
Development and Validation of Knowledge, Attitude, and Practice Questionnaire: Toward Safe Working in Confined Spaces

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase 1: Questionnaire Development
2.2. Phase 2: Validation
Study Setting and Participants
2.3. Statistical Analysis
2.3.1. Item Response Theory
2.3.2. Exploratory Factor Analysis
2.3.3. Confirmatory Factor Analysis
3. Results
3.1. Questionnaire Development and Validity
3.2. Characteristics of the Participants
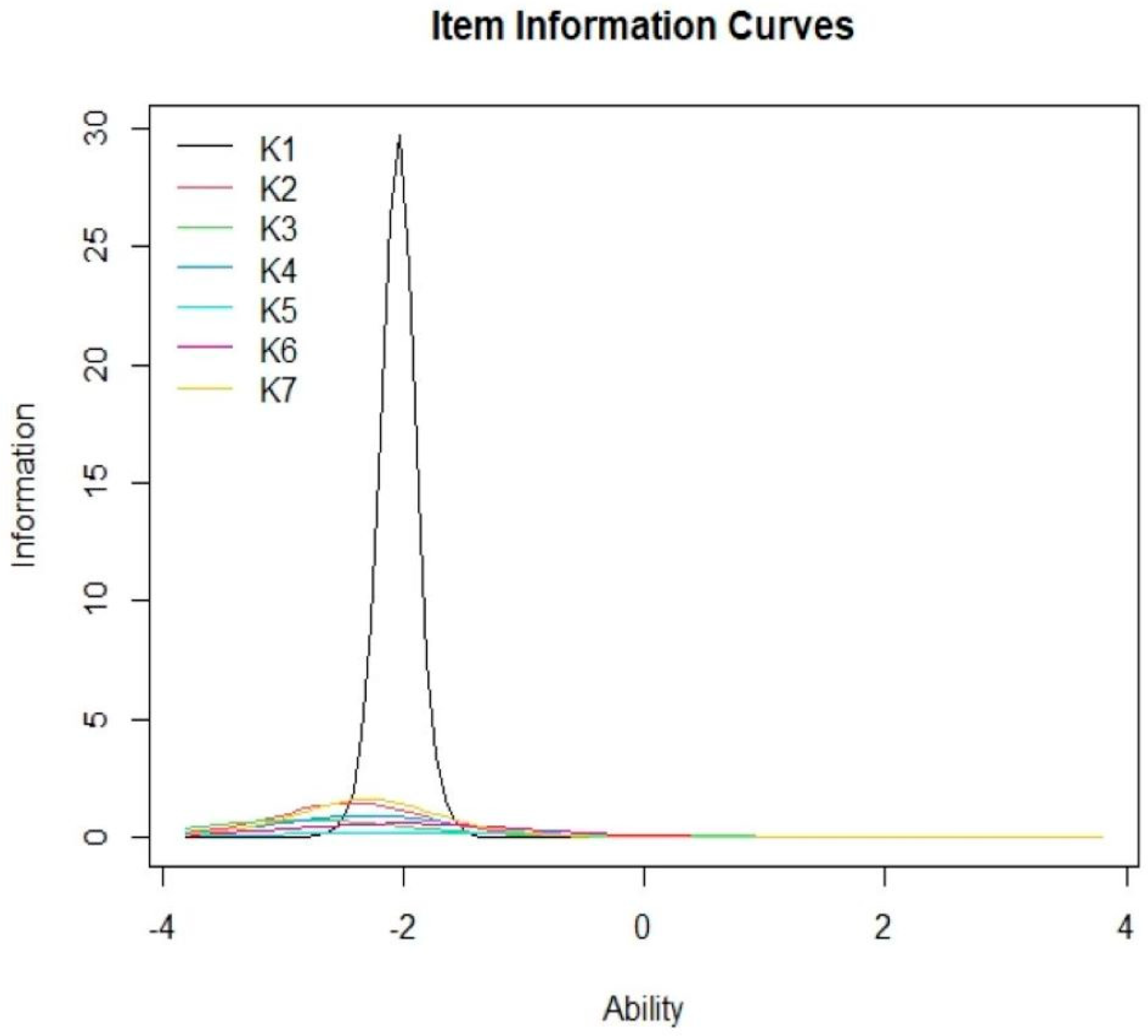
3.3. Item Response Theory
3.4. Exploratory Factor Analysis
3.5. Confirmatory Factor Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Industry Code of Practice for Safe Working in a Confined Space 2010. Available online: https://www.dosh.gov.my/index.php/legislation/codes-of-practice/industrial-hygiene/593-industry-code-of-practice-for-safe-working-in-a-confined-space-2010/file (accessed on 14 April 2020).
- Selman, J.; Spickett, J.; Jansz, J.; Mullins, B. An investigation into the rate and mechanism of incident of work-related confined space fatalities. Saf. Sci. 2018, 109, 333–343. [Google Scholar] [CrossRef]
- Falakh, F.; Setiani, O. Hazard Identification and Risk Assessment in Water Treatment Plant considering Environmental Health and Safety Practice. E3S Web Conf. 2018, 31, 06011. [Google Scholar] [CrossRef] [Green Version]
- McManus, N. Safety, and Health in Confined Spaces; CRC Press: Boca Raton, FL, USA; Taylor & Francis Group: Abingdon, UK, 2018; pp. 1–39. [Google Scholar]
- Nawaz, S.; Strobel, J.; Ghafoor, A.; Lu, Y.; Balakrishnan, V.R. Estimation of the Frequency, Severity and Prmary Causative Factors Associated with Injuries and Fatalities Involving Confined Spaces in Agriculture. Purdue Univ. 2011, 9, 176. [Google Scholar]
- Burlet-Vienney, D.; Chinniah, Y.; Bahloul, A. The need for a comprehensive approach to managing confined space entry: Summary of the literature and recommendations for next steps. J. Occup. Environ. Hyg. 2014, 11, 485–498. [Google Scholar] [CrossRef] [PubMed]
- Botti, L.; Duraccio, V.; Gnoni, M.G.; Mora, C. An integrated holistic approach to health and safety in confined spaces. J. Loss Prev. Process Ind. 2018, 55, 25–35. [Google Scholar] [CrossRef]
- World Health Organization; The International Labour Organization. WHO/ILO Joint Estimates of the Work-Related Burden of Disease and Injury, 2000–2016: Global Monitoring Report; World Health Organization: Geneva, Switzerland; The International Labour Organization: Geneva, Switzerland, 2021. [Google Scholar]
- U. S. Bureau of Labour Statistics. Injuries, Ilnesses and Fatalities: Fact Sheet|Fatal Occupational Injuries Involving Confined Space. Available online: https://www.bls.gov/iif/oshwc/cfoi/confined-spaces-2011-18.htm (accessed on 7 July 2020).
- Department of Occupational Safety and Health, Ministry of Human Resources, Malaysia. National Occupational Accident & Fatality Rate. Available online: https://www.dosh.gov.my/index.php/statistic-v/national-occupational-accident-fatality-rate-v (accessed on 18 August 2020).
- Ayob, A.; Shaari, A.A.; Zaki, M.F.M.; Munaaim, M.A.C. Fatal occupational injuries in the Malaysian construction sector-causes and accidental agents. In IOP Conference Series: Earth and Environmental Science; IOP: Bristol, UK, 2018; Volume 140. [Google Scholar]
- Zakaria, N.H.; Mansor, N.; Abdullah, Z. Workplace accident in Malaysia: Most common causes and solutions. Business Management Review. Bus. J. 2012, 2, 75–88. Available online: http://www.businessjournalz.org/bmr (accessed on 17 August 2020).
- Chiu, C.-C.; Chang, Y.-M.; Wan, T.-J. Characteristic Analysis of Occupational Confined Space Accidents in Taiwan and Its Prevention Strategy. Int. J. Environ. Res. Public Health 2020, 17, 1752. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, H. Industrial Accident Prevention: A Scientific Approach, 4th ed.; McGraw-Hill: New York, NY, USA, 1969; Available online: https://www.worldcat.org/title/industrial-accident-prevention-a-scientific-approach/oclc/571338960 (accessed on 21 July 2020).
- Choudhry, R.M.; Fang, D. Why operatives engage in unsafe work behavior: Investigating factors on construction sites. Saf. Sci. 2008, 46, 566–584. [Google Scholar] [CrossRef]
- Fleming, M.; Lardner, R. Strategies to Promote Safe Behavior as Part of a Health and Safety Management System, 1st ed.; The Keil Centre: Edinburgh, UK, 2002; pp. 32–37. [Google Scholar]
- Asgedom, A.A.; Bråtveit, M.; Moen, B.E. Knowledge, attitude, and practice related to chemical hazards and personal protective equipment among particleboard workers in Ethiopia: A cross-sectional study. BMC Public Health 2019, 19, 440. [Google Scholar] [CrossRef] [Green Version]
- Abdalwhab, S.M.; Yassin, K.E.E. Hazards Arising from Working in Confined Spaces Case Study: Khartoum North Industrial. UofKEJ 2015, 5, 1–7. Available online: http://www.matec-conferences.org/10.1051/matecconf/20166600105 (accessed on 21 June 2021).
- Jiang, H.; Zhang, S.; Ding, Y.; Li, Y.; Zhang, T.; Liu, W.; Fan, Y.; Li, Y.; Zhang, R.; Ma, X. Development and validation of college students’ tuberculosis knowledge, attitudes, and practices questionnaire (CS-TBKAPQ). BMC Public Health 2017, 17, 949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nee, S.O.; Sani, N.A. Assessment of Knowledge, Attitudes, and Practices (KAP) among food handlers at residential colleges and canteen regarding food safety. Sains Malays. 2011, 40, 403–410. [Google Scholar]
- Oraibi, T.; Chiduhiegem, C.R.; Harcourt, P. Challenges of Safety and Health Management Schemes among Construction Firms in Nigeri. Int. J. Eng. Mod. Technol. 2018, 4, 78–83. [Google Scholar]
- The KAP Survey Model (Knowledge, Attitude & Practices). Available online: https://www.researchgate.net/file.PostFileLoader.html?id=56acfe3160614b17788b4592&assetKey=AS%3A323666162716672%401454179434027 (accessed on 10 June 2021).
- Cook, D.A.; Beckman, T.J. Current concepts in validity and reliability for psychometric instruments: Theory and application. Am. J. Med. 2006, 119, 166.e7–166.e16. [Google Scholar] [CrossRef] [PubMed]
- Guldenmund, F.W. The use of questionnaires in safety culture research—An evaluation. Saf. Sci. 2007, 45, 723–743. [Google Scholar] [CrossRef]
- Hodgen, A.; Ellis, L.; Churruca, K.; Bierbaum, M. Safety Culture Assessment in Health Care: A Review of the Literature on Safety Culture Assessment Modes. 2017. Available online: https://www.safetyandquality.gov.au/wp-content/uploads/2017/10/Safety-Culture-Assessment-in-Health-Care-A-review-of-the-literature-on-safety-culture-assessment-modes.pdf (accessed on 20 July 2020).
- Sexton, J.B.; Helmreich, R.L.; Neilands, T.B.; Rowan, K.; Vella, K.; Boyden, J.; Roberts, P.R.; Thomas, E.J. The Safety Attitudes Questionnaire: Psychometric properties, benchmarking data, and emerging research. BMC Health Serv. Res. 2006, 6, 44. [Google Scholar] [CrossRef] [Green Version]
- Department of Occupational Safety and Health Ministry of Human Resources. Laws of Malaysia. Act 514. Occupational Safety and Health Act 1994; Department of Occupational Safety and Health Ministry of Human Resources: Kuala Lumpur, Malaysia, 1994. Available online: https://www.dosh.gov.my/index.php/legislation/acts/23-02-occupational-safety-and-health-act-1994-act-514/file (accessed on 14 April 2020).
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- McDonald, J.A.; Nancy, B.; Victor, G.C.; Renee, L.J. Questionnaire Design. Reprod. Health Epidemiol. Ser. 2003, 4, 1–77. [Google Scholar]
- Burlet-Vienney, D.; Chinniah, Y.; Bahloul, A.; Roberge, B. Design and application of a 5 step risk assessment tool for confined space entries. Saf. Sci. 2015, 80, 144–155. [Google Scholar] [CrossRef]
- Burlet-Vienney, D.; Chinniah, Y.; Bahloul, A.; Roberge, B. Occupational safety during interventions in confined spaces. Saf. Sci. 2015, 79, 19–28. [Google Scholar] [CrossRef]
- Naghavi, K.Z.; Mortazavi, S.B.; Asilian, M.H.; Hajizadeh, E. Exploring the Contributory Factors of Confined Space Accidents Using Accident Investigation Reports and Semi structured Interviews. Saf. Health Work 2019, 10, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Yusoff, M.S.B. ABC of content validation and content validity index calculation. Educ. Med. J. 2019, 11, 49–54. [Google Scholar] [CrossRef]
- Willis, G.B. Cognitive Interviewing: A Tool for Improving Questionnaire Design; Sage Publications: Thousand Oaks, CA, USA, 2004; pp. 3–35. [Google Scholar]
- Yusoff, M.S.B. ABC of response process validation and face validity index calculation. Educ. Med. J. 2019, 11, 55–61. [Google Scholar] [CrossRef]
- Edelen, M.O.; Reeve, B.B. Applying item response theory (IRT) modeling to questionnaire development, evaluation, and refinement. Qual. Life Res. 2007, 16 (Suppl. 1), 5–18. [Google Scholar] [CrossRef] [PubMed]
- Kline, R. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Publications: New York, NY, USA, 2015; pp. 50–162. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 20 August 2020).
- Baker, F. Item Response Theory. 2001. Available online: http://eric.ed.gov/ERICWebPortal/recordDetail?accno=ED458219%5Cnpapers2://publication/uuid/53C840DD-C92B-4719-8EC3-AF2076EDCAB3 (accessed on 15 July 2020).
- Stenbeck, M.; Hambleton, R.K.; Swaminathan, H.; Rogers, H.J. Fundamentals of item response theory. Contemp. Sociol. 1992, 21, 174. [Google Scholar] [CrossRef]
- Bartholomew, D.J.; Steele, F.; Irini Moustaki, J.I.G.C.H. Analysis of multivariate social science data. Wiley Interdiscip. Rev. Comput. Stat. 2009, 1, 128–129. [Google Scholar]
- Drasgow, F.; Lissak, R.I. Modified parallel analysis: A procedure for examining the latent dimensionality of dichotomously scored item responses. J. Appl. Psychol. 1983, 68, 363–373. [Google Scholar] [CrossRef]
- Costello, A.B.; Osborne, J.W. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar]
- Leech, N.L.; Barrett, K.C.; Morgan, G.A. SPSS for Intermediate Statistics: Use and Interpretation, 2nd ed.; Lawrence Erlbaum Associates: New Jersey, NJ, USA, 2008; pp. 63–89. [Google Scholar]
- Brown, T. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York, NY, USA, 2015; pp. 12–92. [Google Scholar]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting structural equation modeling and confirmatory factor analysis results: A review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Steven Owen, V. Focus on research methods is the. Research in Nursing and Health CVI an Acceptable Indicator of Content Validity? Apprais. Recomm. 2007, 30, 459–467. [Google Scholar]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The performance of RMSEA in models with small degrees of freedom. Sociol. Methods Res. 2015, 44, 486–507. [Google Scholar] [CrossRef]
- Schaap-Jonker, H.; Egberink, I.J.L.; Braam, A.W.; Corveleyn, J.M.T. An item response theory analysis of the questionnaire of God representations. Int. J. Psychol. Relig. 2016, 26, 152–166. [Google Scholar] [CrossRef] [Green Version]
- Goni, M.D.; Naing, N.N.; Hasan, H.; Wan-Arfah, N.; Deris, Z.Z.; Arifin, W.N.; Hussin, T.M.A.R.; Abdulrahman, A.S.; Baaba, A.A.; Arshad, M.R. Development and validation of knowledge, attitude, and practice questionnaire for prevention of respiratory tract infections among Malaysian Hajj pilgrims. BMC Public Health 2020, 20, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahiruddin, W.M.; Arifin, W.N.; Mohd-Nazri, S.; Sukeri, S.; Zawaha, I.; Bakar, R.A.; Hamat, R.A.; Malina, O.; Jamaludin, T.Z.M.T.; Pathman, A.; et al. Development and validation of a new knowledge, attitude, belief, and practice questionnaire on leptospirosis in Malaysia. BMC Public Health 2018, 18, 331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arifin, W.N.; Yusoff, M.S.B. Item response theory for medical educationists. Educ. Med. J. 2017, 9, 69–81. [Google Scholar] [CrossRef]
- Sharma, L.R. Analysis of difficulty index, discrimination index and distractor efficiency of multiple choice questions of speech sounds of English. Int. Res. J. MMC. 2021, 2, 15–28. [Google Scholar] [CrossRef]
- DeVellis, R. Scale Development: Theory and Applications; Sage Publications: Thousand Oaks, CA, USA, 2003; Available online: https://fliphtml5.com/wmkd/bibu/basic%09 (accessed on 2 July 2020).
- Soriano, B.J.N.; Duarte, S.G.; Alonso, A.M.F.; Perales, A.B.; Carreño, T.P. Validation of a questionnaire developed to evaluate a pediatric ehealth website for parents. Int. J. Environ. Res. Public Health 2020, 17, 2671. [Google Scholar] [CrossRef]
- Van Griethuijsen, R.A.L.F.; van Eijck, M.W.; Haste, H.; den Brok, P.J.; Skinner, N.C.; Mansour, N.; Savran Gencer, A.; BouJaoude, S. Global patterns in students’ views of science and interest in science. Res. Sci. Educ. 2015, 45, 581–603. [Google Scholar] [CrossRef]
- Arslan, H.O.; Cigdemoglu, C.; Moseley, C. A Three-Tier Diagnostic Test to Assess Pre-Service Teachers’ Misconceptions about Global Warming, Greenhouse Effect, Ozone Layer Depletion, and acid Rain. Int. J. Sci. Educ. 2012, 34, 1667–1686. [Google Scholar] [CrossRef]
- Nasab, H.S.; Ghofranipour, F.; Kazemnejad, A.; Khavanin, A.; Tavakoli, R. Evaluation of knowledge, attitude, and behavior of workers towards occupational health and safety. Iran. J. Public Health 2009, 38, 125–129. [Google Scholar]
- Bohner, G.; Dickel, N. Attitudes, and attitude change. Annu. Rev. Psychol. 2011, 62, 391–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.; Wang, L.; Yin, X. The factor structure of the 12-item general health questionnaire (GHQ-12) in young Chinese civil servants. Health Qual. Life Outcomes 2016, 14, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar-Elena, R.; Campo-Barrio, A.; Morchón, R.; Martínez-Merino, V. Validation of a questionnaire about the perception of occupational biohazard in Spanish companies. Int. J. Occup. Saf. Ergon. JOSE 2016, 22, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Šegalo, S.; Pašalić, A.; Maestro, D.; Jogunčić, A. Development and validation of the questionnaire for the assessment of the occupational exposure and safety in laboratories. Int. J. Sci. Eng. Res. 2019, 10, 1314–1319. [Google Scholar]
- Hair, J.F.; Black, B.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Prentice Hall: New Jersey, NJ, USA, 2010. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Sections | No. of Items | Concepts Measured | Response Options |
|---|---|---|---|
| Proforma (general information) | 19 | Socio-demographic, job characteristic (working experience (years), job scope), workplace characteristic, training, source of information | Closed-ended, multiple-choice |
| Knowledge | 8 (1 reverse statement) | General requirement on safe working in confined spaces, confined spaces entry program, employee training and safety equipment | True/False/Unsure; 1 = True 2 = False 3 = Unsure |
| Attitude | 10 (1 reverse-scored item) | Measure three components towards safe working in confined spaces based on tri-partite theory (Lawrence, 2008). The following components as below:
| Five-Likert scale option 1 = Strongly disagree 2 = Disagree 3 = Unsure 4 = Agree 5 = Strongly agree |
| Practice | 12 | Practices on safe working in confined spaces | Four- Likert scale option 1 = Never 2 = Seldom 3 = Often 4 = Always |
| Variables | Mean (SD) | n (%) |
|---|---|---|
| Age (year) | 32.1 (9.80) | |
| Gender | ||
| Male | 337 (96.3) | |
| Female | 13 (3.7) | |
| Ethnicity | ||
| Malay | 338 (96.6) | |
| vNon-Malay | 12 (3.4) | |
| Marital status | ||
| Single | 171 (48.8) | |
| Married | 177 (50.6) | |
| Widow/widower | 2 (0.6) | |
| Educational level | ||
| No formal education | 1 (0.3) | |
| Primary | 3 (0.9) | |
| Secondary | 165 (47.1) | |
| Tertiary | 181 (51.7) | |
| Employment | ||
| Total work experience (years) | 8.3 (7.96) | |
| Experience in CS (years) | 4.5 (5.62) | |
| Working hour in CS per day | ||
| ≤1 | 298 (85.1) | |
| 2–5 | 40 (11.5) | |
| >5 | 12 (3.4) | |
| Job scope | ||
| Cleaning | 90 (25.7) | |
| Inspection | 24 (6.9) | |
| Maintenance | 110 (31.4) | |
| Production | 126 (36.0) | |
| Training | ||
| Yes | 328 (93.7) | |
| No | 22 (6.3) | |
| Have heard on ICOPs | ||
| Yes | 346 (98.9) | |
| No | 4 (1.1) |
| Items after Removal | b (SE) | α (SE) | χ2 (df = 8) | p Value |
|---|---|---|---|---|
| K1 Occupational risk assessment (Hazard identification, risk assessment and risk control-HIRARC) must be done before the entry of workers in confined spaces | −2.04 (0.09) | 10.89 (34.64) | 2.39 | 0.967 |
| K2 Employers need to ensure that warning signs “DANGER-CONFINED SPACE. NO ENTRY” is placed near the entrance of the confined spaces | −2.44 (0.50) | 2.42 (1.18) | 10.72 | 0.213 |
| K3 Confined space workers are exposed to hazardous gases within the scope of the workplace | −2.84 (0.83) | 1.74 (0.89) | 21.34 | 0.013 |
| K4 Confined space workers must have confined space entry training recognized by the Department of Occupational Safety and Health | −2.30 (0.47) | 1.97 (0.81) | 32.67 | <0.001 |
| K5 Ventilation in the confined space should be placed at the beginning of the confined space work only when work is carried out | −1.83 (0.59) | 0.87 (0.35) | 13.26 | 0.120 |
| K6 Exhaust from any equipment placed near a confined space is the cause of the existence of a hazardous atmosphere in the confined space | −2.00 (0.41) | 1.53 (0.53) | 56.50 | 0.008 |
| K7 Difficulty breathing is a sign of exposure to hazardous atmosphere when working in a confined space | −2.31 (0.40) | 2.53 (1.15) | 22.83 | 0.062 |
| Factors | Items | EFA (n = 150) | CFA (n = 200) | ||
|---|---|---|---|---|---|
| λ | Reliability a | λ | Reliability b | ||
| Attitude | A2 I believe employees and employers are fully responsible for the safety of employees in the workplace | 0.74 | 0.804 | 0.70 | 0.814 |
| A3 I believe the entry permit to the confined space needs to be informed and explained to the employees before the confined space work is carried out | 0.77 | 0.64 | |||
| A6 I will stop working in confined space if the gas tester level indicator exceeds the set standards | 0.46 | - | |||
| A8 I think the health check-ups of confined space workers should be done periodically | 0.47 | 0.45 | |||
| A9 I believe occupational health and safety campaigns are an effective way to promote and educate employees | 0.68 | 0.69 | |||
| A10 Occupational health and safety are my top priority when I do the confined space work | 0.82 | 0.87 | |||
| Practice | P1 I will check the confined space work permit before handling work in the confined space | 0.49 | 0.917 | - | 0.912 |
| P2 I make sure the situation in the confined space is safe before entering the confined space | 0.78 | 0.72 | |||
| P3 I check all safety equipment and work tools are in a safe condition to use | 0.82 | 0.77 | |||
| P4 I tell the employer if the safety equipment to do the work in the confined space is incomplete | 0.79 | 0.72 | |||
| P5 I wear safety gloves while handling work in confined spaces | 0.89 | 0.88 | |||
| P6 I wear a safety helmet when handling work in a confined space | 0.90 | 0.88 | |||
| P7 I wear eye protection when handling work in a confined space | 0.85 | 0.87 | |||
| P8 I wear ear protection when handling work in a confined space | 0.78 | 0.81 | |||
| P9 I wear respiratory protection while handling work in a confined space | 0.88 | 0.81 | |||
| P10 I wear a body harness while handling work in a confined space | 0.57 | 0.57 | |||
| P11 I wear a reflective safety jacket while handling work in a confined space | 0.55 | 0.60 | |||
| P12 I joined the employer for a feedback session after the end of the confined space entry operation | 0.45 | - | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngah, H.; Mohd Hairon, S.; Hamzah, N.A.; Noordin, S.; Shafei, M.N. Development and Validation of Knowledge, Attitude, and Practice Questionnaire: Toward Safe Working in Confined Spaces. Int. J. Environ. Res. Public Health 2022, 19, 1242. https://doi.org/10.3390/ijerph19031242
Ngah H, Mohd Hairon S, Hamzah NA, Noordin S, Shafei MN. Development and Validation of Knowledge, Attitude, and Practice Questionnaire: Toward Safe Working in Confined Spaces. International Journal of Environmental Research and Public Health. 2022; 19(3):1242. https://doi.org/10.3390/ijerph19031242
Chicago/Turabian StyleNgah, Hamiza, Suhaily Mohd Hairon, Nurul Ainun Hamzah, Shahronizam Noordin, and Mohd Nazri Shafei. 2022. "Development and Validation of Knowledge, Attitude, and Practice Questionnaire: Toward Safe Working in Confined Spaces" International Journal of Environmental Research and Public Health 19, no. 3: 1242. https://doi.org/10.3390/ijerph19031242