


More-Than-Human: A Cross-Sectional Study Exploring Children’s Perceptions of Health and Health-Promoting Neighbourhoods in Aotearoa New Zealand
 , , , , and
, , , , and 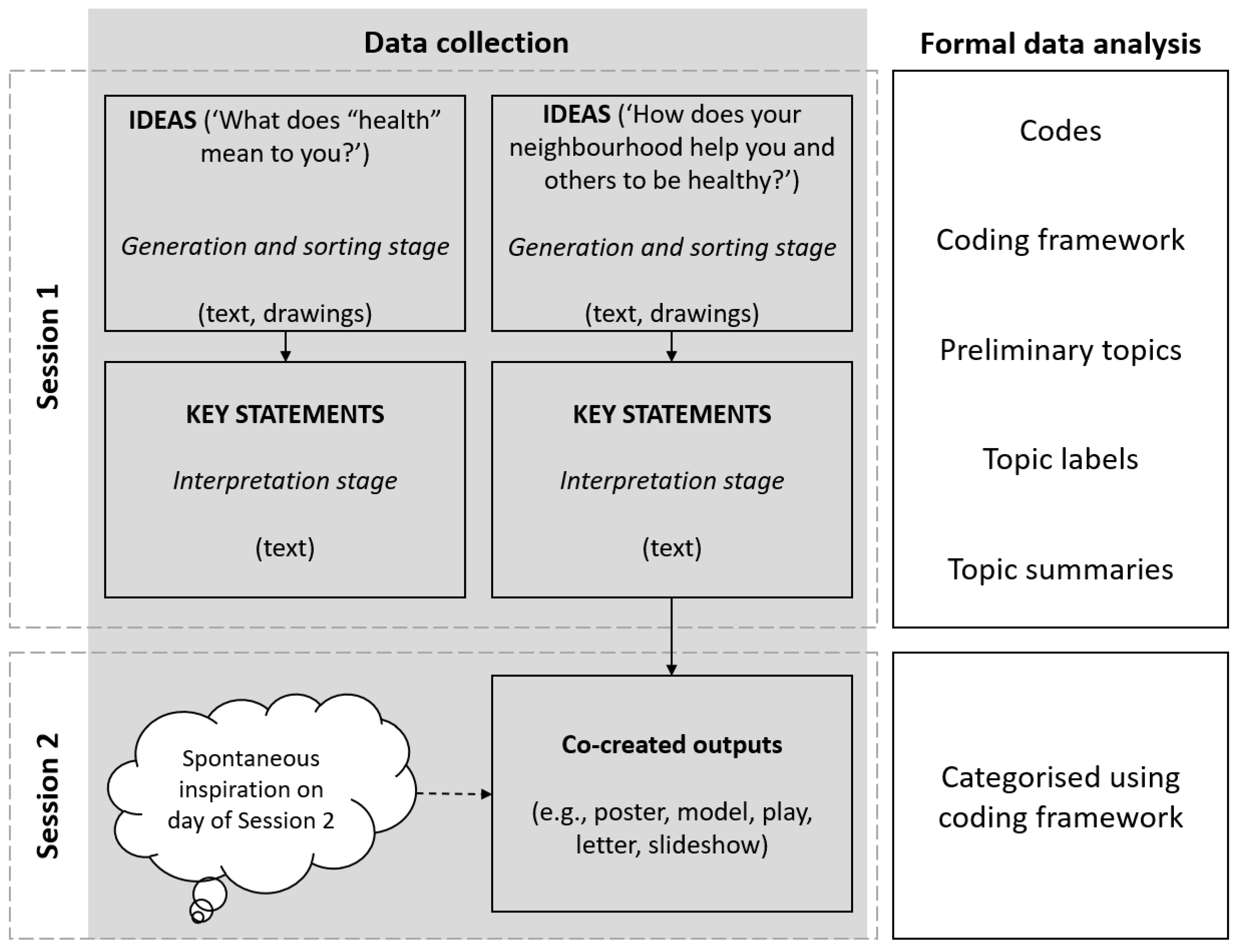{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. The Neighbourhoods and Health Study
1.2. Theoretical Framing: More-Than-Human Theory and Healthy Urban Environments
1.3. Children’s Perspectives on Health and Local Environments in Aotearoa New Zealand
1.4. Summarising the Knowledge Gap
1.5. Aim
2. Protocol and Methods
2.1. Setting
2.2. Recruitment
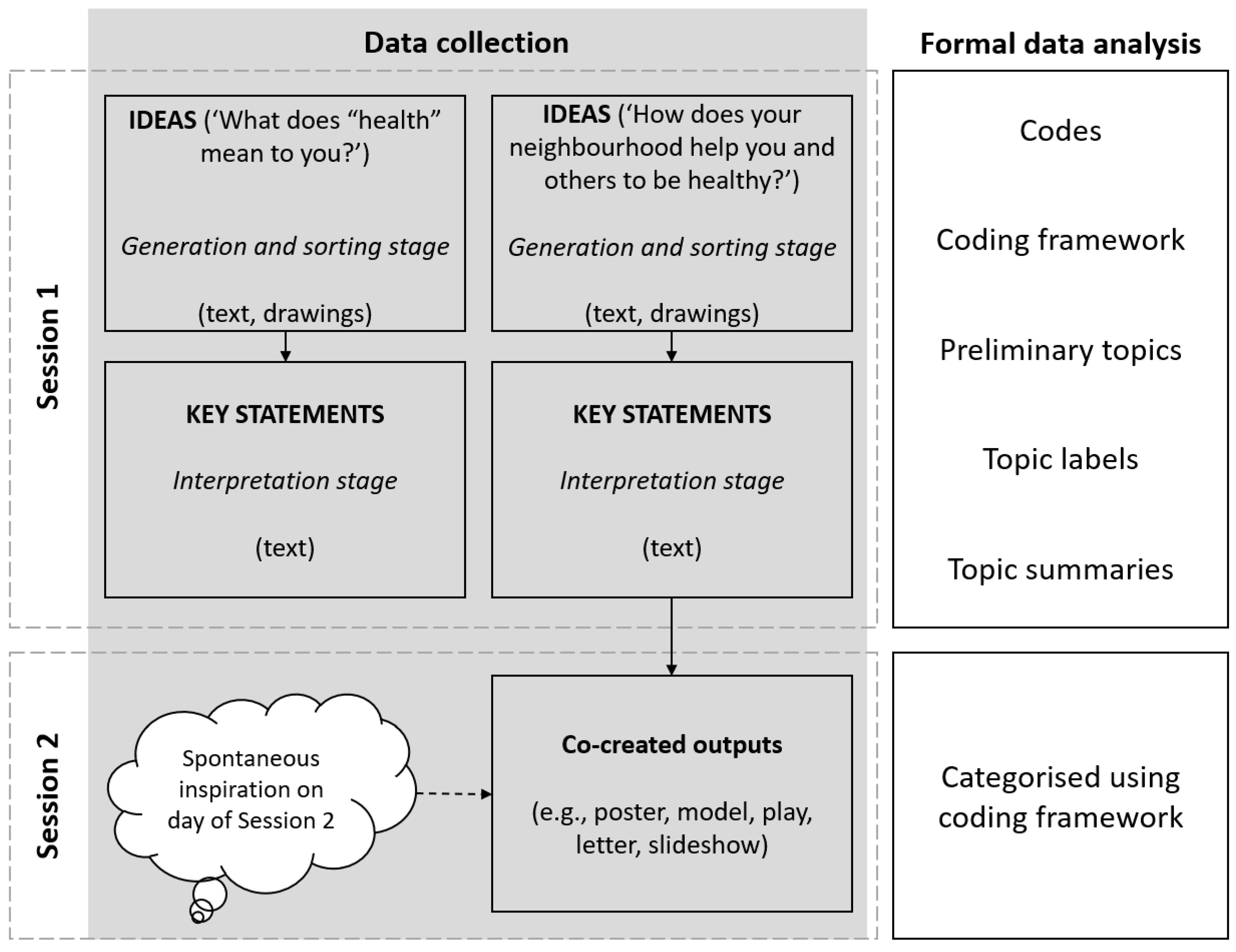
2.3. Data Collection Session One: Concept Mapping
2.4. Data Collection Session Two: Co-Creation of Dissemination Materials/Outputs
2.5. Formal Data Analysis
3. Results
3.1. Participants
3.2. Ideas and Key Statements Generated by Participants
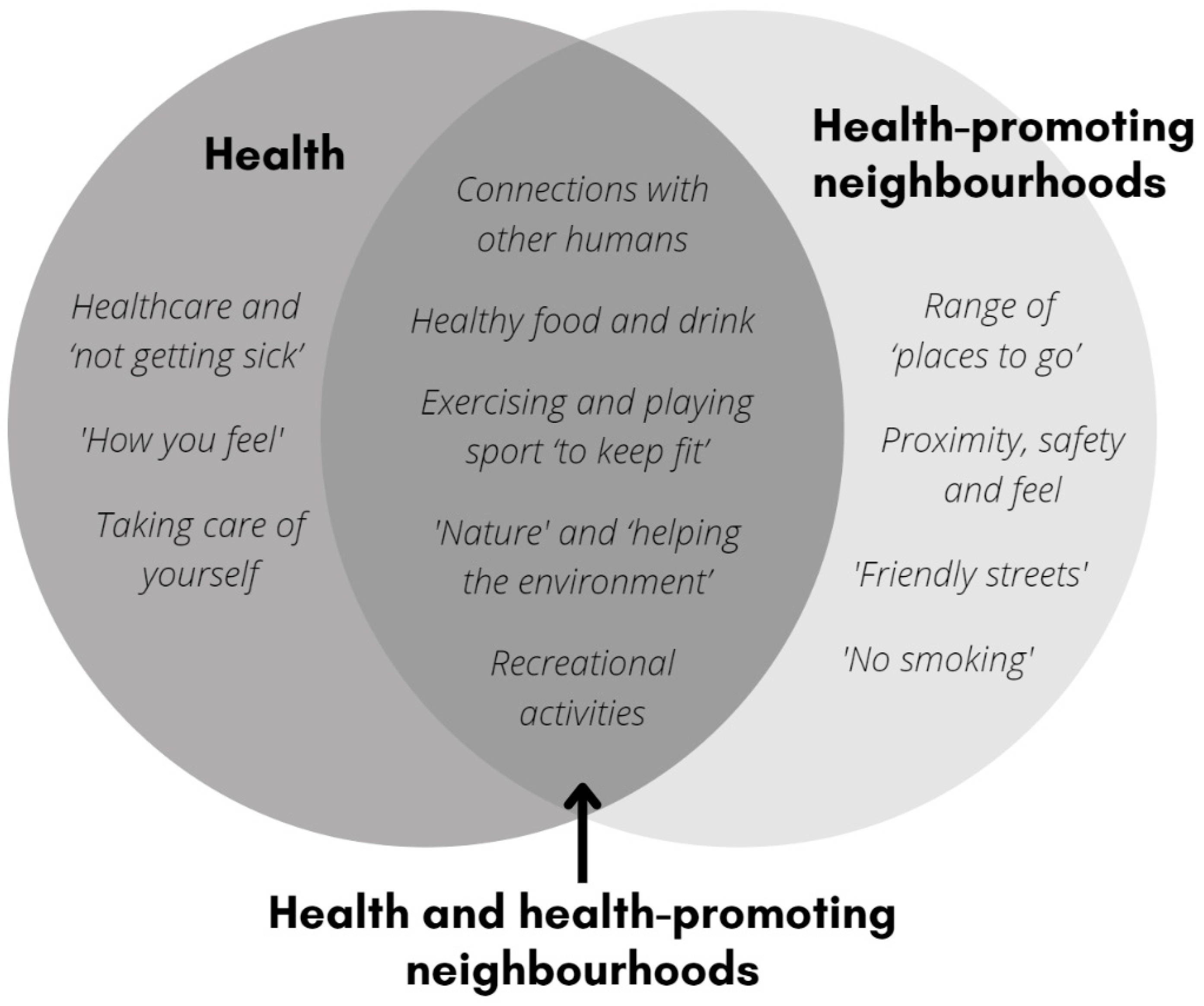
3.3. Children’s Perceptions of Health
3.3.1. Connections with Other Humans
3.3.2. Healthy Food and Drink
3.3.3. Exercising and Playing Sport ‘to Keep Fit’
3.3.4. ‘Nature’ and ‘Helping the Environment’
3.3.5. Recreational Activities
3.3.6. Healthcare and ‘Not Getting Sick’
3.3.7. ‘How You Feel’
3.3.8. Taking Care of Yourself
3.4. Children’s Perceptions of Health-Promoting Neighbourhoods
3.4.1. Connections with Other Humans
3.4.2. Healthy Food and Drink
3.4.3. Exercising and Playing Sport ‘to Keep Fit’
3.4.4. ‘Nature’ and ‘Helping the Environment’
3.4.5. Recreational Activities
3.4.6. Proximity, Safety, and Feel
3.4.7. Range of ‘Places to Go’
3.4.8. ‘Friendly Streets’
3.4.9. ‘No Smoking’
3.5. Co-Created Outputs for Health-Promoting Neighbourhoods
4. Discussion
4.1. Children’s More-Than-Human Thinking
4.2. Implications of Neighbourhoods and Health Study Results
4.3. Reflexive Account of the Research Process
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hunleth, J.M.; Spray, J.S.; Meehan, C.; Lang, C.W.; Njelesani, J. What is the state of children’s participation in qualitative research on health interventions?: A scoping study. BMC Pediatr. 2022, 22, 328. [Google Scholar] [CrossRef] [PubMed]
- Maller, C. Healthy Urban Environments: More-than-Human Theories; Routledge: London, UK, 2018. [Google Scholar]
- Egli, V.; Mandic, S.; Pocock, T.; Narayanan, A.; Williams, L.; Clark, T.; Spasic, L.; Wilson, A.; Witten, K.; Smith, M.; et al. Understanding children’s perceptions of, and priorities for, healthy neighbourhoods in Aotearoa New Zealand: Study protocol for a cross-sectional study. BMJ Open 2021, 11, e047368. [Google Scholar] [CrossRef] [PubMed]
- OHCHR. Convention on the Rights of the Child. Available online: https://www.ohchr.org/en/professionalinterest/pages/crc.aspx (accessed on 7 September 2021).
- Archard, D. Children: Rights and Childhood, 1st ed.; Routledge: London, UK, 1993. [Google Scholar]
- Archard, D. Children: Rights and Childhood, 3rd ed.; Routledge: London, UK, 2015. [Google Scholar]
- UNICEF. What Is the Child Friendly Cities Initiative? Available online: https://childfriendlycities.org/what-is-the-child-friendly-cities-initiative/ (accessed on 9 February 2022).
- Alderson, P. Rights-respecting research: A commentary on ‘the right to be properly researched: Research with children in a messy, real world’, Children’s Geographies, 2009, 7, 4. Child. Geogr. 2012, 10, 233–239. [Google Scholar] [CrossRef]
- Horgan, D.; Forde, C.; Martin, S.; Parkes, A. Children’s participation: Moving from the performative to the social. Child. Geogr. 2017, 15, 274–288. [Google Scholar] [CrossRef]
- Spray, J. Towards a child-centred public health: Lessons from rheumatic fever prevention in Aotearoa New Zealand. Child. Soc. 2020, 34, 552–566. [Google Scholar] [CrossRef]
- Williams, T.; Ward, K.; Smith, M. Conceptualization of Co-Creation, Co-Design and Co-Production with Children for Health-Promoting Physical Environments: A Systematic Search and Scoping Review; University of Auckland: Auckland, New Zealand, 2022. [Google Scholar]
- Ataol, Ö.; Krishnamurthy, S.; van Wesemael, P. Children’s Participation in Urban Planning and Design: A Systematic Review. Child. Youth Environ. 2019, 29, 27–47. [Google Scholar] [CrossRef]
- James, A.; Prout, A. Constructing and Reconstructing Childhood: Contemporary Issues in the Sociological Study of Childhood; Falmer Press: New York, NY, USA, 1990. [Google Scholar]
- James, A.; Prout, A. A new paradigm for the sociology of childhood? Provenance, promise and problems. In Constructing and Reconstructing Childhood Contemporary Issues in the Sociological Study of Childhood, 3rd ed.; Taylor and Francis: Hoboken, NJ, USA, 2015. [Google Scholar]
- Spyrou, S. The limits of children’s voices: From authenticity to critical, reflexive representation. Childhood 2011, 18, 151–165. [Google Scholar] [CrossRef] [Green Version]
- Spencer, G.; Fairbrother, H.; Thompson, J. Privileges of Power: Authenticity, Representation and the “Problem” of Children’s Voices in Qualitative Health Research. Int. J. Qual. Methods 2020, 19, 1609406920958597. [Google Scholar] [CrossRef]
- Strengers, Y.; Maller, C. Dynamic Non-humans in a Changing World. In Social Practices and Dynamic Non-Humans: Nature, Materials and Technologies; Strengers, Y., Maller, C., Eds.; Springer: Cham, Switzerland, 2019; pp. 1–21. [Google Scholar]
- Castree, N. Environmental issues: Relational ontologies and hybrid politics. Prog. Hum. Geogr. 2003, 27, 202–211. [Google Scholar] [CrossRef]
- Braun, B. Environmental issues: Writing a more-than-human urban geography. Prog. Hum. Geogr. 2005, 29, 635–650. [Google Scholar] [CrossRef]
- Braun, B.; Whatmore, S.J. (Eds.) The Stuff of Politics: An Introduction. In Political Matter: Technoscience, Democracy, and Public Life; University of Minnesota Press: Minneapolis, MN, USA, 2010; pp. ix–xl. [Google Scholar]
- Ergler, C.R.; Freeman, C.; Guiney, T. Walking with preschool-aged children to explore their local wellbeing affordances. Geogr. Res. 2021, 59, 118–135. [Google Scholar] [CrossRef]
- Burrows, L.; Wright, J.; McCormack, J. Dosing up on food and physical activity: New Zealand children’s ideas about ‘health’. Health Educ. J. 2009, 68, 157–169. [Google Scholar] [CrossRef]
- Mengwasser, E.; Walton, M. ‘Show me what health means to you!’–Exploring children’s perspectives of health. Pastor. Care Educ. 2012, 31, 4–14. [Google Scholar] [CrossRef]
- King, P.T.; Cormack, D. ‘It feels special when you’re Māori’—Voices of mokopuna Māori aged 6 to 13 years. J. R. Soc. N. Z. 2022, 52, 376–395. [Google Scholar] [CrossRef]
- Oliver, M.; Witten, K.; Kearns, R.A.; Mavoa, S.; Badland, H.M.; Carroll, P.; Drumheller, C.; Tavae, N.; Asiasiga, L.; Jelley, S.; et al. Kids in the city study: Research design and methodology. BMC Public Health 2011, 11, 587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, P.; Witten, K.; Kearns, R.; Donovan, P. Kids in the City: Children’s Use and Experiences of Urban Neighbourhoods in Auckland, New Zealand. J. Urban Des. 2015, 20, 417–436. [Google Scholar] [CrossRef]
- Chaudhury, M.; Hinckson, E.; Badland, H.; Oliver, M. Children’s independence and affordances experienced in the context of public open spaces: A study of diverse inner-city and suburban neighbourhoods in Auckland, New Zealand. Child. Geogr. 2019, 17, 49–63. [Google Scholar] [CrossRef]
- Carroll, P.; Calder-Dawe, O.; Witten, K.; Asiasiga, L. A Prefigurative Politics of Play in Public Places: Children Claim Their Democratic Right to the City Through Play. Space Cult. 2019, 22, 294–307. [Google Scholar] [CrossRef]
- Oliver, M.; McPhee, J.; Carroll, P.; Ikeda, E.; Mavoa, S.; Mackay, L.; Kearns, R.A.; Kytta, M.; Asiasiga, L.; Garrett, N.; et al. Neighbourhoods for Active Kids: Study protocol for a cross-sectional examination of neighbourhood features and children’s physical activity, active travel, independent mobility and body size. BMJ Open 2016, 6, e013377. [Google Scholar] [CrossRef] [Green Version]
- Egli, V.; Villanueva, K.; Donnellan, N.; Mackay, L.; Forsyth, E.; Zinn, C.; Kytta, M.; Smith, M. Understanding children’s neighbourhood destinations: Presenting the Kids-PoND framework. Child. Geogr. 2020, 18, 420–434. [Google Scholar] [CrossRef]
- Egli, V.; Mackay, L.; Jelleyman, C.; Ikeda, E.; Hopkins, S.; Smith, M. Social relationships, nature, and traffic: Findings from a child-centred approach to measuring active school travel route perceptions. Child. Geogr. 2020, 18, 667–683. [Google Scholar] [CrossRef]
- Ergler, C.R.; Kearns, R.A.; Witten, K. Seasonal and locational variations in children’s play: Implications for wellbeing. Soc. Sci. Med. 2013, 91, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Freeman, C.; van Heezik, Y.; Hand, K.; Stein, A. Making Cities More Child- and Nature-Friendly: A Child-Focused Study of Nature Connectedness in New Zealand Cities. Child. Youth Environ. 2015, 25, 176–207. [Google Scholar] [CrossRef]
- Ergler, C.R.; Freeman, C.; Guiney, T. Pre-Schoolers’ Vision for Liveable Cities: Creating ‘Care-Full’ Urban Environments. Tijdschr. Voor Econ. En Soc. Geogr. 2022, 113, 131–150. [Google Scholar] [CrossRef]
- Stats NZ Tatauranga Aotearoa. 2018 Census Place Summaries. Available online: https://www.stats.govt.nz/tools/2018-census-place-summaries/ (accessed on 20 October 2022).
- Carroll, P.; Witten, K.; Smith, M.; Egli, V.; Mavoa, S.; Kytta, M. Conducting Research with Children, Ethically and Effectively, to Inform Public Policy. In Ethics and Integrity in Research with Children and Young People; Advances in Research Ethics and Integrity; Ringgold Inc.: Beaverton, OR, USA, 2021; pp. 167–182. [Google Scholar]
- Connelly, L.M.; Peltzer, J.N. Underdeveloped Themes in Qualitative Research: Relationship with Interviews and Analysis. Clin. Nurse Spec. 2016, 30, 52–57. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; Sage Publications: London, UK, 2021. [Google Scholar]
- Smith, M.; Spender, G.; Fouché, C.; Hoare, K. Understanding child and youth migrant wellbeing: Reflections from a systematic literature review in the Western Pacific region. Wellbeing Space Soc. 2021, 2, 100053. [Google Scholar] [CrossRef]
- Freeman, C.; Ergler, C.; Guiney, T. Planning with Preschoolers: City Mapping as a Planning Tool. Plan. Pract. Res. 2017, 32, 297–318. [Google Scholar] [CrossRef]
- Carroll, P.; Witten, K.; Asiasiga, L.; Lin, E.-Y. Children’s Engagement as Urban Researchers and Consultants in Aotearoa/New Zealand: Can it Increase Children’s Effective Participation in Urban Planning? Child. Soc. 2019, 33, 414–428. [Google Scholar] [CrossRef]
- Sullivan, E.; Egli, V.; Donnellan, N.; Smith, M. Policies to enable children’s voice for healthy neighbourhoods and communities: A systematic mapping review and case study. Kōtuitui N. Z. J. Soc. Sci. Online 2020, 1, 18–44. [Google Scholar] [CrossRef]
- Bosco, F.J.; Joassart-Marcelli, P. Participatory planning and children’s emotional labor in the production of urban nature. Emot. Space Soc. 2015, 16, 30–40. [Google Scholar] [CrossRef]
- Schoeppich, A.; Koller, D.; McLaren, C. Children’s Right to Participate in Playground Development: A Critical Review. Child. Youth Environ. 2021, 31, 1–25. [Google Scholar] [CrossRef]
- Lundy, L. ‘Voice’ is not enough: Conceptualising Article 12 of the United Nations Convention on the Rights of the Child. Br. Educ. Res. J. 2007, 33, 927–942. [Google Scholar] [CrossRef]
- Komulainen, S. The ambiguity of the child’s ‘voice’ in social research. Childhood 2007, 14, 11–28. [Google Scholar] [CrossRef]
- Freeman, C.; Ergler, C.R.; Kearns, R.; Smith, M. COVID-19 in New Zealand and the Pacific: Implications for children and families. Child. Geogr. 2022, 20, 459–468. [Google Scholar] [CrossRef]
- Smith, M.; Donnellan, N.; Zhao, J.; Egli, V.; Ma, C.; Clark, T. Children’s perceptions of their neighbourhoods during COVID-19 lockdown in Aotearoa New Zealand. Child. Geogr. 2022, 1–15. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, T.; Ward, K.; Egli, V.; Mandic, S.; Pocock, T.; Clark, T.C.; Smith, M. More-Than-Human: A Cross-Sectional Study Exploring Children’s Perceptions of Health and Health-Promoting Neighbourhoods in Aotearoa New Zealand. Int. J. Environ. Res. Public Health 2022, 19, 16968. https://doi.org/10.3390/ijerph192416968
Williams T, Ward K, Egli V, Mandic S, Pocock T, Clark TC, Smith M. More-Than-Human: A Cross-Sectional Study Exploring Children’s Perceptions of Health and Health-Promoting Neighbourhoods in Aotearoa New Zealand. International Journal of Environmental Research and Public Health. 2022; 19(24):16968. https://doi.org/10.3390/ijerph192416968
Chicago/Turabian StyleWilliams, Tiffany, Kim Ward, Victoria Egli, Sandra Mandic, Tessa Pocock, Terryann C. Clark, and Melody Smith. 2022. "More-Than-Human: A Cross-Sectional Study Exploring Children’s Perceptions of Health and Health-Promoting Neighbourhoods in Aotearoa New Zealand" International Journal of Environmental Research and Public Health 19, no. 24: 16968. https://doi.org/10.3390/ijerph192416968
APA StyleWilliams, T., Ward, K., Egli, V., Mandic, S., Pocock, T., Clark, T. C., & Smith, M. (2022). More-Than-Human: A Cross-Sectional Study Exploring Children’s Perceptions of Health and Health-Promoting Neighbourhoods in Aotearoa New Zealand. International Journal of Environmental Research and Public Health, 19(24), 16968. https://doi.org/10.3390/ijerph192416968