] | −0.88 [−1.07 to −0.7] |
| Australasia | 35.18 [34.44–35.9] | 16.62 [16.28–16.98] | 19.47 [18.32–20.46] | 5.98 [5.63–6.29] | −3.58 [−3.73 to −3.43] |
| Caribbean | 68.41 [64.58–80.02] | 20.3 [19.2–23.9] | 66.35 [53.73–84.29] | 13.57 [10.98–17.25] | −1.41 [−1.6 to −1.22] |
| Central Asia | 127.7 [122.81–131.32] | 20.09 [19.3–20.65] | 120.93 [108.15–134.95] | 13.01 [11.66–14.5] | −0.8 [−1.27 to −0.32] |
| Central Europe | 232.91 [228.21–236.83] | 18.07 [17.7–18.39] | 107 [94.45–120.43] | 7.9 [6.96–8.88] | −3.24 [−3.42 to −3.07] |
| Central Latin America | 372.98 [364.83–381.36] | 27.39 [26.83–27.91] | 420.7 [354.32–495.29] | 16.65 [14.05–19.57] | −1.77 [−1.91 to −1.64] |
| Central sub-Saharan Africa | 281.53 [215.46–346.69] | 54.83 [42.8–70.26] | 441.62 [313.2–588.97] | 41.92 [30.06–58.49] | −0.92 [−1.06 to −0.78] |
| East Asia | 2449.17 [2101.38–3338.81] | 20.8 [17.87–28.52] | 2,623.12 [2,172.69–3,064.37] | 15 [12.56–17.34] | −0.76 [−1.21 to −0.3] |
| Eastern Europe | 577.47 [565.32–610.37] | 24.3 [23.79–25.65] | 297.9 [264.95–337.88] | 13.3 [11.87–14.96] | −2.48 [−2.92 to −2.03] |
| Eastern sub-Saharan Africa | 346.88 [290.37–406.11] | 26.54 [22.88–30.27] | 477.12 [402.84–564.32] | 18.71 [16.04–21.57] | −1.31 [−1.38 to −1.24] |
| High-income Asia Pacific | 309.48 [296.39–319.04] | 16.81 [16.11–17.36] | 139.52 [127.41–157.78] | 4.82 [4.49–5.67] | −5.19 [−5.48 to −4.9] |
| High-income North America | 532.58 [525.27–540.25] | 18.06 [17.82–18.31] | 438.44 [418.7–450.69] | 10.61 [10.09–10.91] | −1.98 [−2.19 to −1.77] |
| North Africa and Middle East | 1,304.29 [1,055.64–1,451.78] | 42.97 [33.96–47.32] | 1,489.91 [1,194.03–1,747.5] | 26.3 [21.04–30.75] | −1.71 [−1.73 to −1.68] |
| Oceania | 15.05 [12.17–18.62] | 27.33 [22.33–33.73] | 28.14 [21.79–37.03] | 23.93 [18.78–30.95] | −0.4 [−0.45 to −0.35] |
| South Asia | 1,477.65 [1,295.62–1,639.38] | 16.6 [14.45–18.38] | 2,427.2 [1,904.6–2,820.79] | 14.43 [11.36–16.75] | −0.5 [−0.68 to −0.32] |
| Southeast Asia | 1,178.15 [1,032.07–1,292.54] | 27.89 [24.8–30.28] | 1,128 [957.71–1,324.94] | 16.75 [14.27–19.7] | −1.97 [−2.08 to −1.85] |
| Southern Latin America | 69.81 [68.07–71.49] | 14.48 [14.12–14.82] | 91.77 [86.97–96.36] | 12.65 [11.98–13.28] | −0.49 [−0.65 to −0.34] |
| Southern sub-Saharan Africa | 223.49 [184.66–243.76] | 49.87 [41.1–54.86] | 242.62 [205.36–274.05] | 32 [27.6–35.81] | −1.85 [−2.25 to −1.46] |
| Tropical Latin America | 447.43 [431.67–462.95] | 32.92 [31.75–34.07] | 460.3 [437.94–479.79] | 19.21 [18.25–20.06] | −1.56 [−1.72 to −1.39] |
| Western Europe | 671.01 [661.41–679.04] | 15.9 [15.69–16.1] | 261.47 [249.56–270.94] | 4.9 [4.71–5.07] | −4.69 [−4.96 to −4.43] |
| Western sub-Saharan Africa | 331.15 [274.4–389.7] | 21.44 [18.28–24.9] | 585.5 [466.55–718.11] | 17.9 [14.58–21.49] | −0.53 [−0.62 to −0.44] |
| 1990 | 2019 | 1990–2019 | |||
|---|---|---|---|---|---|
| DALYs No. ×102 (95% UI) | Age-Standardized DALYs No. (95% UI) | DALYs No. ×102 (95% UI) | Age-Standardized DALYs No.(95% UI) | EAPC No. (95% CI) | |
| Global | 712,122.4 [664,087.2–770,347.5] | 1,329.47 [1,235.48–1,435.89] | 729,013.26 [648,308.81–801,937.02] | 917.94 [814.15–1,011.37] | −1.26 [−1.4 to −1.13] |
| Gender | |||||
| Female | 208,098.7 [190,562.05–228,247.96] | 780.8 [714.59–856.57] | 193,677.15 [172,363.89–215,808.81] | 489.05 [437.25–543.19] | −1.69 [−1.81 to −1.57] |
| Male | 504,023.7 [467,699.93–557,320.25] | 1,874.15 [1,733.5–2,062.01] | 535,336.11 [463,562.97–586,867.1] | 1,345.5 [1,166.1–1,474.81] | −1.09 [−1.24 to −0.94] |
| SDI region | |||||
| High SDI | 88,858.35 [84,488.89–93,738.76] | 1,059.2 [1,011.15–1,111.18] | 60,335.63 [54,810.99–66,720.78] | 562.11 [515.83–617.59] | −2.48 [−2.61 to −2.34] |
| High-middle SDI | 150,385.15 [139,162.78–163,847.98] | 1,283.56 [1,186.67–1,397.77] | 120,707.72 [107,606.11–134,968.91] | 763.36 [684.32–843.56] | −1.84 [−2.06 to −1.61] |
| Middle SDI | 259579.77 [241133.39–283157.94] | 1,502.58 [1,397.76–1,641.83] | 248,621.98 [220,698.37–27,3031.33] | 987.99 [880.75–1081.77] | −1.36 [−1.52 to −1.2] |
| Low-middle SDI | 137,322.64 [124,626.91–152,489.3] | 1,294.6 [1,171.71–1,430.64] | 185,509.65 [162,145.8–207,601.08] | 1,080.25 [943.53–1,209.33] | −0.59 [−0.76 to −0.43] |
| Low SDI | 75,574.85 [62,708.46–89,015.91] | 1,466.02 [1,258.01–1,680.21] | 113,421.72 [95,173.88–134,008.85] | 1,152.15 [977.14–1,331.52] | −0.8 [−0.9 to −0.71] |
| GBD region | |||||
| Andean Latin America | 4,902.6 [4,396.78–5,555.77] | 1,318.98 [1,192.05–1,505.37] | 5,911.77 [4,806.04–7,089.41] | 924.08 [751.11–1,106.73] | −1.09 [−1.28 to −0.9] |
| Australasia | 2,132.23 [2,044.31–2,233.02] | 1,029.38 [989.2–1,076.27] | 1,156.5 [1,052.18–1,275.7] | 387.26 [356.49–421.88] | −3.47 [−3.61 to −3.32] |
| Caribbean | 4,316.62 [4,008.51–4,947.11] | 1,215.42 [1,126.47–1,398.7] | 3,934.24 [3,259–4,910.97] | 817.37 [674.97–1,022.45] | −1.38 [−1.54 to −1.21] |
| Central Asia | 8,090.8 [7,689.82–8,493.97] | 1,206.66 [1,142.55–1,274.85] | 7,489.92 [6,679.93–8,312.15] | 782.8 [697.12–869.95] | −0.87 [−1.3 to −0.44] |
| Central Europe | 16,346.65 [14,831.85–18,109.27] | 1,287.56 [1,175.67–1,415.02] | 8,445.05 [7,048.61–10,051.43] | 648.16 [551.53–754.05] | −2.6 [−2.7 to −2.49] |
| Central Latin America | 23,218.94 [22,345.71–24,216.2] | 1,489.7 [1,425.47–1,560.82] | 23,693.2 [20,326.43–27,267.39] | 922.94 [792.49–1,062.49] | −1.39 [−1.54 to −1.25] |
| Central sub-Saharan Africa | 19,360.86 [14,749.89–24,324.22] | 3,085.19 [2,423.86–3,728.34] | 27,415.1 [19,745.18–36,123.53] | 2,190.04 [1,597.63–2,895.56] | −1.14 [−1.3 to −0.98] |
| East Asia | 145,289.57 [126,698–192,614.2] | 1,168.54 [1,020.97–1,544.6] | 138,497.86 [118,706.15–157,642.08] | 837.7 [723.05–944.01] | −0.93 [−1.28 to −0.57] |
| Eastern Europe | 42,534.12 [38,443.48–47,374.99] | 1,800.37 [1,645.11–1,988.66] | 24,224.14 [20,793.45–28,542.97] | 1,061.33 [928.45–1,226.45] | −2.04 [−2.34 to −1.73] |
| Eastern sub-Saharan Africa | 22,892.18 [19,073.42–26,929.3] | 1,355.1 [1,168.45–1,551.73] | 30,358.48 [25,860.87–35,891.01] | 927.02 [801.29–1,075.76] | −1.38 [−1.41 to −1.35] |
| High-income Asia Pacific | 17,097.24 [16,178.58–18,040.11] | 960.98 [911.05–1,012.71] | 6,218.29 [5,538.31–7,130.11] | 276.35 [249.83–319.72] | −5.16 [−5.45 to −4.87] |
| High-income North America | 32,522.81 [30,969.3–34,315.68] | 1,140.18 [1,090.86–1,196.71] | 25,423.69 [23,378.27–27,639.57] | 663.99 [617.66–711.86] | −2.04 [−2.22 to −1.86] |
| North Africa and Middle East | 83,280.05 [68,073.75–94,352.54] | 2,336.72 [1,919.06–2,597.23] | 79,889.53 [67,371.19–92,464.84] | 1,306.58 [1,096.23–1,509.14] | −1.98 [−2 to −1.95] |
| Oceania | 929.9 [759.29–1,154.06] | 1,473.91 [1,215.76–1792.4] | 1,685.71 [1,335.17–2,227.61] | 1,288.29 [1,025.87–1,668.58] | −0.41 [−0.46 to −0.36] |
| South Asia | 109,861.14 [97,282.68–122,275.73] | 1,129.31 [990.19–1,267.57] | 182,324.75 [150,456.67–211,791.51] | 1,043.94 [863.88–1,219.94] | −0.25 [−0.52 to 0.02] |
| Southeast Asia | 75,747.96 [65,807.14–84,504.62] | 1,610.09 [1,417.2–1,782.49] | 64,509.58 [56,424.98–73,794.92] | 928.71 [812.9–1,061.73] | −2.15 [−2.27 to −2.03] |
| Southern Latin America | 3,997.18 [3,812.6–4,206.72] | 812.95 [775.2–856.68] | 5,014.58 [4,678.14–5,364.26] | 719.16 [671.78–767.72] | −0.48 [−0.62 to −0.33] |
| Southern sub-Saharan Africa | 13,189.66 [10,969.98–14,323.93] | 2,674.85 [2,219.32–2,906.18] | 13,313.67 [11,190.95–15,106.98] | 1,658.74 [1,414.26–1,865.44] | −1.9 [−2.29 to −1.51] |
| Tropical Latin America | 26,201.65 [25,171.8–27,343.38] | 1,737.19 [1,669.2–1,811.97] | 25,168.11 [23,753.68–26,462.55] | 1,064.89 [1,004.12–1,120.26] | −1.36 [−1.53 to −1.19] |
| Western Europe | 37,593.78 [35,935.68–39,545.26] | 958.21 [921.19–1,002.05] | 14,339.7 [13,059.96–15,807.33] | 314.57 [291.18–341.19] | −4.48 [−4.75 to −4.22] |
| Western sub-Saharan Africa | 22,616.45 [18,889–26,903.33] | 1,202.26 [1,026.31–1,388.47] | 39,999.37 [32,526.35–48,363.36] | 1,007.76 [839.47–1,192.36] | −0.51 [−0.55 to −0.46] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Y.; Chen, M.; Yang, R.; Wumaierjiang, M.; Huang, S. Global, Regional, and National Burden of Road Injuries from 1990 to 2019. Int. J. Environ. Res. Public Health 2022, 19, 16479. https://doi.org/10.3390/ijerph192416479
Xu Y, Chen M, Yang R, Wumaierjiang M, Huang S. Global, Regional, and National Burden of Road Injuries from 1990 to 2019. International Journal of Environmental Research and Public Health. 2022; 19(24):16479. https://doi.org/10.3390/ijerph192416479
Chicago/Turabian StyleXu, Yifan, Meikai Chen, Ruitong Yang, Muhemaiti Wumaierjiang, and Shengli Huang. 2022. "Global, Regional, and National Burden of Road Injuries from 1990 to 2019" International Journal of Environmental Research and Public Health 19, no. 24: 16479. https://doi.org/10.3390/ijerph192416479