
Examining the Association between Sports Participation and Mental Health of Adolescents

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Quantitative Examination
2.1.1. Participants
2.1.2. Outcome Measures
2.1.3. Study Factors
2.1.4. Covariates
2.1.5. Data Analysis
2.2. Qualitative Exploration
2.2.1. Participants
2.2.2. Procedure
2.2.3. Data Management and Analysis
3. Results
3.1. Quantitative Findings
3.2. Qualitative Findings
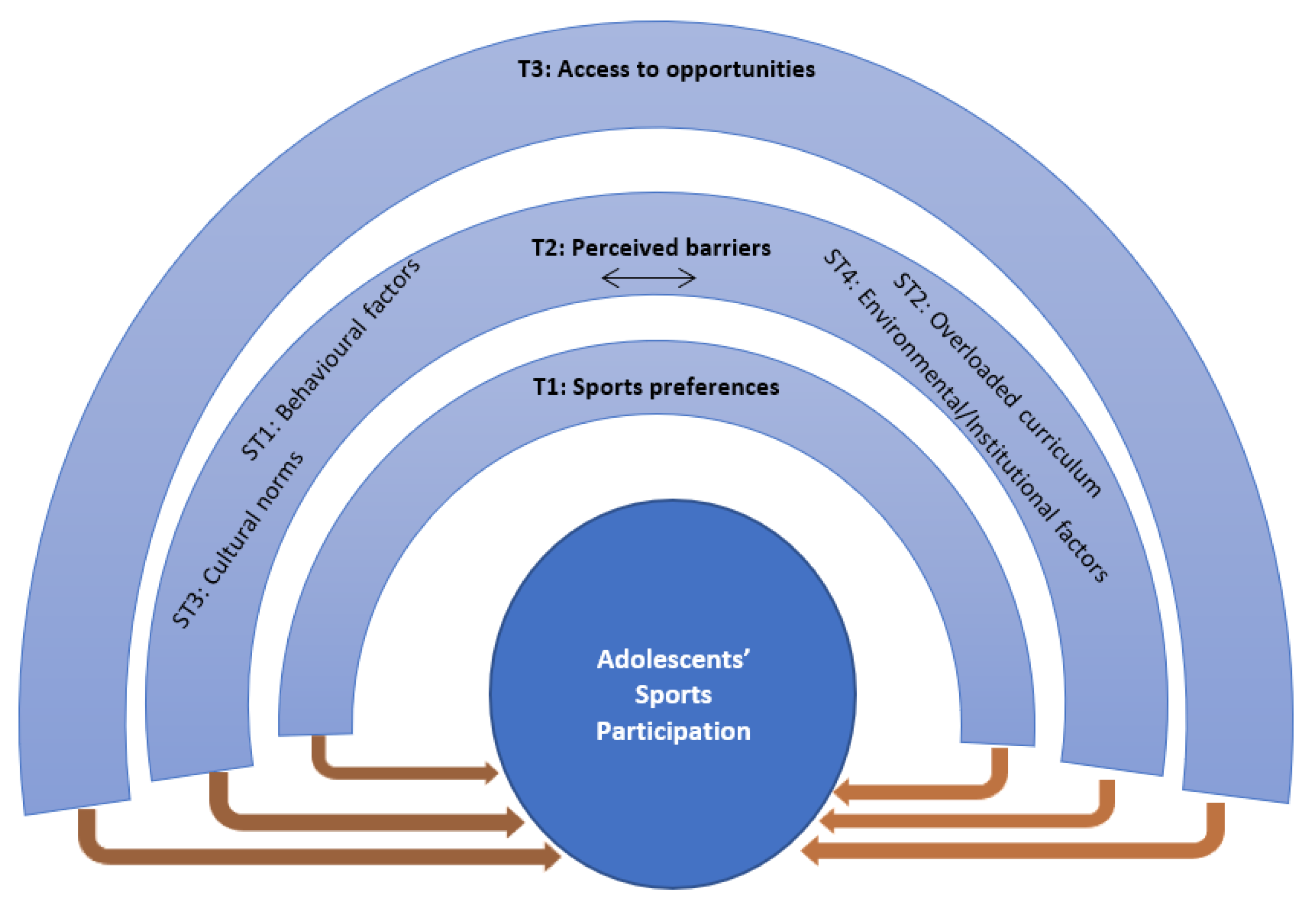
3.2.1. Theme 1: Sports Preferences
3.2.2. Theme 2: Perceived Barriers
- Subtheme 1: Behavioral factors. Participants stated that behavioral factors, such as laziness, timidity, and fear of accidents, were barriers for sport participation. Few participants reported spending leisure time on computers with their siblings at home. Boys mentioned a preference for watching television and video games, while girls preferred using mobile phones over sports. Girls also reported spending a lot of time on social media and screen-based activities, which reduced time for play. Girls also felt that they had fewer sports options available at home that encouraged them to use digital screens.
“Our friends are passing their time at home involving with new projectors, computer games, mobile game, Facebook. Therefore, they could not manage time for playing sports.”(Girls, Focus Group 2)
“Our laziness may be the reasons for not playing sports. There is assembly in schools but many of my friends are reluctant to join the assembly despite reminding them. We simply can’t accuse schools for not creating opportunities ….”(Girls, Focus Group 1)
- Subtheme 2: Overloaded curriculum. Participants reported high academic pressure as one of the main barriers to sports participation. They stated after-school activities usually consisted of homework followed by unstructured behaviors, such as television viewing or using a mobile phone. In addition to attending academic activities at school, students described needing to attend after-school private tutoring and other extra-curricular (non-sports) activities, such as playing music and singing. As such, students reported no time to engage in indoor or outdoor sports activities. High academic pressure was also reported to increase their stress, which was sometimes managed by using social media.
“The biggest reason for not participating in any sports is that we do not get sufficient time after school. Because of coaching and tuition at home, helping family for chores, we do not get time to play.”(Girls, Focus Group 1)
“We go for private tuition/coaching after school. Then we read ourselves at home.”(Boys, Focus Group 2)
- Subtheme 3: Cultural norms. Sociocultural barriers to not engage in any sports are more prevalent among girls than boys. Girls reported that they have many restrictions on their movements and often are not allowed to go out for play. For example, lack of family support and domestic responsibilities (e.g., household chores) were reported as barriers to engage in sport. Girls also reported not having enough places to play indoors. Instead of going out for sports, a few participants described that they spent time on their smartphones talking or chatting with friends. Some girls stated that a culture of outdoor sports is not common in their society.
“Parents prohibit us. I mean they don’t allow us to go out and play…. Not even in the rooftop.”(Girls, Focus Group 1)
“We grew up, parents do not let us go out. There are many boys out there who can disturb, they do not want to allow us to play as we are girls.”(Girls, Focus Group 2)
“Our life has become a captive life as grow up ….. parents don’t allow us to go out in on order to protect us from being bullied by street boys and also to follow the tradition of the society.”(Girls, Focus Group 1)
- Subtheme 4: Environmental/institutional factors. The lack of facilities at schools and after school seemed to affect the engagement of adolescents in sports participation. Some adolescents reported difficulties engaging in sports in school due to limited sport facilities (e.g., lack of playground, sports equipment), short recess time, sports day only once a year, and limited after-school activities.
“Recess time is too short. So, we do not get any time to play.” (Girls, Focus Group 1)(Girls, Focus Group 1)
“We usually eat by talking and sitting in the classroom for our short recess time.”(Boys, Focus Group 2)
“Activity is done one day a week…Monday. We are given ideas of physical activities from the textbook in a physical education class. We are just taught from the textbook….. No extra care is given, or opportunity is created to encourage us to participate in sports at school, and there is no value attached with participation in sports.”(Boys, Focus Group 1)
3.2.3. Theme 3: Access to Opportunities
“It would be better if physical education class would be held for two days instead of one day.”(Boys, Focus Group 2)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malm, C.; Jakobsson, J.; Isaksson, A. Physical Activity and Sports-Real Health Benefits: A Review with Insight into the Public Health of Sweden. Sports 2019, 7, 127. [Google Scholar] [CrossRef] [PubMed]
- Brière, F.N.; Yale-Soulière, G.; Gonzalez-Sicilia, D.; Harbec, M.-J.; Morizot, J.; Janosz, M. Prospective associations between sport participation and psychological adjustment in adolescents. J. Epidemiol. Community Health 2018, 72, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Soltanian, A.R.; Nabipour, I.; Akhondzadeh, S.; Moeini, B.; Bahreini, F.; Barati, M.; Faradmal, J. Association between physical activity and mental health among high-school adolescents in Boushehr province: A population based study. Iran. J. Psychiatry 2011, 6, 112–116. [Google Scholar] [PubMed]
- Sterdt, E.; Liersch, S.; Walter, U. Correlates of physical activity of children and adolescents: A systematic review of reviews. Health Educ. J. 2014, 73, 72–89. [Google Scholar] [CrossRef]
- Hopkins, C.S.; Hopkins, C.; Kanny, S.; Watson, A. A Systematic Review of Factors Associated with Sport Participation among Adolescent Females. Int. J. Environ. Res. Public Health 2022, 19, 3353. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.M.; Cromartie, F.; Butler, S.; Bae, J. Effects of Early Sport Participation on Self-esteem and Happiness. Sport. J. 2018, 20, 1–20. [Google Scholar]
- Hoffmann, M.D.; Barnes, J.D.; Tremblay, M.S.; Guerrero, M.D. Associations between organized sport participation and mental health difficulties: Data from over 11,000 US children and adolescents. PLoS ONE 2022, 17, e0268583. [Google Scholar] [CrossRef]
- Bjørnarå, H.B.; Westergren, T.; Sejersted, E.; Torstveit, M.K.; Hansen, B.H.; Berntsen, S.; Bere, E. Does organized sports participation in childhood and adolescence positively influence health? A review of reviews. Prev. Med. Rep. 2021, 23, 101425. [Google Scholar] [CrossRef]
- Panza, M.J.; Graupensperger, S.; Agans, J.P.; Doré, I.; Vella, S.A.; Evans, M.B. Adolescent sport participation and symptoms of anxiety and depression: A systematic review and meta-analysis. J. Sport. Exerc. Psychol. 2020, 42, 201–218. [Google Scholar] [CrossRef]
- Khan, K.M.; Thompson, A.M.; Blair, S.N.; Sallis, J.F.; Powell, K.E.; Bull, F.C.; Bauman, A.E. Sport and exercise as contributors to the health of nations. Lancet 2012, 380, 59–64. [Google Scholar] [CrossRef]
- YLiu, a.; Ke, Y.; Liang, Y.; Zhu, Z.; Cao, Z.; Zhuang, J.; Cai, Y.; Wang, L.; Chen, P.; Tang, Y. Results from the China 2022 report card on physical activity for children and adolescents. J. Exerc. Sci. Fit. 2023, 21, 1–5. [Google Scholar]
- Widyastari, D.A.; Saonuam, P.; Pongpradit, K.; Wongsingha, N.; Choolers, P.; Kesaro, S.; Thangchan, W.; Pongpaopattanakul, P.; Phankasem, K.; Musor, M.; et al. Results from the Thailand 2022 report card on physical activity for children and youth. J. Exerc. Sci. Fit. 2022, 20, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Schulte-Körne, G. Mental Health Problems in a School Setting in Children and Adolescents. Dtsch. Arztebl. Int. 2016, 113, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Klasen, H.; Crombag, A.-C. What works where? A systematic review of child and adolescent mental health interventions for low and middle income countries. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 595–611. [Google Scholar] [CrossRef]
- Uddin, R.; Burton, N.W.; Maple, M.; Khan, S.R.; Khan, A. Suicidal ideation, suicide planning, and suicide attempts among adolescents in 59 low-income and middle-income countries: A population-based study. Lancet Child. Adolesc. Health 2019, 3, 223–233. [Google Scholar] [CrossRef]
- Mabrouk, A.; Mbithi, G.; Chongwo, E.; Too, E.; Sarki, A.; Namuguzi, M.; Atukwatse, J.; Ssewanyana, D.; Abubakar, A. Mental health interventions for adolescents in sub-Saharan Africa: A scoping review. Front. Psychiatry 2022, 13, 937723. [Google Scholar] [CrossRef]
- Li, F.; Cui, Y.; Li, Y.; Guo, L.; Ke, X.; Liu, J.; Luo, X.; Zheng, Y.; Leckman, J.F. Prevalence of mental disorders in school children and adolescents in China: Diagnostic data from detailed clinical assessments of 17,524 individuals. J. Child. Psychol. Psychiatry 2022, 63, 34–46. [Google Scholar] [CrossRef]
- Hossain, M.D.; Ahmed, H.U.; Chowdhury, W.A.; Niessen, L.W.; Alam, D.S. Mental disorders in Bangladesh: A systematic review. BMC Psychiatry 2014, 14, 216. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, R.; Burton, N.W. Prevalence and correlates of depressive symptoms in secondary school children in Dhaka city, Bangladesh. Ethn. Health 2020, 25, 34–46. [Google Scholar] [CrossRef]
- Breaking the Silence: A Discussion on Child Mental Health in the Developing World. 15 Jun 2020. Available online: https://reliefweb.int/report/world/breaking-silence-discussion-child-mental-health-developing-world (accessed on 3 November 2022).
- Hulteen, R.M.; Smith, J.J.; Morgan, P.J.; Barnett, L.M.; Hallal, P.C.; Colyvas, K.; Lubans, D.R. Global participation in sport and leisure-time physical activities: A systematic review and meta-analysis. Prev. Med. 2016, 95, 14–25. [Google Scholar] [CrossRef]
- Anjum, A.; Hossain, S.; Hasan, M.T.; Uddin, M.E.; Sikder, M.T. Anxiety among urban, semi-urban and rural school adolescents in Dhaka, Bangladesh: Investigating prevalence and associated factors. PLoS ONE 2022, 17, e0262716. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.R.; Kolbe-Alexander, T.; Khan, A. Effectiveness of a school-based intervention on physical activity and screen time among adolescents. J. Sci. Med. Sport. 2022, 25, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Levin, K.A.; Currie, C. Reliability and validity of an adapted version of the Cantril Ladder for use with adolescent samples. Soc. Indic. Res. 2014, 119, 1047–1063. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 17. 2021; StataCorp LLC: College Station, TX, USA.
- Ibrahim, M.F.; Wan Ismail, W.S.; Nik Jaafar, N.R.; Mohd Mokhtaruddin, U.K.; Ong, H.Y.; Abu Bakar, N.H.; Mohd Salleh Sahimi, H. Depression and its association with self-esteem and lifestyle factors among school-going adolescents in Kuala Lumpur, Malaysia. Front. Psychiatry 2022, 13, 913067. [Google Scholar] [CrossRef] [PubMed]
- Perera, B.; Torabi, M.R.; Jayawardana, G.; Pallethanna, N. Depressive symptoms among adolescents in Sri Lanka: Prevalence and behavioral correlates. J. Adolesc. Health 2006, 39, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Fromel, K.; Kudlacek, M.; Groffik, D.; Svozil, Z.; Simunek, A.; Garbaciak, W. Promoting healthy lifestyle and well-being in adolescents through outdoor physical activity. Int. J. Environ. Res. Public Health 2017, 14, 533. [Google Scholar] [CrossRef]
- Lee, K.S.; Trost, S.G. Physical activity patterns of Singaporean adolescents. Pediatr. Exerc. Sci. 2006, 18, 400–414. [Google Scholar] [CrossRef]
- Knubben, K.; Reischies, F.M.; Adli, M.; Schlattmann, P.; Bauer, M.; Dimeo, F. A randomised, controlled study on the effects of a short-term endurance training programme in patients with major depression. Br. J. Sport. Med. 2007, 41, 29–33. [Google Scholar] [CrossRef]
- Nabkasorn, C.; Miyai, N.; Sootmongkol, A.; Junprasert, S.; Yamamoto, H.; Arita, M.; Miyashita, K. Effects of physical exercise on depression, neuroendocrine stress hormones and physiological fitness in adolescent females with depressive symptoms. Eur. J. Public Health 2006, 16, 179–184. [Google Scholar] [CrossRef]
- Paluska, S.A.; Schwenk, T.L. Physical activity and mental health: Current concepts. Sport. Med. 2000, 29, 167–180. [Google Scholar] [CrossRef]
- Brown, H.E.; Pearson, N.; Braithwaite, R.E.; Brown, W.J.; Biddle, S.J.H. Physical activity interventions and depression in children and adolescents: A systematic review and meta-analysis. Sport. Med. 2013, 43, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Boone, E.M.; Leadbeater, B.J. Game on: Diminishing risks for depressive symptoms in early adolescence through positive involvement in team sports. J. Res. Adolesc. 2006, 16, 79–90. [Google Scholar] [CrossRef]
- Agata, K.; Monyeki, M.A. Association between sport participation, body composition, physical fitness, and social correlates among adolescents: The PAHL study. Int. J. Environ. Res. Public Health 2018, 15, 2793. [Google Scholar] [CrossRef] [PubMed]
- Babiss, L.A.; Gangwisch, J.E. Sports participation as a protective factor against depression and suicidal ideation in adolescents as mediated by self-esteem and social support. J. Dev. Behav. Pediatr. 2009, 30, 376–384. [Google Scholar] [CrossRef]
- Jewett, R.; Sabiston, C.M.P.D.; Brunet, J.P.D.; O'Loughlin, E.K.M.A.; Scarapicchia, T.M.A.; O'Loughlin, J.P.D. School sport participation during adolescence and mental health in early adulthood. J. Adolesc. Health 2014, 55, 640–644. [Google Scholar] [CrossRef]
- Lorenzetti, V.; Allen, N.B.; Fornito, A.; Yücel, M. Structural brain abnormalities in major depressive disorder: A selective review of recent MRI studies. J. Affect. Disord. 2009, 117, 1–17. [Google Scholar] [CrossRef]
- Whitehead, S.; Biddle, S. Adolescent girls' perceptions of physical activity: A focus group study. Eur. Phys. Educ. Rev. 2008, 14, 243–262. [Google Scholar] [CrossRef]
- Slater, A.; Tiggemann, M. Gender differences in adolescent sport participation, teasing, self-objectification and body image concerns. J. Adolesc. 2011, 34, 455–463. [Google Scholar] [CrossRef]
- O'Brien, W.; Coppinger, T.; Hogan, I.; Belton, S.; Murphy, M.H.; Powell, C.; Woods, C. The association of family, friends, and teacher support with girls' sport and physical activity on the island of ireland. J. Phys. Act. Health 2021, 18, 929–936. [Google Scholar] [CrossRef]
- Dishman, R.K.; Hales, D.P.; Pfeiffer, K.A.; Felton, G.; Saunders, R.; Ward, D.S.; Dowda, M.; Pate, R.R. Physical self-concept and self-esteem mediate cross-sectional relations of physical activity and sport participation with depression symptoms among adolescent girls. Health Psychol. 2006, 25, 396–407. [Google Scholar] [CrossRef]
- Pedersen, S.; Seidman, E. Team sports achievement and self-esteem development among urban adolescent girls. Psychol. Women Q. 2004, 28, 412–422. [Google Scholar] [CrossRef]
- Badura, P.; Geckova, A.M.; Sigmundova, D.; Van Dijk, J.P.; Reijneveld, S.A. When children play, they feel better: Organized activity participation and health in adolescents Energy balance-related behaviors. BMC Public Health 2015, 15, 1090. [Google Scholar] [CrossRef] [PubMed]
- Kvaskova, L.; Recka, K.; Jezek, S.; Macek, P. Time spent on daily activities and its association with life satisfaction among Czech adolescents from 1992 to 2019. Int. J. Environ. Res. Public Health 2022, 19, 9422. [Google Scholar] [CrossRef] [PubMed]
- Pierannunzio, D.; Spinelli, A.; Berchialla, P.; Borraccino, A.; Charrier, L.; Dalmasso, P.; Lazzeri, G.; Vieno, A.; Ciardullo, S.; Nardone, P. Physical activity among Italian adolescents: Association with life satisfaction, self-rated health and peer relationships. Int. J. Environ. Res. Public Health 2022, 19, 4799. [Google Scholar] [CrossRef]
- Meyer, S.; Grob, A.; Gerber, M. No fun, no gain: The stress-buffering effect of physical activity on life satisfaction depends on adolescents' intrinsic motivation. Psychol. Sport Exerc. 2021, 56, 102004. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Depressive Symptoms | Life Satisfaction | ||
|---|---|---|---|---|
| Boys | Girls | Boys | Girls | |
| β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | |
| Involved with team sports | −1.22 (−2.55, −0.10) | −2.44 (−4.63, −0.24) | 1.72 (1.04, 2.40) | 1.47 (0.38, 2.57) |
| Involved with non-team sports | −2.50 (−3.83, −1.16) | 0.75 (−1.41, 2.91) | 1.63 (0.92, 2.34) | 1.09 (0.6, 2.12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, A.; Ahmed, K.R.; Hidajat, T.; Kolbe-Alexander, T.; Edwards, E.J. Examining the Association between Sports Participation and Mental Health of Adolescents. Int. J. Environ. Res. Public Health 2022, 19, 17078. https://doi.org/10.3390/ijerph192417078
Khan A, Ahmed KR, Hidajat T, Kolbe-Alexander T, Edwards EJ. Examining the Association between Sports Participation and Mental Health of Adolescents. International Journal of Environmental Research and Public Health. 2022; 19(24):17078. https://doi.org/10.3390/ijerph192417078
Chicago/Turabian StyleKhan, Asaduzzaman, Kazi R. Ahmed, Tarissa Hidajat, Tracy Kolbe-Alexander, and Elizabeth J. Edwards. 2022. "Examining the Association between Sports Participation and Mental Health of Adolescents" International Journal of Environmental Research and Public Health 19, no. 24: 17078. https://doi.org/10.3390/ijerph192417078
APA StyleKhan, A., Ahmed, K. R., Hidajat, T., Kolbe-Alexander, T., & Edwards, E. J. (2022). Examining the Association between Sports Participation and Mental Health of Adolescents. International Journal of Environmental Research and Public Health, 19(24), 17078. https://doi.org/10.3390/ijerph192417078