
Artificial Intelligence Enabled Personalised Assistive Tools to Enhance Education of Children with Neurodevelopmental Disorders—A Review

 ,
,  , ,
, , 
Abstract
:1. Introduction
1.1. Mental Disorders
1.1.1. ADHD
1.1.2. Dyslexia
1.1.3. Autism Spectrum Disorders
1.2. Personalised Assistive Tools Using Artificial Intelligence for Children with NDD
2. Current Management Approaches for Children with NDD
2.1. Individualised Educational Approaches for a Child with ADHD
2.2. Individualised Educational Approaches for Children with Dyslexia
2.3. Teaching Support in Schools for Students with ASDs
2.4. Challenges in Implementing Individualised Learning Approaches in Schools
2.5. Use of Artificial Intelligence in Therapies and Supportive Education of Children with Mental Disorders
2.5.1. Conventional Methods Using AI
2.5.2. Advanced Methods Using AI
2.5.3. Importance of AI in Therapies and Supportive Education
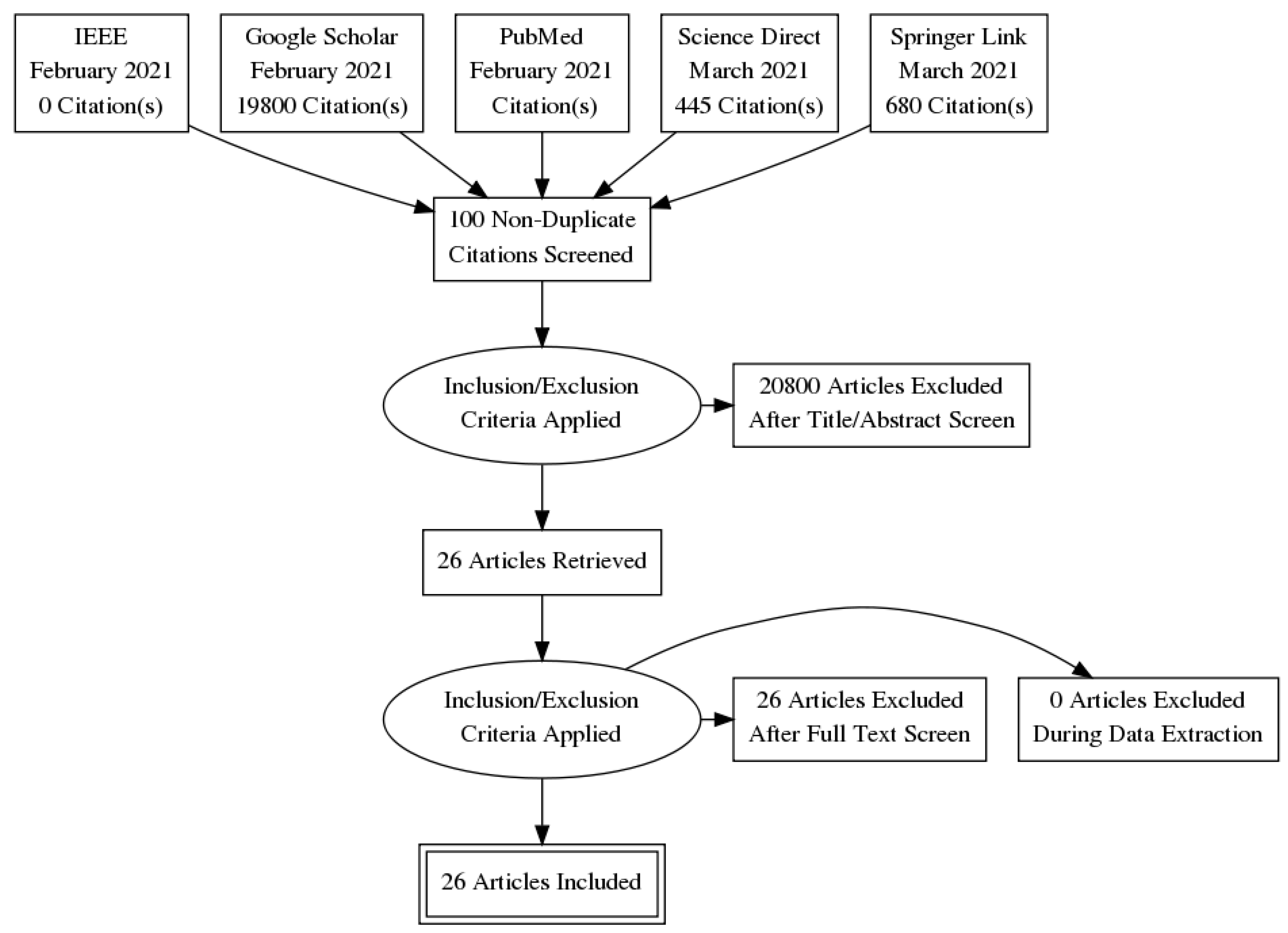
3. Materials and Methods
- They described the use of AI tools to help students with ADHD, Dyslexia and/or ASD in their learning:
- They were published between the years 2011 and 2021.
- They were published in a peer-reviewed journal.
- They were published in English.
- They described the use of AI tools to help students with other disorders apart from the NDDs ADHD, dyslexia and/or ASD.
- The article was not published in English.
- The article was not published in a peer-reviewed journal.
- The article was published before 2011.
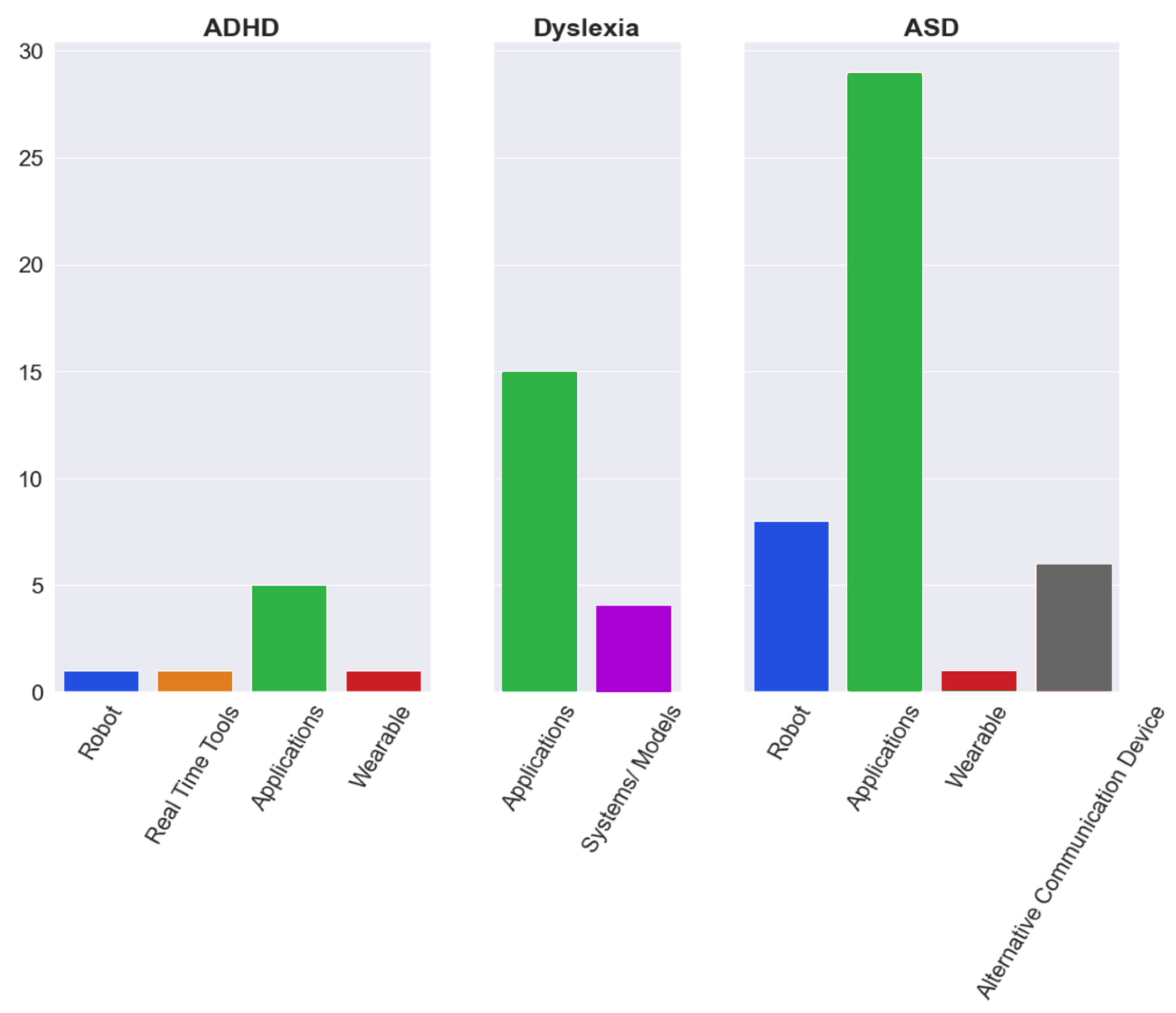
4. Results
4.1. Summary of Articles Collated
4.2. Effectiveness of AI Tools for Personalised Education
5. Discussion of Main Findings and Results of Study
5.1. Limitations of Existing AI Tools for Personalised Education
5.1.1. Suitable Datasets
5.1.2. Ethical Considerations
5.1.3. Cost of Implementing AI Tools
5.1.4. Information Loss
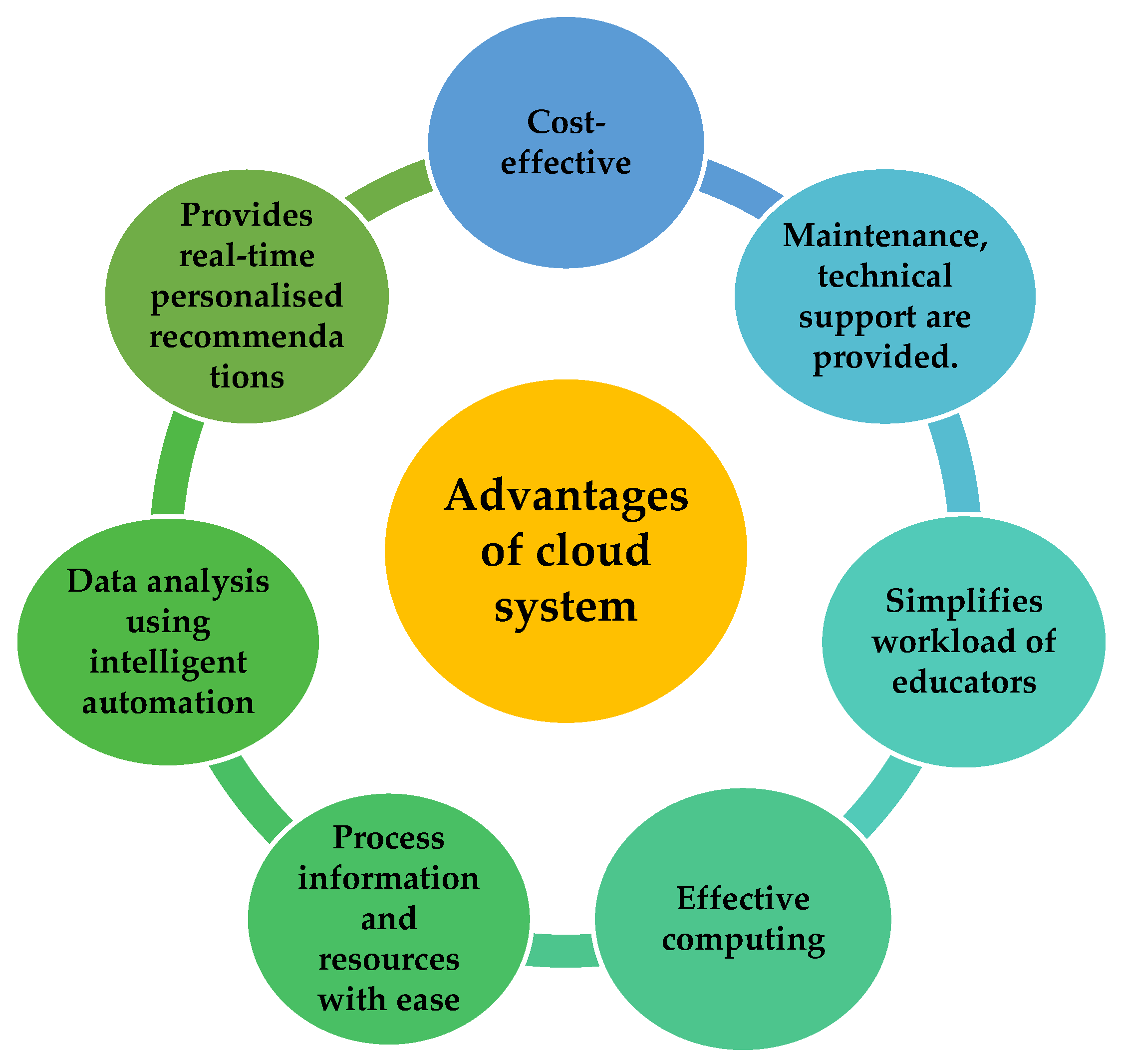
5.2. Cloud Computing in Schools
5.2.1. Advantages of Using AI in Cloud Computing
5.2.2. Disadvantages of Using AI in Cloud Computing
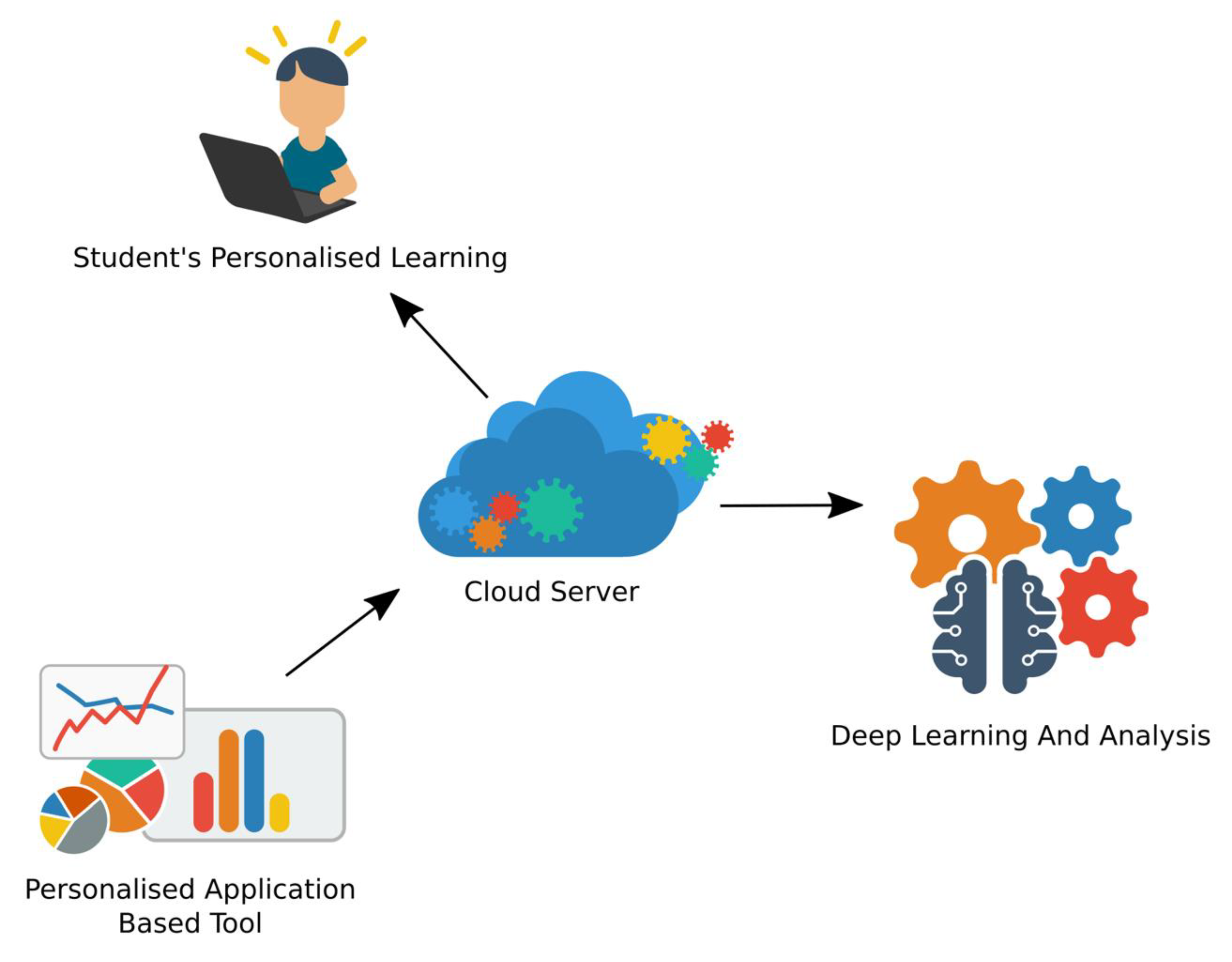
6. Proposal for a Future AI Tool
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- Jeste, S. Neurodevelopmental Behavioral and Cognitive Disorders. Contin. Lifelong Learn. Neurol. 2015, 21, 690–714. [Google Scholar] [CrossRef] [PubMed]
- Renemane, L.; Kivite-Urtane, A.; Rancans, E. Suicidality and Its Relation with Physical and Mental Conditions: Results from a Cross-Sectional Study of the Nationwide Primary Care Population Sample in Latvia. Medicina 2021, 57, 970. [Google Scholar] [CrossRef] [PubMed]
- Nepon, J.; Belik, S.-L.; Bolton, J.; Sareen, J. The relationship between anxiety disorders and suicide attempts: Findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress. Anxiety 2010, 27, 791–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Jitender, S.; Afifi, T.O.; Shay-Lee, B.; Johnson, E.A.; Bolton, J.M. Recent Stressful Life Events and Suicide Attempt. Psychiatr. Ann. 2012, 42, 101–108. [Google Scholar] [CrossRef]
- Foley, D.L.; Goldston, D.B.; Costello, E.J.; Angold, A. Proximal Psychiatric Risk Factors for Suicidality in Youth: The Great Smoky Mountains Study. Arch. Gen. Psychiatry 2006, 63, 1017–1024. [Google Scholar] [CrossRef]
- Oerbeck, B.; Overgaard, K.R.; Aspenes, S.T.; Pripp, A.H.; Mordre, M.; Aase, H.; Reichborn-Kjennerud, T.; Zeiner, P. ADHD, comorbid disorders and psychosocial functioning: How representative is a child cohort study? Findings from a national patient registry. BMC Psychiatry 2017, 17, 23. [Google Scholar] [CrossRef] [Green Version]
- Jensen, C.M.; Steinhausen, H.-C. Comorbid mental disorders in children and adolescents with attention-deficit/hyperactivity disorder in a large nationwide study. Atten. Defic. Hyperact. Disord. 2015, 7, 27–38. [Google Scholar] [CrossRef]
- Mattila, M.-L.; Hurtig, T.; Haapsamo, H.; Jussila, K.; Kuusikko-Gauffin, S.; Kielinen, M.; Linna, S.-L.; Ebeling, H.; Bloigu, R.; Joskitt, L.; et al. Comorbid Psychiatric Disorders Associated with Asperger Syndrome/High-functioning Autism: A Community- and Clinic-based Study. J. Autism Dev. Disord. 2010, 40, 1080–1093. [Google Scholar] [CrossRef]
- Gjevik, E.; Eldevik, S.; Fjæran-Granum, T.; Sponheim, E. Kiddie-SADS Reveals High Rates of DSM-IV Disorders in Children and Adolescents with Autism Spectrum Disorders. J. Autism Dev. Disord. 2010, 41, 761–769. [Google Scholar] [CrossRef] [Green Version]
- Yerys, B.E.; Wallace, G.; Sokoloff, J.L.; Shook, D.A.; James, J.D.; Kenworthy, L. Attention deficit/hyperactivity disorder symptoms moderate cognition and behavior in children with autism spectrum disorders. Autism Res. 2009, 2, 322–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, B.H.; Oerbeck, B.; Skirbekk, B.; Petrovski, B.É.; Kristensen, H. Neurodevelopmental disorders: Prevalence and comorbidity in children referred to mental health services. Nord. J. Psychiatry 2018, 72, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, R. Mental Illness in Children: Childhood Illness and Supporting the Family. Brain Sci. 2017, 7, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danielson, M.; Bitsko, R.H.; Ghandour, R.M.; Holbrook, J.R.; Kogan, M.D.; Blumberg, S.J. Prevalence of Parent-Reported ADHD Diagnosis and Associated Treatment Among U.S. Children and Adolescents, 2016. J. Clin. Child Adolesc. Psychol. 2018, 47, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Akutagava-Martins, G.C.; Rohde, L.A.; Hutz, M.H. Genetics of attention-deficit/hyperactivity disorder: An update. Expert Rev. Neurother. 2016, 16, 145–156. [Google Scholar] [CrossRef]
- Linnet, K.M.; Dalsgaard, S.; Obel, C.; Wisborg, K.; Henriksen, T.B.; Rodriguez, A.; Kotimaa, A.; Moilanen, I.; Thomsen, P.H.; Olsen, J.; et al. Maternal Lifestyle Factors in Pregnancy Risk of Attention Deficit Hyperactivity Disorder and Associated Behaviors: Review of the Current Evidence. Am. J. Psychiatry 2003, 160, 1028–1040. [Google Scholar] [CrossRef] [PubMed]
- Levin, H.; Hanten, G.; Max, J.; Li, X.; Swank, P.; Ewing-Cobbs, L.; Dennis, M.; Menefee, D.S.; Schachar, R. Symptoms of Attention-Deficit/Hyperactivity Disorder Following Traumatic Brain Injury in Children. J. Dev. Behav. Pediatr. 2007, 28, 108–118. [Google Scholar] [CrossRef]
- Hesdorffer, D.C.; Ludvigsson, P.; Olafsson, E.; Gudmundsson, G.; Kjartansson, O.; Hauser, W.A. ADHD as a risk factor for incident unprovoked seizures and epilepsy in children. Arch. Gen. Psychiatry 2004, 61, 731–736. [Google Scholar] [CrossRef]
- Sridhar, C.; Bhat, S.; Acharya, U.R.; Adeli, H.; Bairy, G.M. Diagnosis of attention deficit hyperactivity disorder using imaging and signal processing techniques. Comput. Biol. Med. 2017, 88, 93–99. [Google Scholar] [CrossRef]
- Koh, J.; Ooi, C.P.; Lim-Ashworth, N.S.; Vicnesh, J.; Tor, H.T.; Lih, O.S.; Tan, R.-S.; Acharya, U.; Fung, D.S.S. Automated classification of attention deficit hyperactivity disorder and conduct disorder using entropy features with ECG signals. Comput. Biol. Med. 2021, 140, 105120. [Google Scholar] [CrossRef]
- Biederman, J.; Monuteaux, M.C.; Mick, E.; Spencer, T.; Wilens, T.E.; Silva, J.M.; Snyder, L.E.; Faraone, S.V. Young adult outcome of attention deficit hyperactivity disorder: A controlled 10-year follow-up study. Psychol. Med. 2006, 36, 167–179. [Google Scholar] [CrossRef]
- DuPaul, G.J.; Gormley, M.J.; Laracy, S.D. Comorbidity of LD and ADHD: Implications of DSM-5 for Assessment and Treatment. J. Learn. Disabil. 2013, 46, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Snowling, M.J.; Gooch, D.C.; Henderson, L.M. Dyslexia. In Encyclopedia of Human Behavior, 2nd ed.; Ramachandran, Ed.; Academic Press: San Diego, CA, USA, 2012; pp. 732–739. [Google Scholar]
- Tsampalas, E.; Dimitrios, S.; Papadimitropoulou, P.; Vergou, M.; Zakopoulou, V. Learning Paths and Learning Styles in Dyslexia: Possibilites and Effectiveness—Case Study of Two Elementary School Students Aged 7 Years Old. Eur. J. Spec. Educ. Res. 2018, 3, 25–41. [Google Scholar]
- Perrachione, T.K.; Del Tufo, S.; Winter, R.; Murtagh, J.; Cyr, A.; Chang, P.; Halverson, K.; Ghosh, S.; Christodoulou, J.A.; Gabrieli, J.D. Dysfunction of Rapid Neural Adaptation in Dyslexia. Neuron 2016, 92, 1383–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, S.; Gillberg, C. Swedish child and adolescent psychiatric out-patients: A five-year cohort. Eur. Child Adolesc. Psychiatry 2003, 12, 30–35. [Google Scholar] [CrossRef]
- Baygin, M.; Dogan, S.; Tuncer, T.; Barua, P.D.; Faust, O.; Arunkumar, N.; Abdulhay, E.W.; Palmer, E.E.; Acharya, U.R. Automated ASD detection using hybrid deep lightweight features extracted from EEG signals. Comput. Biol. Med. 2021, 134, 104548. [Google Scholar] [CrossRef]
- Khodatars, M.; Shoeibi, A.; Sadeghi, D.; Ghaasemi, N.; Jafari, M.; Moridian, P.; Khadem, A.; Alizadehsani, R.; Zare, A.; Kong, Y.; et al. Deep learning for neuroimaging-based diagnosis and rehabilitation of Autism Spectrum Disorder: A review. Comput. Biol. Med. 2021, 139, 104949. [Google Scholar] [CrossRef]
- Tang, G.; Gudsnuk, K.; Kuo, S.-H.; Cotrina, M.L.; Rosoklija, G.; Sosunov, A.; Sonders, M.S.; Kanter, E.; Castagna, C.; Yamamoto, A.; et al. Loss of mTOR-Dependent Macroautophagy Causes Autistic-like Synaptic Pruning Deficits. Neuron 2014, 83, 1131–1143. [Google Scholar] [CrossRef] [Green Version]
- Sharif, H.; Khan, R.A. A novel framework for automatic detection of Autism: A study on Corpus Callosum and Intracranial Brain Volume. arXiv 2019. [Google Scholar]
- Yoro, A.J.; Fourie, J.V.; Van Der Merwe, M. Learning support strategies for learners with neurodevelopmental disorders: Perspectives of recently qualified teachers. Afr. J. Disabil. 2020, 9, 561. [Google Scholar] [CrossRef] [PubMed]
- Richa, S.; Fahed, M.; Khoury, E.; Mishara, B. Suicide in Autism Spectrum Disorders. Arch. Suicide Res. 2014, 18, 327–339. [Google Scholar] [CrossRef]
- Ewe, L.P. ADHD symptoms and the teacher–student relationship: A systematic literature review. Emot. Behav. Diffic. 2018, 24, 136–155. [Google Scholar] [CrossRef]
- Henricsson, L.; Rydell, A.-M. Elementary School Children with Behavior Problems: Teacher-Child Relations and Self-Perception. A Prospective Study. Merrill-Palmer Q. 2004, 50, 111–138. [Google Scholar] [CrossRef]
- Gwernan-Jones, R.; Moore, D.A.; Cooper, P.; Russell, A.E.; Richardson, M.; Rogers, M.; Thompson-Coon, J.; Stein, K.; Ford, T.J.; Garside, R. A systematic review and synthesis of qualitative research: The influence of school context on symptoms of attention deficit hyperactivity disorder. Emot. Behav. Diffic. 2016, 21, 83–100. [Google Scholar] [CrossRef] [Green Version]
- Teaching Children With Attention Deficit Hyperactivity Disorder: Instructional Strategies and Practices; US Department of Education Office of Special Education and Rehabilitative Services: Washington, DC, USA, 2006.
- Hanover Research. Best Practices in Personalized Learning; Hanover Research: Washington, DC, USA, 2006, 2012; pp. 4–41. [Google Scholar]
- Hume, K. Visual Structure in the School Setting; Indiana Resource Centre for Asutism; Indiana University: Bloomington, IN, USA, 2011. [Google Scholar]
- Hoque, M.E. Analysis of speech properties of neurotypicals and individuals diagnosed with autism and down syndrome. In Proceedings of the ASSETS’08: The 10th International ACM SIGACCESS Conference on Computers and Accessibility, Halifax, NS, Canada, 13–15 October 2008. [Google Scholar]
- Siam, K.; Al-Natour, M. Teacher’s Differentiated Instruction Practices and Implementation Challenges for Learning Disabilities in Jordan. Int. Educ. Stud. 2016, 9, 167. [Google Scholar] [CrossRef] [Green Version]
- Pham, T.-H.; Vicnesh, J.; Wei, J.K.E.; Oh, S.L.; Arunkumar, N.; Abdulhay, E.W.; Ciaccio, E.J.; Acharya, U.R. Autism Spectrum Disorder Diagnostic System Using HOS Bispectrum with EEG Signals. Int. J. Environ. Res. Public Heal. 2020, 17, 971. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.L.; Jahmunah, V.; Arunkumar, N.; Abdulhay, E.W.; Gururajan, R.; Adib, N.; Ciaccio, E.J.; Cheong, K.H.; Acharya, U.R. A novel automated autism spectrum disorder detection system. Complex Intell. Syst. 2021, 7, 2399–2413. [Google Scholar] [CrossRef]
- Dubreuil-Vall, L.; Ruffini, G.; Camprodon, J.A. Deep Learning Convolutional Neural Networks Discriminate Adult ADHD From Healthy Individuals on the Basis of Event-Related Spectral EEG. Front. Neurosci. 2020, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tor, H.T.; Ooi, C.P.; Lim-Ashworth, N.S.; Wei, J.K.E.; Jahmunah, V.; Oh, S.L.; Acharya, U.R.; Fung, D.S.S. Automated detection of conduct disorder and attention deficit hyperactivity disorder using decomposition and nonlinear techniques with EEG signals. Comput. Methods Programs Biomed. 2021, 200, 105941. [Google Scholar] [CrossRef]
- Acharya, U.R.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adeli, H.; Subha, D.P. Automated EEG-based screening of depression using deep convolutional neural network. Comput. Methods Programs Biomed. 2018, 161, 103–113. [Google Scholar] [CrossRef]
- He, L.; Cao, C. Automated depression analysis using convolutional neural networks from speech. J. Biomed. Inform. 2018, 83, 103–111. [Google Scholar] [CrossRef]
- Detecting Depression Using a Framework Combining Deep Multimodal Neural Networks with a Purpose-Built Automated Evaluation. Psychol. Assess. 2019, 31, 1019. [CrossRef] [Green Version]
- Indolia, S.; Goswami, A.; Mishra, S.; Asopa, P. Conceptual Understanding of Convolutional Neural Network—A Deep Learning Approach. Procedia Comput. Sci. 2018, 132, 679–688. [Google Scholar] [CrossRef]
- Lih, O.S.; Jahmunah, V.; San, T.R.; Ciaccio, E.J.; Yamakawa, T.; Tanabe, M.; Kobayashi, M.; Faust, O.; Acharya, U.R. Comprehensive electrocardiographic diagnosis based on deep learning. Artif. Intell. Med. 2020, 103, 101789. [Google Scholar] [CrossRef]
- Oh, S.L.; Vicnesh, J.; Ciaccio, E.J.; Yuvaraj, R.; Acharya, U.R. Deep Convolutional Neural Network Model for Automated Diagnosis of Schizophrenia Using EEG Signals. Appl. Sci. 2019, 9, 2870. [Google Scholar] [CrossRef] [Green Version]
- Cascade, R.; Chunking, N.S. Long Short-Term Memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar]
- Hinton, G.E.; Salakhutdinov, R.R. Reducing the Dimensionality of Data with Neural Networks. Science 2006, 313, 504–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belpaeme, T.; Baxter, P.E.; Read, R.; Wood, R.; Cuayáhuitl, H.; Kiefer, B.; Racioppa, S.; Kruijff-Korbayová, I.; Athanasopoulos, G.; Enescu, V.; et al. Multimodal Child-Robot Interaction: Building Social Bonds. J. Hum. Robot Interact. 2013, 1, 33–53. [Google Scholar] [CrossRef] [Green Version]
- Sanghvi, J.; Castellano, G.; Leite, I.; Pereira, A.; McOwan, P.W.; Paiva, A. Automatic analysis of affective postures and body motion to detect engagement with a game companion. In Proceedings of the 6th International Conference on Human-Robot Interaction—HRI ’11, Lausanne, Switzerland, 6–9 March 2011; pp. 305–312. [Google Scholar]
- Kim, J.C.; Azzi, P.; Jeon, M.; Howard, A.M.; Park, C.H. Audio-based emotion estimation for interactive robotic therapy for children with autism spectrum disorder. In Proceedings of the 2017 14th International Conference on Ubiquitous Robots and Ambient Intelligence (URAI), Jeju, Korea, 28 June–1 July 2017; pp. 39–44. [Google Scholar]
- Anzalone, S.M.; Boucenna, S.; Ivaldi, S.; Chetouani, M. Evaluating the Engagement with Social Robots. Int. J. Soc. Robot. 2015, 7, 465–478. [Google Scholar] [CrossRef]
- Colton, M.B.; Ricks, D.J.; Goodrich, M.A.; Dariush, B.; Fujimura, K.; Fujiki, M. Toward therapist-in-the-loop assistive robotics for children with autism and specific language impairment. In Proceedings of the 23rd Convention of the Society for the Study of Artificial Intelligence and Simulation of Behaviour, AISB 2009, Edinburgh, UK, 6–9 April 2009. [Google Scholar]
- Hernandez, J.; Riobo, I.; Rozga, A.; Abowd, G.D.; Picard, R.W. Using electrodermal activity to recognize ease of engagement in children during social interactions. In Proceedings of the 2014 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Seattle, WA, USA, 13–17 September 2014; pp. 307–317. [Google Scholar]
- Esteban, P.G.; Baxter, P.; Belpaeme, T.; Billing, E.; Cai, H.; Cao, H.-L.; Coeckelbergh, M.; Costescu, C.; David, D.; De Beir, A.; et al. How to Build a Supervised Autonomous System for Robot-Enhanced Therapy for Children with Autism Spectrum Disorder. Paladyn J. Behav. Robot. 2017, 8, 18–38. [Google Scholar] [CrossRef]
- Rudovic, O.; Lee, J.; Dai, M.; Schuller, B.; Picard, R.W. Personalized machine learning for robot perception of affect and engagement in autism therapy. Sci. Robot. 2018, 3, eaao6760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fridin, M. Storytelling by a kindergarten social assistive robot: A tool for constructive learning in preschool education. Comput. Educ. 2014, 70, 53–64. [Google Scholar] [CrossRef]
- Sonne, T.; Obel, C.; Grønbæk, K. Designing real time assistive technologies: A study of children with ADHD. In Proceedings of the Annual Meeting of the Australian Special Interest Group for Computer Human Interaction, Parkville, VIC, Australia, 7–10 December 2015; pp. 34–38. [Google Scholar]
- Lynch, M. Assistive techology to help children with attention deficit hyperactivity disorder succeed academically. Assitive Technology, 9 May 2018. [Google Scholar]
- Somma, F.; Rega, A.; Gigliotta, O. Artificial Intelligence-powered cognitive training applications for children with attention deficit hyperactivity disorder: A brief review. Child. Worldw. 2019, 2, 4. [Google Scholar]
- Lopresti, E. Rehabilitation and Prosthetic Services; Device Review: Watchminder by Watchminder. 2015. Available online: https://www.prosthetics.va.gov/AssistiveTechnology/reviews/Device_Review_WatchMinder.asp (accessed on 25 February 2021).
- Huang, X.; Baker, J.; Reddy, R. A historical perspective of speech recognition. Commun. ACM 2014, 57, 94–103. [Google Scholar] [CrossRef]
- Bouck, E.C.; Flanagan, S.; Joshi, G.S.; Sheikh, W.; Schleppenbach, D. Speaking Math—A Voice Input, Speech Output Calculator for Students with Visual Impairments. J. Spéc. Educ. Technol. 2011, 26, 1–14. [Google Scholar] [CrossRef]
- Ndombo, M.; Ojo, S.; Osunmakinde, I. An intelligent integrative assistive system for dyslexic learners. J. Assist. Technol. 2013, 7, 172–187. [Google Scholar] [CrossRef]
- Athanaselis, T.; Bakamidis, S.; Dologlou, I.; Argyriou, E.N.; Symvonis, A. Making assistive reading tools user friendly: A new platform for Greek dyslexic students empowered by automatic speech recognition. Multimedia Tools Appl. 2014, 68, 681–699. [Google Scholar] [CrossRef]
- Hamid, S.S.A.; Admodisastro, N.; Kamaruddin, A. A study of computer-based learning model for students with dyslexia. In Proceedings of the 2015 9th Malaysian Software Engineering Conference (MySEC), Kuala Lumpur, Malaysia, 16–17 December 2015; pp. 284–289. [Google Scholar]
- Lynch, M. 11 Must-Have Apps and Tools for Dyslexic Students. Available online: https://gokicker.com/dyslexia-tools/ (accessed on 18 October 2021).
- Michalos, A.C. Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014; p. 5736. [Google Scholar]
- Sood, M.R.; Toornstra, A.; Sereno, M.I.; Boland, M.; Filaretti, D.; Sood, A. A Digital App to Aid Detection, Monitoring, and Management of Dyslexia in Young Children (DIMMAND): Protocol for a Digital Health and Education Solution. JMIR Res. Protoc. 2018, 7, e135. [Google Scholar] [CrossRef]
- World’s First App Screens for Dyslexia in Minutes Using Artificial Intelligence. 2020. Available online: https://dystech.com.au/education/worlds-first-app-screens-for-dyslexia-in-minutes-using-artificial-intelligence/ (accessed on 24 August 2021).
- Schneps, M.H.; Thomson, J.M.; Chen, C.; Sonnert, G.; Pomplun, M. E-Readers Are More Effective than Paper for Some with Dyslexia. PLoS ONE 2013, 8, e75634. [Google Scholar] [CrossRef]
- Spanish Application Using AI to Overcome Dyslexia Wins 2019 UNESCO ICT Prize. UNESCO, 2020. Available online: https://en.unesco.org/news/spanish-application-using-ai-help-overcome-dyslexia-wins-2019-unesco-ict-prize (accessed on 24 August 2021).
- Rello, L.K.; Williams, A.; Ali, N.C.; White, J.P. Bigham, Dytective: Towards Detecting Dyslexia across Languages Using an Online Game. In Proceedings of the 13th International Web for All Conference, Montreal, QC, Canada, 11–13 April 2016. [Google Scholar]
- Agama, A.A.; Gómez, R.M. DytectiveU application: Contribution to the literacy in children with dyslexia. Espirales Rev. Multidiscip. De Investig. 2021, 5, 27–35. [Google Scholar] [CrossRef]
- Shukla, R.; Bhattacharyya, B.; Nadu, T.; Agarwal, R.; Nadu, T. A Comprehensive Study of Audio Visual Aids for Dyslexic Children. IJEET 2020, 11, 211–218. [Google Scholar]
- Abirached, B.; Zhang, Y.; Aggarwal, J.K.; Tamersoy, B.; Fernandes, T.; Carlos, J. Improving communication skills of children with ASDs through interaction with virtual characters. In Proceedings of the 2011 IEEE 1st International Conference on Serious Games and Applications for Health (SeGAH), Braga, Portugal, 16–18 November 2011; pp. 1–4. [Google Scholar] [CrossRef]
- Brain Power, L.L.C. Brain Power Releases First Augmented Reality Smartglasses to Help People with Autism Increase Social, School, and Job Success. Business Wire (English). 11AD. Available online: https://www.businesswire.com/news/home/20171107006113/en/Brain-Power-Releases-First-Augmented-Reality-Smartglasses-to-Help-People-with-Autism-Increase-Social-School-and-Job-Success (accessed on 7 December 2021).
- Fernandez, M. This Emotionally Intelligent Device Is Helping Kids with Autism Form Bonds. Health, 21 March 2018. [Google Scholar]
- Google Glass Helps Kids with Autism Read Facial Expressions. Stanford Medicine. 2018. Available online: https://med.stanford.edu/news/all-news/2018/08/google-glass-helps-kids-with-autism-read-facial-expressions.html (accessed on 24 February 2021).
- Miller, B. How Kaspar the Robot Is Helping Autistic Students to Socialise. News, 5 June 2018. [Google Scholar]
- Wood, L.J.; Zaraki, A.; Robins, B.; Dautenhahn, K. Developing Kaspar: A Humanoid Robot for Children with Autism. Int. J. Soc. Robot. 2021, 13, 491–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaraki, A.; Khamassi, M.; Wood, L.; Lakatos, G.; Tzafestas, C.; Amirabdolahian, F.; Robins, B.; Dautenhahn, K. A Novel Reinforcement-Based Paradigm for Children to Teach the Humanoid Kaspar Robot. Int. J. Soc. Robot. 2019, 12, 709–720. [Google Scholar] [CrossRef] [Green Version]
- Papakostas, G.; Sidiropoulos, G.; Papadopoulou, C.; Vrochidou, E.; Kaburlasos, V.; Papadopoulou, M.; Holeva, V.; Nikopoulou, V.-A.; Dalivigkas, N. Social Robots in Special Education: A Systematic Review. Electronics 2021, 10, 1398. [Google Scholar] [CrossRef]
- Enabling Devices. Apps for Individuals on the Autism Spectrum. 2019, pp. 1–16. Available online: https://enablingdevices.com/wp-content/uploads/2019/03/Apps-for-Individuals-with-Autism.pdf (accessed on 7 December 2021).
- Novack, M.N.; Hong, E.; Dixon, D.R.; Granpeesheh, D. An Evaluation of a Mobile Application Designed to Teach Receptive Language Skills to Children with Autism Spectrum Disorder. Behav. Anal. Pract. 2019, 12, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Rouhi, A.; Spitale, M.; Catania, F.; Cosentino, G.; Gelsomini, M.; Garzotto, F. Emotify: Emotional game for children with autism spectrum disorder based-on machine learning. In Proceedings of the 24th International Conference on Intelligent User Interfaces: Companion, Marina del Ray, CA, USA, 16–20 March 2019; pp. 31–32. [Google Scholar]
- Wang, X.; Goh, D.H.-L.; Lim, E.-P.; Vu, A.W.L.; Chua, A.Y.K. Examining the Effectiveness of Gamification in Human Computation. Int. J. Hum.-Comput. Interact. 2017, 33, 813–821. [Google Scholar] [CrossRef]
- Alcorn, A.M.; Ainger, E.; Charisi, V.; Mantinioti, S.; Petrović, S.; Schadenberg, B.R.; Tavassoli, T.; Pellicano, E. Educators’ Views on Using Humanoid Robots with Autistic Learners in Special Education Settings in England. Front. Robot. AI 2019, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Study Proves AI Robots Can Boost Social Skills in Children on Autism Spectrum. Big Data Made Simple. 2020. Available online: https://bigdata-madesimple.com/ai-robots-boost-social-skills-children-autism-spectrum/ (accessed on 7 December 2021).
- Jain, S.; Thiagarajan, B.; Shi, Z.; Clabaugh, C.; Matarić, M.J. Modeling engagement in long-term, in-home socially assistive robot interventions for children with autism spectrum disorders. Sci. Robot. 2020, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Rakhymbayeva, N.; Seitkazina, N.; Turabayev, D.; Pak, A.; Sandygulova, A. A Long-term Study of Robot-Assisted Therapy for Children with Severe Autism and ADHD. In Proceedings of the Companion of the 2020 ACM/IEEE International Conference on Human-Robot Interaction, Cambridge, UK, 23–26 March 2020; pp. 401–402. [Google Scholar] [CrossRef] [Green Version]
- Autism Spectrum Disorders (ASD): Common Assistive Technologies. 2020. Available online: https://guides.library.illinois.edu/c.php?g=515793&p=3526329 (accessed on 25 February 2021).
- Elsahar, Y.; Hu, S.; Bouazza-Marouf, K.; Kerr, D.; Mansor, A. Augmentative and Alternative Communication (AAC) Advances: A Review of Configurations for Individuals with a Speech Disability. Sensors 2019, 19, 1911. [Google Scholar] [CrossRef] [Green Version]
- Muharib, R.; Alzrayer, N.M. The Use of High-Tech Speech-Generating Devices as an Evidence-Based Practice for Children with Autism Spectrum Disorders: A Meta-analysis. Rev. J. Autism Dev. Disord. 2018, 5, 43–57. [Google Scholar] [CrossRef]
- Muharib, R.; Correa, V.I.; Wood, C.L.; Haughney, K.L. Effects of Functional Communication Training Using GoTalk NowTM iPad® Application on Challenging Behavior of Children With Autism Spectrum Disorder. J. Spéc. Educ. Technol. 2019, 34, 71–79. [Google Scholar] [CrossRef]
- Hopkins, I.M.; Gower, M.W.; Perez, T.A.; Smith, D.S.; Amthor, F.R.; Wimsatt, F.C.; Biasini, F.J. Avatar Assistant: Improving Social Skills in Students with an ASD Through a Computer-Based Intervention. J. Autism Dev. Disord. 2011, 41, 1543–1555. [Google Scholar] [CrossRef] [PubMed]
- Rice, L.M.; Wall, C.A.; Fogel, A.; Shic, F. Computer-Assisted Face Processing Instruction Improves Emotion Recognition, Mentalizing, and Social Skills in Students with ASD. J. Autism Dev. Disord. 2015, 45, 2176–2186. [Google Scholar] [CrossRef] [PubMed]
- Macaulay, T. Robot Uses AI to Personalize Teaching of Autistic Children. Neural Human-Centric News and Analysis. 2020. Available online: https://thenextweb.com/news/robot-uses-ai-to-personalize-teaching-of-autistic-children (accessed on 24 February 2021).
- Arshad, N.I.; Hashim, A.S.; Ariffin, M.M.; Aszemi, N.M.; Low, H.M.; Norman, A.A.; Min, L.H. Robots as Assistive Technology Tools to Enhance Cognitive Abilities and Foster Valuable Learning Experiences among Young Children With Autism Spectrum Disorder. IEEE Access 2020, 8, 116279–116291. [Google Scholar] [CrossRef]
- Purnama, Y.; Herman, F.A.; Hartono, J.; Neilsen; Suryani, D.; Sanjaya, G. Educational Software as Assistive Technologies for Children with Autism Spectrum Disorder. Procedia Comput. Sci. 2021, 179, 6–16. [Google Scholar] [CrossRef]
- Ham, B. Personalized ‘deep learning’ equips robots for autism therapy. MIT News. 2018. Available online: https://news.mit.edu/2018/personalized-deep-learning-equips-robots-autism-therapy-0627 (accessed on 7 December 2021).
- Regan, P.M.; Jesse, J. Ethical challenges of edtech, big data and personalized learning: Twenty-first century student sorting and tracking. Ethic-Inf. Technol. 2019, 21, 167–179. [Google Scholar] [CrossRef]
- Kourtney, K. Chapter 1: Ethical Considerations When Using Artificial Intelligence-Based Assistive Technologies in Education. 2021. Available online: https://openeducationalberta.ca/educationaltechnologyethics/chapter/ethical-considerations-when-using-artificial-intelligence-based-assistive-technologies-in-education/ (accessed on 25 February 2021).
- Smith, S.W.; Bourgeois, D.T.; James, L.; Mortati, J. The Ethical and Legal Implications of Information Systems; 2021. Available online: https://bus206.pressbooks.com/chapter/chapter-12-the-ethical-and-legal-implications-of-information-systems/ (accessed on 25 February 2021).
- Paul, Y.; Hickok, E.; Sinha, A.; Tiwari, U. Artificial Intelligence in the Healthcare Industry in India; The Centre for Internet and Society: Bengaluru, India, 2018. [Google Scholar]
- Tsai, Y.S.; Gasevic, D. Learning analytics in higher education—Challenges and policies: A review of eight learning analytics policies. In Proceedings of the Seventh International Learning Analytics & Knowledge Conference, Vancouver, BC, Canada, 13–17 March 2017; pp. 233–242. [Google Scholar]
- Zilvinskis, J.; Wills, J., III. Learning Analytics in Higher Education: A Reflection. InSight A J. Sch. Teach. 2019, 14, 43–54. [Google Scholar] [CrossRef]
- 15 Pros and 6 Cons of Artificial Intelligence in the Classroom. 2021. Available online: https://livetilesglobal.com/pros-cons-artificial-intelligence-classroom/ (accessed on 24 February 2021).
- Cloud-Based Intranet vs. On-Premise Intranet: Which Is Best? Available online: https://www.bizportals365.com/blog/cloud-intranet-vs-on-premise-intranet/ (accessed on 24 February 2021).
- Shi, Y.; Yang, H.H.; Yang, Z.; Wu, D. Trends of Cloud Computing in Education. Lect. Notes Comput. Sci. 2014, 116–128. [Google Scholar] [CrossRef]
- Yang, H.H.; Yuen, S.C.Y. Handbook of Research on Practices and Outcomes in E-Learning: Issues and Trends; Hershey: New York, NY, USA, 2009; pp. 1–557. [Google Scholar]
- Hastings, R. Researching, Evaluating, and Choosing a Backup Service in the Cloud. Comput. Libr. 2012, 32, 68–71. [Google Scholar]
- Kanjilal, J. Benefits and Drawbacks of AI in Cloud Computing. 2021. Available online: https://searchcloudcomputing.techtarget.com/tip/Benefits-and-drawbacks-of-AI-in-cloud-computing (accessed on 8 July 2020).
- Jørgensen, F.A. The Internet of Things. A New Companion to Digit. Humanit 2015, 2012, 42–53. [Google Scholar]
- Bansal, P.; Panchal, R.; Bassi, S.; Kumar, A. Blockchain for Cybersecurity: A Comprehensive Survey. In Proceedings of the 2020 IEEE 9th International Conference on Communication Systems and Network Technologies (CSNT), Gwalior, India, 10–12 April 2020; pp. 260–265. [Google Scholar]
- Taha, S.; Shen, X. A Physical-Layer Location Privacy-Preserving Scheme for Mobile Public Hotspots in NEMO-Based VANETs. IEEE Trans. Intell. Transp. Syst. 2013, 14, 1665–1680. [Google Scholar] [CrossRef]
- Han, J.; Susilo, W.; Mu, Y.; Yan, J. 2z5zcd 99psxpw. IEEE Trans. Parallel Distrib. Syst. 2012, 23, 2150–2162. [Google Scholar] [CrossRef]
- Drigas, A.S.; Ioannidou, R.-E. A Review on Artificial Intelligence in Special Education. Commun. Comput. Inf. Sci. 2013, 278, 385–391. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Learning Area | Intervention |
|---|---|
| Reading comprehension | Establish a sustained silent reading time daily. Allow the child to read a book silently while listening to the teacher reading the story to the whole class. Getting the child to make a storyboard, retell a story during story sessions, role-play characters in a favourite story. Allowing the child to play board games/computer games to enhance reading comprehension skills. Maintaining a word-bank book for words that are hard to read. Providing students with another set of books to be read at home [36] |
| Phonics | Teaching children simple reminders on how to learn tougher phonics. Teaching children how to recognise word families for phonetic concepts. Allowing students to play board games, such as Bingo or computer games, to enhance phonics. Using picture–letter charts for children who can identify sounds but not letters [36] |
| Writing | Using storyboards to teach students to recognise parts of a story for writing. Creating a post-office in the classroom for students to write and receive letters from their teachers and peers. Using tape recorders to dictate as an alternative to writing or having teacher/peer to write for students who would tell the story [36] |
| Spelling | Aligning spelling words to frequently used words by children everyday. Partnering the child with another peer to encourage each other to quiz on spelling words. Using colour-coded letters to help students spell difficult words. Combining movement activities with spelling lessons [36] |
| Handwriting | Using special writing paper or teaching how to use a finger spacing to space out each word when writing. Teaching handwriting skills through structured programmes [36] |
| Mathematics computation | Using mnemonics to describe fundamental steps easily for Maths computation. Colour-coding arithmetic symbols to provide visual cues, allowing students to use calculators for basic computation, using computer/board games for practicing computations [36] |
| Learning Area | Intervention |
|---|---|
| 1. Failure in reading, grouping letters in words. | Using visual perceptions, such as signage or touching letters, to help in reading. Providing simultaneous stimulation of each ear using different sounds [23] |
| 2. Phonology | Employing strategies that help phonological processing, such as ‘minimal pairs,’ ‘common syllable words,’ and ‘vocal syllabification’ [23] |
| 3. Grammar | Using grammatical processing strategies, such as ‘syllabification,’ ‘declension of nouns,’ ‘stress,’ and ‘nouns’ [23] |
| 4. Writing | Using the syntactic approach to teach punctuation and sentences/paragraphs. Using the ‘segmentation with highlighting’ technique for sentence and text segmentation [23] |
| Structured Teaching Strategies | Intervention |
|---|---|
| Physical structure | Establish a supportive classroom environment by creating clear physical or visual boundaries such that expected behaviours for each defined space can be taught and reinforced [39] |
| Reducing auditory and visual disturbances | Too much auditory or visual stimuli may hamper processing power; hence, unnecessary distractions are removed in classrooms to help students focus better on concepts taught [39] |
| Visual schedules | Implementing visual schedules for the day (instead of using verbal probes), according to the learning needs of each student to enhance student independence and engagement during lessons [39] |
| Work system | Implementing a work system for any type of educational activity helps to organise the student by providing a systematic work routine [39] |
| Visual structures | Adding a physical or visual aspect to some tasks to help students understand better how an activity needs to be completed [39] |
| Boolean Search String | |||
|---|---|---|---|
| Database | Title | AND [Title/Abstract/Full Text] | No. of Articles |
| IEEE | “Autism spectrum disorder”, AND/OR “Attention deficit hyperactivity disorder” AND/OR “dyslexia”, Artificial intelligence AND/OR tools, students AND/OR learning | Machine learning, Neural networks, deep learning | Autism: 0, ADHD: 1, Dyslexia: 0 |
| Google Scholar | Autism: 12 100, ADHD: 3900, Dyslexia: 3800 | ||
| PubMed | Autism: 0, ADHD: 0, Dyslexia: 0 | ||
| Science Direct | Autism: 176, ADHD: 172, Dyslexia: 97 | ||
| Springer Link | Autism: 357, ADHD: 179, Dyslexia: 144 | ||
| Author/Year | AI Tool | Features/Model Used for Training | Type of Technology | Learning Area Addressed | Effectiveness |
|---|---|---|---|---|---|
| AI Assistive Tools Used to Teach Students with ADHD. | |||||
| 2014 [61] | KAR robot | - | Assistive technology | Improve social skills via storytelling. | Improves children’s cognitive performance. |
| 2015 [62] | Child activity sensing and training tool |
| Real time assistive technology | Real-time assistive tool that tracks activities and helps students sustain attention. | An assistive intervention that is based on a smartphone and has the potential to aid a child with ADHD who has lost focus in his/her work. |
| 2018 [63,64] | WatchMinder vibrating watch |
| Wearable technology | Helps to send constant reminders to students to refocus on their work. | The watch has been effective as a simple memory aid for ADHD children with the auditory or vibrating alarm feature. The watch has been found to be affordable, durable, dependable and effective by users [65] |
| 2018 [63] | Speech recognition software (Dragon Naturallyspeaking(Dragon Sytems company, United States, version 15, /Voice Finger/ViaTalk (LLC Company, New York/Tazti (Voice Tech Group company, United States) |
| Assistive technology | Replaces writing activity with speech to allow students to express themselves efficiently without tiring themselves | Dragon Naturallyspeaking, Voice Finger, Via Talk, Tazti softwares have been reported to be beneficial to students with ADHD and resulted in improvement in the areas of writing, reading and spelling [65] |
| 2018 [63,67] | Talking calculators |
| Assistive technology | Helps students hear and process numbers easily for mathematics. | Students are able to complete assessments faster with the help of the calculator and has helped students gain independence [67] |
| AI assistive tools used to teach students with Dyslexia. | |||||
| 2013 [68] | Intelligent dyslexic system | Machine learning algorithm, visualisation concept | Assistive technology | Helps students gain knowledge on alphabets and letters | The technology has the potential to improve the reading and writing skills of students. |
| 2014 [69] | Agent DYSL adaptive reading system | Machine learning algorithm, Mel-frequency cepstral coefficients, discrete cosine transform | Assistive technology | Enables the personalisation of reading environment of Greek students. | Students’ reading pace and accuracy were increased. |
| 2015 [70] | Computer-based learning model | Machine learning technique | - | Explores the use of machine learning method to improve effectiveness of learning process. | - |
| 2017 [71] | Applications for reading and writing (Learning Ally, Natural reader, dyslexia quest, sound literacy, ginger page, v books pdf voice reader, openWeb, reading intro by OZ phonics, OCR instantly pro, MindMeister) | Generation of audio files, pytorch deep convolutional text-to-speech models (PytorchDcTts) | Digital application | Helps students with reading and writing skills. | Audiobooks, such as learning Ally, has enabled students to gain confidence, independence and success [72]. |
| 2018 [73] | DIMMAND, capturaTalk application |
| Digital application | Provides tailored interventions for difficulties encountered in literacy. | Information is not available. |
| 2020 [74] | Voice dream reader, natural reader, web reader |
| Digital application | Helps with building reading skills. | E-readers have been found to generally improve reading speed and comprehension as compared to reading on paper [75]. |
| 2020 [76,77] | DytectiveU |
| Digital application | Provides personalised game-based exercises to enhance specific cognitive skills related linked to dyslexia. | The DytectiveU application is reported to be able to offer students a variety of actions that are helpful in the learning of reading and writing [78]. |
| 2020 [79] | Generative adversarial network | Conversion of image/speech to text | Assistive technology | Converts natural language text to images to aid students in their learning. | - |
| AI assistive tools used to teach students with ASD. | |||||
| 2011 [80] | LIFEisGAME game |
| Digital application | To teach students to recognise facial emotions. | Information is not available. |
| 2017 [81,82] | ‘Empower me’ application |
| Wearable technology | Encourages social interaction between user and peers/educators. | Students were able to improve their social skills using the Google glass. It was also reported to be fun, useful and engaging [83]. |
| 2018 [84,85] | Kaspar robot |
| Assistive technology | Helps enhance social interaction skills. | The human-like body and features of Kaspar have been reported to help an ASD student to be more interactive [87]. |
| 2018 [88] | ABA flashcards- Emotions, Autism emotion, conversation builder, emotions and feelings- autism, Find me, Kid in storybook maker, learning with Rufus, Look in my eyes: Train engineer, Model me going places 2, Pictello, Social stories, Special stories, The social express, Toca Boca |
| Digital application | Teaches social skills | Information is not available. |
| 2018 [88] | ABA find it, Agnitus, Autism learning games- camp discovery, Intro to letters, Intro to Math, Math Bingo, Pop Math, Starfall ABC, Word wagon |
| Digital application | Helps in different learning areas | The camp discovery enabled participants to show high learning rates over a short period of time. It has been suggested that the application teaches the selected skills effectively [89]. |
| 2019 [90] | Emotify game |
| Digital application | Helps students to recognise and express feelings. | The application caused participants to experience more engagement and exhibit higher behavioural intentions towards it [91]. |
| 2019 [92,93] | Milo, NAO, Pepper, Aisoy 1, Keepon robots |
| Assistive technology | Helps build social and communication skills. | Social robots, such as NAO, have been reported to improve social skills in students, especially in terms of eye contact and concentration. Nonverbal children also reportedly started pronouncing some words [95]. |
| 2020 [88,96] | GoTalks speech generating device, AAC speech buddy, Proloquo2go, talking Larry, Touch chat HD, VAST autism 1-Core |
| Augmentative/alternative communication device | Helps with building communication skills. | Review studies report that high-technology speech generating devices are very effective in teaching manding, intraverbal and multistep tacting to ASD students [98]. |
| 2020 [96,99,100] | Facesay games |
| Digital application | Software games help recognise behavioural and emotional clues and enhance social skills. | Facesay application is found to be very promising, cost-effective and efficient for teaching affect recognition and mentalising constructs to high-functioning ASD students [101]. |
| 2020 [102] | Personalised ‘Kiwi’ robot for learning |
| Assistive technology | Adapts lessons according to students’ changing needs. | Kiwi robot has been reported to improve the Maths skills and social skills in ASD students who were part of the study group [103]. |
| 2020 [96] | Life skills winner application |
| Digital application | Teaches students daily living skills through the application. | Information is not available. |
| 2020 [103] | PvBOT robot | LEGO Mindstorms EV3 model | Assistive technology | Helps to teach students ‘place value’ concept in Mathematics. | PvBOT is helpful in motivating students to pay attention and stay focused for a longer period. |
| 2021 [104] | Squizzy educational software | Scrum methodology | Assistive technology | Helps children stay focused during activities that involve cognition, such as colour selection or using pictures. | Effective in the cognitive aspect of therapy. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barua, P.D.; Vicnesh, J.; Gururajan, R.; Oh, S.L.; Palmer, E.; Azizan, M.M.; Kadri, N.A.; Acharya, U.R. Artificial Intelligence Enabled Personalised Assistive Tools to Enhance Education of Children with Neurodevelopmental Disorders—A Review. Int. J. Environ. Res. Public Health 2022, 19, 1192. https://doi.org/10.3390/ijerph19031192
Barua PD, Vicnesh J, Gururajan R, Oh SL, Palmer E, Azizan MM, Kadri NA, Acharya UR. Artificial Intelligence Enabled Personalised Assistive Tools to Enhance Education of Children with Neurodevelopmental Disorders—A Review. International Journal of Environmental Research and Public Health. 2022; 19(3):1192. https://doi.org/10.3390/ijerph19031192
Chicago/Turabian StyleBarua, Prabal Datta, Jahmunah Vicnesh, Raj Gururajan, Shu Lih Oh, Elizabeth Palmer, Muhammad Mokhzaini Azizan, Nahrizul Adib Kadri, and U. Rajendra Acharya. 2022. "Artificial Intelligence Enabled Personalised Assistive Tools to Enhance Education of Children with Neurodevelopmental Disorders—A Review" International Journal of Environmental Research and Public Health 19, no. 3: 1192. https://doi.org/10.3390/ijerph19031192
APA StyleBarua, P. D., Vicnesh, J., Gururajan, R., Oh, S. L., Palmer, E., Azizan, M. M., Kadri, N. A., & Acharya, U. R. (2022). Artificial Intelligence Enabled Personalised Assistive Tools to Enhance Education of Children with Neurodevelopmental Disorders—A Review. International Journal of Environmental Research and Public Health, 19(3), 1192. https://doi.org/10.3390/ijerph19031192