
Advanced Operationalization Framework for Climate-Resilient Urban Public Health Care Services: Composite Indicators-Based Scenario Assessment of Khon Kaen City, Thailand


Abstract
:1. Introduction
2. Materials and Methods
2.1. Scenarios Storyline Development
2.2. Composite Indicators Development
2.2.1. Indicators Identification
2.2.2. Normalization and Aggregation
- Sub-indicator layer: Input data were derived from both the public health care facilities’ questionnaire survey and the given scenario storylines. Distance to target normalization was applied for representing a fraction of the highest target value, which conserves the proportion and trackability of the original data. All sub-indicators under an indicator were calculated with equal-weighted arithmetic (additive) aggregation to represent an indicator.
- Indicator level: An indicator represents a value of at least one sub-indicator or an average value of many sub-indicators. Conceptually, individual indicators shall have a different degree of influence on the outcome of the potential impact pillar to which it belongs. Therefore, proportionately weighted normalization was used for the indicator layer; a single attribute value was divided by the sum total of the values of attributes. Weighted values can be assigned based on the experts’ judgement (hazards and vulnerability-related indicators) and equal-weighted (exposure-related indicators). In terms of aggregation scheme selection, there is a possibility that at least one of the indicator’s values may contain “0”; hence, arithmetic (additive) aggregation is operated.
- Pillar level: Based on the IPCC climate risk concept [18], the potential impact is a multiplication result of hazard, exposure, and vulnerability pillars. Therefore, the absence of one pillar or being assigned as 0 in one of the terms meant no potential impact occurred. To this connection, the geometric (multiplicative) aggregation method is executed for this non-compensability relationship among the pillars. In this regard, the possibility of potential impact value derived from the set of the composite indicators must be present in absolute terms between 0 to 1. A value of 0 means no potential impact, and 1 is the possible worst potential impact.
2.3. Questionnaire Survey and Data Analysis
2.4. Sensitivity Analysis
3. Results
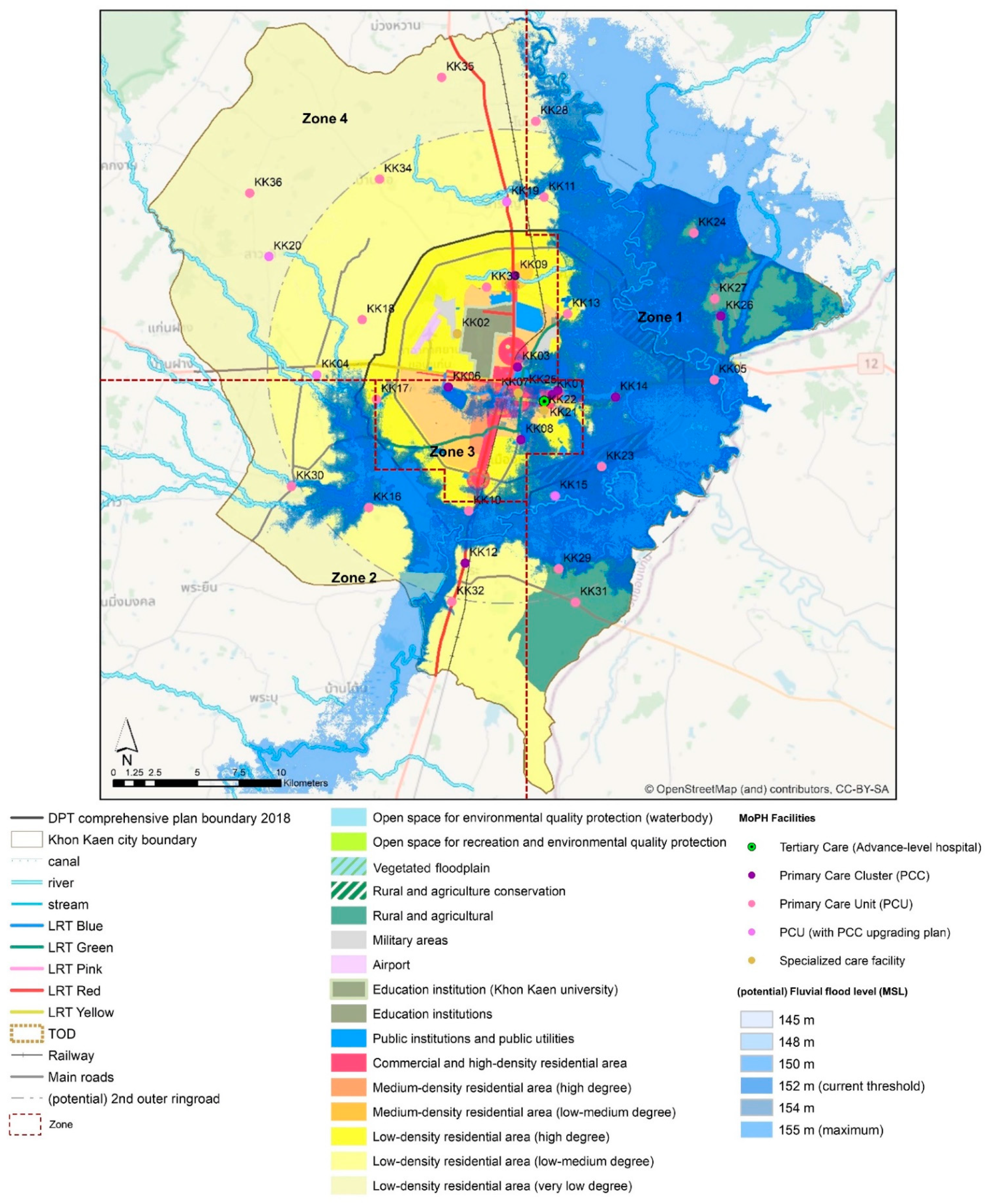
3.1. Study Area—Khon Kaen City
3.2. Khon Kaen City Thailand in 2037
3.2.1. Trend Scenario Storyline
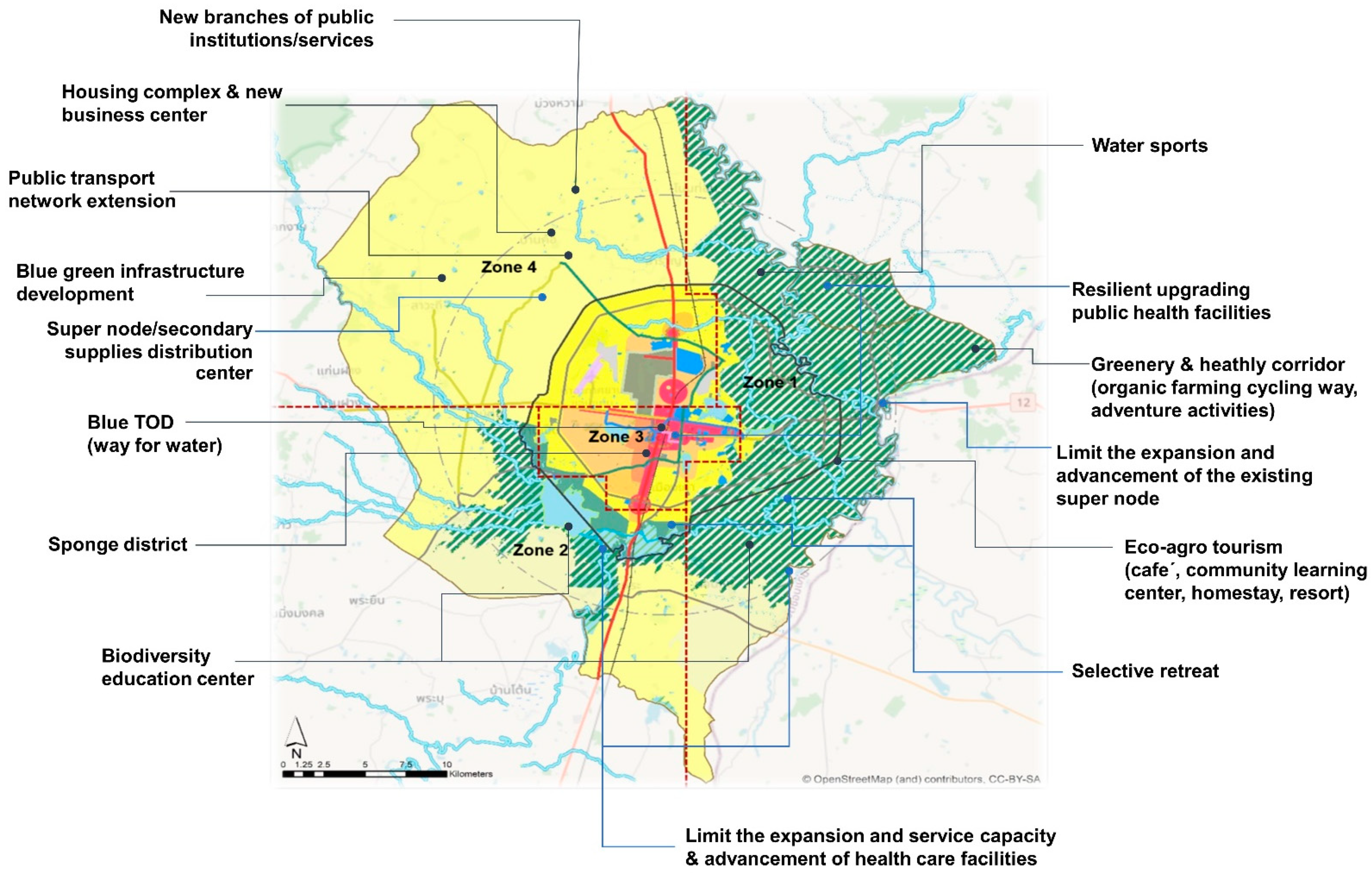
3.2.2. Desirable Scenario Storyline
3.3. Composite Indicators Development
3.3.1. Sensitivity
3.3.2. Coping Capacity and Adaptive Capacity
3.4. Dataset and Normalization
3.5. Potential Impact Analysis
3.6. Sensitivity Analysis
4. Discussion
4.1. Composite Indicators-Based Scenario Assessment—A Novel Tool for Climate-Resilient Health Care Services
4.2. Constraints and Scalability Opportunities
4.2.1. Sectoral Benchmarking in Needs
4.2.2. Data Constraints and Statistical Conciseness
- Balancing the number of indicators
- Statistical and Theoretical Convergence
- Quality of Input Data
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organization). Hospitals Safe from Disasters; United Nations: New York, NY, USA, 2009; pp. 1–31. Available online: http://www.unisdr.org/2009/campaign/pdf/wdrc-2008-2009-information-kit.pdf (accessed on 26 July 2019).
- JC (The Joint Commission). Emergency Management in Health Care. An All Hazards Approach, 4th ed.; Hible, L., Ed.; Joint Commission Resources, Inc.: Oak Brook, IL, USA, 2019. [Google Scholar]
- WHO (World Health Organization). Comprehensive Safe Hospital Framework; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- WHO (World Health Organization); PAHO (Pan American Health Organization). Hospital Safety Index: Guide for Evaluators. 2015. Available online: http://www.who.int/hac/techguidance/hospital_safety_index_evaluators.pdf (accessed on 26 July 2019).
- WHO (World Health Organization). Operational Framework for Building Climate Resilient Health Systems; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- WHO (World Health Organization). WHO Guidance for Climate Resilient and Environmentally Sustainable Health Care Facilities; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- CCGHC (Canadian Coalition for Green Health Care). Health Care Facility Climate Change Resiliency Toolkit. 2021. Available online: https://greenhealthcare.ca/climatescorecard/introduction1 (accessed on 19 March 2021).
- Paterson, J.; Berry, P.; Ebi, K.; Varangu, L. Health Care Facilities Resilient to Climate Change Impacts. Int. J. Environ. Res. Public Health 2014, 11, 13097–13116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HHS (U.S. Department of Health and Human Services). Sustainable and Climate Resilient Health Care Facilities Toolkit. 2018. Available online: https://toolkit.climate.gov/tool/sustainable-and-climate-resilient-health-care-facilities-toolkit#:~:text=This%20toolkit%20includes%20a%20best,associated%20with%20climate%20change%20impacts (accessed on 26 July 2019).
- Hinkel, J. “Indicators of vulnerability and adaptive capacity”: Towards a clarification of the science-policy interface. Glob. Environ. Chang. 2011, 21, 198–208. [Google Scholar] [CrossRef]
- Nardo, M.; Saisana, M.; Saltelli, A.; Tarantola, S. Tools for composite indicators building. Eur. Comm. Rev. Ispra 2005, 15, 19–20. [Google Scholar]
- Becker, W.; Paruolo, P.; Saisana, M.; Saltelli, A. Weights and Importance in Composite Indicators: Mind the Gap. In Handbook of Uncertainty Quantification; Ghanem, R., Owhadi, H., Higdon, D., Eds.; Springer International Publishing: Cham, Swizerland, 2015; pp. 1–30. [Google Scholar] [CrossRef]
- Talukder, B.; Hipel, K.W.; van Loon, G.W. Developing composite indicators for agricultural sustainability assessment: Effect of normalization and aggregation techniques. Resources 2017, 6, 66. [Google Scholar] [CrossRef] [Green Version]
- Paruolo, P.; Saisana, M.; Saltelli, A. Ratings and rankings: Voodoo or science? J. R. Stat. Soc. Ser. A Stat. Soc. 2013, 176, 609–634. [Google Scholar] [CrossRef] [Green Version]
- Greiving, S. Analyse- und Bewertungskonzepte für Risiken im Vergleich. Inf. Zur Raumentwickl. 2019, 46, 62–73. [Google Scholar]
- Beccari, B. Correction: A Comparative Analysis of Disaster Risk, Vulnerability and Resilience Composite Indicators. PLoS Curr. 2016, 14, 8. [Google Scholar] [CrossRef]
- Parsons, M.; Glavac, S.; Hastings, P.; Marshall, G.; McGregor, J.; McNeill, J.; Stayner, R. Top-down assessment of disaster resilience: A conceptual framework using coping and adaptive capacities. Int. J. Disaster Risk Reduct. 2016, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Oppenheimer, M.; Campos, M.; Warren, R.; Birkmann, J.; Luber, G.; O’Neill, B.; Takahashi, K. Emergent Risks and Key Vulnerabilities. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Recursos Naturales y ambiente; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; Available online: https://www.ipcc.ch/site/assets/uploads/2018/02/WGIIAR5-Chap19_FINAL.pdf (accessed on 26 June 2019).
- Birkmann, J. (Ed.) Data, Indicators and Criteria for Measuring Vulnerability: Theoretical Bases and Requirements in Measuring Vulnerability to Natural Hazards: Towards Disaster Resilient Societies, 2nd ed.; United Nations University Press: Tokyo, Japan, 2013; Available online: http://archive.unu.edu/unupress/sample-chapters/1135-MeasuringVulnerabilityToNaturalHazards.pdf (accessed on 23 January 2020).
- O’Brien, K.; Eriksen, S.; Nygaard, L.P.; Schjolden, A. Why different interpretations of vulnerability matter in climate change discourses. Clim. Policy 2007, 7, 73–88. [Google Scholar] [CrossRef]
- De Marchi, B.; Scolobig, A. The views of experts and residents on social vulnerability to flash floods in an Alpine region of Italy. Disasters 2012, 36, 316–337. [Google Scholar] [CrossRef]
- de Andrade, M.M.N.; Szlafsztein, C.F. Vulnerability assessment including tangible and intangible components in the index composition: An Amazon case study of flooding and flash flooding. Sci. Total Environ. 2018, 630, 903–912. [Google Scholar] [CrossRef] [PubMed]
- Ebi, K.L.; Boyer, C.; Bowen, K.J.; Frumkin, H.; Hess, J. Monitoring and evaluation indicators for climate change-related health impacts, risks, adaptation, and resilience. Int. J. Environ. Res. Public Health 2018, 15, 1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biddle, L.; Wahedi, K.; Bozorgmehr, K. Health system resilience: A literature review of empirical research. Health Policy Plan. 2020, 35, 1084–1109. [Google Scholar] [CrossRef]
- Greiving, S.; Arens, S.; Becker, D.; Fleischhauer, M.; Hurth, F. Improving the as-sessment of potential and actual impacts of climate change and extreme events through a parallel modelling of climatic and societal changes at different scales. J. Extrem. Events 2018, 4, 1850003. [Google Scholar] [CrossRef]
- Godschalk, D.R. Urban Hazard Migration: Creating Resilient Cities. Nat. Hazards Rev. 2003, 6988, 136–143. [Google Scholar] [CrossRef]
- Tanner, T.; Mitchell, T.; Polack, E.; Guenther, B. Urban Governance for Adaptation: Assessing Climate Change Resilience in Ten Asian Cities. IDS Work. Pap. 2009, 2009, 1–47. [Google Scholar] [CrossRef]
- Bahadur, A.V.V.; Ibrahim, M.; Tanner, T. The resilience renaissance? Unpacking of resilience for tackling climate change and disasters. In Strengthening Climate Resilience Discussion Paper 1; IDS: Brighton, UK, 2010; 45p. [Google Scholar]
- Ahern, J. From fail-safe to safe-to-fail: Sustainability and resilience in the new urban world. Landsc. Urban Plan. 2011, 100, 341–343. [Google Scholar] [CrossRef] [Green Version]
- Liao, K.H. A theory on urban resilience to floods-A basis for alternative planning practices. Ecol. Soc. 2012, 17, 48. [Google Scholar] [CrossRef]
- Rodin, J. The Resilience Dividend: Being Strong in a World Where Things Go Wrong; Public Affairs: Seattle, WA, USA, 2014. [Google Scholar]
- The Rockefeller Foundation & ARUP. City Resilience Index; The Rockefeller Foundation & ARUP: London, UK, 2015. [Google Scholar]
- Tyler, S.; Nugraha, E.; Nguyen, H.K.; Nguyen, N.; Van Sari, A.D.; Thinpanga, P.; Verma, S.S. Indicators of urban climate resilience: A contextual approach. Environ. Sci. Policy 2016, 66, 420–426. [Google Scholar] [CrossRef]
- UNISDR. Disaster Resilience Scorecard for Cities; UNISDR: Geneva, Switzerland, 2015; Volume 56. [Google Scholar]
- Meerow, S.; Stults, M. Comparing conceptualizations of urban climate resilience in theory and practice. Sustainability 2016, 8, 701. [Google Scholar] [CrossRef] [Green Version]
- DOH-HEMS (Department of Health-Health Emergency Management Staff). Safe Hospitals in Emergencies and Disasters: Philippine Indicators; DOH-HEMS: Manila, Philippines, 2009. Available online: http://home.doh.gov.ph/uploads/downloads/DOH_INTRANET_safehospitalsinemergenciesphilippineindicators_225104.pdf (accessed on 17 April 2019).
- Relias. A 96-Hour Wait: The Joint Commission’s New Emergency Plan for Hospitals. 2008. Available online: https://www.reliasmedia.com/articles/16281-a-96-hour-wait-the-joint-commission-s-new-emergency-plan-for-hospitals (accessed on 26 March 2019).
- Guenther, R.; Balbus, J. Primary Protection: Enhancing Health Care Resilience for a Changing Climate. 2014. Available online: https://toolkit.climate.gov/sites/default/files/SCRHCFIBestPracticesReportfinal22014Web.pdf (accessed on 12 July 2019).
- Health Research & Educational Trust. Increasing Supplier Diversity in Health Care; Health Research & Educational Trust: Chicago, IL, USA, 2015. Available online: https://www.aha.org/system/files/hpoe/Reports-HPOE/2015/2015_supplier_diversity_FINAL.pdf (accessed on 15 September 2019).
- IROQUOIS. 96 Hour Sustainability Assessment Hospital Planning Guidance. 2018. Available online: http://www.iroquois.org/wp-content/uploads/2018/06/96-Hour-Sustainability-Assessment-Planning-Guidance-v6-15-18.pdf (accessed on 17 July 2019).
- University of Rochester. 96 Hour Sustainability. 2021. Available online: https://www.urmc.rochester.edu/emergency-preparedness/preparedness-and-response-tools-resources/96-hour-sustainability.aspx (accessed on 17 April 2021).
- JC (The Joint Commission). Plans-Emergency Management 96 Hour Plan. 2021. Available online: https://www.jointcommission.org/standards/standard-faqs/critical-access-hospital/emergency-management-em/000001216/?p=1 (accessed on 17 April 2021).
- HHS (U.S. Department of Health and Human Services). Hospital All-Hazards Self-Assessment (HAH). Available online: https://www.cdc.gov/cpr/readiness/healthcare/documents/hah_508_compliant_final.pdf (accessed on 12 July 2019).
- U.S. Healthcare & Public Health Sector Coordinating Councils. Working without Technology: How Hospitals and Healthcare Organizations Can Manage Communication Failure. Available online: https://www.phe.gov/Preparedness/planning/cip/Documents/workingwithouttechnology.pdf (accessed on 21 June 2019).
- Design and Construction Division. Sustainable Architecture: Concept and Implementation for Primary Care Unit in Thailand; Department of Health Service Support, Ministry of Public Health, Printing Business Office War Veterans Organization of Thailand: Bangkok, Thailand, 2007; 219p. (In Thai)
- DMS (Department of Medical Service). Hospital Safety Index: Guide for Evaluator. 2018. Available online: https://www.dms.go.th/backend//Content/Content_File/Population_Health/Attach/25621118161500PM_HSI.pdf?contentId=18325 (accessed on 26 July 2019). (In Thai)
- Levinson, D.R. Hospital Emergency Preparedness and Response during Superstorm Sandy. 2014. Available online: https://www.hsdl.org/?view&did=757768 (accessed on 21 June 2019).
- Palmer, J. Five Lessons That Have Made Hospitals Better Prepared Since Hurricanes Katrina and Sandy. 2017. Available online: https://www.psqh.com/news/five-lessons-made-hospitals-better-prepared-since-hurricanes-katrina-sandy/ (accessed on 12 May 2018).
- Thammasat University Hospital. History of the 2011 Flood Crisis of Thammasat Chalermprakiat Hospital; Nititham Printing: Bangkok, Thailand, 2012; 224p. (In Thai) [Google Scholar]
- Goddard, M.; Jacobs, R. Using composite indicators to measure performance in health care. In Performance Measurement for Health System Improvement; Smith, P.C., Mossialos, E., Papanicolas, I., Eds.; Cambridge University Press: Cambridge, UK, 2010; pp. 339–368. [Google Scholar] [CrossRef]
- Hiete, M.; Merz, M.; Schultmann, F. Scenario-based impact analysis of a power outage on healthcare facilities in Germany. Int. J. Disaster Resil. Built Environ. 2011, 2, 222–244. [Google Scholar] [CrossRef]
- Hollnagel, E.; Braithwaite, J.; Wears, R.L. (Eds.) Resilient Health Care; Ashgate: Farnham, UK, 2013. [Google Scholar]
- Braithwaite, J.; Wears, R.L.; Hollnagel, E. Resilient health care: Reconciling work-as-imagined and work-as-done. In Resilient Health Care: Reconciling Work-as-Imagined and Work-as-Done; CRC Press: London, UK, 2016; Volume 3. [Google Scholar] [CrossRef]
- Riaz, N.; Wolden, S.L.; Gelblum, D.Y.; Eric, J. A Community Checklist for Health Sector Resilience Informed by Hurricane Sandy. HHS Public Access 2016, 118, 6072–6078. [Google Scholar] [CrossRef]
- Kruk, M.E.; Ling, E.J.; Bitton, A.; Cammett, M.; Cavanaugh, K.; Chopra, M.; Warnken, H. Building resilient health systems: A proposal for a resilience index. BMJ 2017, 357, j2323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jollife, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374. [Google Scholar] [CrossRef] [PubMed]
- Ringnér, M. What is principal component analysis? Nat. Biotechnol. 2008, 26, 303–304. [Google Scholar] [CrossRef] [PubMed]
- OCHA Service. Thailand-Subnational Administrative Boundaries. 2021. Available online: https://data.humdata.org/dataset/thailand-administrative-boundaries (accessed on 15 April 2021).
- KKH—Khon Kaen Hospital. Direction and Strategic Plan of Khon Kaen Hospital 2016–2020; Khon Kaen Hospital Policy and Strategy Division: Khon Kaen, Thailand, 2016; Available online: https://www.kkh.go.th/wp-content/uploads/2018/04/เล่ม-แผนยุทธศาสตร์-2020-ฉ-แก้ไขครั้งที่-1-V2.pdf (accessed on 4 March 2021). (In Thai)
- Council of the European Union. Council Directive 2008/114/EC of 8 December 2008 on the Identification and Designation of European Critical Infrastructures and the Assessment of the Need to Improve Their Protection. 2008. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2008:345:0075:0082:EN:PDF (accessed on 16 November 2021).
- Ferketich, S. Focus on Psychometrics: Aspects of Item Analysis. Res. Nurs. Health 1991, 14, 165–168. [Google Scholar] [CrossRef]
- Björklund, M. Be careful with your principal components. Evolution 2019, 73, 2151–2158. [Google Scholar] [CrossRef]
- Health Catalyst. The Four Keys to Increasing Hospital Capacity without Construction This Site Uses Cookies Impacts of Limited Hospital Capacity. 2019. Available online: https://www.healthcatalyst.com/insights/increasing-hospital-capacity-4-keys (accessed on 7 September 2020).
- WHO (World Health Organization). Vulnerable Groups. 2020. Available online: https://www.who.int/environmental_health_emergencies/vulnerable_groups/en/ (accessed on 7 September 2020).
- Srisasalux, J. Vulnerable Groups: Who are They and what are Relevant Ethical Concerns (กลุ่มเปราะบาง (Vulnerable Groups) คือใคร มีข้อพิจารณาด้านจริยธรรมอย่างไร); Health System Research Insititute (HSRI): Nonthaburi, Thailand, 2013; Available online: https://kb.hsri.or.th/dspace/bitstream/handle/11228/3717/jaruayporn.pdf?sequence=2&isAllowed=y (accessed on 7 September 2020). (In Thai)
- Marder, K. Identifying Vulnerable Patients and Why They Matter. 2018. Available online: https://www.healthcatalyst.com/insights/identifying-vulnerable-patients-why-they-matter (accessed on 7 September 2020).
- ThaiPublica. Crisis of the Thai Public Health System Reveals 558 Government Hospitals Financial Deficits,−12,700 Mio THB (วิกฤติระบบสาธารณสุขไทย กางตัวเลข รพ.รัฐ เงินบํารุงติดลบ 558 แห่ง 12,700 ล้าน). 2017. Available online: https://thaipublica.org/2017/12/public-health-services-65/ (accessed on 7 September 2020). (In Thai).
- Barria, S. Will Thailand’s Universal Health Care System Keep Its Reputation in the Face of COVID-19? 2020. Available online: https://publicservices.international/resources/news/will-thailands-universal-health-care-system-keep-its-reputation-in-the-face-of-covid-19?id=10717&lang=en#_ftn3 (accessed on 7 September 2020).
- Wikipedia. Downtime. 2020. Available online: https://en.wikipedia.org/wiki/Downtime (accessed on 7 September 2020).
- JCI (Joint Commission International). Planned and Unplanned Downtime–Part 1–Communication. 2020. Available online: https://www.jointcommissioninternational.org/standards/hospital-standards-communication-center/planned-and-unplanned-downtime-part-1-communication/ (accessed on 7 September 2020).
- Vorne. Reduce Down Time in Manufacturing. 2020. Available online: https://www.vorne.com/solutions/reduce-down-time-in-manufacturing.htm (accessed on 7 September 2020).
- Schank, J.; Savitz, S.; Munson, K.; Perkinson, B.; McGee, J.; Sollinger, J. Designing Adaptable Ships: Modularity and Flexibility in Future Ship Designs. In Designing Adaptable Ships: Modularity and Flexibility in Future Ship Designs; RAND Corporation: Santa Monica, CA, USA, 2016. [Google Scholar] [CrossRef] [Green Version]
- IGI Global. Modularity. 2020. Available online: https://www.igi-global.com/dictionary/modularity/19145 (accessed on 14 September 2020).
- Baldwin, C.Y.; Clark, K.B. What Is Modularity. In Design Rules: The Power of Modularity; MIT Press: Cambridge, UK; London, UK, 2000; Available online: https://ebookcentral.proquest.com/lib/dortmundtech/detail.action?docID=3338418 (accessed on 15 September 2020).
- Cambridge. Cambridge Free English Dictionary and Thesaurus. 2020. Available online: https://dictionary.cambridge.org/dictionary/ (accessed on 7 September 2020).
- Syahrir, I.; Vanany, I. Healthcare and Disaster Supply Chain: Literature Review and Future Research. Procedia Manuf. 2015, 4, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Ow, B. Redundancy in Systems is Critical. 2018. Available online: https://medium.com/@AxelUnlimited/redundancy-in-systems-is-critical-5471b79a3b17 (accessed on 15 September 2020).
- Husted, J.A.; Cook, R.J.; Farewell, V.T.; Gladman, D.D. Methods for assessing responsiveness: A critical review and recommendations. J. Clin. Epidemiol. 2000, 53, 459–468. [Google Scholar] [CrossRef]
- Seltzer, B.J. What is Resource Mobilization and Why Is It So Important? 2014. Available online: https://healthcommcapacity.org/resource-mobilization-important/#:~:text=Resource%20mobilization%20refers%20to%20all,as%20%E2%80%9CNew%20Business%20Development%E2%80%9D (accessed on 15 September 2020).
- Lillrank, P. Integration and coordination in healthcare: An operations management view. J. Integr. Care 2012, 20, 6–12. [Google Scholar] [CrossRef]
- Subedi, J. Disaster informatics: Information management as a tool for effective disaster risk reduction. Advanced ICTs for Disaster Management and Threat Detection: Collaborative and Distributed Frameworks. In Information Science Reference; IGI Global: Hershey, Pennsylvania, USA, 2010; pp. 80–93. [Google Scholar]
- UNDRR (United Nations Office for Disaster Risk Reduction). Terminology. 2020. Available online: https://www.undrr.org/terminology (accessed on 7 September 2020).
- Quick, K.S.; Feldman, M.S. Distinguishing participation and inclusion. J. Plan. Educ. Res. 2011, 31, 272–290. [Google Scholar] [CrossRef]
- Zubir, S.S.; Amirrol, H. Disaster risk reduction through community participation. WIT Trans. Ecol. Environ. 2011, 148, 195–206. [Google Scholar] [CrossRef] [Green Version]
- UNDP (United Nations Development Programme). Capacity Development for Disaster Risk Reduction; UNDP: New York, NY, USA, 2010. [Google Scholar]
- Zamfir, I. Understanding Capacity-Building/Capacity Development: A Core Concept of Development Policy; European Parliamentary Research Service: Brussels, Belgium, 2017; Available online: https://www.europarl.europa.eu/thinktank/en/document.html?reference=EPRS_BRI(2017)599411 (accessed on 17 September 2020).
- Greiving, S.; Zebisch, M.; Schneiderbauer, S.; Fleischhauer, M.; Lindner, C.; Lückenkötter, J.; Schauser, I. A consensus based vulnerability assessment to climate change in Germany. Int. J. Clim. Change Strateg. Manag. 2015, 7, 306–326. [Google Scholar] [CrossRef]
- UNISDR (United Nations International Strategy for Disaster Reduction). UNISDR Monitoring and Evaluation Framework; UNISDR: Geneva, Switzerland, 2015; Available online: https://www.undrr.org/publication/monitoring-and-evaluation-framework (accessed on 17 September 2020).
- Katich, K. Monitoring and evaluation in Disaster Risk Management. In EAP DRM Knowledge Notes; No. 21; World Bank: Washington, DC, USA, 2010; pp. 1–12. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Composite Indicator Layers | Aggregation Schemes | Weighting Schemes | Normalization Schemes |
|---|---|---|---|
| Pillar | Multiplicative | Equal weight | Proportionate normalization |
| Indicator | Additive | Equal weight and Expert weight | Proportionate normalization |
| Sub-indicator | Additive | Equal weight | Distance to target normalization |
| Indicators | Trend Scenario | Desired Scenario | ||
|---|---|---|---|---|
| Area-Based | Service Network | Area-Based | Service Network | |
| H1: Fluvial flood | 0.588 | 0.639 | 0.588 | 0.639 |
| H2: Pluvial flood | 1.279 | 1.279 | 1.279 | 1.279 |
| H3: Water scarcity | 1.442 | 1.442 | 1.442 | 1.442 |
| Weighted normalized Hazard | 0.827 | 0.840 | 0.827 | 0.840 |
| E1: Exposure of public health facility’s building(s) | 1.040 | 1.017 | 1.040 | 1.017 |
| E2: Exposure of working systems | 1.594 | 1.178 | 0.263 | 0.279 |
| Weighted normalized Exposure | 0.659 | 0.549 | 0.326 | 0.324 |
| V1: Over carrying capacity | 0.800 | 0.800 | 0.480 | 0.710 |
| V2: Variety of vulnerable patients | 0.683 | 0.778 | 0.683 | 0.778 |
| V3: Resource insufficiency | 0.624 | 0.608 | 0.440 | 0.555 |
| V4: Poor system conditions and maintenance of essential working systems | 0.064 | 0.033 | 0.000 | 0.000 |
| V5: Downtime of essential working systems | 0.053 | 0.045 | 0.053 | 0.045 |
| V6: Flexibility and modularity | 0.456 | 0.480 | 0.000 | 0.000 |
| V7: Diversity of suppliers | 0.217 | 0.122 | 0.047 | 0.031 |
| V8: Redundancy | 0.416 | 0.397 | 0.081 | 0.097 |
| V9: Responsiveness | 0.626 | 0.559 | 0.000 | 0.000 |
| V10: Resource mobilization | 0.359 | 0.535 | 0.000 | 0.000 |
| V11: Integration and coordination | 0.300 | 0.084 | 0.000 | 0.000 |
| V12: Information | 0.388 | 0.424 | 0.000 | 0.000 |
| V13: Preparedness and risk transfer | 0.720 | 0.594 | 0.000 | 0.000 |
| V14: Participation and inclusiveness | 0.742 | 0.808 | 0.000 | 0.000 |
| V15: Capacity development | 0.642 | 0.167 | 0.000 | 0.000 |
| V16: Mainstreaming climate-risk in planning process | 0.440 | 0.487 | 0.000 | 0.000 |
| V17: Monitoring and evaluation | 0.300 | 0.323 | 0.000 | 0.000 |
| Weighted normalized Vulnerability | 0.461 | 0.426 | 0.105 | 0.130 |
| Potential impact = HxExV Very low (0.000–0.016) Low (>0.016–0.125) Medium (>0.125–0.422) High (>0.422–1.000) | 0.251 | 0.196 | 0.028 | 0.035 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puntub, W.; Greiving, S. Advanced Operationalization Framework for Climate-Resilient Urban Public Health Care Services: Composite Indicators-Based Scenario Assessment of Khon Kaen City, Thailand. Int. J. Environ. Res. Public Health 2022, 19, 1283. https://doi.org/10.3390/ijerph19031283
Puntub W, Greiving S. Advanced Operationalization Framework for Climate-Resilient Urban Public Health Care Services: Composite Indicators-Based Scenario Assessment of Khon Kaen City, Thailand. International Journal of Environmental Research and Public Health. 2022; 19(3):1283. https://doi.org/10.3390/ijerph19031283
Chicago/Turabian StylePuntub, Wiriya, and Stefan Greiving. 2022. "Advanced Operationalization Framework for Climate-Resilient Urban Public Health Care Services: Composite Indicators-Based Scenario Assessment of Khon Kaen City, Thailand" International Journal of Environmental Research and Public Health 19, no. 3: 1283. https://doi.org/10.3390/ijerph19031283