
Conceptual Framework for Smart Health: A Multi-Dimensional Model Using IPO Logic to Link Drivers and Outcomes

Abstract
:1. Introduction
2. Methods
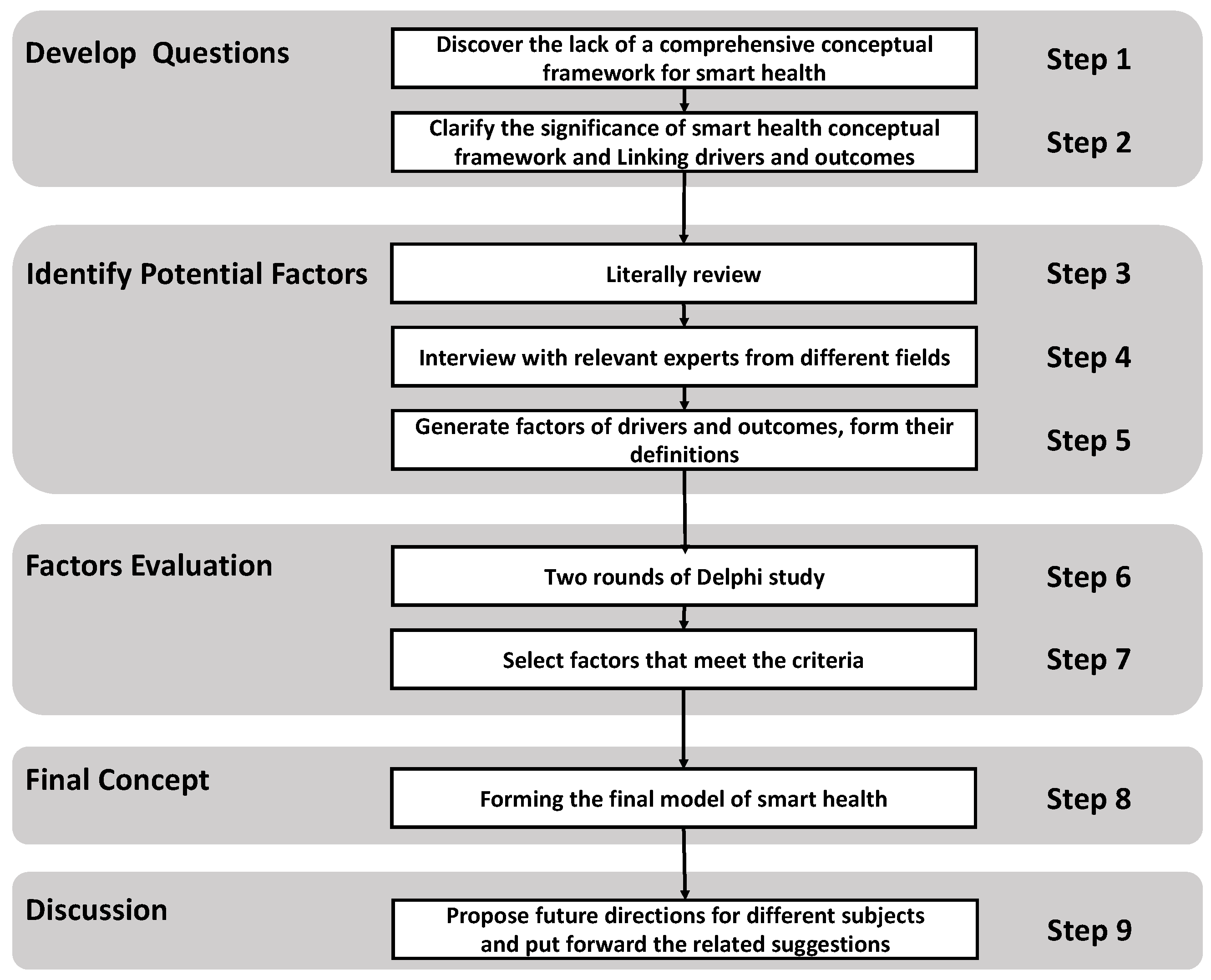
2.1. Modified Delphi Method
- (1)
- Review the literature and develop a questionnaire;
- (2)
- Form a group of experts;
- (3)
- Distribute the questionnaire on expert opinions;
- (4)
- Analyze and integrate group opinions;
- (5)
- Conduct a second round of questionnaire design and surveys;
- (6)
- Achieve a consensus.
2.2. Literature Review
- (1)
- The study must constitute primary research of any design;
- (2)
- It must be published in print format or on the Internet;
- (3)
- It must contain a definition or attempt to define smart health in clear terms;
- (4)
- It must be relevant to health or health systems.
2.3. Focus Group Interviews
- (1)
- In your opinion, what is the purpose of smart health?
- (2)
- What are the three to five characteristics of smart health?
- (3)
- How can smart health be achieved?
- (4)
- What is the current impact of smart health on personal and professional healthcare?
- (5)
- What impact is smart health likely to have in the next 5 years?
2.4. Factor Generation
2.5. Profile of Panel
2.6. Delphi Rounds
2.7. Consensus and Stability Levels
3. Results and Analysis
3.1. Data Analysis
3.2. Drivers
3.2.1. Technology
3.2.2. Community
3.2.3. Policy
3.2.4. Service
3.2.5. Management
3.3. Outcomes
3.3.1. Efficient
3.3.2. Smart
3.3.3. Security
3.3.4. Trust
3.3.5. Economy
3.3.6. Sustainability
3.3.7. Planned
3.3.8. Equitable
3.3.9. Multiple Participation and Better Health
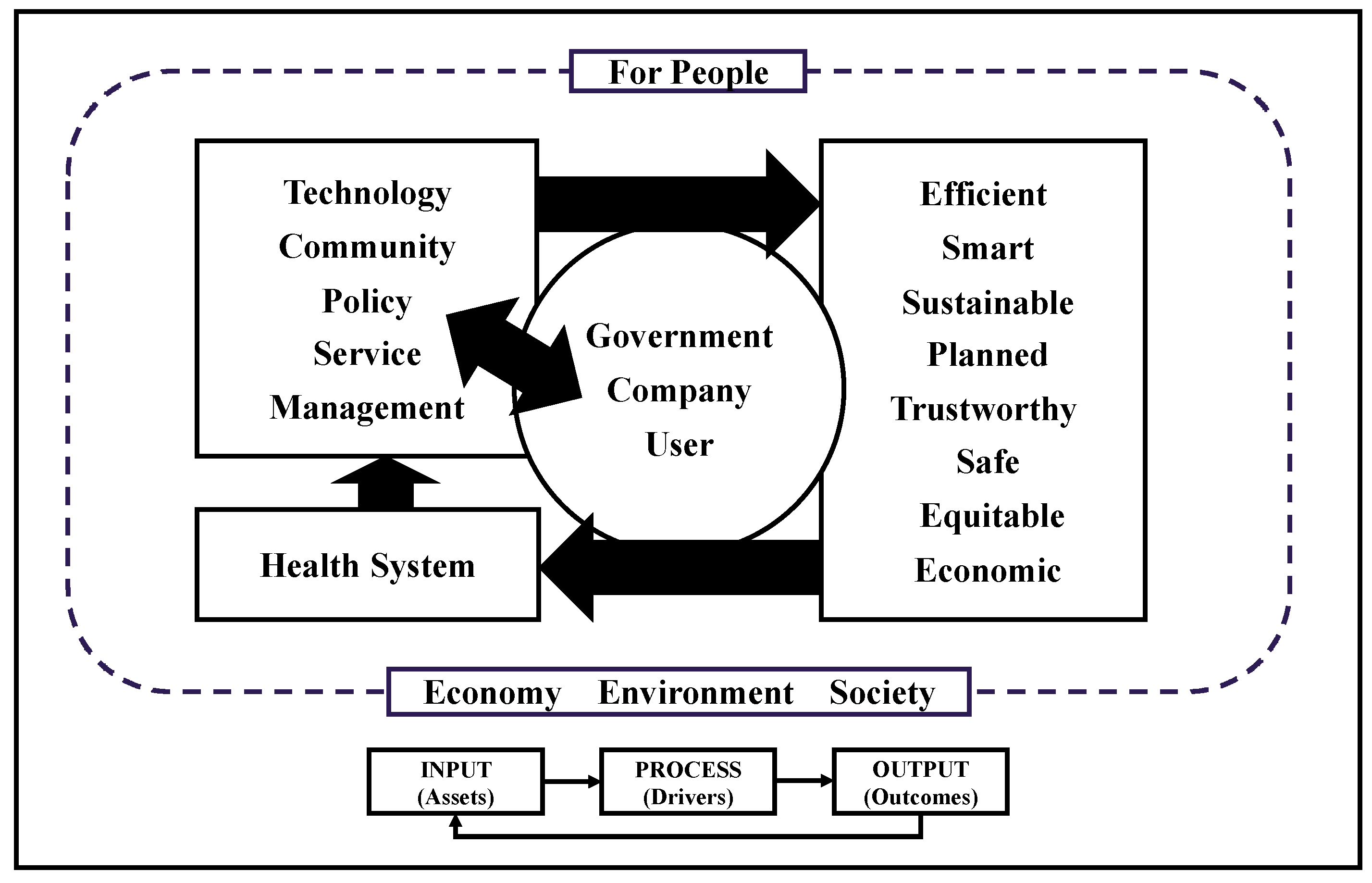
3.4. The Proposed Multidimensional Framework
4. Discussion
4.1. Smart Health and Relevant Concept
4.2. Smart Health and Smart City
4.3. Delphi Methodology for Identifying Smart Health Factors
4.4. Implications for Practice
4.5. Limitations
4.6. Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Definition and Primary Theme of Smart Health
| NO | Reference | Definition | Theme |
| 1 | [83] | A healthcare system that enables patients and doctors to communicate with each other and remotely exchange the information monitored, collected, and analyzed from patients’ daily activities via the IoT. | Technology Services Efficiency |
| 2 | [18] | Smart healthcare can be defined as an integration of patients and doctors into a common platform for intelligent health monitoring by analyzing day-to-day human activities. | Technology Services |
| 3 | [10] | Smart healthcare uses a new generation of information technologies, such as the internet of things (loT), big data, cloud computing, and artificial intelligence, to transform the traditional medical system in an overarching fashion, thereby rendering healthcare more efficient, convenient, and personalized. | Technology Efficient Trust Sustainable |
| 4 | [84] | Smart Health provides the healthiest possible living environment by improving quality of life. Combining disruptive technologies (Internet of Things (IoT) + Cloud Computing + Smart Sensing + Big Data technologies), this system constitutes a paradigm shift in the field of ICT that seeks to promote and render optimal solutions and care coordination in a form of collaborative management called “smart health”. | Technology Services Management Better -health Efficiency |
| 5 | [85] | The emerging field of s-health constitutes isolated, intelligent, customized health services, usually employing sensor data gathering and cloud processing. | Technology Services |
| 6 | [77] | Smart health is the provision of health services by using a context-aware network and the sensing infrastructure of smart cities. | Technology Services |
| 7 | [86] | This term, which inherently integrates ideas from ubiquitous computing and ambient intelligence applied to the future P4-medicine concept, is tightly connected to concepts of wellness and well-being, and incorporates big data, collected by vast quantities of biomedical sensors and actuators, to monitor, predict, and improve patients’ physical and mental conditions. | Technology Efficiency Health |
| 8 | [60] | Intelligent medicine refers to the construction of an interactive platform for the sharing of medical information based on electronic health records and the comprehensive use of the IoT, internet, cloud computing, big data, and other technologies to realize the interaction of patients, medical institutions, and medical personnel and equipment, and intelligently match the needs of the medical biosphere. | Technology Services Efficiency Sustainable |
| 9 | [8] | The infrastructure and technology of smart cities reconstruct the thinking behind existing healthcare systems (e.g., m-health, e-health, etc.) and telemedicine to create a new and comfortable ubiquitous concept that is called smart health. | Technology Thinking |
| 10 | [87] | Smart health integrates ideas from ubiquitous computing and ambient intelligence applied to predictive, personalized, preventive, and participatory healthcare systems. | Technology Efficiency Health Trust Sustainable |
| 12 | [88] | Smart health refers not only to ICT development, but also to a state of thinking, a lifestyle and approach, and a vow for connected entities to improve healthcare facilities in the home, city, country, and globe with the aid of a number of intelligent agents. | Technology Services Thinking Efficiency |
Appendix B. MDM Questionnaire (Round 2)
- Rules for filling in the survey: please give a score according to your understanding of the importance of the drivers (projects) of smart healthcare. (Round 2.).
| Design Factor | Please Circle One Number Per Row below Using the Scale: | ||||
| 1 Being Very Unimportant and 5 Being Very Important | |||||
| Technology | 1 | 2 | 3 | 4 | 5 |
| Service | 1 | 2 | 3 | 4 | 5 |
| Policy | 1 | 2 | 3 | 4 | 5 |
| Community | 1 | 2 | 3 | 4 | 5 |
| Management | 1 | 2 | 3 | 4 | 5 |
| Other influencing factors (if any): | |||||
- B.
- Rules for filling in the survey: please give a score according to your understanding of the importance of the outcomes (target) of smart healthcare. (Round 2).
| Design Factor | Please Circle One Number Per Row below Using the Scale: | ||||
| 1 Being Very Unimportant and 5 Being Very Important | |||||
| Efficient | 1 | 2 | 3 | 4 | 5 |
| Intelligent | 1 | 2 | 3 | 4 | 5 |
| Sustainable | 1 | 2 | 3 | 4 | 5 |
| Planned | 1 | 2 | 3 | 4 | 5 |
| Trustworthy | 1 | 2 | 3 | 4 | 5 |
| Safe | 1 | 2 | 3 | 4 | 5 |
| Equitable | 1 | 2 | 3 | 4 | 5 |
| Better Health | 1 | 2 | 3 | 4 | 5 |
| Economic | 1 | 2 | 3 | 4 | 5 |
| Other influencing factors (if any): | |||||
Appendix C. MDM Questionnaire (Round 3)
| Design Factor | Approve/ Do Not Approve | Reason | |
| Drivers | Community | ||
| Management | |||
| Outcomes | Planned | ||
| Equitable | |||
| Better Health | |||
| Multiple participation | |||
References
- Murray, C.J.; Hanlon, M.; Lavado, R.; Haakenstad, A.; Graves, C.; Brooks, B.P.; Dieleman, J.; Frostad, J.; Leach-Kemon, K.; Tardif, A. Financing Global Health 2012: The End of the Golden Age; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2012. [Google Scholar]
- Rodriguez, R.; Svensson, G.; Wood, G. Sustainability Trends in Public Hospitals: Efforts and Priorities. Eval. Program Plan. 2020, 78, 101742. [Google Scholar] [CrossRef]
- Goodspeed, R. Smart Cities: Moving beyond Urban Cybernetics to Tackle Wicked Problems. Camb. J. Reg. Econ. Soc. 2015, 8, 79–92. [Google Scholar] [CrossRef]
- Zheng, X.; Rodríguez-Monroy, C. The Development of Intelligent Healthcare in China. Telemed. E-Health 2015, 21, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wu, C.K.; Koo, C.H.; Tsang, Y.T.; Liu, Y.; Chi, H.R.; Tsang, K.-F. Smart Healthcare in the Era of Internet-of-Things. IEEE Consum. Electron. Mag. 2019, 8, 26–30. [Google Scholar] [CrossRef]
- Nasr, M.; Islam, M.M.; Shehata, S.; Karray, F.; Quintana, Y. Smart Healthcare in the Age of AI: Recent Advances, Challenges, and Future Prospects. IEEE Access 2021, 9, 145248–145270. [Google Scholar] [CrossRef]
- Chui, K.; Alhalabi, W.; Pang, S.; Pablos, P.; Liu, R.; Zhao, M. Disease Diagnosis in Smart Healthcare: Innovation, Technologies and Applications. Sustainability 2017, 9, 2309. [Google Scholar] [CrossRef] [Green Version]
- Pramanik, M.I.; Lau, R.Y.K.; Demirkan, H.; Azad, M.A.K. Smart Health: Big Data Enabled Health Paradigm within Smart Cities. Expert Syst. Appl. 2017, 87, 370–383. [Google Scholar] [CrossRef]
- Baig, M.M.; Gholamhosseini, H. Smart Health Monitoring Systems: An Overview of Design and Modeling. J. Med. Syst. 2013, 37, 1–14. [Google Scholar] [CrossRef]
- Tian, S.; Yang, W.; Grange, J.M.L.; Wang, P.; Huang, W.; Ye, Z. Smart Healthcare: Making Medical Care More Intelligent. Glob. Health J. 2019, 3, 62–65. [Google Scholar] [CrossRef]
- Han, H.; Hawken, S. Introduction: Innovation and Identity in next-Generation Smart Cities. City Cult. Soc. 2018, 12, 1–4. [Google Scholar] [CrossRef]
- Hollands, R.G. Critical Interventions into the Corporate Smart City. Camb. J. Reg. Econ. Soc. 2015, 8, 61–77. [Google Scholar] [CrossRef] [Green Version]
- Yusof, M.M.; Kuljis, J.; Papazafeiropoulou, A.; Stergioulas, L.K. An Evaluation Framework for Health Information Systems: Human, Organization and Technology-Fit Factors (HOT-Fit). Int. J. Med. Inform. 2008, 77, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B. Evaluating Informatics Applications—Clinical Decision Support Systems Literature Review. Int. J. Med. Inform. 2001, 64, 15–37. [Google Scholar] [CrossRef]
- Kaplan, B.; Shaw, N.T. Future Directions in Evaluation Research: People, Organizational, and Social Issues. Methods Inf. Med. 2004, 43, 215–231. [Google Scholar] [CrossRef]
- Manga, V.E.; Forton, O.T.; Mofor, L.A.; Woodard, R. Health Care Waste Management in Cameroon: A Case Study from the Southwestern Region. Resour. Conserv. Recycl. 2011, 57, 108–116. [Google Scholar] [CrossRef]
- Govind, R.; Chatterjee, R.; Mittal, V. Timely Access to Health Care: Customer-Focused Resource Allocation in a Hospital Network. Int. J. Res. Mark. 2008, 25, 294–300. [Google Scholar] [CrossRef]
- Lohachab, A. Bootstrapping Urban Planning: Addressing Big Data Issues in Smart Cities. In Research Anthology on Big Data Analytics, Architectures, and Applications; IGI Global: Hershey, PA, USA, 2022; pp. 1329–1358. [Google Scholar]
- Yang, G.; Pang, Z.; Deen, M.J.; Dong, M.; Zhang, Y.-T.; Lovell, N.; Rahmani, A.M. Homecare Robotic Systems for Healthcare 4.0: Visions and Enabling Technologies. IEEE J. Biomed. Health Inform. 2020, 24, 2535–2549. [Google Scholar] [CrossRef]
- Wolfe, A. Institute of Medicine Report: Crossing the Quality Chasm: A New Health Care System for the 21st Century. Policy Politics Nurs. Pract. 2001, 2, 233–235. [Google Scholar] [CrossRef]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-Quality Health Systems in the Sustainable Development Goals Era: Time for a Revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef] [Green Version]
- Ilgen, D.R.; Hollenbeck, J.R.; Johnson, M.; Jundt, D. Teams in Organizations: From Input-Process-Output Models to IMOI Models. Annu. Rev. Psychol. 2005, 56, 517–543. [Google Scholar] [CrossRef]
- Davis, W.S.; Yen, D.C. The Information System Consultant’s Handbook: Systems Analysis and Design, 1st ed.; Davis, W.S., Yen, D.C., Eds.; CRC Press: Boca Raton, FL, USA, 2019; ISBN 978-1-315-21974-5. [Google Scholar]
- Dalkey, N.; Helmer, O. An Experimental Application of the DELPHI Method to the Use of Experts. Manag. Sci. 1963, 9, 458–467. [Google Scholar] [CrossRef]
- Hsu, Y.; Lee, C.; Kreng, V.B. The Application of Fuzzy Delphi Method and Fuzzy AHP in Lubricant Regenerative Technology Selection. Expert Syst. Appl. 2010, 37, 419–425. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Tavakkoli-Moghaddam, R.; Heydar, M.; Ebrahimnejad, S. Multi-Criteria Decision Making for Plant Location Selection: An Integrated Delphi–AHP–PROMETHEE Methodology. Arab. J. Sci. Eng. 2013, 38, 1255–1268. [Google Scholar] [CrossRef]
- Wu, Y.J.; Chen, J.-C. A Structured Method for Smart City Project Selection. Int. J. Inf. Manag. 2021, 56, 101981. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Stalmeijer, R.E.; McNaughton, N.; Van Mook, W.N.K.A. Using Focus Groups in Medical Education Research: AMEE Guide No. 91. Med. Teach. 2014, 36, 923–939. [Google Scholar] [CrossRef]
- Kitzinger, J. Qualitative Research: Introducing Focus Groups. BMJ 1995, 311, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Pan, N. Fuzzy AHP Approach for Selecting the Suitable Bridge Construction Method. Autom. Constr. 2008, 17, 958–965. [Google Scholar] [CrossRef]
- Hsu, C.; Sandford, B.A. The Delphi Technique: Making Sense of Consensus. Pract. Assess. Res. Eval. 2007, 12, 10. [Google Scholar] [CrossRef]
- Cerè, G.; Rezgui, Y.; Zhao, W. Urban-Scale Framework for Assessing the Resilience of Buildings Informed by a Delphi Expert Consultation. Int. J. Disaster Risk Reduct. 2019, 36, 101079. [Google Scholar] [CrossRef]
- Alshehri, S.A.; Rezgui, Y.; Li, H. Delphi-Based Consensus Study into a Framework of Community Resilience to Disaster. Nat. Hazards 2015, 75, 2221–2245. [Google Scholar] [CrossRef]
- Greatorex, J.; Dexter, T. An Accessible Analytical Approach for Investigating What Happens between the Rounds of a Delphi Study. J. Adv. Nurs. 2000, 32, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Goldman, K.; Gross, P.; Heeren, C.; Herman, G.; Kaczmarczyk, L.; Loui, M.C.; Zilles, C. Identifying Important and Difficult Concepts in Introductory Computing Courses Using a Delphi Process. In Proceedings of the 39th SIGCSE Technical Symposium on Computer Science Education, Portland, OR, USA, 12–15 March 2008; pp. 256–260. [Google Scholar]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining Consensus: A Systematic Review Recommends Methodologic Criteria for Reporting of Delphi Studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Hu, Y.-C.; Yen, G.-F.; Tsao, S.-J. Green Supplier Selection for Sustainable Development of the Automotive Industry Using Grey Decision-Making. Sustain. Dev. 2018, 26, 890–903. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of Healthcare Interventions: An Overview of Reviews and Development of a Theoretical Framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef] [Green Version]
- Walter, Z.; Lopez, M.S. Physician Acceptance of Information Technologies: Role of Perceived Threat to Professional Autonomy. Decis. Support Syst. 2008, 46, 206–215. [Google Scholar] [CrossRef]
- Lapointe, S.; Rivard, A. A Multilevel Model of Resistance to Information Technology Implementation. MIS Q. 2005, 29, 461. [Google Scholar] [CrossRef] [Green Version]
- Bhattacherjee, A.; Hikmet, N. Physicians’ Resistance toward Healthcare Information Technology: A Theoretical Model and Empirical Test. Eur. J. Inf. Syst. 2007, 16, 725–737. [Google Scholar] [CrossRef]
- Nadal, C.; Sas, C.; Doherty, G. Technology Acceptance in Mobile Health: Scoping Review of Definitions, Models, and Measurement. J. Med. Internet Res. 2020, 22, e17256. [Google Scholar] [CrossRef]
- Lidz, C.W.; Albert, K.; Appelbaum, P.; Dunn, L.B.; Overton, E.; Pivovarova, E. Why Is Therapeutic Misconception So Prevalent? Camb. Q. Health Ethics 2015, 24, 231–241. [Google Scholar] [CrossRef]
- Appelbaum, P.S.; Lidz, C.W.; Grisso, T. Therapeutic Misconception in Clinical Research: Frequency and Risk Factors. IRB Ethics Hum. Res. 2004, 26, 1. [Google Scholar] [CrossRef]
- Lin, C.-L.; Chen, J.K.C.; Ho, H.-H. BIM for Smart Hospital Management during COVID-19 Using MCDM. Sustainability 2021, 13, 6181. [Google Scholar] [CrossRef]
- World Health Organization. Everybody’s Business—Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. WHO Global Strategy on People-Centred and Integrated Health Services: Interim Report; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Kuruvilla, S.; Bustreo, F.; Kuo, T.; Mishra, C.; Taylor, K.; Fogstad, H.; Gupta, G.R.; Gilmore, K.; Temmerman, M.; Thomas, J.; et al. The Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030): A Roadmap Based on Evidence and Country Experience. Bull. World Health Organ. 2016, 94, 398–400. [Google Scholar] [CrossRef] [PubMed]
- Ryan-Fogarty, Y.; O’Regan, B.; Moles, R. Greening Healthcare: Systematic Implementation of Environmental Programmes in a University Teaching Hospital. J. Clean. Prod. 2016, 126, 248–259. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Rokhani, F.Z.; Shariff Ghazali, S.; Chew, B.H. Defining the Concepts of a Smart Nursing Home and Its Potential Technology Utilities That Integrate Medical Services and Are Acceptable to Stakeholders: A Scoping Review Protocol. BMJ Open 2021, 11, e041452. [Google Scholar] [CrossRef] [PubMed]
- Stroetmann, K. Achieving the Integrated and Smart Health and Wellbeing Paradigm: A Call for Policy Research and Action on Governance and Business Models. Int. J. Med. Inform. 2012, 82, e29–e37. [Google Scholar] [CrossRef]
- Yusof, M.M.; Papazafeiropoulou, A.; Paul, R.J.; Stergioulas, L.K. Investigating Evaluation Frameworks for Health Information Systems. Int. J. Med. Inform. 2008, 77, 377–385. [Google Scholar] [CrossRef]
- Flessa, S.; Huebner, C. Innovations in Health Care—A Conceptual Framework. IJERPH 2021, 18, 10026. [Google Scholar] [CrossRef]
- Heyen, N.B.; Reiβ, T. Das Gesundheitswesen Aus Innovationssystemperspektive: Acht Thesen Und Handlungsmöglichkeiten. Teil 1. Soz. Fortschr. 2014, 63, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Zhang, L.; Wei, M. How Does Smart Healthcare Service Affect Resident Health in the Digital Age? Empirical Evidence From 105 Cities of China. Front. Public Health 2022, 9, 833687. [Google Scholar] [CrossRef]
- Pan, J.; Ding, S.; Wu, D.; Yang, S.; Yang, J. Exploring Behavioural Intentions toward Smart Healthcare Services among Medical Practitioners: A Technology Transfer Perspective. Int. J. Prod. Res. 2019, 57, 5801–5820. [Google Scholar] [CrossRef]
- Su, Y.; Hou, F.; Qi, M.; Li, W.; Ji, Y. A Data-Enabled Business Model for a Smart Healthcare Information Service Platform in the Era of Digital Transformation. J. Healthc. Eng. 2021, 2021, 5519891. [Google Scholar] [CrossRef]
- Sukkird, V.; Shirahada, K. Technology Challenges to Healthcare Service Innovation in Aging Asia: Case of Value Co-Creation in Emergency Medical Support System. Technol. Soc. 2015, 43, 122–128. [Google Scholar] [CrossRef]
- Xue, X.; Zeng, Y.; Zhang, Y.; Lee, S.; Yan, Z. A Study on an Application System for the Sustainable Development of Smart Healthcare in China. IEEE Access 2021, 9, 111960–111974. [Google Scholar] [CrossRef]
- Ethics and Information Technology: A Case-Based Approach to a Health Care System in Transition; Health Informatics Series; Anderson, J.G.; Goodman, K.W. (Eds.) Springer: New York, NY, USA, 2004; ISBN 978-0-387-95308-3. [Google Scholar]
- Holden, R.J.; Carayon, P.; Gurses, A.P.; Hoonakker, P.; Hundt, A.S.; Ozok, A.A.; Rivera-Rodriguez, A.J. SEIPS 2.0: A Human Factors Framework for Studying and Improving the Work of Healthcare Professionals and Patients. Ergonomics 2013, 56, 1669–1686. [Google Scholar] [CrossRef] [Green Version]
- Mosadeghrad, A.M. Factors Influencing Healthcare Service Quality. Int. J. Health Policy Manag. 2014, 3, 77–89. [Google Scholar] [CrossRef]
- Gatteschi, V.; Lamberti, F.; Demartini, C.; Pranteda, C.; Santamaría, V. Blockchain and Smart Contracts for Insurance: Is the Technology Mature Enough? Future Internet 2018, 10, 20. [Google Scholar] [CrossRef] [Green Version]
- Rikhardsson, P.; Yigitbasioglu, O. Business Intelligence & Analytics in Management Accounting Research: Status and Future Focus. Int. J. Account. Inf. Syst. 2018, 29, 37–58. [Google Scholar] [CrossRef] [Green Version]
- Aghazadeh, H. Strategic Marketing Management: Achieving Superior Business Performance through Intelligent Marketing Strategy. Procedia Soc. Behav. Sci. 2015, 207, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.Q.; Preston, D.S.; Xia, W. Enhancing Hospital Supply Chain Performance: A Relational View and Empirical Test. J. Oper. Manag. 2013, 31, 391–408. [Google Scholar] [CrossRef]
- Saad, S.A.G. Management of Hospitals Solid Waste in Khartoum State. Environ. Monit. Assess. 2013, 185, 8567–8582. [Google Scholar] [CrossRef] [PubMed]
- Xin, Y. Comparison of Hospital Medical Waste Generation Rate Based on Diagnosis-Related Groups. J. Clean. Prod. 2015, 100, 202–207. [Google Scholar] [CrossRef]
- Campion, N.; Thiel, C.L.; Woods, N.C.; Swanzy, L.; Landis, A.E.; Bilec, M.M. Sustainable Healthcare and Environmental Life-Cycle Impacts of Disposable Supplies: A Focus on Disposable Custom Packs. J. Clean. Prod. 2015, 94, 46–55. [Google Scholar] [CrossRef]
- Faezipour, M.; Ferreira, S. Assessing Water Sustainability Related to Hospitals Using System Dynamics Modeling. Procedia Comput. Sci. 2014, 36, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Teke, A.; Timur, O. Assessing the Energy Efficiency Improvement Potentials of HVAC Systems Considering Economic and Environmental Aspects at the Hospitals. Renew. Sustain. Energy Rev. 2014, 33, 224–235. [Google Scholar] [CrossRef]
- Yarmohammadian, M.H.; Atighechian, G.; Shams, L.; Haghshenas, A. Are Hospitals Ready to Response to Disasters? Challenges, Opportunities and Strategies of Hospital Emergency Incident Command System (HEICS). J. Res. Med. Sci. 2011, 16, 1070–1077. [Google Scholar]
- Arah, O.A.; Westert, G.P.; Hurst, J.; Klazinga, N.S. A Conceptual Framework for the OECD Health Care Quality Indicators Project. Int. J. Qual. Health Care 2006, 18, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Franken, M.; Koolman, X. Health System Goals: A Discrete Choice Experiment to Obtain Societal Valuations. Health Policy 2013, 112, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Teriman, S.; Yigitcanlar, T.; Mayere, S. Sustainable Urban Development: A Quadruple Bottom Line Assessment Framework. In Proceedings of the Conference Proceedings of the Second Infrastructure Theme Postgraduate Conference 2009: Rethinking Sustainable Development, Planning, Infrastructure Engineeering, Design and Managing Urban Infrastructure; Queensland University of Technology: Brisbane, Australia, 2009; pp. 228–238. [Google Scholar]
- Solanas, A.; Patsakis, C.; Conti, M.; Vlachos, I.; Ramos, V.; Falcone, F.; Postolache, O.; Perez-martinez, P.; Pietro, R.; Perrea, D.; et al. Smart Health: A Context-Aware Health Paradigm within Smart Cities. IEEE Commun. Mag. 2014, 52, 74–81. [Google Scholar] [CrossRef]
- Sadegh, S.S.; Khakshour Saadat, P.; Sepehri, M.M.; Assadi, V. A Framework for M-Health Service Development and Success Evaluation. Int. J. Med. Inform. 2018, 112, 123–130. [Google Scholar] [CrossRef]
- Albino, V.; Berardi, U.; Dangelico, R.M. Smart Cities: Definitions, Dimensions, Performance, and Initiatives. J. Urban Technol. 2015, 22, 3–21. [Google Scholar] [CrossRef]
- Haarstad, H. Constructing the Sustainable City: Examining the Role of Sustainability in the ‘Smart City’Discourse. J. Environ. Policy Plan. 2017, 19, 423–437. [Google Scholar] [CrossRef]
- Negev, M.; Davidovitch, N.; Garb, Y.; Tal, A. Stakeholder Participation in Health Impact Assessment: A Multicultural Approach. Environ. Impact Assess. Rev. 2013, 43, 112–120. [Google Scholar] [CrossRef]
- Smith, A.M.; Fischbacher, M. New Service Development: A Stakeholder Perspective. Eur. J. Mark. 2005, 39, 1025–1048. [Google Scholar] [CrossRef]
- Lee, Y.K. Review of the Role of the Internet of Things (IoT) on the Consumer Market: Focusing on Smart Tourism, Healthcare, and Retailing. In Examining the Socio-Technical Impact of Smart Cities; IGI Global: Hershey, PA, USA, 2021; pp. 180–198. [Google Scholar] [CrossRef]
- Arulananthan, C.; Hanifa, S.M. Smart Health–Potential and Pathways: A Survey. IOP Conf. Ser. Mater. Sci. Eng. 2017, 225, 012065. [Google Scholar]
- Bedón-Molina, J.; Lopez, M.J.; Derpich, I.S. A Home-Based Smart Health Model. Adv. Mech. Eng. 2020, 12, 1687814020935282. [Google Scholar] [CrossRef]
- Holzinger, A.; Röcker, C.; Ziefle, M. From Smart Health to Smart Hospitals. In Smart Health; Lecture Notes in Computer Science; Holzinger, A., Röcker, C., Ziefle, M., Eds.; Springer International Publishing: Cham, Switzerland, 2015; Volume 8700, pp. 1–20. ISBN 978-3-319-16225-6. [Google Scholar]
- Röcker, C.; Ziefle, M.; Holzinger, A. From Computer Innovation to Human Integration: Current Trends and Challenges for Pervasive HealthTechnologies. In Pervasive Health; Springer: Berlin/Heidelberg, Germany, 2014; pp. 1–17. [Google Scholar]
- Clancy, C.M. Getting To ‘Smart’ Health Care: Comparative Effectiveness Research Is a Key Component of, but Tightly Linked with, Health Care Delivery in the Information Age. Health Aff. 2006, 25, W589–W592. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Design Factor | Definition |
|---|---|
| Technology | Smart health is based on information and communication technology (ICT) and is used to connect hospital staff, data, devices, core systems, and core infrastructure through the Internet of Things (IoT) for better diagnosis and treatment. Smart health also requires the acceptance of new technologies by both doctors and patients. |
| Service | With the help of an efficient medical system, smart medical care can streamline the process of medical treatment, improve the efficiency of medical treatment, facilitate communication between doctors and patients, and realize paperless and standardized case management through “Internet medicine”, “telemedicine”, and “consultation navigation”. It also enables paperless and standardized case management. |
| Policy | Achieving the goal of smart health requires government leadership within a well-designed framework. It includes a series of regulations and actions, such as rational allocation of healthcare resources, provision of basic health insurance, a configuration of the healthcare infrastructure, and multisectoral coordination. |
| Community | Through community medical service centers, smart medical care establishes electronic health records for community residents, tracks the health of community residents (especially the elderly), provides basic medical services, establishes (mandatory) referral systems, and reduces medical pressure on large hospitals. |
| Management | Smart health requires a systematic division of labor among several specialties and a rational allocation of manpower (recruitment, revenue allocation, etc.), finance (assets, prices, etc.), and safety (graded care, pollutant discharge, etc.) through medical (hospital) information systems. |
| Efficient | Smart medicine improves the efficiency of staff and patient access through system optimization, thereby increasing the satisfaction of both doctors and patients. |
| Intelligent | Smart health combines the concepts of evidence-based medicine and specialized treatment with connected platforms and data to provide fast and accurate access to treatment options. |
| Sustainable | Smart health establishes a new management model, attracts talent, and promotes knowledge upgradation as well as the patient-centered and robust development of the medical insurance system. |
| Planned | The government provides the framework for smart health development, leads proactive change in the healthcare industry, fulfills regulatory and leadership obligations, and harmonizes healthcare data standards. |
| Trustworthy | Compared to traditional healthcare, the smart health model can improve patient satisfaction, build trust between doctors and patients, and reduce doctor–patient conflicts. |
| Equitable | Smart health reduces the risk of medical errors and substandard care, properly manages medical data, and maintains patient privacy. It demonstrates good resilience in the event of crises, such as medical cramming and paralysis. |
| Fair | Smart health achieves medical coverage for all by rationally allocating medical resources, avoiding excessive concentration of resources, and narrowing the gap between urban and rural areas. |
| Better Health | Smart health can increase the average life expectancy of society, reduce disease morbidity and mortality, reduce disease suffering, and improve quality of life. |
| Economic | Smart health leverages smart technology to reduce healthcare costs while reducing ineffective and harmful healthcare waste through community-based hierarchical care. |
| Domain | Code | Time (Year) | Career | Degree |
|---|---|---|---|---|
| Intelligent Technologist | A1 | 22 | University Professor | PhD |
| A2 | 7 | Corporate R&D staff | Undergraduate | |
| Doctors | B1 | 19 | Neurologist | PhD |
| B2 | 5 | Neurologist | PhD | |
| Hospital Administrators | C1 | 10 | Medical Service | Master’s |
| C2 | 12 | Medical Service | Master’s | |
| Government Officials | D1 | 17 | Government Officials | Undergraduate |
| D2 | 16 | Government Officials | Undergraduate | |
| Research Scholars | E1 | 19 | University Professor | PhD |
| E2 | 17 | University Professor | PhD |
| Rating Scale | Perceived Impact |
|---|---|
| 1 | no impact |
| 2 | small impact |
| 3 | moderate impact |
| 4 | large impact |
| 5 | very high or profound impact |
| Percentage of Experts Indicating a Large or Profound Impact | Decision |
|---|---|
| 70% and above | Include |
| 40% to 69% | Indeterminate |
| 39% and below | Exclude |
| Design Factor | First Round | Second Round | ||||
|---|---|---|---|---|---|---|
| Mean | SD | CDIjt | Number of Consenting Participants (N = 10) | Number of Consenting Participants (N = 10) | ||
| Drivers | Technology | 4.3 | 0.50 | 0.11 | 10 | / |
| Community | 3.3 | 0.78 | 0.17 | 4 | 8 | |
| Policy | 4.5 | 0.73 | 0.16 | 9 | / | |
| Services | 4.1 | 0.78 | 0.17 | 8 | / | |
| Management | 3.5 | 1.01 | 0.22 | 6 | 7 | |
| Outcomes | Efficient | 4.6 | 0.53 | 0.12 | 10 | / |
| Intelligent | 4.1 | 0.60 | 0.13 | 9 | / | |
| Sustainable | 3.7 | 0.83 | 0.18 | 7 | / | |
| Planned | 3.7 | 0.83 | 0.18 | 5 | 7 | |
| Trustworthy | 3.6 | 1.12 | 0.25 | 7 | / | |
| Safe | 4.1 | 0.78 | 0.17 | 8 | / | |
| Equitable | 3.8 | 1.32 | 0.29 | 6 | 8 | |
| Better Health | 3.5 | 1.22 | 0.27 | 6 | 6 | |
| Economic | 3.8 | 1.20 | 0.26 | 8 | / | |
| Multiple Participation | New | 5 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, J.; Huang, S.; Wang, L.; Deng, W.; Yang, T. Conceptual Framework for Smart Health: A Multi-Dimensional Model Using IPO Logic to Link Drivers and Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 16742. https://doi.org/10.3390/ijerph192416742
Deng J, Huang S, Wang L, Deng W, Yang T. Conceptual Framework for Smart Health: A Multi-Dimensional Model Using IPO Logic to Link Drivers and Outcomes. International Journal of Environmental Research and Public Health. 2022; 19(24):16742. https://doi.org/10.3390/ijerph192416742
Chicago/Turabian StyleDeng, Jianwei, Sibo Huang, Liuan Wang, Wenhao Deng, and Tianan Yang. 2022. "Conceptual Framework for Smart Health: A Multi-Dimensional Model Using IPO Logic to Link Drivers and Outcomes" International Journal of Environmental Research and Public Health 19, no. 24: 16742. https://doi.org/10.3390/ijerph192416742